
The Health History of First-Degree Relatives’ Dyslipidemia Can Affect Preferences and Intentions following the Return of Genomic Results for Monogenic Familial Hypercholesterolemia

 ,
,  , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Materials and Methods
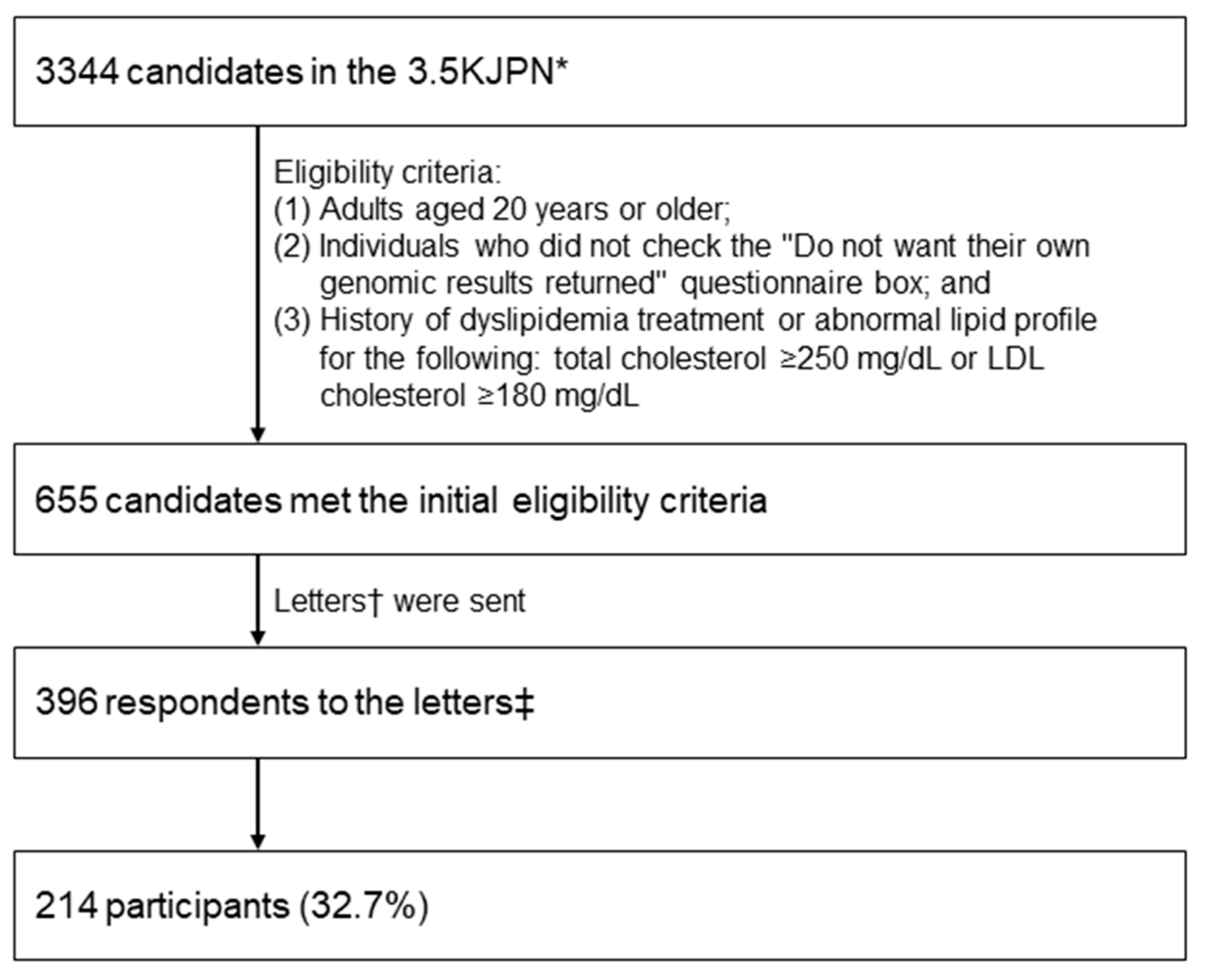
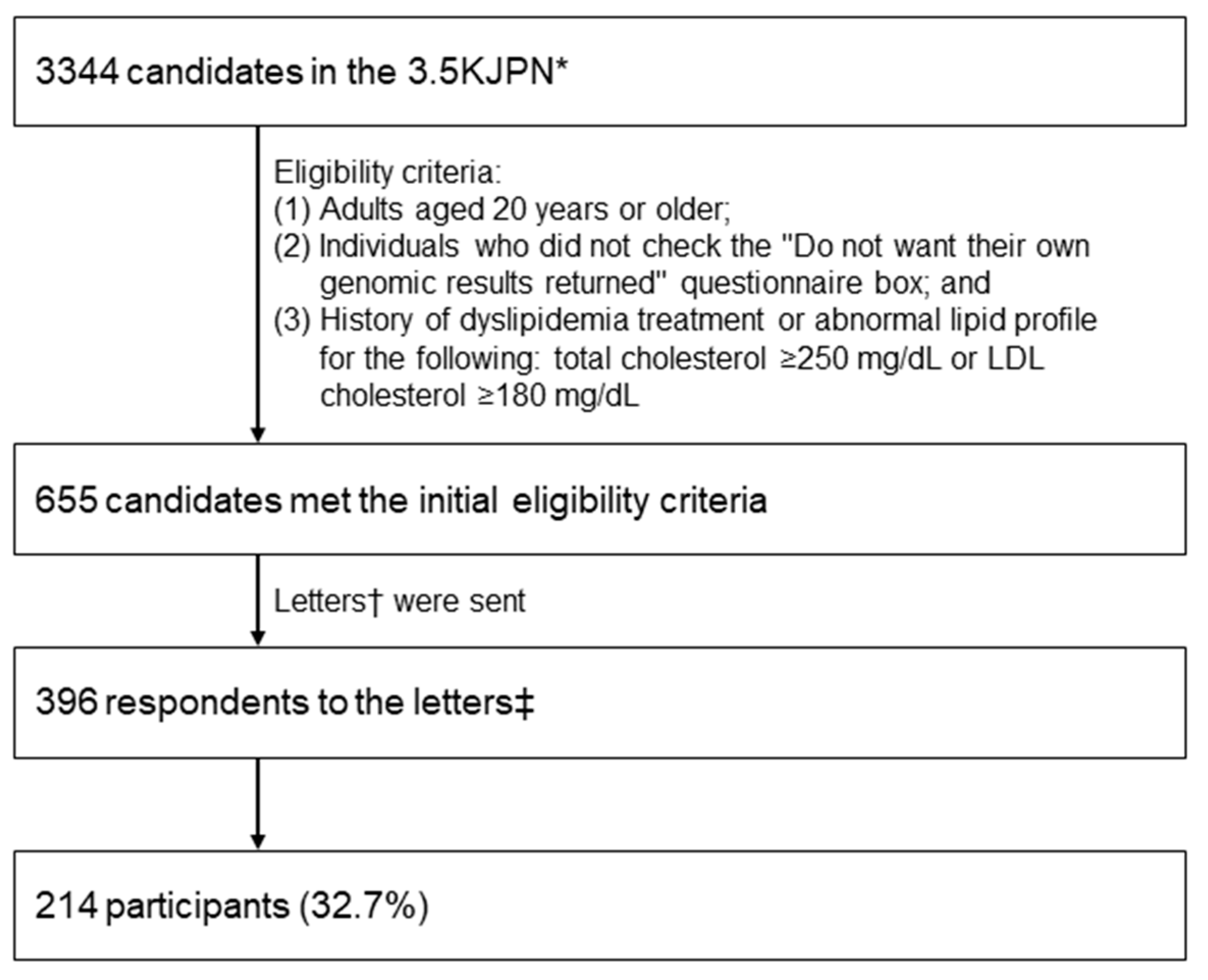
2.1. Study Population and Participant Recruitment
2.2. Questionnaire
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
3.1. Participant Characteristics
3.2. Preferences and Intentions Regarding the FH Genetic Test Results
3.3. Family Health History
3.4. Associations between Participant Characteristics and Preferences/Intentions Regarding the FH Genetic Test Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harada-Shiba, M.; Arai, H.; Ohmura, H.; Okazaki, H.; Sugiyama, D.; Tada, H.; Dobashi, K.; Matsuki, K.; Minamino, T.; Yamashita, S.; et al. Guidelines for the Diagnosis and Treatment of Adult Familial Hypercholesterolemia 2022. J. Atheroscler. Thromb. 2023, 30, CR005. [Google Scholar] [CrossRef]
- Ginsburg, G.S.; Wu, R.R.; Orlando, L.A. Family Health History: Underused for Actionable Risk assessment. Lancet 2019, 394, 596–603. [Google Scholar] [CrossRef]
- Bylstra, Y.; Lim, W.K.; Kam, S.; Tham, K.W.; Wu, R.R.; Teo, J.X.; Davila, S.; Kuan, J.L.; Chan, S.H.; Bertin, N.; et al. Family history assessment significantly enhances delivery of precision medicine in the genomics era. Genome Med. 2021, 13, 3. [Google Scholar] [CrossRef] [PubMed]
- Mars, N.; Lindbohm, J.V.; della Briotta Parolo, P.; Widén, E.; Kaprio, J.; Palotie, A.; Ripatti, S. Systematic comparison of family history and polygenic risk across 24 common diseases. Am. J. Hum. Genet. 2022, 109, 2152–2162. [Google Scholar] [CrossRef] [PubMed]
- Khera, A.V.; Emdin, C.A.; Drake, I.; Natarajan, P.; Bick, A.G.; Cook, N.R.; Chasman, D.I.; Baber, U.; Mehran, R.; Rader, D.J.; et al. Genetic risk, adherence to a healthy lifestyle, and coronary disease. N. Engl. J. Med. 2016, 375, 2349–2358. [Google Scholar] [CrossRef]
- Hunter, J.E.; Riddle, L.; Joseph, G.; Amendola, L.M.; Gilmore, M.J.; Zepp, J.M.; Shuster, E.; Bulkley, J.E.; Muessig, K.R.; Anderson, K.P.; et al. Most people share genetic test results with relatives even if the findings are normal: Family communication in a diverse population. Genet. Med. 2023, 25, 100923. [Google Scholar] [CrossRef]
- Kuriyama, S.; Yaegashi, N.; Nagami, F.; Arai, T.; Kawaguchi, Y.; Osumi, N.; Sakaida, M.; Suzuki, Y.; Nakayama, K.; Hashizume, H.; et al. The Tohoku Medical Megabank Project: Design and mission. J. Epidemiol. 2016, 26, 493–511. [Google Scholar] [CrossRef]
- Yasuda, J.; Katsuoka, F.; Danjoh, I.; Kawai, Y.; Kojima, K.; Nagasaki, M.; Saito, S.; Yamaguchi-Kabata, Y.; Tadaka, S.; Motoike, I.N.; et al. Regional genetic differences among Japanese populations and performance of genotype imputation using whole-genome reference panel of the Tohoku Medical Megabank Project. BMC Genom. 2018, 19, 551. [Google Scholar] [CrossRef]
- Kawame, H.; Fukushima, A.; Fuse, N.; Nagami, F.; Suzuki, Y.; Sakurai-Yageta, M.; Yasuda, J.; Yamaguchi-Kabata, Y.; Kinoshita, K.; Ogishima, S.; et al. The return of individual genomic results to research participants: Design and pilot study of Tohoku Medical Megabank Project. J. Hum. Genet. 2022, 67, 9–17. [Google Scholar] [CrossRef]
- Yamamoto, K.; Hachiya, T.; Fukushima, A.; Nakaya, N.; Okayama, A.; Tanno, K.; Aizawa, F.; Tokutomi, T.; Hozawa, A.; Shimizu, A. Population-based biobank participants’ preferences for receiving genetic test results. J. Hum. Genet. 2017, 62, 1037–1048. [Google Scholar] [CrossRef]
- Tokutomi, T.; Fukushima, A.; Yamamoto, K.; Bansho, Y.; Hachiya, T.; Shimizu, A. f-treeGC: A questionnaire-based family tree-creation software for genetic counseling and genome cohort studies. BMC Med. Genet. 2017, 18, 71. [Google Scholar] [CrossRef] [PubMed]
- Acheson, L.S.; Wang, C.; Zyzanski, S.J.; Lynn, A.; Ruffin, M.T.; Gramling, R.; Rubinstein, W.S.; O’Neill, S.M.; Nease, D.E. Family history and perceptions about risk and prevention for chronic diseases in primary care: A report from the Family HealthwareTM Impact Trial. Genet. Med. 2010, 12, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Henneman, L.; Vermeulen, E.; van El, C.G.; Claassen, L.; Timmermans, D.R.M.; Cornel, M.C. Public attitudes towards genetic testing revisited: Comparing opinions between 2002 and 2010. Eur. J. Hum. Genet. 2013, 21, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Eum, H.; Lee, M.; Yoon, J.; Cho, J.; Lee, E.S.; Choi, K.S.; Lee, S.; Jung, S.-Y.; Lim, M.C.; Kong, S.-Y.; et al. Differences in attitudes toward genetic testing among the public, patients, and health-care professionals in Korea. Eur. J. Hum. Genet. 2018, 26, 1432–1440. [Google Scholar] [CrossRef] [PubMed]
- Cherkas, L.F.; Harris, J.M.; Levinson, E.; Spector, T.D.; Prainsack, B. A Survey of UK Public Interest in Internet-Based Personal Genome Testing. PLoS ONE 2010, 5, e13473. [Google Scholar] [CrossRef] [PubMed]
- Morren, M.; Rijken, M.; Baanders, A.N.; Bensing, J. Perceived Genetic Knowledge, Attitudes towards Genetic Testing, and the Relationship between These among Patients with a Chronic Disease. Patient Educ. Couns. 2007, 65, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Funanage, V.L. Impact of genetic testing on human health: The current landscape and future for personalized medicine. Delaware J. Public Health 2021, 7, 10–11. [Google Scholar] [CrossRef] [PubMed]
- Carrasco-Ramiro, F.; Peiró-Pastor, R.; Aguado, B. Human Genomics Projects and Precision Medicine. Gene Ther. 2017, 24, 551–561. [Google Scholar] [CrossRef]
- Jukarainen, S.; Kiiskinen, T.; Kuitunen, S.; Havulinna, A.S.; Karjalainen, J.; Cordioli, M.; Rämö, J.T.; Mars, N.; Samocha, K.E.; Ollila, H.M.; et al. Genetic risk factors have a substantial impact on healthy life years. Nat. Med. 2022, 28, 1893–1901. [Google Scholar] [CrossRef]
- Ginsburg, G.S.; Phillips, K.A. Precision medicine: From science to value. Health Aff. 2018, 37, 694–701. [Google Scholar] [CrossRef]
- Ginsburg, G.S.; Willard, H.F. Genomic and personalized medicine: Foundations and applications. Transl. Res. 2009, 154, 277–287. [Google Scholar] [CrossRef]
- Weitzel, K.W.; Alexander, M.; Bernhardt, B.A.; Calman, N.; Carey, D.J.; Cavallari, L.H.; Field, J.R.; Hauser, D.; Junkins, H.A.; Levin, P.A.; et al. The IGNITE network: A model for genomic medicine implementation and research. BMC Med. Genom. 2015, 9, 1. [Google Scholar] [CrossRef]
- Bloss, C.S.; Jeste, D.V.; Schork, N.J. Genomics for disease treatment and prevention. Psychiatr. Clin. N. Am. 2011, 34, 147–166. [Google Scholar] [CrossRef] [PubMed]
- Understanding Genetic Risk: How Genetics Shape Your Health. Available online: https://www.hudsonalpha.org/understanding-genetic-risk-how-genetics-shape-your-health/#:~:text=,informed%20decisions%20about%20our%20health.www.hudsonalpha.org/understanding-genetic-risk-how-genetics-shape-your-health/#:~:text=,informed%20decisions%20about%20o (accessed on 5 February 2024).
- MacLeod, R.; Metcalfe, A.; Ferrer-Duch, M. A family systems approach to genetic counseling: Development of narrative interventions. J. Genet. Couns. 2021, 30, 22–29. [Google Scholar] [CrossRef]
- Alver, M.; Palover, M.; Saar, A.; Läll, K.; Zekavat, S.M.; Tõnisson, N.; Leitsalu, L.; Reigo, A.; Nikopensius, T.; Ainla, T.; et al. Recall by genotype and cascade screening for familial hypercholesterolemia in a population-based biobank from Estonia. Genet. Med. 2019, 21, 1173–1180. [Google Scholar] [CrossRef] [PubMed]
- Yanes, T.; Willis, A.M.; Meiser, B.; Tucker, K.M.; Best, M. Psychosocial and behavioral outcomes of genomic testing in cancer: A systematic review. Eur. J. Hum. Genet. 2019, 27, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Heshka, J.T.; Palleschi, C.; Howley, H.; Wilson, B.; Wells, P.S. A systematic review of perceived risks, psychological and behavioral impacts of genetic testing. Genet. Med. 2008, 10, 19–32. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions, and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |

{kind=link}
| n | Proportion | ||
|---|---|---|---|
| Gender | Male | 71 | 33.2% |
| Female | 143 | 66.8% | |
| Age | Median (mean, range), years | 67 | (64.4, 35–90) |
| ≥65 years | 124 | 57.9% | |
| <65 years | 90 | 42.1% | |
| Wished for their familial hypercholesterolemia genetic results to be returned | Yes | 214 | 100.0% |
| No | 0 | 0.0% | |
| Medical history of the participants | Dyslipidemia | 214 | 100.0% |
| Heart disease | 21 | 9.8% | |
| Stroke | 3 | 1.4% | |
| Disclosed their pedigrees and family health histories | Yes | 186 | 86.9% |
| No | 28 | 13.1% | |
| Number of disclosed first-degree relatives | Median (range) | 6 | (2–12) |
| Participants with first-degree relatives with the indicated disease | Dyslipidemia | 95 | 44.4% |
| Heart disease | 66 | 30.8% | |
| Stroke | 58 | 27.1% |
| Preferences and Intentions | Number of Answers (%) | |||||
|---|---|---|---|---|---|---|
| Agree and Somewhat Agree | Disagree, Somewhat Disagree, Neither Agree nor Disagree, and Missing Information | |||||
| If the genetic test result was positive (pathogenic variant detected): | I want to share the result with: | my partner | 180 | 84.1% | 34 | 15.9% |
| my children | 175 | 81.8% | 39 | 18.2% | ||
| my grandchildren | 110 | 51.4% | 104 | 48.6% | ||
| my siblings | 140 | 65.4% | 74 | 34.6% | ||
| my other family members | 80 | 37.4% | 134 | 62.6% | ||
| The result will be useful for managing the health of: | my own health | 210 | 98.1% | 4 | 1.9% | |
| my children’s health | 192 | 89.7% | 22 | 10.3% | ||
| my grandchildren’s health | 151 | 70.6% | 63 | 29.4% | ||
| my parent’s health | 109 | 50.9% | 105 | 49.1% | ||
| my sibling’s health | 150 | 70.1% | 64 | 29.9% | ||
| the health of my other family members | 97 | 45.3% | 117 | 54.7% | ||
| If the genetic test result was negative (no pathogenic variant detected): | I want to share the result with: | my partner | 177 | 82.7% | 37 | 17.3% |
| my children | 175 | 81.8% | 39 | 18.2% | ||
| my grandchildren | 119 | 55.6% | 95 | 44.4% | ||
| my siblings | 136 | 63.6% | 78 | 36.4% | ||
| my other family members | 85 | 39.7% | 129 | 60.3% | ||
| The result will be useful for managing the health of: | my own health | 205 | 95.8% | 9 | 4.2% | |
| my children’s health | 188 | 87.9% | 26 | 12.1% | ||
| my grandchildren’s health | 142 | 66.4% | 72 | 33.6% | ||
| my parent’s health | 106 | 49.5% | 108 | 50.5% | ||
| my sibling’s health | 143 | 66.8% | 71 | 33.2% | ||
| the health of my other family members | 96 | 44.9% | 118 | 55.1% | ||
| Characteristics | Outcomes a | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| If the Genetic Test Result Was Positive (Pathogenic Variant Detected): | If the Genetic Test Result Was Negative (No Pathogenic Variant Detected): | |||||||||
| I Want to Share the Result with: | The Result Will Be Useful for Managing the Health of: | I Want to Share the Result with: | The Result Will Be Useful for Managing the Health of: | |||||||
| My Siblings | My Other Family Members | My Parent’s Health | My Sibling’s Health | My Grandchildren | My Siblings | My Children’s Health | My Parent’s Health | My Sibling’s Health | ||
| Gender b | B (S.E.) | –0.97 (0.44) | ||||||||
| Wald | 4.91 | |||||||||
| p value | 0.0268 * | |||||||||
| OR | 0.38 | |||||||||
| 95% CI | 0.16–0.90 | |||||||||
| Age c | B (S.E.) | –1.03 (0.31) | –0.90 (0.31) | |||||||
| Wald | 10.78 | 8.40 | ||||||||
| p value | 0.0010 † | 0.0038 † | ||||||||
| OR | 0.36 | 0.41 | ||||||||
| 95% CI | 0.19–0.66 | 0.22–0.74 | ||||||||
| Medical history of the participants’ heart disease d | B (S.E.) | |||||||||
| Wald | ||||||||||
| p value | ||||||||||
| OR | ||||||||||
| 95% CI | ||||||||||
| Health history of first-degree relatives’ dyslipidemia d | B (S.E.) | 0.80 (0.31) | 0.49 (0.31) | 0.68 (0.31) | 0.68 (0.33) | 0.89 (0.31) | 0.68 (0.31) | 0.70 (0.32) | ||
| Wald | 6.41 | 2.47 | 4.84 | 4.39 | 8.46 | 5.00 | 4.88 | |||
| p value | 0.0113 * | 0.1157 | 0.0277 * | 0.0361 * | 0.0036 † | 0.0253 * | 0.0271 * | |||
| OR | 2.22 | 1.63 | 1.97 | 1.98 | 2.45 | 1.98 | 2.01 | |||
| 95% CI | 1.20–4.15 | 0.89–3.01 | 1.08–3.62 | 1.05–3.79 | 1.35–4.51 | 1.09–3.63 | 1.09–3.76 | |||
| Health history of first-degree relatives’ heart disease d | B (S.E.) | 0.66 (0.31) | ||||||||
| Wald | 4.40 | |||||||||
| p value | 0.0359 * | |||||||||
| OR | 1.93 | |||||||||
| 95% CI | 1.05–3.62 | |||||||||
| Health history of first-degree relatives’ stroke d | B (S.E.) | 0.59 (0.35) | −0.77 (0.35) | |||||||
| Wald | 2.78 | 4.84 | ||||||||
| p value | 0.0955 | 0.0278 * | ||||||||
| OR | 1.80 | 0.46 | ||||||||
| 95% CI | 0.92–3.65 | 0.23–0.90 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tokutomi, T.; Yoshida, A.; Fukushima, A.; Yamamoto, K.; Ishigaki, Y.; Kawame, H.; Fuse, N.; Nagami, F.; Suzuki, Y.; Sakurai-Yageta, M.; et al. The Health History of First-Degree Relatives’ Dyslipidemia Can Affect Preferences and Intentions following the Return of Genomic Results for Monogenic Familial Hypercholesterolemia. Genes 2024, 15, 384. https://doi.org/10.3390/genes15030384
Tokutomi T, Yoshida A, Fukushima A, Yamamoto K, Ishigaki Y, Kawame H, Fuse N, Nagami F, Suzuki Y, Sakurai-Yageta M, et al. The Health History of First-Degree Relatives’ Dyslipidemia Can Affect Preferences and Intentions following the Return of Genomic Results for Monogenic Familial Hypercholesterolemia. Genes. 2024; 15(3):384. https://doi.org/10.3390/genes15030384
Chicago/Turabian StyleTokutomi, Tomoharu, Akiko Yoshida, Akimune Fukushima, Kayono Yamamoto, Yasushi Ishigaki, Hiroshi Kawame, Nobuo Fuse, Fuji Nagami, Yoichi Suzuki, Mika Sakurai-Yageta, and et al. 2024. "The Health History of First-Degree Relatives’ Dyslipidemia Can Affect Preferences and Intentions following the Return of Genomic Results for Monogenic Familial Hypercholesterolemia" Genes 15, no. 3: 384. https://doi.org/10.3390/genes15030384
APA StyleTokutomi, T., Yoshida, A., Fukushima, A., Yamamoto, K., Ishigaki, Y., Kawame, H., Fuse, N., Nagami, F., Suzuki, Y., Sakurai-Yageta, M., Uruno, A., Suzuki, K., Tanno, K., Ohmomo, H., Shimizu, A., Yamamoto, M., & Sasaki, M. (2024). The Health History of First-Degree Relatives’ Dyslipidemia Can Affect Preferences and Intentions following the Return of Genomic Results for Monogenic Familial Hypercholesterolemia. Genes, 15(3), 384. https://doi.org/10.3390/genes15030384