
A Review of Biomaterials and Associated Performance Metrics Analysis in Pre-Clinical Finite Element Model and in Implementation Stages for Total Hip Implant System

 ,
,  ,
,  , , , ,
, , , ,  , and
, and
Abstract
1. Introduction
2. Biomaterials for Total Hip Implant System
2.1. Important Parameters for Hip Implant Materials
2.1.1. Young’s Modulus
2.1.2. Fatigue Crack
2.1.3. Stress Shielding
2.1.4. Wear Behavior
2.2. Material Used in Total Hip Implant System
2.2.1. Metallic Alloys
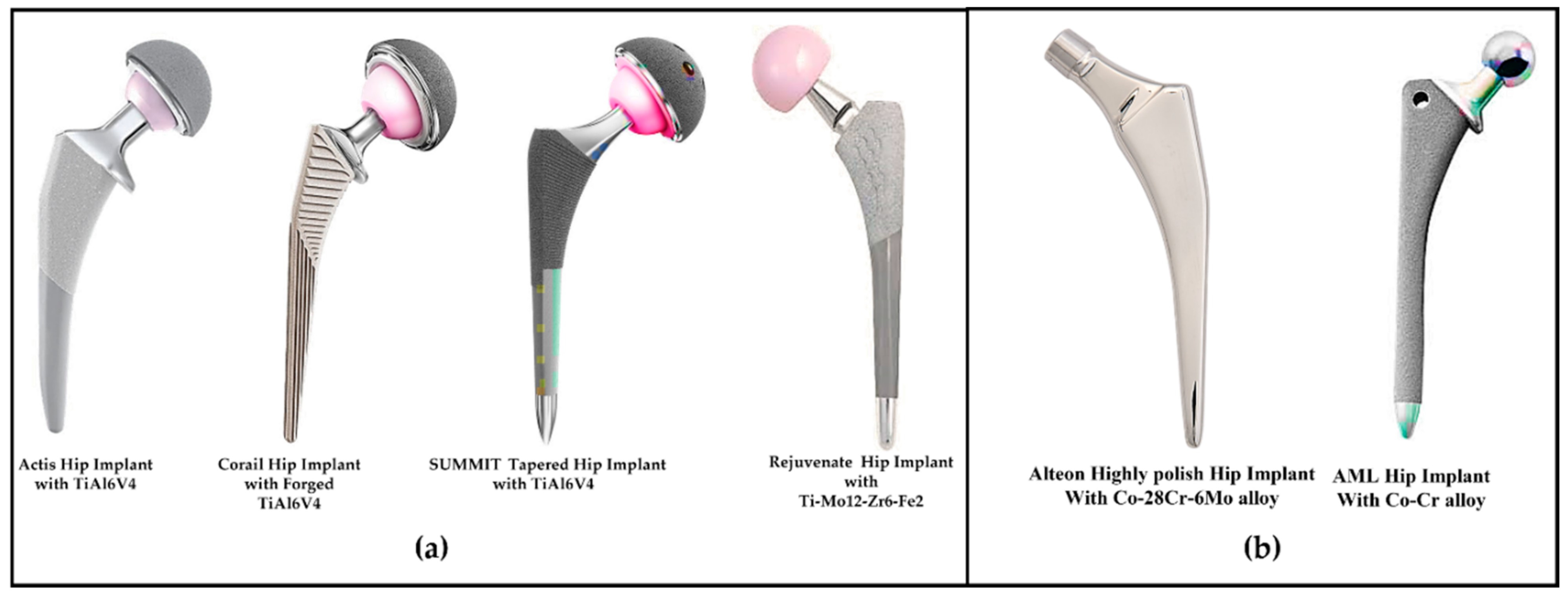
2.2.2. Titanium Alloys
2.2.3. Cobalt Alloys
2.2.4. Ceramics Alloys
2.2.5. Polymer
2.2.6. Polyether-Ether-Ketone and Hydroxyapatite
3. Performance Study of Hip Implant with Different Biomaterials in Pre-Clinical Stage
3.1. Micromotion
3.2. Wear Estimation
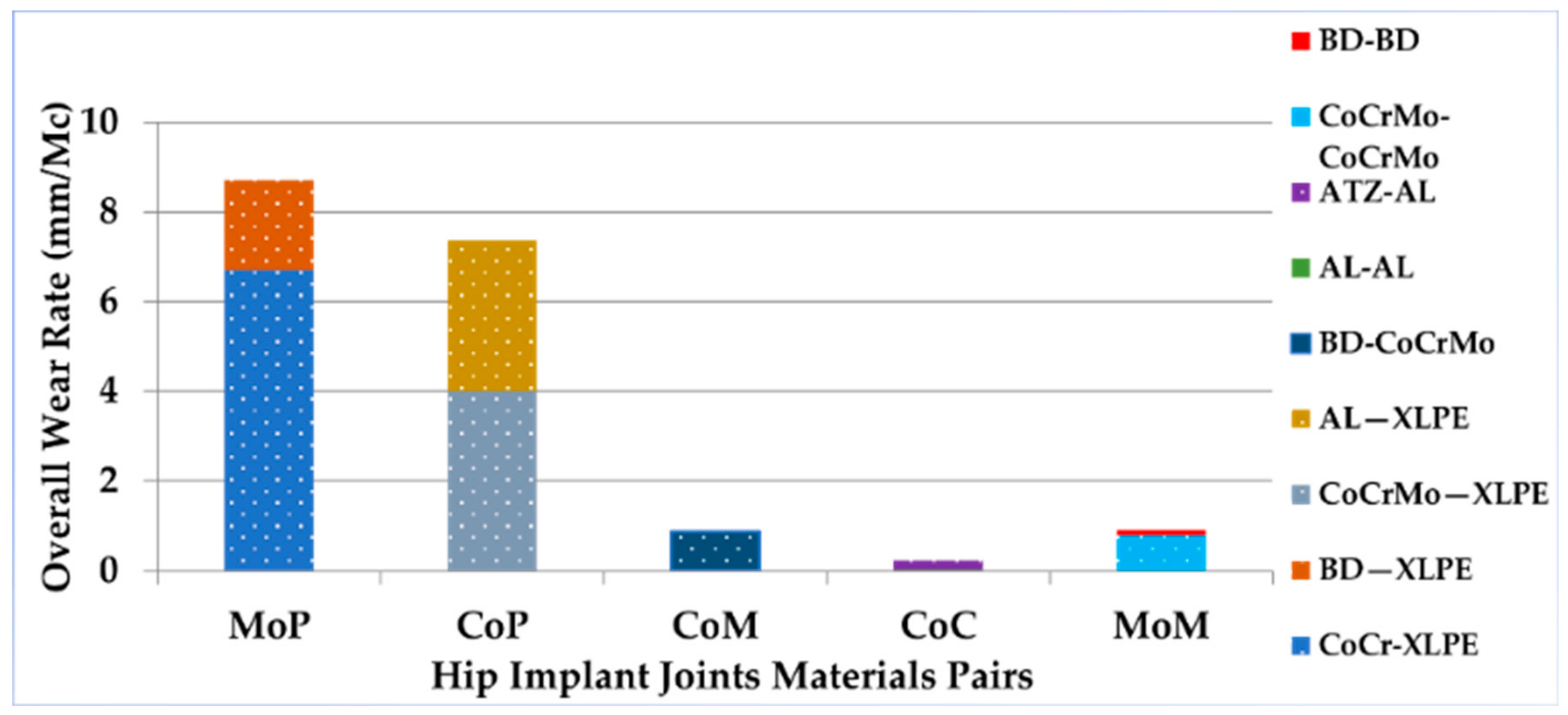
3.2.1. Wear Rate for Different Hip Implant Biomaterials
3.2.2. Taper-Head Junction
3.2.3. Acetabular Head–Liner Junction
3.3. Fatigue Behavior Analysis
3.3.1. Fatigue Life Estimation for Fully Reversed Loading Conditions
3.3.2. Fatigue Life Estimation Using Non-Fully Reversed Loading Conditions
3.3.3. Fatigue Life Estimation for Different Biomaterials
4. Biocompatibility and Tissue Response for Different Biomaterials in, In Vitro, In Vivo, and Clinical Stage Studies
4.1. In Vitro and In Vivo Studies
4.2. Clinical Stage
4.2.1. Impact of Bone Remodeling and Coating of the Hip Implant with Different Biomaterials
4.2.2. Impact of Wear Debris on the Hip Implant System
4.2.3. Taper Junction and Acetabular Head–Liner Junction
4.2.4. Adverse Tissue Response to Wear Debris and Ions
5. Major Factors of THI with Different Biomaterials and Forthcoming Research Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bottai, V.; Dell’Osso, G.; Celli, F.; Bugelli, G.; Cazzella, N.; Cei, E.; Guido, G.; Giannotti, S. Total hip replacement in osteoarthritis: The role of bone metabolism and its complications. Clin. Cases Miner. Bone Metab. 2015, 12, 247–250. [Google Scholar] [CrossRef] [PubMed]
- Oh, E.S.; Sieber, F.E.; Leoutsakos, J.-M.; Inouye, S.K.; Lee, H.B. Sex Differences in Hip Fracture Surgery: Preoperative Risk Factors for Delirium and Postoperative Outcomes. J. Am. Geriatr. Soc. 2016, 64, 1616–1621. [Google Scholar] [CrossRef] [PubMed]
- Colic, K.; Sedmak, A. The current approach to research and design of the artificial hip prosthesis: A review. Rheumatol. Orthop. Med. 2016, 1, 1–7. [Google Scholar] [CrossRef]
- Nasiri, M.; Luo, Y. Study of sex differences in the association between hip fracture risk and body parameters by DXA-based biomechanical modeling. Bone 2016, 90, 90–98. [Google Scholar] [CrossRef]
- Buddy Ratner, A.H.; Schoen, F.; Lemons, L. Biomaterials Science—An Introduction to Materials in Medicine; Elsevier: Amsterdam, The Netherlands, 2004; Available online: https://www.elsevier.com/books/biomaterials-science/ratner/978-0-08-047036-8 (accessed on 26 March 2022).
- Munemoto, M.; Grammatopoulos, G.; Tanaka, Y.; Gibbons, M.; Athanasou, N.A. The pathology of failed McKee-Farrar implants: Correlation with modern metal-on-metal-implant failure. J. Mater. Sci. Mater. Med. 2017, 28, 66. [Google Scholar] [CrossRef]
- American Joint Replacement Registry. The Results of the 2020 American Joint Replacement Registry. Proliance. 2020. Available online: https://www.prolianceorthopedicassociates.com/dr-barrett-blog/the-results-of-the-2020-american-joint-replacement-registry (accessed on 26 March 2022).
- Şensoy, A.T.; Çolak, M.; Kaymaz, I.; Findik, F. Optimal Material Selection for Total Hip Implant: A Finite Element Case Study. Arab. J. Sci. Eng. 2019, 44, 10293–10301. [Google Scholar] [CrossRef]
- Feyzi, M.; Fallahnezhad, K.; Taylor, M.; Hashemi, R. The mechanics of head-neck taper junctions: What do we know from finite element analysis. J. Mech. Behav. Biomed. Mater. 2021, 116, 104338. [Google Scholar] [CrossRef] [PubMed]
- Feyzi, M.; Fallahnezhad, K.; Taylor, M.; Hashemi, R. A review on the finite element simulation of fretting wear and corrosion in the taper junction of hip replacement implants. Comput. Biol. Med. 2021, 130, 104196. [Google Scholar] [CrossRef] [PubMed]
- Senalp, A.Z.; Kayabasi, O.; Kurtaran, H. Static, dynamic and fatigue behavior of newly designed stem shapes for hip prosthesis using finite element analysis. Mater. Des. 2007, 28, 1577–1583. [Google Scholar] [CrossRef]
- Wu, J.S.-S.; Hung, J.-P.; Shu, C.-S.; Chen, J.-H. The computer simulation of wear behavior appearing in total hip prosthesis. Comput. Methods Programs Biomed. 2002, 70, 81–91. [Google Scholar] [CrossRef]
- Chethan, K.; Zuber, M.; Bhat, S.; Shenoy, S.B. Comparative Study of Femur Bone Having Different Boundary Conditions and Bone Structure Using Finite Element Method. Open Biomed. Eng. J. 2018, 12, 115–134. [Google Scholar] [CrossRef]
- Ulrich, S.D.; Seyler, T.M.; Bennett, D.; Delanois, R.E.; Saleh, K.J.; Thongtrangan, I.; Kuskowski, M.; Cheng, E.Y.; Sharkey, P.F.; Parvizi, J.; et al. Total hip arthroplasties: What are the reasons for revision? Int. Orthop. 2008, 32, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Willert, H.-G.; Semlitsch, M. Reactions of the articular capsule to wear products of artificial joint prostheses. J. Biomed. Mater. Res. 1977, 11, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Merola, M.; Affatato, S. Materials for Hip Prostheses: A Review of Wear and Loading Considerations. Materials 2019, 12, 495. [Google Scholar] [CrossRef]
- Choroszyński, M.R.; Skrzypek, S.J. Biomaterials for hip implants—Important considerations relating to the choice of materials. Bio-Algorithms Med-Syst. 2017, 13, 133–145. [Google Scholar] [CrossRef]
- Mehboob, H.; Tarlochan, F.; Mehboob, A.; Chang, S.-H.; Ramesh, S.; Harun, W.S.W.; Kadirgama, K. A novel design, analysis and 3D printing of Ti-6Al-4V alloy bio-inspired porous femoral stem. J. Mater. Sci. Mater. Med. 2020, 31, 78. [Google Scholar] [CrossRef]
- Dalli, D. Development of a Low-Wearing Novel Hip Joint Prosthesis with a Longer Lifespan. Ph.D. Thesis, Faculty of Engineering, University of Malta, Msida, Malta, 2021. [Google Scholar]
- N, C.K.; Ogulcan, G.; N, S.B.; Zuber, M.; B, S.S. Wear estimation of trapezoidal and circular shaped hip implants along with varying taper trunnion radiuses using finite element method. Comput. Methods Programs Biomed. 2020, 196, 105597. [Google Scholar] [CrossRef]
- Hip Replacement Products|Zimmer Biomet. Zimmer Biomet. Available online: https://www.zimmerbiomet.com/en/products-and-solutions/specialties/hip.html#two (accessed on 26 March 2022).
- Matthew, J.; Donachie, J. Titanium: A Technical Guide, 2nd ed.; ASM International: Almere, The Netherlands, 2000. [Google Scholar]
- Kaivosoja, E.; Tiainen, V.-M.; Takakubo, Y.; Rajchel, B.; Sobiecki, J.; Konttinen, Y.; Takagi, M. Materials Used for Hip and Knee Implants; Elsevier: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Singh, S.K.; Tandon, P. Heterogeneous modeling based prosthesis design with porosity and material variation. J. Mech. Behav. Biomed. Mater. 2018, 87, 124–131. [Google Scholar] [CrossRef]
- Darwich, A.; Nazha, H.; Daoud, M. Effect of Coating Materials on the Fatigue Behavior of Hip Implants: A Three-dimensional Finite Element Analysis. J. Appl. Comput. Mech. 2020, 6, 284–295. [Google Scholar] [CrossRef]
- Mohammed, M.T.; Khan, Z.A.; Siddiquee, A.N. Beta Titanium Alloys: The Lowest Elastic Modulus for Biomedical Applications: A Review. Int. J. Chem. Mol. Nucl. Mater. Metall. Eng. 2014, 8, 822–827. [Google Scholar]
- Wang, X.; Xu, S.; Zhou, S. Topological design and additive manufacturing of porous metals for bone scaffolds and orthopaedic implants: A review. Biomaterials 2016, 83, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Gill, P.; Munroe, N.; Pulletikurthi, C.; Pandya, S.; Haider, W. Effect of Manufacturing Process on the Biocompatibility and Mechanical Properties of Ti-30Ta Alloy. J. Mater. Eng. Perform. 2011, 20, 819–823. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bertrand, E.; Gloriant, T.; Gordin, D.M.; Vasilescu, C.; Drob, P.; Drob, S. Synthesis and characterisation of a new superelastic Ti–25Ta–25Nb biomedical alloy. J. Mech. Behav. Biomed. Mater. 2010, 3, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.L.; Li, S.J.; Sun, S.Y.; Yang, R. Effect of Zr and Sn on Young’s modulus and superelasticity of Ti-Nb-based alloys. Mater. Sci. Eng. 2006, 441, 112–118. [Google Scholar] [CrossRef]
- Yilmazer, M.N.H.; Akahori, T.; Nakai, M.; Tsutsumi, H. Effects of severe plastic deformation and thermomechanical treatments on microstructures and mechanical properties of β-type titanium alloys for biomedical applications. In Proceedings of the 13th Conference on Processing and Fabrication of Advanced Materials, Sendai, Japan, 12–14 December 2009; pp. 1401–1410. [Google Scholar]
- Niinomi, M.; Nakai, M. Titanium-Based Biomaterials for Preventing Stress Shielding between Implant Devices and Bone. Int. J. Biomater. 2011, 2011, 8365871. [Google Scholar] [CrossRef]
- DePuy Synthes—Hip Replacement Prosthesis & Femoral Stems. Available online: https://www.jnjmedtech.com/en-US/specialty/hip-replacement-prosthesis-femoral-stems (accessed on 26 March 2022).
- Stryker—Hip Implants. Available online: https://www.stryker.com/us/en/portfolios/orthopaedics/joint-replacement/hip.html (accessed on 26 March 2022).
- Fokter, S.; Levasic, V.; Kovac, S. The innovation trap: Modular neck in total hip arthroplasty. Zdr. Vestn. 2017, 86, 115–126. [Google Scholar]
- Hanawa, T. Overview of Metals and Applications; Woodhead Publishing Limited: Sawston, UK, 2010; pp. 3–24. [Google Scholar]
- Park, J.B. Biomaterials Science and Engineering; Springer: Boston, MA, USA, 1984. [Google Scholar]
- Latitud Femoral Head for Total Hip Replacement. Meril Orthopedics. Available online: https://www.merillife.com/medical-devices/orthopedics/total-hip-replacement/latitud-femoral-head (accessed on 22 July 2022).
- Ben-Nissan, S.C.B.; Choi, A.H. Bioceramics.; Elsevier Inc.: Amsterdam, The Netherlands, 2019; p. 14. [Google Scholar]
- Willmann, G. Ceramics for Total Hip Replacement—What a Surgeon Should Know. Orthopedics 1998, 21, 173–177. [Google Scholar] [CrossRef]
- Piconi, C.; Porporati, A.A. Bioinert Ceramics: Zirconia and Alumina. In Handbook of Bioceramics and Biocomposites; Antoniac, I.V., Ed.; Springer International Publishing: Cham, Switzerland, 2016; pp. 59–89. [Google Scholar]
- Hamadouche, M.; Meunier, A.; Nizard, R.; Hannouche, D.; Bizot, P.; Sedel, L. Alumina-on-Alumina Articulation in Total Hip Arthroplasty: From Bench-side to Bedside. Semin. Arthroplast. 2006, 17, 125–133. [Google Scholar] [CrossRef]
- Cooper, J.R.; Dowson, D.; Fisher, J.; Jobbins, B. Ceramic bearing surfaces in total artificial joints: Resistance to third body wear damage from bone cement particles. J. Med. Eng. Technol. 1991, 15, 63–67. [Google Scholar] [CrossRef]
- Davidson, J.; Poggie, R.; Mishra, A. Abrasive Wear of Ceramic, Metal, and UHMWPE Bearing Surfaces from Third-Body Bone, PMMA Bone Cement, and Titanium Debris. Bio-Medical Mater. Eng. 1994, 4, 213–229. [Google Scholar] [CrossRef]
- Implant Material. CeramTec, The Ceramic Experts. Available online: https://www.ceramtec-medical.com/en/biolox/implant-material (accessed on 26 March 2022).
- BIOLOX®forte. Ceram Tech. Available online: https://www.ceramtec-medical.com/en/biolox/implant-material (accessed on 22 July 2022).
- Hannouche, D.; Nich, C.; Bizot, P.; Meunier, A.; Nizard, R.; Sedel, L. Fractures of Ceramic Bearings. Clin. Orthop. Relat. Res. 2003, 417, 19–26. [Google Scholar] [CrossRef]
- Hannink, R.H.J.; Kelly, P.M.; Muddle, B.C. Transformation Toughening in Zirconia-Containing Ceramics. J. Am. Ceram. Soc. 2004, 83, 461–487. [Google Scholar] [CrossRef]
- Evans, A.G.; Heuer, A.H. REVIEW-Transformation Toughening in Ceramics: Martensitic Transformations in Crack-Tip Stress Fields. J. Am. Ceram. Soc. 1980, 63, 241–248. [Google Scholar] [CrossRef]
- Klee, M. Concise encyclopedia of advanced ceramic materials. Edited by R. J. Brook, Pergamon, Oxford 1991, 588 pp., hardcover, £ 110, ISBN 0-08-034720-78. Adv. Mater. 1992, 4, 826–827. [Google Scholar] [CrossRef]
- Gadow, R.; Kern, F. Novel Zirconia-Alumina Nanocomposites Combining High Strength and Toughness. Adv. Eng. Mater. 2010, 12, 1220–1223. [Google Scholar] [CrossRef]
- Sobieraj, M.C.; Rimnac, C.M. Ultra high molecular weight polyethylene: Mechanics, morphology, and clinical behavior. J. Mech. Behav. Biomed. Mater. 2009, 2, 433–443. [Google Scholar] [CrossRef]
- ISO 11542-1:2001; Plastics—Ultra-High-Molecular-Weight Polyethylene (PE-UHMW) Moulding and Extrusion Materials—Part 1: Designation System and Basis for Specifications. ISO: Geneva, Switzerland, 2001. Available online: https://www.iso.org/standard/30102.html (accessed on 30 August 2022).
- Wang, A.; Dumbleton, J.H. Ultra-High-Molecular-Weight Polyethylene (UHMWPE) as a Bearing Material in Hip Joint Replacements. In Encyclopedia of Tribology; Wang, Q.J., Chung, Y.-W., Eds.; Springer US: Boston, MA, USA, 2013; pp. 3933–3939. [Google Scholar]
- Collins, M.N.; Barron, D.; Birkinshaw, C. Ultra High Molecular Weight Polyethylene (UHMWPE) for Orthopaedic Devices: Structure/Property Relationships. In Polyethylene-Based Blends, Composites and Nanocomposites; Wiley: Hoboken, NJ, USA, 2015; pp. 21–39. [Google Scholar]
- Stephen, M.R.; Burnett, J. FRCSC, Dipl ABOS. Total Hip Arthroplasty: Techniques and Results. BC Med. J. 2010, 52, 455–464. Available online: https://bcmj.org/articles/total-hip-arthroplasty-techniques-and-results (accessed on 30 August 2022).
- Oral, E.; Ghali, B.W.; Muratoglu, O.K. The elimination of free radicals in irradiated UHMWPEs with and without vitamin E stabilization by annealing under pressure. J. Biomed. Mater. Res. Part B Appl. Biomater. 2011, 97B, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Oral, E.; Rowell, S.L.; Muratoglu, O.K. The effect of α-tocopherol on the oxidation and free radical decay in irradiated UHMWPE. Biomaterials 2006, 27, 5580–5587. [Google Scholar] [CrossRef] [PubMed]
- Oral, E.; Wannomae, K.K.; Hawkins, N.; Harris, W.H.; Muratoglu, O.K. α-Tocopherol-doped irradiated UHMWPE for high fatigue resistance and low wear. Biomaterials 2004, 25, 5515–5522. [Google Scholar] [CrossRef]
- Bracco, P.; Kurtz, S.; Costa, L. Vitamin-E-Blended UHMWPE Biomaterials. In UHMWPE Biomaterials Handbook, 2nd ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2009; Volume 16, pp. 237–247. [Google Scholar]
- otal Hip System. KYOCERA Corporation. Available online: https://global.kyocera.com/prdct/medical/initia.html (accessed on 23 July 2022).
- Stratton-Powell, A.A.; Pasko, K.M.; Brockett, C.L.; Tipper, J.L. The Biologic Response to Polyetheretherketone (PEEK) Wear Particles in Total Joint Replacement: A Systematic Review. Clin. Orthop. Relat. Res. 2016, 474, 2394–2404. [Google Scholar] [CrossRef]
- Godara, A.; Raabe, D.; Green, S. The influence of sterilization processes on the micromechanical properties of carbon fiber-reinforced PEEK composites for bone implant applications. Acta Biomater. 2007, 3, 209–220. [Google Scholar] [CrossRef]
- Wang, A.; Lin, R.; Polineni, V.; Essner, A.; Stark, C.; Dumbleton, J. Carbon fiber reinforced polyether ether ketone composite as a bearing surface for total hip replacement. Tribol. Int. 1998, 31, 661–667. [Google Scholar] [CrossRef]
- Ma, R.; Guo, D. Evaluating the bioactivity of a hydroxyapatite-incorporated polyetheretherketone biocomposite. J. Orthop. Surg. Res. 2019, 14, 32. [Google Scholar] [CrossRef]
- Trindade, R.; Albrektsson, T.; Galli, S.; Prgomet, Z.; Tengvall, P.; Wennerberg, A. Bone Immune Response to Materials, Part II: Copper and Polyetheretherketone (PEEK) Compared to Titanium at 10 and 28 Days in Rabbit Tibia. J. Clin. Med. 2019, 8, 814. [Google Scholar] [CrossRef]
- Ma, H.; Suonan, A.; Zhou, J.; Yuan, Q.; Liu, L.; Zhao, X.; Lou, X.; Yang, C.; Li, D.; Zhang, Y.-G. PEEK (Polyether-ether-ketone) and its composite materials in orthopedic implantation. Arab. J. Chem. 2021, 14, 102977. [Google Scholar] [CrossRef]
- Hydroxyapatite (HAp). FLUIDINOVA. Available online: https://www.fluidinova.com/hydroxyapatite-properties-uses-and-applications (accessed on 2 August 2022).
- Grupp, T.M.; Utzschneider, S.; Schröder, C.; Schwiesau, J.; Fritz, B.; Maas, A.; Blömer, W.; Jansson, V. Biotribology of alternative bearing materials for unicompartmental knee arthroplasty. Acta Biomater. 2010, 6, 3601–3610. [Google Scholar] [CrossRef] [PubMed]
- Brockett, C.; Carbone, S.; Abdelgaied, A.; Fisher, J.; Jennings, L. Influence of contact pressure, cross-shear and counterface material on the wear of PEEK and CFR-PEEK for orthopaedic applications. J. Mech. Behav. Biomed. Mater. 2016, 63, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Zajc, J.; Predan, J.; Gubeljak, N.; Moličnik, A.; Fokter, S.K. Modular femoral neck failure after revision of a total hip arthroplasty: A finite element analysis. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Jong, I.C.; Rogers, B.G.; Springer, W.T. GC 2009-267: Teaching Von Mises Stress: From Principal Axes to Nonprincipal Axes. In Proceedings of the ASEE Annual Conference, Austin, TX, USA, 14–17 June 2009. [Google Scholar]
- Equivalent Total Strain Result In ANSYS® Structural Analyses. Mechanicalland. Available online: https://mechanicalland.com/contact/ (accessed on 26 March 2022).
- Joshi, T.; Gupta, G. Effect of dynamic loading on hip implant using finite element method. Mater. Today: Proc. 2021, 46, 10211–10216. [Google Scholar] [CrossRef]
- Kn, C.; Zuber, M.; Bhat, S.; B, S.S.; Kini, C.R. Static structural analysis of different stem designs used in total hip arthroplasty using finite element method. Heliyon 2019, 5, e01767. [Google Scholar] [CrossRef]
- Joshi, T.; Sharma, R.; Mittal, V.K.; Gupta, V. Comparative investigation and analysis of hip prosthesis for different bio-compatible alloys. Mater. Today: Proc. 2021, 43, 105–111. [Google Scholar] [CrossRef]
- Kumar, A.; Rathi, A.; Sharma, N.K.; Singh, J. Studies on Titanium Hip Joint Implants using Finite Element Simulation. In Proceedings of the World Congress on Engineering 2016, WCE 2016, London, UK, 29 June–1 July 2016. [Google Scholar] [CrossRef]
- Head, W.C.; Bauk, D.J.; Emerson, R.H. Titanium as the material of choice for cementless femoral components in total hip arthroplasty. Clin. Orthop. Relat. Res. 1995, 311, 85–90. [Google Scholar]
- Anguiano-Sanchez, J.; Martinez-Romero, O.; Siller, H.; Elizondo, J.A.D.; Flores-Villalba, E.; Rodriguez, C.A. Influence of PEEK Coating on Hip Implant Stress Shielding: A Finite Element Analysis. Comput. Math. Methods Med. 2016, 2016, 6183679. [Google Scholar] [CrossRef] [PubMed]
- Enab, T.A.; Fouda, N.; Eldesouky, I. Comparison of Functionally Graded Hip Stem Implants with Various Second-Generation Titanium Alloys. J. Appl. Comput. Mech. 2021, 7, 1315–1323. [Google Scholar] [CrossRef]
- Yamako, G.; Janssen, D.; Hanada, S.; Anijs, T.; Ochiai, K.; Totoribe, K.; Chosa, E.; Verdonschot, N. Improving stress shielding following total hip arthroplasty by using a femoral stem made of β type Ti-33.6Nb-4Sn with a Young’s modulus gradation. J. Biomech. 2017, 63, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Huiskes, R.; Weinans, H.; van Rietbergen, B. The relationship between stress shielding and bone resorption around total hip stems and the effects of flexible materials. Clin. Orthop. Relat. Res. 1992, 274, 124–134. [Google Scholar] [CrossRef]
- Andreaus, U.; Colloca, M. Prediction of micromotion initiation of an implanted femur under physiological loads and constraints using the finite element method. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2009, 223, 589–605. [Google Scholar] [CrossRef]
- Kadir, M.R.A. Computational Biomechanics of the Hip Joint; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Otani, T.; Whiteside, L.A.; White, S.E.; McCarthy, D.S. Effects of femoral component material properties on cementless fixation in total hip arthroplasty: A comparison study between carbon composite, titanium alloy, and stainless steel. J. Arthroplast. 1993, 8, 67–74. [Google Scholar] [CrossRef]
- Sumner, T.T.D.R.; Urban, R.M.; Galante, J.O. The bone-biomaterial interface. Bone ingrowth into porous coatings attached to prosthesis of differing stiffness. In The Bone-Biomaterial Interface; Davies, J.E., Ed.; University of Toronto Press: Toronto, ON, Canada, 1991; Chapter 35. [Google Scholar]
- Elliott, B.; Goswami, T. Implant material properties and their role in micromotion and failure in total hip arthroplasty. Int. J. Mech. Mater. Des. 2011, 8, 1–7. [Google Scholar] [CrossRef]
- Kuiper, J.H.; Huiskes, R. Friction and stem stiffness affect dynamic interface motion in total hip replacement. J. Orthop. Res. 1996, 14, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-C.; Lai, Y.-S.; Cheng, C.-K.; Chang, T.-K. A cementless, proximally fixed anatomic femoral stem induces high micromotion with nontraumatic femoral avascular necrosis: A finite element study. J. Orthop. Transl. 2014, 2, 149–156. [Google Scholar] [CrossRef]
- Remond, G.; Nockolds, C.; Phillips, M.; Roques-Carmes, C. Implications of polishing techniques in quantitative x-ray microanalysi. J. Res. Natl. Inst. Stand. Technol. 2002, 107, 639–662. [Google Scholar] [CrossRef] [PubMed]
- Sporer, S.M.; Chalmers, P.N. Cutaneous Manifestation of Metallosis in a Metal-on-Metal Total Hip Arthroplasty After Acetabular Liner Dissociation. J. Arthroplast. 2012, 27, 1580.e13–1580.e16. [Google Scholar] [CrossRef] [PubMed]
- Willert, H.G.; Bertram, H.; Buchhorn, G.H. Osteolysis in alloarthroplasty of the hip. The role of ultra-high molecular weight polyethylene wear particles. Clin. Orthop. Relat. Res. 1990, 258, 95–107. [Google Scholar] [CrossRef]
- Maxian, T.A.; Brown, T.D.; Pedersen, D.R.; Callaghan, J.J. The Frank Stinchfield Award. 3-Dimensional sliding/contact computational simulation of total hip wear. Clin. Orthop. Relat. Res. 1996, 333, 41–50. [Google Scholar] [CrossRef]
- Maxian, T.A.; Brown, T.D.; Pedersen, D.R.; Callaghan, J.J. A sliding-distance-coupled finite element formulation for polyethylene wear in total hip arthroplasty. J. Biomech. 1996, 29, 687–692. [Google Scholar] [CrossRef]
- Maxian, T.A.; Brown, T.D.; Pedersen, D.R.; McKellop, H.A.; Lu, B.; Callaghan, J.J. Finite Element Analysis of Acetabular Wear. Validation, and backing and fixation effects. Clin. Orthop. Relat. Res. 1997, 344, 111–117. [Google Scholar] [CrossRef]
- Patil, S.; Bergula, A.; Chen, P.C.; Colwell, C.W.; D’Lima, D. Polyethylene wear and acetabular component orientation. J. Bone Jt. Surg. 2003, 85 (Suppl. 4), 56–63. [Google Scholar] [CrossRef] [PubMed]
- Raimondi, M.T.; Santambrogio, C.; Pietrabissa, R.; Raffelini, F.; Molfetta, L. Improved mathematical model of the wear of the cup articular surface in hip joint prostheses and comparison with retrieved components. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2001, 215, 377–390. [Google Scholar] [CrossRef]
- Teoh, S.; Chan, W.; Thampuran, R. An elasto-plastic finite element model for polyethylene wear in total hip arthroplasty. J. Biomech. 2001, 35, 323–330. [Google Scholar] [CrossRef]
- Bolland, B.J.R.F.; Culliford, D.J.; Langton, D.J.; Millington, J.P.S.; Arden, N.K.; Latham, J.M. High failure rates with a large-diameter hybrid metal-on-metal total hip replacement: Clinical, radiological and retrieval analysis. J. Bone Jt. Surgery. Br. Vol. 2011, 93, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Langton, D.J.; Sidaginamale, R.; Lord, J.K.; Nargol, A.V.F.; Joyce, T.J. Taper junction failure in large-diameter metal-on-metal bearings. Bone Jt. Res. 2012, 1, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.; Tay, G.H.; Godbolt, D.B.; Crawford, R.W. Pseudotumor in a Well-Fixed Metal-on-Polyethylene Uncemented Hip Arthroplasty. J. Arthroplast. 2012, 27, 493.e13–493.e17. [Google Scholar] [CrossRef] [PubMed]
- Kyomoto, M.; Shoyama, Y.; Saiga, K.; Moro, T.; Ishihara, K. Reducing fretting-initiated crevice corrosion in hip simulator tests using a zirconia-toughened alumina femoral head. J. Biomed. Mater. Res. Part B Appl. Biomater. 2017, 106, 2815–2826. [Google Scholar] [CrossRef]
- Morlock, M.M.; Dickinson, E.C.; Günther, K.-P.; Bünte, D.; Polster, V. Head Taper Corrosion Causing Head Bottoming Out and Consecutive Gross Stem Taper Failure in Total Hip Arthroplasty. J. Arthroplast. 2018, 33, 3581–3590. [Google Scholar] [CrossRef]
- Fallahnezhad, K.; Farhoudi, H.; Oskouei, R.H.; Taylor, M. Influence of geometry and materials on the axial and torsional strength of the head–neck taper junction in modular hip replacements: A finite element study. J. Mech. Behav. Biomed. Mater. 2016, 60, 118–126. [Google Scholar] [CrossRef]
- Jauch, S.; Huber, G.; Hoenig, E.; Baxmann, M.; Grupp, T.; Morlock, M. Influence of material coupling and assembly condition on the magnitude of micromotion at the stem–neck interface of a modular hip endoprosthesis. J. Biomech. 2011, 44, 1747–1751. [Google Scholar] [CrossRef]
- Haschke, H.; Konow, T.; Huber, G.; Morlock, M.M. Influence of flexural rigidity on micromotion at the head-stem taper interface of modular hip prostheses. Med. Eng. Phys. 2019, 68, 1–10. [Google Scholar] [CrossRef]
- Dyrkacz, R.M.R.; Brandt, J.M.; Morrison, J.B.; O’Brien, S.T.; Ojo, O.A.O.; Turgeon, T.R.; Wyss, U.P. Finite element analysis of the head–neck taper interface of modular hip prostheses. Tribol. Int. 2015, 91, 206–213. [Google Scholar] [CrossRef]
- Collier, J.; Surprenant, V.; Jensen, R.; Mayor, M.; Surprenant, H. Corrosion between the components of modular femoral hip prostheses. J. Bone Jt. Surg. Br. Vol. 1992, 74-B, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, J.R.; Gilbert, J.L.; Jacobs, J.; Bauer, T.; Paprosky, W.; Leurgans, S. A Multicenter Retrieval Study of the Taper Interfaces of Modular Hip Prostheses. Clin. Orthop. Relat. Res. 2002, 401, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Uddin, M.; Zhang, L. Predicting the wear of hard-on-hard hip joint prostheses. Wear 2013, 301, 192–200. [Google Scholar] [CrossRef]
- Jamari, J.; Ammarullah, M.I.; Santoso, G.; Sugiharto, S.; Supriyono, T.; Prakoso, A.T.; Basri, H.; van der Heide, E. Computational Contact Pressure Prediction of CoCrMo, SS 316L and Ti6Al4V Femoral Head against UHMWPE Acetabular Cup under Gait Cycle. J. Funct. Biomater. 2022, 13, 64. [Google Scholar] [CrossRef]
- Jamari, J.; Ammarullah, M.I.; Santoso, G.; Sugiharto, S.; Supriyono, T.; van der Heide, E. In Silico Contact Pressure of Metal-on-Metal Total Hip Implant with Different Materials Subjected to Gait Loading. Metals 2022, 12, 1241. [Google Scholar] [CrossRef]
- Chang, K.-H. Fatigue and Fracture Analysis. In e-Design-Computer-Aided Engineering Design; Elsevier Inc.: Amsterdam, The Netherlands, 2015; Chapter 9; pp. 463–521. [Google Scholar]
- Hamrock, B.J.; Schmid, S.R.; Jacobson, B.O. Fatigue and Impact. In Fundamentals of Machine Elements, 2nd ed.; McGraw-Hill Publishing Company: New York, NY, USA, 2005; Chapter 7. [Google Scholar]
- Kayabasi, O.; Ekici, B. The effects of static, dynamic and fatigue behavior on three-dimensional shape optimization of hip prosthesis by finite element method. Mater. Des. 2007, 28, 2269–2277. [Google Scholar] [CrossRef]
- Thrivikraman, G.; Madras, G.; Basu, B. ChemInform Abstract: In vitro/in vivo Assessment and Mechanisms of Toxicity of Bioceramic Materials and Its Wear Particulates. ChemInform 2014, 45, 12763–12781. [Google Scholar] [CrossRef]
- Vu, N.B.; Truong, N.H.; Dang, L.T.; Phi, L.T.; Ho, N.T.-T.; Pham, T.N.; Phan, T.P.; Van Pham, P. In vitro and in vivo biocompatibility of Ti-6Al-4V titanium alloy and UHMWPE polymer for total hip replacement. Biomed. Res. Ther. 2016, 3, 14. [Google Scholar] [CrossRef]
- Takamura, K.; Hayashi, K.; Ishinishi, N.; Yamada, T.; Sugioka, Y. Evaluation of carcinogenicity and chronic toxicity associated with orthopedic implants in mice. J. Biomed. Mater. Res. 1994, 28, 583–589. [Google Scholar] [CrossRef]
- Yuan, Y.; Liu, C.; Qian, J.; Wang, J.; Zhang, Y. Size-mediated cytotoxicity and apoptosis of hydroxyapatite nanoparticles in human hepatoma HepG2 cells. Biomaterials 2010, 31, 730–740. [Google Scholar] [CrossRef]
- Brodt, S.; Matziolis, G.; Buckwitz, B.; Zippelius, T.; Strube, P.; Roth, A. Long-term follow-up of bone remodelling after cementless hip arthroplasty using different stems. Sci. Rep. 2020, 10, 10143. [Google Scholar] [CrossRef] [PubMed]
- Rivière, C.; Grappiolo, G.; Jr, C.A.E.; Vidalain, J.-P.; Chen, A.-F.; Boehler, N.; Matta, J.; Vendittoli, P.-A. Long-term bone remodelling around ‘legendary’ cementless femoral stems. EFORT Open Rev. 2018, 3, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Craven, T.G.; Carson, W.L.; Asher, M.A.; Robinson, R.G. The Effects of Implant Stiffness on the Bypassed Bone Mineral Density and Facet Fusion Stiffness of the Canine Spine. Spine 1994, 19, 1664–1673. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-L.; Lin, T.; Liu, A.; Shi, M.-M.; Hu, B.; Shi, Z.-L.; Yan, S.-G. Does hydroxyapatite coating have no advantage over porous coating in primary total hip arthroplasty? A meta-analysis. J. Orthop. Surg. Res. 2015, 10, 21. [Google Scholar] [CrossRef]
- Svehla, M.; Morberg, P.; Bruce, W.; Zicat, B.; Walsh, W. The effect of substrate roughness and hydroxyapatite coating thickness on implant shear strength. J. Arthroplast. 2002, 17, 304–311. [Google Scholar] [CrossRef]
- Jacobs, J.J.; Gilbert, J.L.; Urban, R.M. Corrosion of Metal Orthopaedic Implants*. J. Bone Jt. Surg. 1998, 80, 268–282. [Google Scholar] [CrossRef]
- Eltit, F.; Wang, Q.; Wang, R. Mechanisms of Adverse Local Tissue Reactions to Hip Implants. Front. Bioeng. Biotechnol. 2019, 7, 176. [Google Scholar] [CrossRef]
- Cooper, H.; Urban, R.M.; Wixson, R.L.; Meneghini, R.; Jacobs, J.J. Adverse Local Tissue Reaction Arising from Corrosion at the Femoral Neck-Body Junction in a Dual-Taper Stem with a Cobalt-Chromium Modular Neck. J. Bone Jt. Surg. 2013, 95, 865–872. [Google Scholar] [CrossRef]
- Tipper, J.; Firkins, P.; Besong, A.; Barbour, P.; Nevelos, J.; Stone, M.; Ingham, E.; Fisher, J. Characterisation of wear debris from UHMWPE on zirconia ceramic, metal-on-metal and alumina ceramic-on-ceramic hip prostheses generated in a physiological anatomical hip joint simulator. Wear 2001, 250, 120–128. [Google Scholar] [CrossRef]
- Goldsmith, A.A.J.; Dowson, D.; Isaac, G.H.; Lancaster, J.G. A comparative joint simulator study of the wear of metal-on-metal and alternative material combinations in hip replacements. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2000, 214, 39–47. [Google Scholar] [CrossRef]
- Hart, A.J.; Quinn, P.D.; Sampson, B.; Sandison, A.; Atkinson, K.; Skinner, J.; Powell, J.J.; Mosselmans, J. The chemical form of metallic debris in tissues surrounding metal-on-metal hips with unexplained failure. Acta Biomater. 2010, 6, 4439–4446. [Google Scholar] [CrossRef] [PubMed]
- Goode, A.E.; Perkins, J.M.; Sandison, A.; Karunakaran, C.; Cheng, H.; Wall, D.; Skinner, J.A.; Hart, A.J.; Porter, A.E.; McComb, D.W.; et al. Chemical speciation of nanoparticles surrounding metal-on-metal hips. Chem. Commun. 2012, 48, 8335–8337. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Amstutz, H.C.; Le Duff, M.J. Correlation between Serum Metal Ion Levels and Adverse Local Tissue Reactions after Conserve® plus Hip Resurfacing Arthroplasty. HIP Int. 2017, 27, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Billi, F.; Campbell, P. Nanotoxicology of metal wear particles in total joint arthroplasty: A review of current concepts. J. Appl. Biomater. Biomech. 2010, 8, 1–6. [Google Scholar]
- Hedberg, Y.; Wallinder, I.O. Metal release and speciation of released chromium from a biomedical CoCrMo alloy into simulated physiologically relevant solutions. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 102, 693–699. [Google Scholar] [CrossRef]
- Papageorgiou, I.; Brown, C.; Schins, R.; Singh, S.; Newson, R.; Davis, S.; Fisher, J.; Ingham, E.; Case, C.P. The effect of nano- and micron-sized particles of cobalt–chromium alloy on human fibroblasts in vitro. Biomaterials 2007, 28, 2946–2958. [Google Scholar] [CrossRef]
- Smith, L.J.; Holmes, A.L.; Kandpal, S.K.; Mason, M.D.; Zheng, T.; Wise, J.P. The cytotoxicity and genotoxicity of soluble and particulate cobalt in human lung fibroblast cells. Toxicol. Appl. Pharmacol. 2014, 278, 259–265. [Google Scholar] [CrossRef]
- Chamaon, K.; Schönfeld, P.; Awiszus, F.; Bertrand, J.; Lohmann, C.H. Ionic cobalt but not metal particles induces ROS generation in immune cells in vitro. J. Biomed. Mater. Res. Part B Appl. Biomater. 2018, 107, 1246–1253. [Google Scholar] [CrossRef]
- Campbell, P.; Ebramzadeh, E.; Nelson, S.; Takamura, K.; De Smet, K.; Amstutz, H.C. Histological Features of Pseudotumor-like Tissues From Metal-on-Metal Hips. Clin. Orthop. Relat. Res. 2010, 468, 2321–2327. [Google Scholar] [CrossRef]
- Eltit, F.; Assiri, A.; Garbuz, D.; Duncan, C.; Masri, B.; Greidanus, N.; Bell, R.; Sharma, M.; Cox, M.; Wang, R. Adverse reactions to metal on polyethylene implants: Highly destructive lesions related to elevated concentration of cobalt and chromium in synovial fluid. J. Biomed. Mater. Res. Part A 2017, 105, 1876–1886. [Google Scholar] [CrossRef]
- Talha, M.; Ma, Y.; Kumar, P.; Lin, Y.; Singh, A. Role of protein adsorption in the bio corrosion of metallic implants—A review. Colloids Surf. B Biointerfaces 2019, 176, 494–506. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Gilbert, J.L. The effect of simulated inflammatory conditions and pH on fretting corrosion of CoCrMo alloy surfaces. Wear 2017, 390–391, 302–311. [Google Scholar] [CrossRef]
- López, J.; Humphriss, R.L.; Beswick, A.; Thom, H.H.Z.; Hunt, L.P.; Burston, A.; Fawsitt, C.; Hollingworth, W.; Higgins, J.; Welton, N.; et al. Choice of implant combinations in total hip replacement: Systematic review and network meta-analysis. BMJ 2017, 359, j4651. [Google Scholar] [CrossRef]
- Di Martino, A.; Castagnini, F.; Stefanini, N.; Bordini, B.; Geraci, G.; Pilla, F.; Traina, F.; Faldini, C. Survival rates and reasons for revision of different stem designs in total hip arthroplasty for developmental dysplasia: A regional registry study. J. Orthop. Traumatol. 2021, 22, 29. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials | Type | Young’s Modulus (Gpa) | Yield Strength (Mpa) | Ultimate Strength (Mpa) | Poisson Ratio | Density (Kg/m3) |
|---|---|---|---|---|---|---|
| Ti6Al4V | α + β | 110 | 800 | 900 | 0.342 | 4500 |
| Ti6Al7Nb | α + β | 120 | 950 | 1050 | 0.33 | 4510 |
| Ti-29Nb-13Ta-4.5Zr | β | 40–80 | >1000 | 911 | 0.33 | 5000 |
| Ti-15Mo-5Zr | β | 78 | 920 | 960 | 0.33 | 5060 |
| Ti-15Mo-5Zr-3Al | β | 82 | 864 | 1475 | 0.3 | 4950 |
| Ti-13Nb-13Zr | Near β | 84 | 900 | 1037 | 0.3 | 4990 |
| Ti-29Nb-13Ta-4.6Zr | β | 80 | 864 | 911 | 0.3 | 5000 |
| Ti-35Nb-7Zr-5Ta | β | 55 | 596 | 742 | 0.3 | 5000 |
| Ti-13Nb-13Zr | β | 82 | 908 | 1037 | 0.3 | 4990 |
| Ti-35Nb-5Ta-7Zr-0.4O | β | 66 | 976 | 1010 | 0.34 | 5600 |
| Ni-Ti Alloys | - | 58 | 472 | 1290 | 0.325 | 6560 |
| Ni-Ta Alloys | - | 83 | 690 | 895 | 0.3 | 6450 |
| Inconel 718 (UNS N07718) | - | 200 | 1100 | 1375 | 0.29 | 8230 |
| Co-Cr | - | 220 | 450 | 270 | 0.3 | 8500 |
| Co-Ni-Cr-Mo | - | 230 | 1000 | 1650 | 0.29 | 8700 |
| Bio-steels | - | 210 | 180–600 | 480–900 | 0.29 | 7500 |
| UHMWPE | - | 0.689 | 20.7 | 40 | 0.33 | 931–949 |
| PEEK | - | 3.76–3.95 | 87–95 | - | 0.37 | 1230 |
| HA | 13 | 38 | 48 | 0.27 | 3005 |
| References | Implant Stem Material | Von Mises Stress (MPa) | Equivalent von Mises Strain | Deformation (mm) |
|---|---|---|---|---|
| Şensoy et al. [8] | Nickel–titanium alloy | 980 | 0.01695 | 15.35 |
| Stainless steel | 1104 | 0.00526 | 13.94 | |
| Ti6AlV | 989 | 0.008999 | 16.59 | |
| Joshi et al. [74] | Co-Cr-Mo | 575 | 0.0028 | 0.155 |
| Ti-6AL-4V | 550.00 | 0.0055 | 0.35 | |
| Ti-6Al-7Nb | 540.00 | 0.0049 | 0.33 | |
| Chethan et al. [75] | Ti–4Al–6V | 622.24 | 0.0054 | 0.490 |
| Co-Cr | 623.48 | 0.0031 | 0.28 | |
| Joshi et al. [76] | Ti-6AL-4V | 622.24 | 0.01 | 0.49 |
| Co-Cr Alloy | 722.7 | 0.0039707 | 0.25684 | |
| Co-Cr-Mo | 728.88 | 0.003417 | 0.21916 | |
| Ti-6Al-7Nb | 702.75 | 0.0062826 | 0.41773 | |
| Ti-6Al-4V | 709.64 | 0.0069297 | 0.45639 | |
| Ti-29Nb-13Ta-4.6Zr | 722.7 | 0.0097282 | 0.62927 | |
| Ti-13Nb-13Zr | 722.7 | 0.009265 | 0.5993 | |
| Kumar et al. [77] | Ti-6Al-4V | 0.58 | 5.27 × 10−6 | 0.45 |
| Ti-6Al-7Nb | 0.575 | 4.7 × 10−6 | 0.43 | |
| Ti-13Nb-13Zr | 0.583 | 7.07 × 10−6 | 0.58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soliman, M.M.; Chowdhury, M.E.H.; Islam, M.T.; Musharavati, F.; Nabil, M.; Hafizh, M.; Khandakar, A.; Mahmud, S.; Nezhad, E.Z.; Shuzan, M.N.I.; et al. A Review of Biomaterials and Associated Performance Metrics Analysis in Pre-Clinical Finite Element Model and in Implementation Stages for Total Hip Implant System. Polymers 2022, 14, 4308. https://doi.org/10.3390/polym14204308
Soliman MM, Chowdhury MEH, Islam MT, Musharavati F, Nabil M, Hafizh M, Khandakar A, Mahmud S, Nezhad EZ, Shuzan MNI, et al. A Review of Biomaterials and Associated Performance Metrics Analysis in Pre-Clinical Finite Element Model and in Implementation Stages for Total Hip Implant System. Polymers. 2022; 14(20):4308. https://doi.org/10.3390/polym14204308
Chicago/Turabian StyleSoliman, Md Mohiuddin, Muhammad E. H. Chowdhury, Mohammad Tariqul Islam, Farayi Musharavati, Mohammad Nabil, Muhammad Hafizh, Amith Khandakar, Sakib Mahmud, Erfan Zal Nezhad, Md Nazmul Islam Shuzan, and et al. 2022. "A Review of Biomaterials and Associated Performance Metrics Analysis in Pre-Clinical Finite Element Model and in Implementation Stages for Total Hip Implant System" Polymers 14, no. 20: 4308. https://doi.org/10.3390/polym14204308
APA StyleSoliman, M. M., Chowdhury, M. E. H., Islam, M. T., Musharavati, F., Nabil, M., Hafizh, M., Khandakar, A., Mahmud, S., Nezhad, E. Z., Shuzan, M. N. I., & Abir, F. F. (2022). A Review of Biomaterials and Associated Performance Metrics Analysis in Pre-Clinical Finite Element Model and in Implementation Stages for Total Hip Implant System. Polymers, 14(20), 4308. https://doi.org/10.3390/polym14204308