
Prenatal Diagnosis and Outcomes in Fetuses with Hemivertebra
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
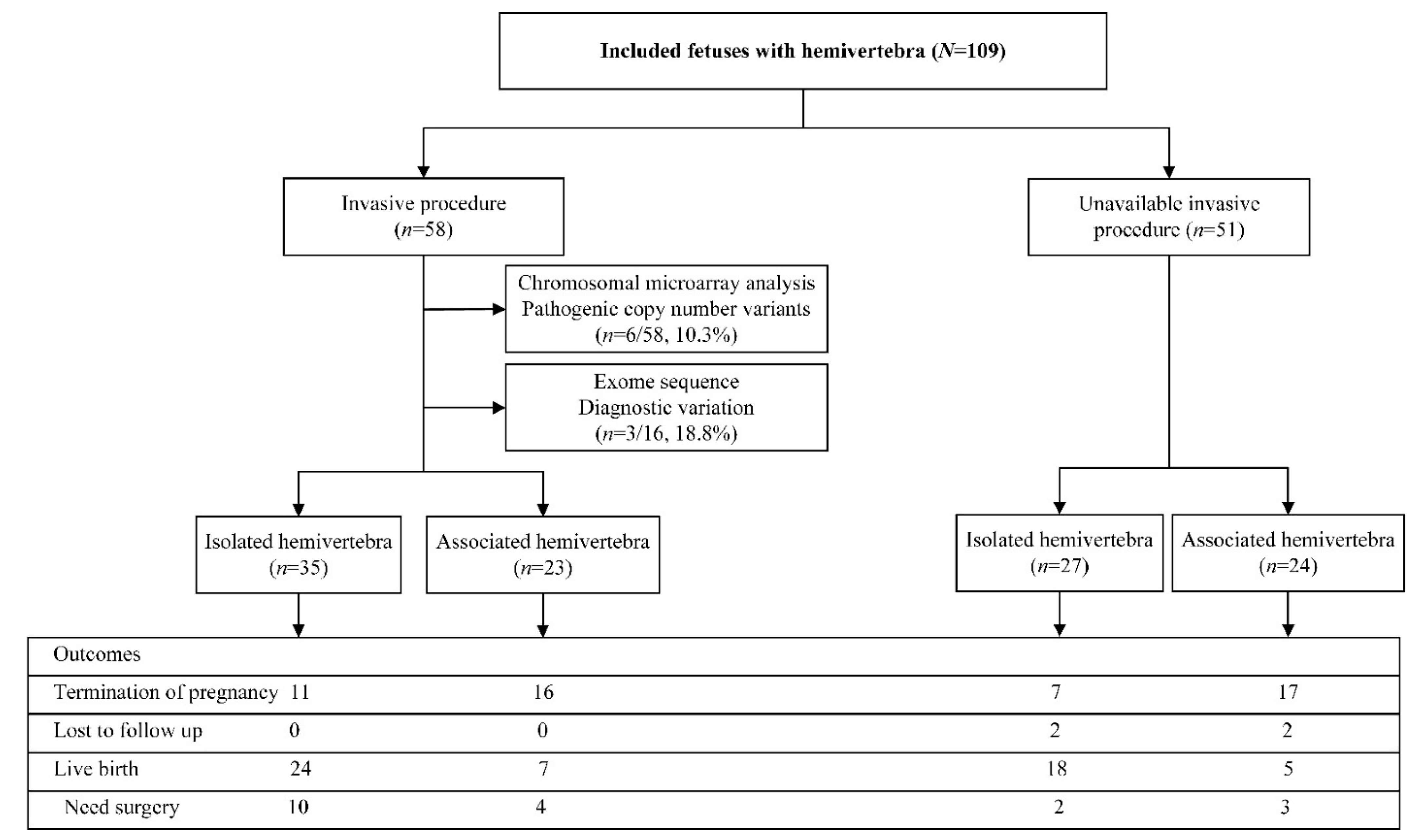
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Basude, S.; McDermott, L.; Newell, S.; Wreyford, B.; Denbow, M.; Hutchinson, J.; Abdel-Fattah, S. Fetal hemivertebra: Associations and perinatal outcome. Ultrasound Obstet. Gynecol. 2015, 45, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Lemire, G.T.; Beauregard-Lacroix, É.; Campeau, P.M.; Parent, S.; Roy-Beaudry, M.; Soglio, D.D.; Grignon, A.; Rypens, F.; Wavrant, S.; Laberge, A.-M.; et al. Retrospective analysis of fetal vertebral defects: Associated anomalies, etiologies, and outcome. Am. J. Med. Genet. Part A 2020, 182, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Zelop, C.M.; Pretorius, D.H.; Benacerraf, B.R. Fetal hemivertebrae: Associated anomalies, significance, and outcome. Obstet. Gynecol. 1993, 81, 412–416. [Google Scholar] [PubMed]
- Johal, J.; Loukas, M.; Fisahn, C.; Chapman, J.R.; Oskouian, R.J.; Tubbs, R.S. Hemivertebrae: A comprehensive review of embryology, imaging, classification, and management. Child’s Nerv. Syst. 2016, 32, 2105–2109. [Google Scholar] [CrossRef]
- Tanaka, T.; Uhthoff, H.K. The Pathogenesis of Congenital Vertebral Malformations: A Study Based on Observations made in 11 Human Embryos and Fetuses. Acta Orthop. Scand. 1981, 52, 413–425. [Google Scholar] [CrossRef]
- Wapner, R.J.; Martin, C.L.; Levy, B.; Ballif, B.C.; Eng, C.M.; Zachary, J.M.; Savage, M.; Platt, L.D.; Saltzman, D.; Grobman, W.A.; et al. Chromosomal Microarray versus Karyotyping for Prenatal Diagnosis. N. Engl. J. Med. 2012, 367, 2175–2184. [Google Scholar] [CrossRef]
- Levy, B.; Wapner, R. Prenatal diagnosis by chromosomal microarray analysis. Fertil. Steril. 2018, 109, 201–212. [Google Scholar] [CrossRef]
- Qi, Q.; Jiang, Y.; Zhou, X.; Meng, H.; Hao, N.; Chang, J.; Bai, J.; Wang, C.; Wang, M.; Guo, J.; et al. Simultaneous Detection of CNVs and SNVs Improves the Diagnostic Yield of Fetuses with Ultrasound Anomalies and Normal Karyotypes. Genes 2020, 11, 1397. [Google Scholar] [CrossRef]
- Petrovski, S.; Aggarwal, V.; Giordano, J.L.; Stosic, M.; Wou, K.; Bier, L.; Spiegel, E.; Brennan, K.; Stong, N.; Jobanputra, V.; et al. Whole-exome sequencing in the evaluation of fetal structural anomalies: A prospective cohort study. Lancet 2019, 393, 758–767. [Google Scholar] [CrossRef]
- Powel, J.E.; Spiliopoulos, M.; Ferreira, C.R.; Rosenthal, E.; Sinkovskaya, E.; Brown, S.; Sham, C.; Jelin, A.C.; Al Kouatly, H.B. 265 Hemivertebra: Systematic review of cases with cytogenetic abnormalities, associated anomalies and proposed prenatal management. Am. J. Obstet. Gynecol. 2021, 224, S175. [Google Scholar] [CrossRef]
- Powel, J.E.; Spiliopoulos, M.; Ferreira, C.R.; Rosenthal, E.; Sinkovskaya, E.; Brown, S.; Sham, C.; Jelin, A.C.; Al Kouatly, H.B. 346 Review of syndromic genetic etiology in patients with hemivertebra and implications in prenatal management. Am. J. Obstet. Gynecol. 2021, 224, S227–S228. [Google Scholar] [CrossRef]
- Zhou, H.; Cheng, K.; Li, Y.; Fu, F.; Li, R.; Zhang, Y.; Yang, X.; Jing, X.; Li, F.; Han, J.; et al. The Genetic and Clinical Outcomes in Fetuses with Isolated Fetal Growth Restriction: A Chinese Single-Center Retrospective Study. Front Genet. 2022, 13, 856522. [Google Scholar] [CrossRef] [PubMed]
- Riggs, E.R.; Andersen, E.F.; Cherry, A.M.; Kantarci, S.; Kearney, H.; Patel, A.; Raca, G.; Ritter, D.I.; South, S.T.; Thorland, E.C.; et al. Technical standards for the interpretation and reporting of constitutional copy-number variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics (ACMG) and the Clinical Genome Resource (ClinGen). Genet. Med. 2020, 22, 245–257, Correction in: Genet. Med. 2021, 23, 2230. [Google Scholar] [CrossRef] [PubMed]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef] [PubMed]
- Pauta, M.; Martinez-Portilla, R.J.; Borrell, A. Diagnostic yield of exome sequencing in fetuses with multisystem malformations: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2022, 59, 715–722. [Google Scholar] [CrossRef]
- Bohiltea, R.E.; Ducu, I.; Mihai, B.M.; Iordache, A.-M.; Dima, V.; Vladareanu, E.M.; Bacalbasa, N.; Bohiltea, A.-T.; Salmen, T.; Varlas, V. First-Trimester Diagnosis of Supernumerary Hemivertebra. Diagnostics 2022, 12, 373. [Google Scholar] [CrossRef]
- Yue, F.; Xi, Q.; Zhang, X.; Jiang, Y.; Zhang, H.; Liu, R. Molecular cytogenetic characterization of 16p11.2 microdeletions with diverse prenatal phenotypes: Four cases report and literature review. Taiwan. J. Obstet. Gynecol. 2022, 61, 544–550. [Google Scholar] [CrossRef]
- Lai, W.; Feng, X.; Yue, M.; Cheung, P.; Choi, V.; Song, Y.-Q.; Luk, K.; Cheung, J.; Gao, B. Identification of Copy Number Variants in a Southern Chinese Cohort of Patients with Congenital Scoliosis. Genes 2021, 12, 1213. [Google Scholar] [CrossRef]
- Lin, S.; Shi, S.; Zhou, Y.; Ji, Y.; Huang, P.; Wu, J.; Chen, B.; Luo, Y. Intrauterine phenotypic features associated with 16p11.2 recurrent microdeletions. Prenat. Diagn. 2018, 38, 381–389. [Google Scholar] [CrossRef]
- White, P.H.; Farkas, D.R.; McFadden, E.E.; Chapman, D.L. Defective somite patterning in mouse embryos with reduced levels of Tbx6. Development 2003, 130, 1681–1690. [Google Scholar] [CrossRef] [Green Version]
- Nikaido, M.; Kawakami, A.; Sawada, A.; Furutani-Seiki, M.; Takeda, H.; Araki, K. Tbx24, encoding a T-box protein, is mutated in the zebrafish somite-segmentation mutant fused somites. Nat. Genet. 2002, 31, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Sparrow, D.B.; McInerney-Leo, A.; Gucev, Z.S.; Gardiner, B.; Marshall, M.; Leo, P.J.; Chapman, D.L.; Tasic, V.; Shishko, A.; Brown, M.A.; et al. Autosomal dominant spondylocostal dysostosis is caused by mutation in TBX6. Hum. Mol. Genet. 2013, 22, 1625–1631. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, M.; Duffourd, Y.; Jouan, T.; Poe, C.; Jean-Marçais, N.; Verloes, A.; St-Onge, J.; Riviere, J.-B.; Petit, F.; Pierquin, G.; et al. Autosomal recessive variations of TBX6, from congenital scoliosis to spondylocostal dysostosis. Clin. Genet. 2016, 91, 908–912. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.; Yang, N.; Wu, N.; Xu, X.; Chen, W.; Zhang, L.; Li, Y.; Du, R.-Q.; Dong, S.; Zhao, S.; et al. Increased TBX6 gene dosages induce congenital cervical vertebral malformations in humans and mice. J. Med. Genet. 2020, 57, 371–379. [Google Scholar] [CrossRef]
- Wu, N.; Ming, X.; Xiao, J.; Wu, Z.; Chen, X.; Shinawi, M.; Shen, Y.; Yu, G.; Liu, J.; Xie, H.; et al. TBX6 Null Variants and a Common Hypomorphic Allele in Congenital Scoliosis. N. Engl. J. Med. 2015, 372, 341–350. [Google Scholar] [CrossRef]
- The 1000 Genomes Project Consortium. An integrated map of genetic variation from 1092 human genomes. Nature 2012, 491, 56–65. [Google Scholar] [CrossRef]
- Lord, J.; McMullan, D.J.; Eberhardt, R.Y.; Rinck, G.; Hamilton, S.J.; Quinlan-Jones, E.; Prigmore, E.; Keelagher, R.; Best, S.K.; Carey, G.K.; et al. Prenatal exome sequencing analysis in fetal structural anomalies detected by ultrasonography (PAGE): A cohort study. Lancet 2019, 393, 747–757. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | Isolated HV (%, n/N) | Non-Isolated HV (%, n/N) | p-Value |
| Diagnostic rate of CMA | 11.4, 4/35 | 8.7, 2/23 | 1.000 |
| Diagnostic rate of WES | 11.1, 1/9 | 28.6, 2/7 | 0.550 |
| Live birth rate | 67.7, 42/62 | 12.5, 12/47 | <0.001 |
| Operation rate | 28.6, 12/42 | 58.3, 7/12 | 0.087 |
| Associated Anomalies | Number |
|---|---|
| Skeletal system | 13 (19.1%) |
| Butterfly vertebra | 5 |
| Talipes equinovarus | 2 |
| Short long bone | 2 |
| Ectrodactyly | 1 |
| Congenital club hand | 1 |
| Partial absence of 7th ribs | 1 |
| Preaxial polydactyly | 1 |
| Genitourinary system | 13 (19.1%) |
| Renal agenesis or hypoplasia | 5 |
| Polycystic kidney dysplasia | 2 |
| Unilateral hydronephrosis with or without ureter ectasis | 4 |
| Hypospadias | 1 |
| Renal duplication | 1 |
| Cardiovascular system | 11 (16.2%) |
| Ventricular septal defect | 3 |
| Hypoplastic heart | 1 |
| Pulmonary atresia | 1 |
| Tetralogy of Fallot | 1 |
| Aortic stenosis | 1 |
| Coarctation of aorta | 1 |
| Cardiac Malposition | 1 |
| Complete atrioventricular septal defect | 1 |
| Complete transposition of great artery | 1 |
| Central nervous system | 7 (10.3%) |
| Spina bifida with or without meningocele | 5 |
| Microcephaly | 2 |
| Craniofacial | 6 (8.8%) |
| Cleft lip and/or palate | 5 |
| Anterior nasal excrescence | 1 |
| Gastrointestinal system | 4 (5.9%) |
| Small stomach | 2 |
| Congenital megacolon | 1 |
| Esophageal atresia with tracheoesophageal fissure | 1 |
| Others | 14 (20.6%) |
| Polyhydramnios | 8 |
| Fetal growth restriction | 3 |
| Oligohydramnios | 2 |
| Pleural effusion | 1 |
| Patient | MA | GA at the Suspicion of Hemivertebra | Affected Vertebra | Associated Anomaly | Microarray Result | Length | Type | Classification |
|---|---|---|---|---|---|---|---|---|
| 1 | 31.0 | 25 + 6 | L1 | Pulmonary atresia | arr [hg19] 8q24.3 (140131302_ 146295771) X3 arr [hg19] 21q22.2q22.3 (39737188_ 48093361) X1 | 6.16 Mb 8.36 Mb | Duplication Deletion | P P |
| 2 | 29.0 | 21 + 1 | T10, T12, L2, L3 | / | arr [hg19] (15)X2 hmz | / | UPD 15 | P |
| 3 | 33.0 | 23 + 2 | L3, S1, S2 | Renal dysplasia, ventricular septal defect, pulmonary atresia, right aortic arch, persistent left superior vena cava, and sacrococcygeal dysplasia | arr [hg19] (21) X2~3 | 33.08 Mb | Mosaic | P |
| 4 | 33.5 | 26 + 1 | T11 | / | arr [hg19] 17p11.2 (16657319_20417235) X1 | 3.76 Mb | Deletion | P |
| 5 | 30.0 | 22 + 3 | T11 | / | arr [hg19] 16p11.2 (29428531_30190029) X1 | 761 Kb | Deletion | P |
| 6 | 23.0 | 24 + 1 | L1 | / | arr [hg19] 16p11.2 (29567295_30240227) X1 | 611 kb | Deletion | P |
| 7 | 25.0 | 25 + 0 | T6 | / | arr [hg19] 15q13.2q13.3 (31104221_32915723) X3 | 1.81 Mb | Duplication | VUS |
| 8 | 29.0 | 25 + 0 | C7 | Spina bifida, renal agenesis | arr [hg19] 6p22.3 (21730212-21957713) X1 | 228 Kb | Deletion | VUS |
| 9 | 28.0 | 27 + 2 | L3 | left renal hypoplasia, right hydronephrosis, oligohydramnios | arr [hg19] 2q37.3 (238143761_238617753) X3 | 474 Kb | Duplication | VUS |
| 10 | 31.4 | 26 + 3 | T3, T8 | / | arr [hg19] 5q31.1 (135273369_135477266) X3 | 204 Kb | Duplication | VUS |
| 11 | 24.2 | 27 + 5 | L5 | / | arr [hg19] 6q23.3q24.1 (138266085_139126324) X3 | 806 Kb | Duplication | VUS |
| Patient | Ultrasound Findings | Gene | Transcripts | Variant | Origin | Inheritance | Classification | Zygosity | Condition |
|---|---|---|---|---|---|---|---|---|---|
| 12 | Multiple HV | DLL3 | NM_203486.3 | c.1250G > T (p. Cys417Phe) | Pat | AR | LP | Het | Chondrodysplasia punctata, X-linked dominant |
| c.1277G > A (p. Cys426Tyr) | Mat | AR | LP | Het | |||||
| 13 | Multiple HV, short long bone | EBP | NM_006579.2 | c.328C > T (p. Arg110Ter) | De novo | AD | P | Het | Spondylocostal dysostosis 1, autosomal recessive |
| 14 | Multiple HV, spinal bifida | FLNB | NM_001164317.1 | c.7213C > A ** (p. Arg2405Ser) | De novo | AD | LP | Het | Larsen syndrome |
| 15 | L1 HV | PTCH1 | NM_000264.3 | c.2687C > T p. (Pro896Leu) | Mat | AD | VUS | Het | Basal cell nevus syndrome |
| 16 | L3 HV | ERCC6 | NM_000124.3 | c.3061A > G p. (Ile1021Val) | Pat | AR | VUS | Het | Cockayne syndrome B |
| 17 | L1 HV | RBM10 | NM_001204468.1 | c.1980 + 7G > C | Mat | XR | VUS | Hemi | TARP syndrome |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, H.; Wang, Y.; Huang, R.; Fu, F.; Li, R.; Cheng, K.; Wang, D.; Yu, Q.; Zhang, Y.; Jing, X.; et al. Prenatal Diagnosis and Outcomes in Fetuses with Hemivertebra. Genes 2022, 13, 1623. https://doi.org/10.3390/genes13091623
Zhou H, Wang Y, Huang R, Fu F, Li R, Cheng K, Wang D, Yu Q, Zhang Y, Jing X, et al. Prenatal Diagnosis and Outcomes in Fetuses with Hemivertebra. Genes. 2022; 13(9):1623. https://doi.org/10.3390/genes13091623
Chicago/Turabian StyleZhou, Hang, You Wang, Ruibin Huang, Fang Fu, Ru Li, Ken Cheng, Dan Wang, Qiuxia Yu, Yongling Zhang, Xiangyi Jing, and et al. 2022. "Prenatal Diagnosis and Outcomes in Fetuses with Hemivertebra" Genes 13, no. 9: 1623. https://doi.org/10.3390/genes13091623
APA StyleZhou, H., Wang, Y., Huang, R., Fu, F., Li, R., Cheng, K., Wang, D., Yu, Q., Zhang, Y., Jing, X., Lei, T., Han, J., Yang, X., Li, D., & Liao, C. (2022). Prenatal Diagnosis and Outcomes in Fetuses with Hemivertebra. Genes, 13(9), 1623. https://doi.org/10.3390/genes13091623