Current Insight of Collagen Biomatrix for Gingival Recession: An Evidence-Based Systematic Review




Abstract
1. Introduction
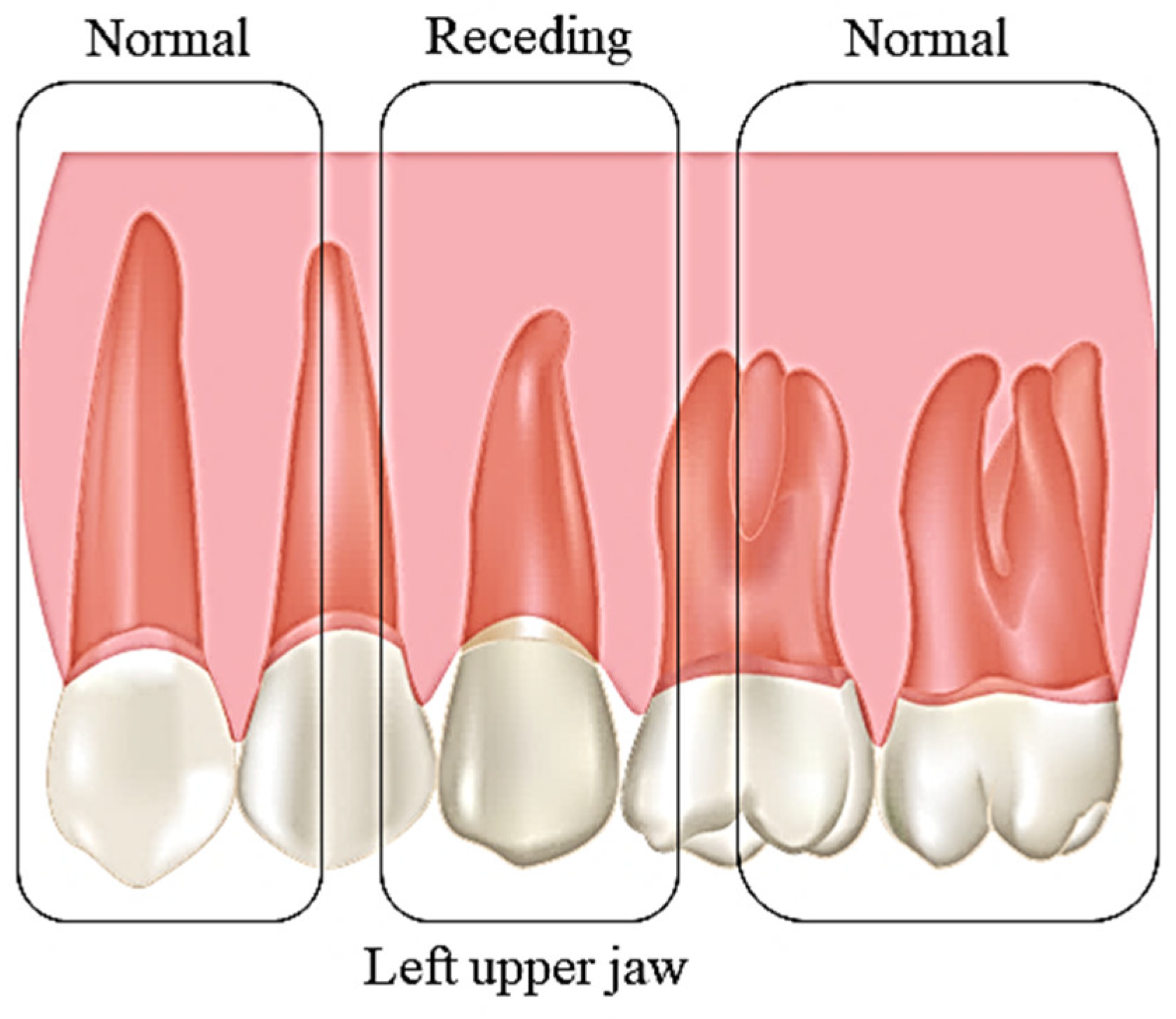
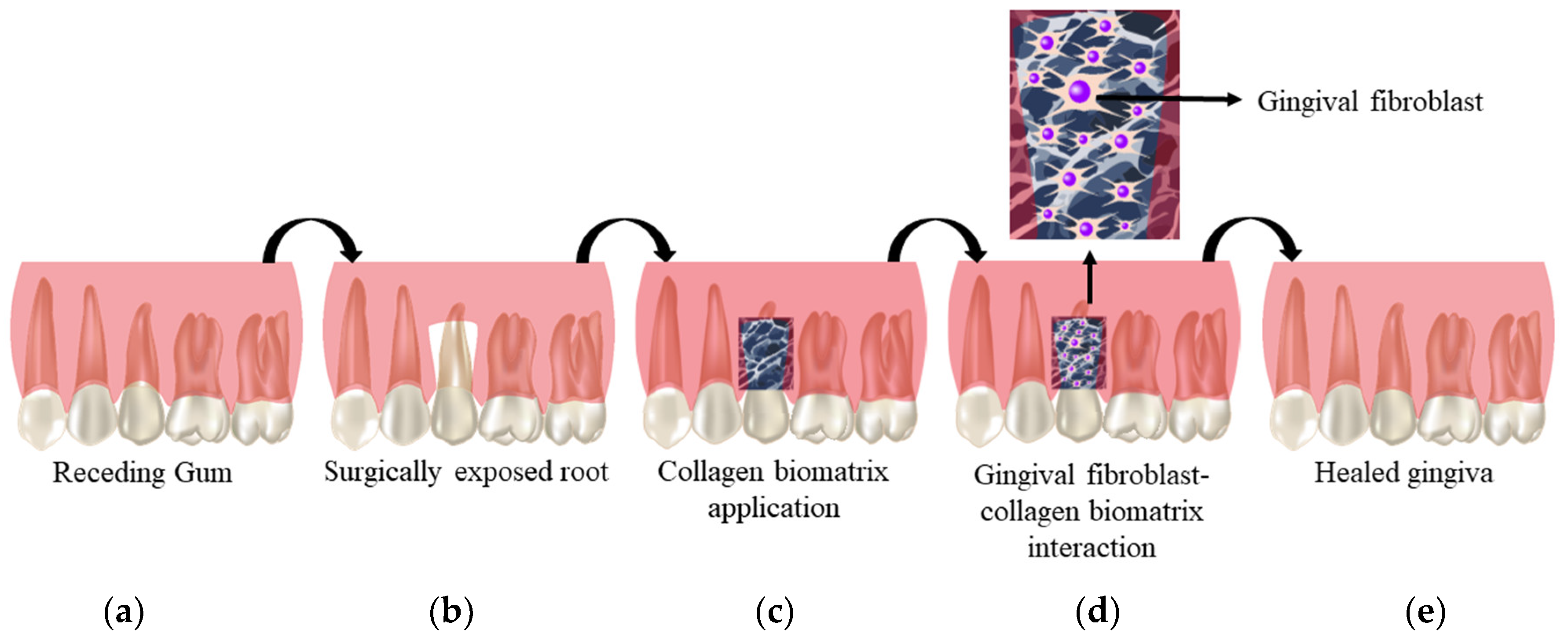
1.1. Gingival Recession (GR)
1.2. Collagen (Col)
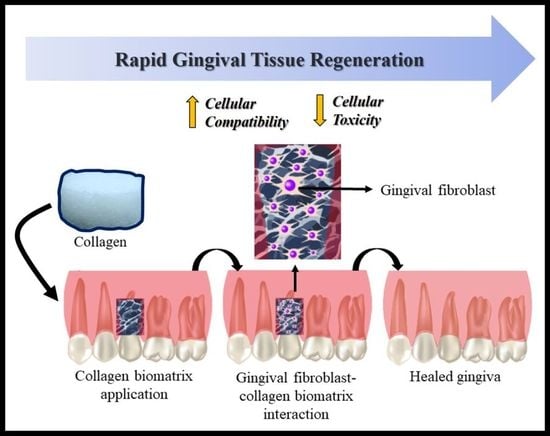
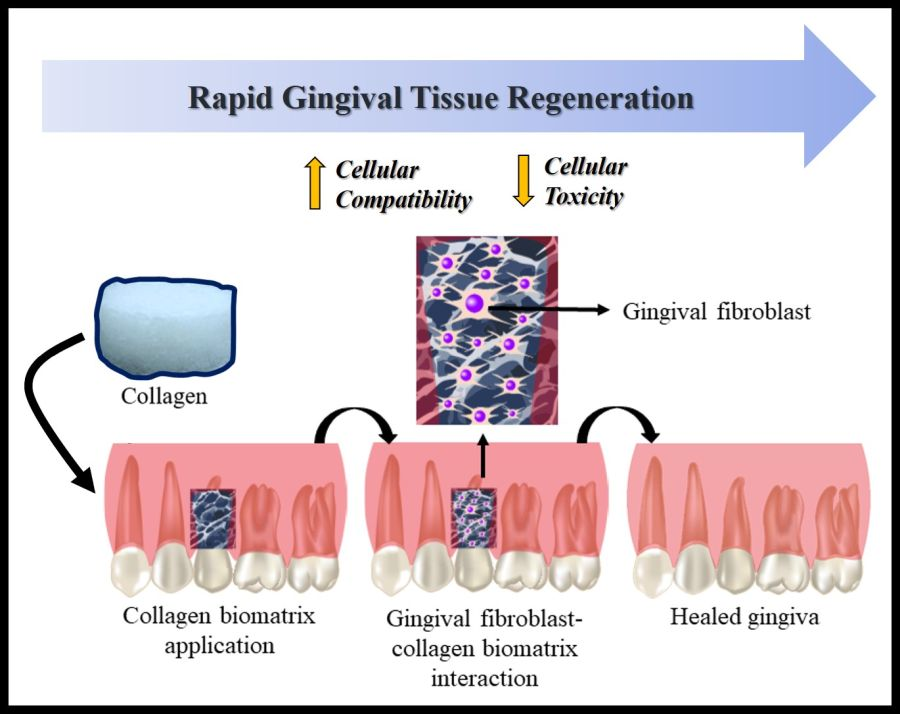
1.3. Collagen for Periodontal Tissue Regeneration
1.4. Cell–Biomaterial Interaction
1.5. The Role of Pre-Clinical Investigation and Safe Approach of Collagen Biomatrix for GR
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Extraction and Management
2.5. Strategy for Data Extraction
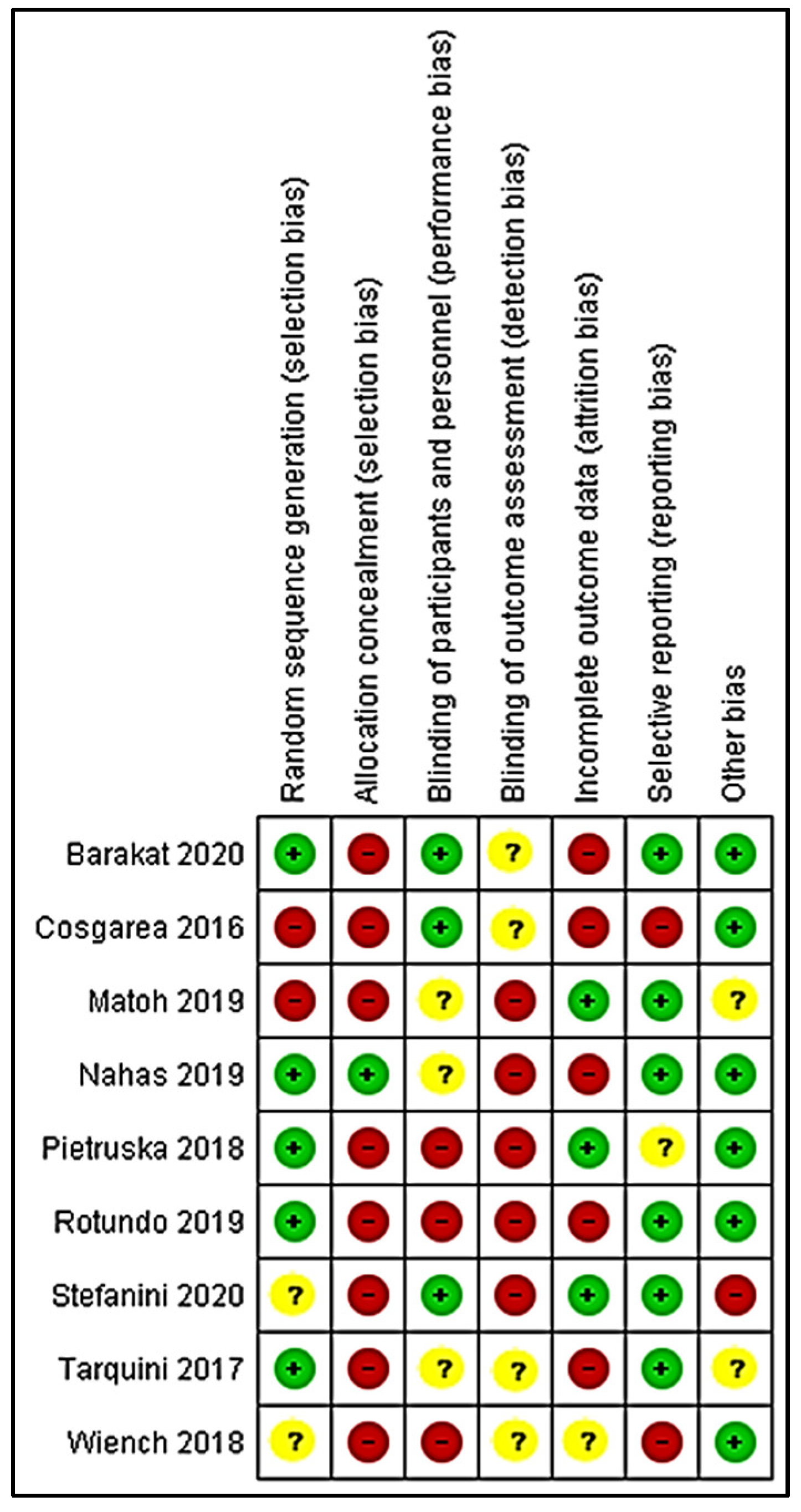
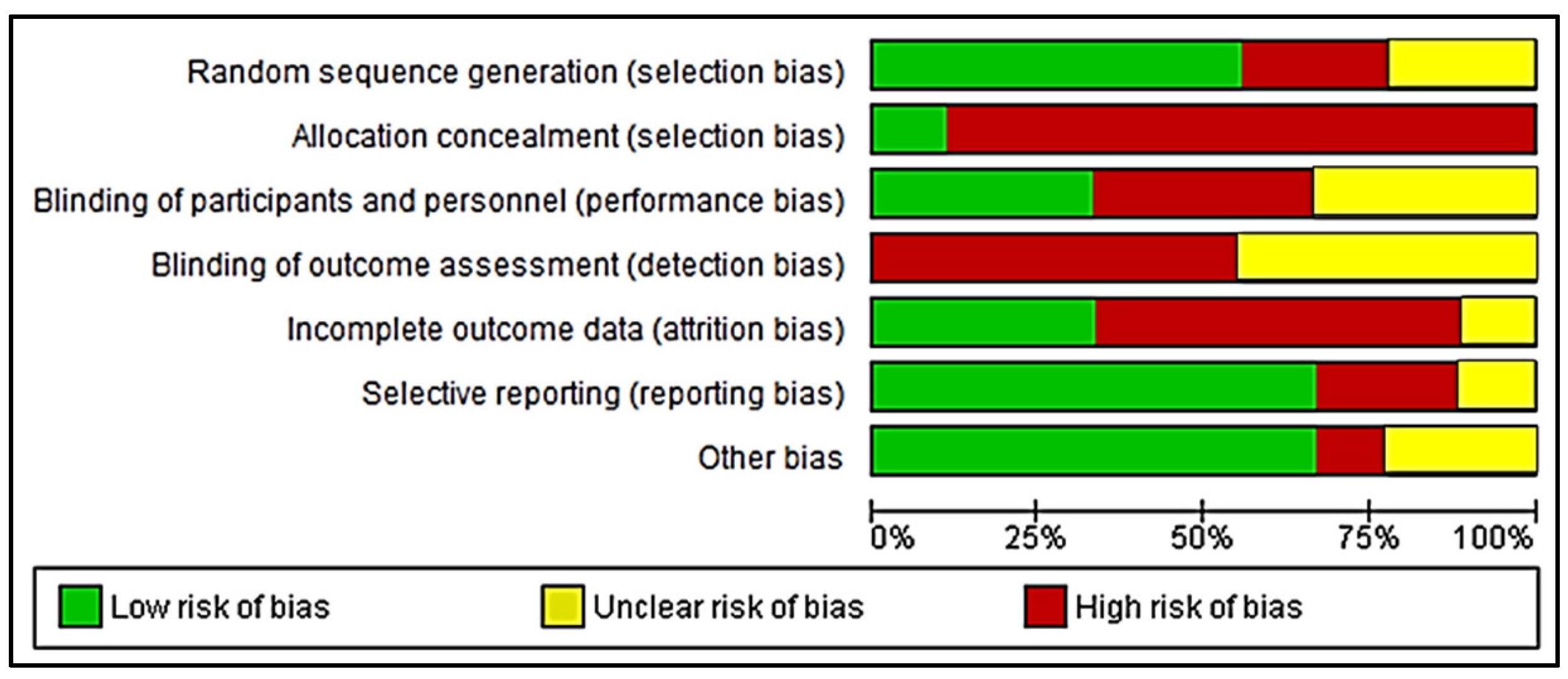
2.6. Risk of Bias Assessment
3. Results
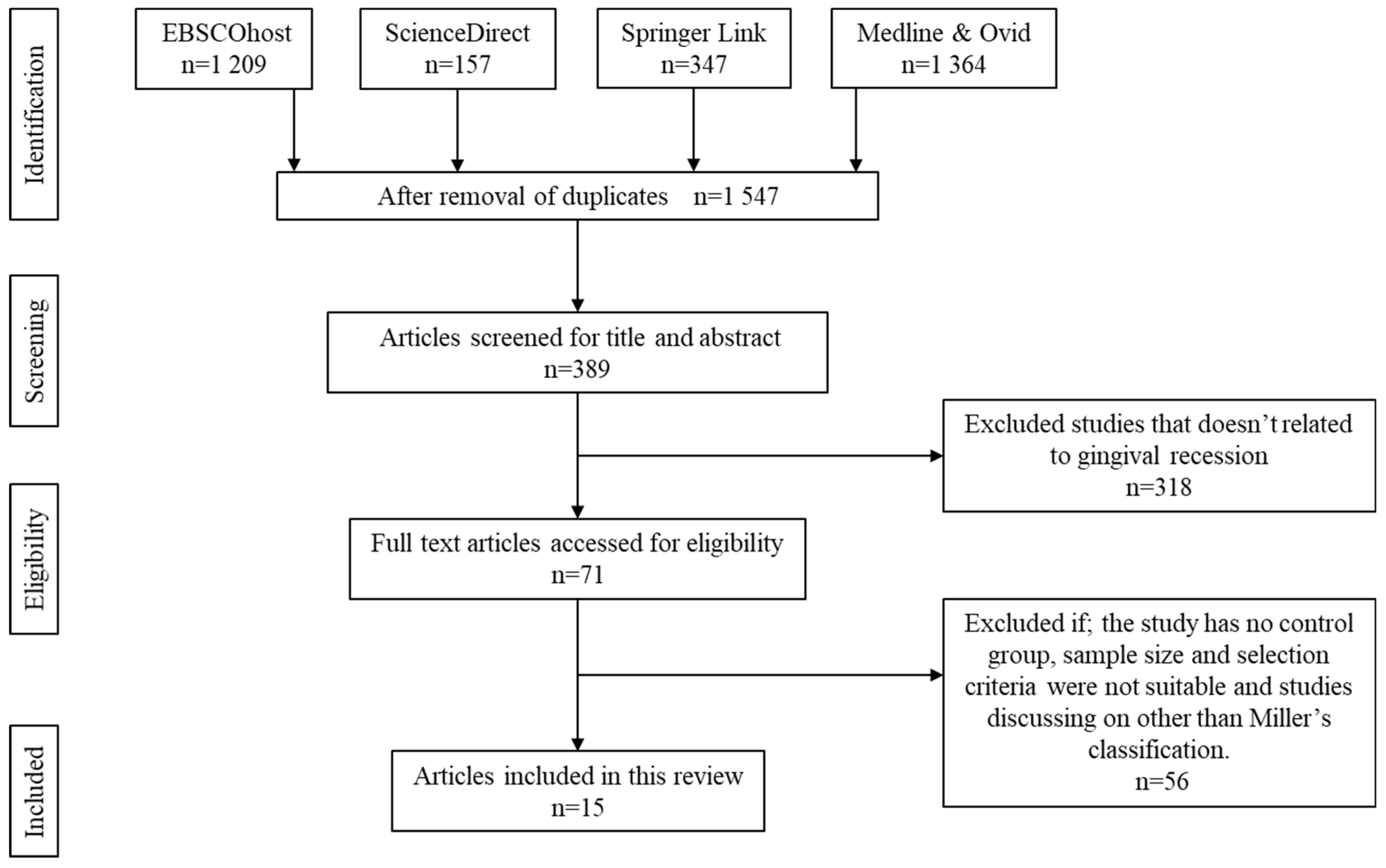
3.1. Literature Search
3.2. Bioscaffold Three-Dimensional Structure
3.3. Cellular–Bioscaffold Interaction
3.4. The Efficiency of Gingival Tissue Regeneration
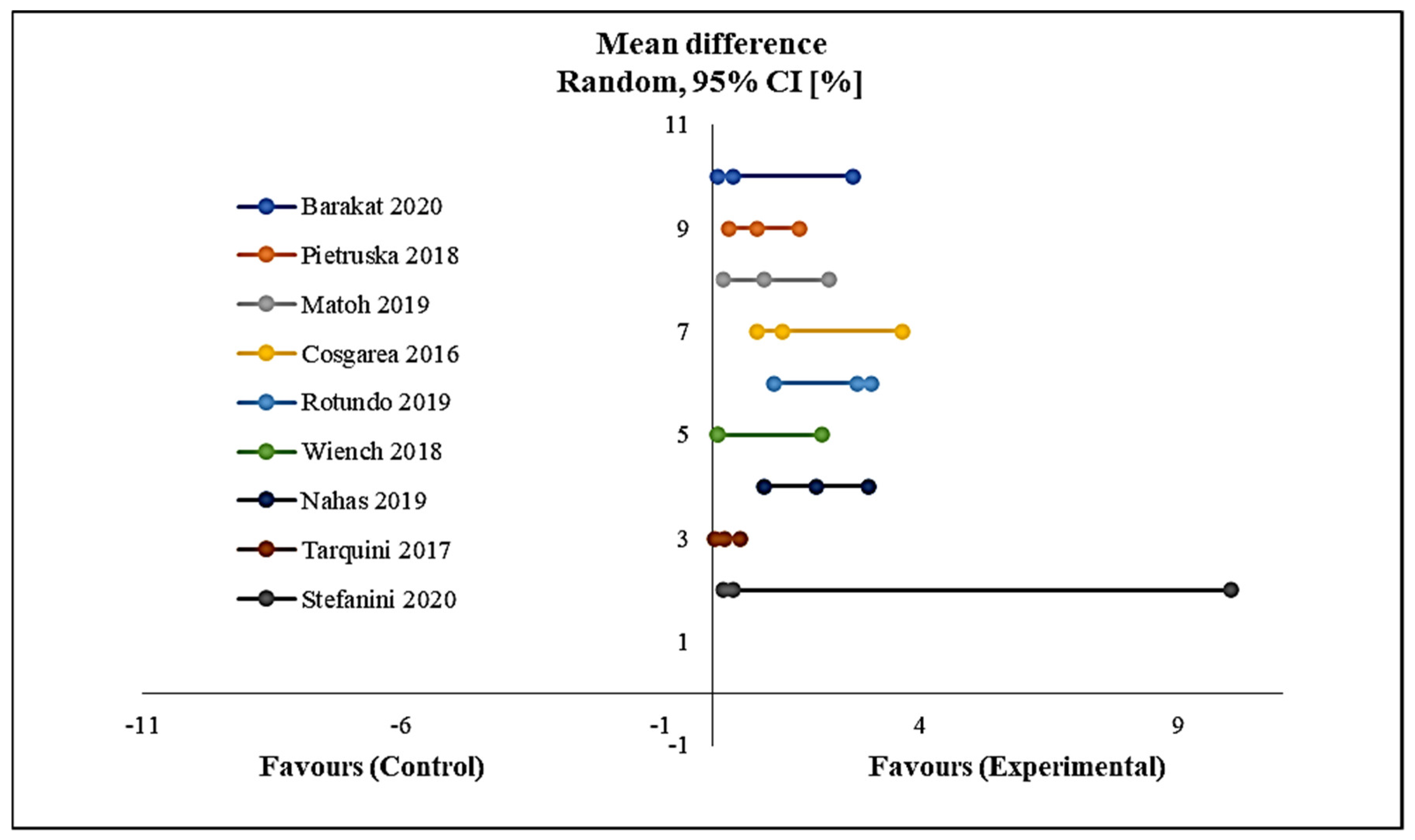
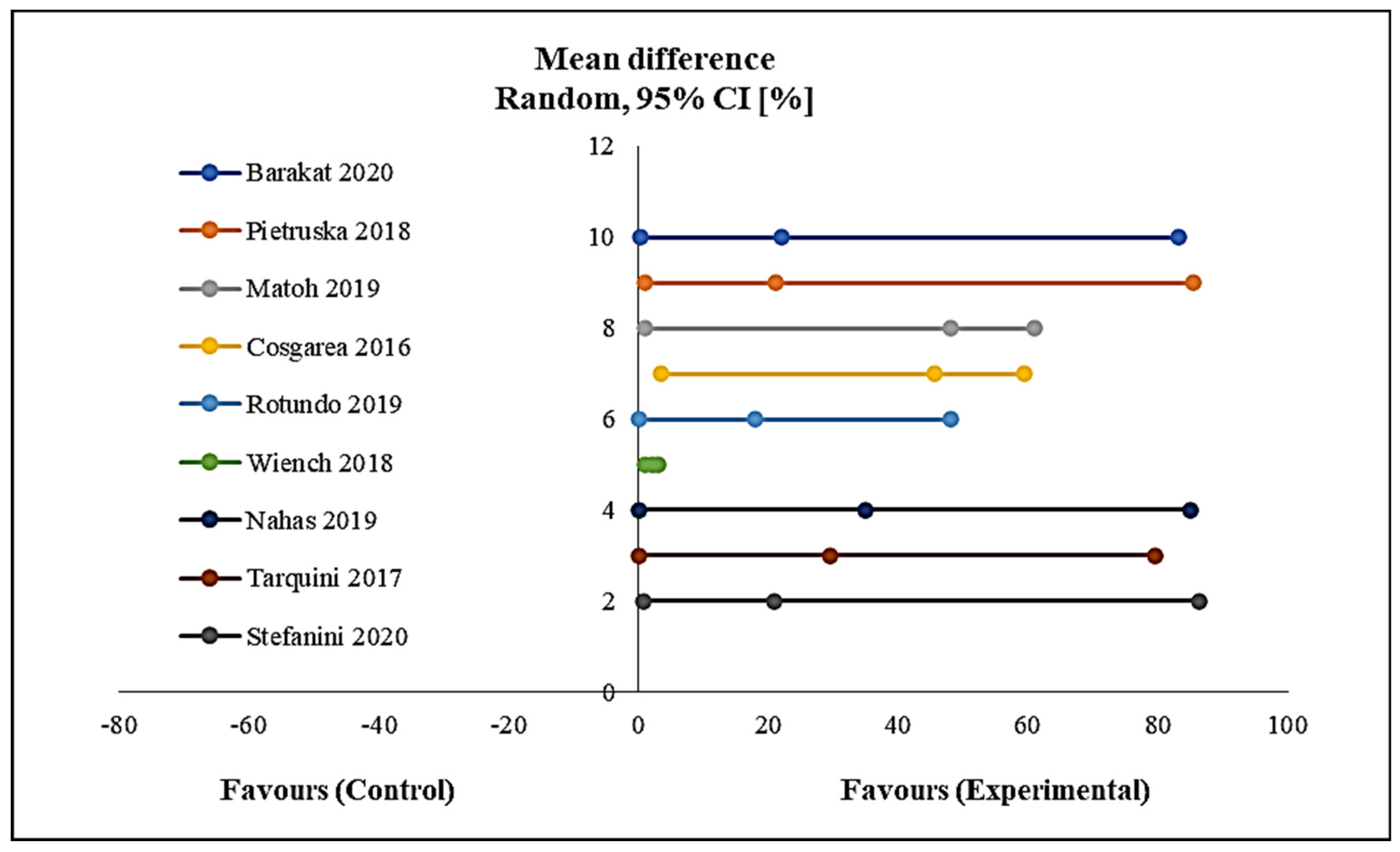
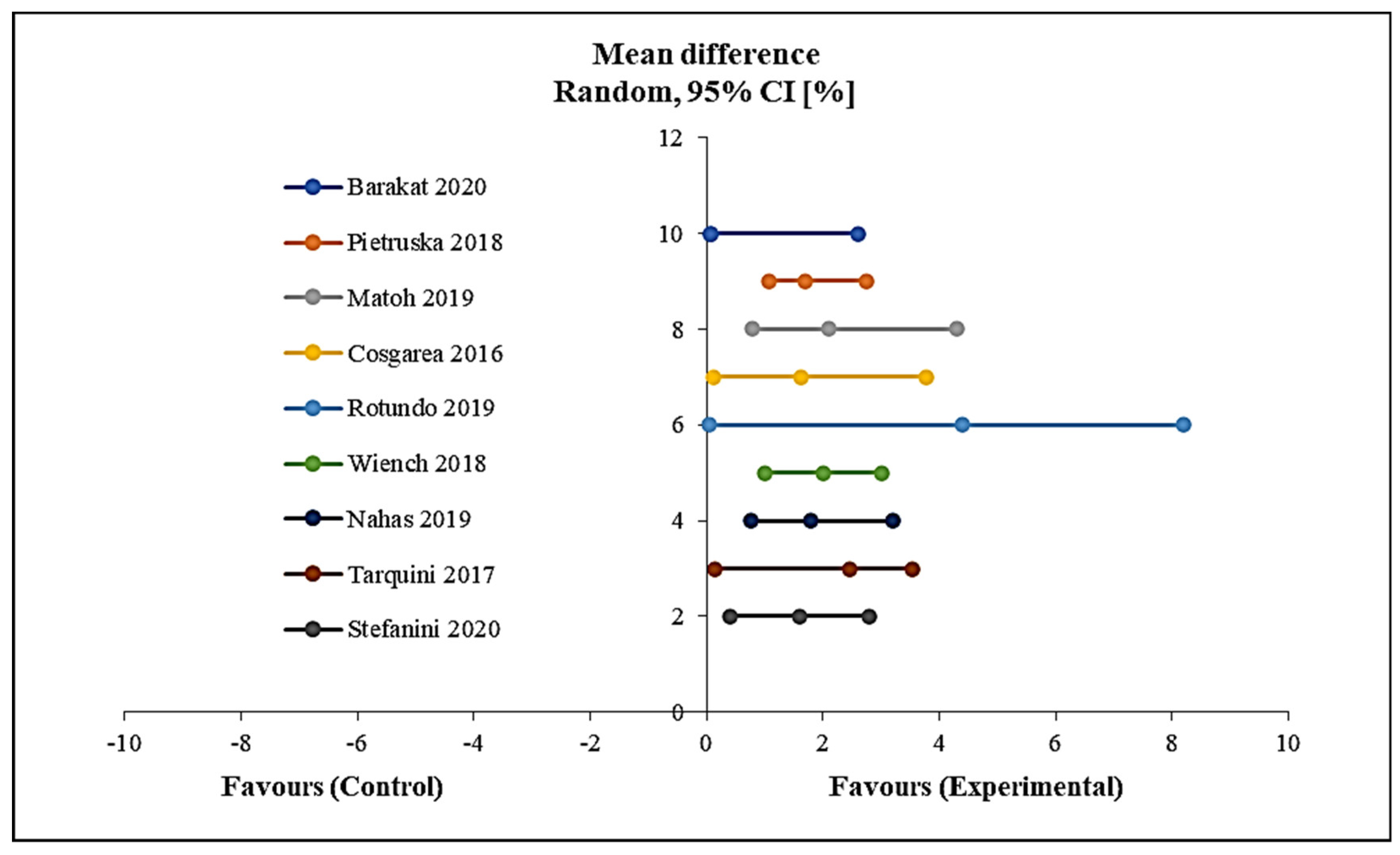
3.5. Clinical Trial Effectiveness
4. Discussion
5. COVID-19 Outbreak and Dentistry
6. Conclusions
7. Limitation
8. Future Trends and Perspective
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Handelman, C.S.; Eltink, A.P.; BeGole, E. Quantitative measures of gingival recession and the influence of gender, race, and attrition. Prog. Orthod. 2018, 19, 5. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.C.; Cáceres, M.; Martínez, C.; Oyarzún, A.; Martínez, J. Gingival wound healing: An essential response disturbed by aging? J. Dent. Res. 2014, 94, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Pradeep, K.; Rajababu, P.; Satyanarayana, D.; Sagar, V. Gingival recession: Review and strategies in treatment of recession. Case Rep. Dent. 2012, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.; Nixon, P.J.; Chan, M.F.W.-Y. Gingival recession: Part 1. Aetiology and non-surgical management. Br. Dent. J. 2011, 211, 251–254. [Google Scholar] [CrossRef][Green Version]
- Kumar, A.; Masamatti, S.S. A new classification system for gingival and palatal recession. J. Indian Soc. Periodontol. 2013, 17, 175–181. [Google Scholar] [CrossRef]
- Jati, A.S.; Furquim, L.Z.; Consolaro, A. Gingival recession: Its causes and types, and the importance of orthodontic treatment. Dent. Press J. Orthod. 2016, 21, 18–29. [Google Scholar] [CrossRef]
- Alani, A.; Kelleher, M. Restorative complications of orthodontic treatment. Br. Dent. J. 2016, 221, 389–400. [Google Scholar] [CrossRef]
- Mahesh, L.; Kurtzman, G.M.; Shukla, S. Regeneration in periodontics: Collagen—A review of its properties and applications in dentistry. Compend. Contin. Educ. Dent. 2015, 36. [Google Scholar]
- Ministry of Health Malaysia. National Oral Health Survey of Adults 2010 (NOHSA 2010). Available online: http://www.myhealth.gov.my/en/gum-health-and-denture (accessed on 20 May 2020).
- Sakti, E.S.; Budijanto, D.; Kurniawan, R.; Widiantini, W.; Mulya, D. InfoDatin. 2019, pp. 1–6. Available online: https://pusdatin.kemkes.go.id/resources/download/pusdatin/infodatin/infodatin-gigi.pdf (accessed on 11 July 2020).
- Rosdiani, A.F.; Widiyanti, P.; Rudyardjo, D.I. Synthesis and characterization biocomposite collagen-chitosan-glycerol as scaffold for gingival recession therapy. J. Int. Dent. Med. Res. 2017, 10, 118–122. [Google Scholar]
- Nurfriana, P.; Widiyanti, P.; Rudyardjo, D.I. Effect of collagen-chitosan-glycerol composition in scaffold for gingival recession therapy. J. Biomim. Biomater. Biomed. Eng. 2019, 40, 101–108. [Google Scholar] [CrossRef]
- Hatayama, T.; Nakada, A.; Nakamura, H.; Mariko, W.; Tsujimoto, G.; Nakamura, T. Regeneration of gingival tissue using in situ tissue engineering with collagen scaffold. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 124, 348–354.e1. [Google Scholar] [CrossRef][Green Version]
- Schmitt, C.M.; Schlegel, K.A.; Gammel, L.; Moest, T. Gingiva thickening with a porcine collagen matrix in a preclinical dog model: Histological outcomes. J. Clin. Periodontol. 2019, 46, 1273–1281. [Google Scholar] [CrossRef] [PubMed]
- Shirakata, Y.; Sculean, A.; Shinohara, Y.; Sena, K.; Takeuchi, N.; Bosshardt, D.D.; Noguchi, K. Healing of localized gingival recessions treated with a coronally advanced flap alone or combined with an enamel matrix derivative and a porcine acellular dermal matrix: A preclinical study. Clin. Oral Investig. 2015, 20, 1791–1800. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.-K.; Sun, Y.-K.; Lee, J.-S.; Choi, S.-H.; Jung, U.-W. Root coverage using porcine collagen matrix with fibroblast growth factor-2: A pilot study in dogs. J. Clin. Periodontol. 2016, 44, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Barakat, H.; Dayoub, S. Treatment of miller type I and II gingival recession defects using three-dimensional porcine collagen matrix with coronally advanced flap: A randomized clinical split-mouth trial (a 1-year follow-up). Indian J. Dent. Res. 2020, 31, 209–216. [Google Scholar] [CrossRef]
- Matoh, U.; Petelin, M.; Gašperšič, R. Split-mouth comparison of coronally advanced flap with connective tissue graft or collagen matrix for treatment of isolated gingival recessions. Int. J. Periodontics Restor. Dent. 2019, 39, 439–446. [Google Scholar] [CrossRef]
- Cosgarea, R.; Juncar, R.; Arweiler, N.; Lascu, L.; Sculean, A. Clinical evaluation of a porcine acellular dermal matrix for the treatment of multiple adjacent class I, II, and III gingival recessions using the modified coronally advanced tunnel technique. Quintessence Int. 2016, 47, 739–747. [Google Scholar] [CrossRef]
- Rotundo, R.; Genzano, L.; Patel, D.; D’Aiuto, F.; Nieri, M. Adjunctive benefit of a xenogenic collagen matrix associated with coronally advanced flap for the treatment of multiple gingival recessions: A superiority, assessor-blind, randomized clinical trial. J. Clin. Periodontol. 2019, 46, 1013–1023. [Google Scholar] [CrossRef]
- Wiench, R.; Ilków, A.; Gilowski, Ł.; Kulczycka, J.; Stelmańska-Bekus, P.; Skaba, D.; Krzemiński, T.F. Efficacy of coronally advanced flap technique with collagen matrix mucoderm in covering multiple recessions–preliminary results. J. Stomatol. 2018, 71, 478–482. [Google Scholar] [CrossRef]
- Nahas, R.; Gondim, V.; Carvalho, C.V.; Calderero, L.M.; Rosa, E.F.; Sakiyama, T.; Neto, J.B.C.; Pannuti, C.M.; Romito, G.A. Treatment of multiple recessions with collagen matrix versus connective tissue: A randomized clinical trial. Braz. Oral Res. 2019, 33. [Google Scholar] [CrossRef]
- Tarquini, G. Coronally Advanced flap technique to treat class I and II gingival recession in combination with connective tissue graft or equine collagen matrix: A retrospective study. Int. J. Periodontics Restor. Dent. 2017, 37, e217–e223. [Google Scholar] [CrossRef] [PubMed]
- Stefanini, M.; Mounssif, I.; Barootchi, S.; Tavelli, L.; Wang, H.-L.; Zucchelli, G. An exploratory clinical study evaluating safety and performance of a volume-stable collagen matrix with coronally advanced flap for single gingival recession treatment. Clin. Oral Investig. 2020, 24, 3181–3191. [Google Scholar] [CrossRef] [PubMed]
- Pietruska, M.; Skurska, A.; Podlewski, Ł.; Milewski, R.; Pietruski, J. Clinical evaluation of Miller class I and II recessions treatment with the use of modified coronally advanced tunnel technique with either collagen matrix or subepithelial connective tissue graft: A randomized clinical study. J. Clin. Periodontol. 2018, 46, 86–95. [Google Scholar] [CrossRef]
- Ibrahim, M.S.; El-Wassefy, N.A.; Farahat, D.S. Biocompatibility of dental biomaterials. In Biomaterials for Oral and Dental Tissue Engineering; Tayebi, L., Moharamzadeh, K., Eds.; Woodhead Publishing: Waltham, MA, USA, 2017; pp. 117–140. ISBN 9780081009673. [Google Scholar]
- Busra, F.M.; Rajab, N.F.; Tabata, Y.; Saim, A.B.; Idrus, R.B.H.; Chowdhury, S.R. Rapid treatment of full-thickness skin loss using ovine tendon collagen type I scaffold with skin cells. J. Tissue Eng. Regen. Med. 2019, 13, 874–891. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Kim, G.K. Collagen. In High Yield Orthopaedics; Kim, G.K., Ed.; Elsevier: Philadelphia, PA, USA, 2010; pp. 107–109. ISBN 978-1-4160-0236-9. [Google Scholar]
- Kaur, P.; Kakar, V. Collagen: Role in oral tissues: A review. Int. J. Sci. Res. 2014, 3, 1–4. [Google Scholar]
- Silvipriya, K.S.; Kumar, K.K.; Bhat, A.R.; Kumar, B.D.; John, A.; Lakshmanan, P. Collagen: Animal Sources and Biomedical Application. J. Appl. Pharm. Sci. 2015, 5, 123–127. [Google Scholar] [CrossRef]
- Ashraf, F.; Koshy, A.V.; Baldwan, P.; Bakr, M.A. Basics of collagen. Int. J. Curr. Med. Pharm. Res. 2017, 3, 1894–1896. [Google Scholar] [CrossRef]
- Patel, A.; Chapple, I. Periodontal aspects of esthetic dentistry: Managing recession defects. In Essentials of Esthetic Dentistry: Principles and Practice of Esthetic Dentistry; Wilson, N.H.F., Millar, B.J., Eds.; Elsevier: London, UK, 2015; Volume 1, pp. 137–163. ISBN 9780723455585. [Google Scholar]
- Sarlati, F.; Moghaddas, O.; Shabahangfar, R.; Safari, S.; Valaei, N. Inter- and intra-examiner agreement of three classification systems of gingival recession. J. Adv. Periodontol. Implant Dent. 2019, 11, 1–6. [Google Scholar] [CrossRef]
- Chowdhury, S.R.; Mh Busra, M.F.; Lokanathan, Y.; Ng, M.H.; Law, J.X.; Cletus, U.C.; Binti Haji Idrus, R. Collagen type I: A versatile biomaterial. In Novel Biomaterials for Regenerative Medicine, Advances in Experimental Medicine and Biology; Chun, H.J., Ed.; Springer Nature Singapore Pte Ltd.: Singapore, 2018; Volume 1077, pp. 389–414. [Google Scholar]
- Busra, M.F.M.; Lokanathan, Y. Recent development in the fabrication of collagen scaffolds for tissue engineering applications: A review. Curr. Pharm. Biotechnol. 2019, 20, 992–1003. [Google Scholar] [CrossRef]
- Fauzi, M.; Chowdhury, S.R.; Idrus, R.; Aminuddin, B. Fabrication of collagen type I scaffold for skin tissue engineering. Regen. Res. 2014, 3, 60–61. Available online: http://regres.tesma.org.my/index-4.html (accessed on 25 May 2020).
- El-Sayed, K.M.F.; Paris, S.; Becker, S.T.; Neuschl, M.; Buhr, W.; Sälzer, S.; Wulff, A.; Elrefai, M.; Darhous, M.S.; El-Masry, M.; et al. Periodontal regeneration employing gingival margin-derived stem/progenitor cells: An animal study. J. Clin. Periodontol. 2012, 39, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.C.; Martínez, C.; Martínez, J.; McCulloch, C.A. Role of Fibroblast Populations in Periodontal Wound Healing and Tissue Remodeling. Front. Physiol. 2019, 10, 270. [Google Scholar] [CrossRef] [PubMed]
- Mitrano, T.I.; Grob, M.S.; Carrión, F.; Nova-Lamperti, E.; Luz, P.A.; Fierro, F.S.; Quintero, A.; Chaparro, A.; Sanz, A. Culture and characterization of mesenchymal stem cells from human gingival tissue. J. Periodontol. 2010, 81, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.-M.; Liu, X. Advancing biomaterials of human origin for tissue engineering. Prog. Polym. Sci. 2016, 53, 86–168. [Google Scholar] [CrossRef]
- Ramalho, I.; Bergamo, E.; Lopes, A.; Medina-Cintrón, C.; Neiva, R.; Witek, L.; Coelho, P. Periodontal tissue regeneration using brain-derived neurotrophic factor delivered by collagen sponge. Tissue Eng. Part A 2019, 25, 1072–1083. [Google Scholar] [CrossRef]
- Kim, Y.-T.; Wikesjö, U.M.E.; Jung, U.-W.; Lee, J.-S.; Kim, T.-G.; Kim, C.-K. Comparison Between a β-Tricalcium Phosphate and an Absorbable Collagen Sponge Carrier Technology for rhGDF-5–Stimulated Periodontal Wound Healing/Regeneration. J. Periodontol. 2013, 84, 812–820. [Google Scholar] [CrossRef]
- Khan, R.; Khan, M.H. Use of collagen as a biomaterial: An update. J. Indian Soc. Periodontol. 2013, 17, 539–542. [Google Scholar] [CrossRef]
- Naomi, R.; Ratanavaraporn, J.; Fauzi, M.B. Comprehensive review of hybrid collagen and silk fibroin for cutaneous wound healing. Materials. 2020, 13, 3097. [Google Scholar] [CrossRef]
- Tang, L.; Li, N.; Xie, H.; Jin, Y. Characterization of mesenchymal stem cells from human normal and hyperplastic gingiva. J. Cell. Physiol. 2010, 226, 832–842. [Google Scholar] [CrossRef]
- El-Sayed, K.M.F.; Dörfer, M. Gingival mesenchymal stem/progenitor cells: A unique tissue engineering gem. Stem Cells Int. 2016, 2016, 1–16. [Google Scholar] [CrossRef]
- Ballini, A.; Cantore, S.; Scacco, S.; Coletti, D.; Tatullo, M. Mesenchymal stem cells as promoters, enhancers, and playmakers of the translational regenerative medicine 2018. Stem Cells Int. 2018, 2018, 6927401. [Google Scholar] [CrossRef] [PubMed]
- Andrukhov, O.; Behm, C.; Blufstein, A.; Rausch-Fan, X. Immunomodulatory properties of dental tissue-derived mesenchymal stem cells: Implication in disease and tissue regeneration. World J. Stem Cells 2019, 11, 604–617. [Google Scholar] [CrossRef] [PubMed]
- Collins, K.L.; Gates, E.M.; Gilchrist, C.L.; Hoffman, B.D. Bio-Instructive Cues in Scaffolds for Musculoskeletal Tissue Engineering and Regenerative Medicine. In Bio-Instructive Scaffolds for Musculoskeletal Tissue Engineering and Regenerative Medicine; Brown, J.L., Kumbar, S.G., Banik, B.L., Eds.; Elsevier Inc.: Charlottesville, VA, USA, 2017; pp. 3–35. ISBN 978-0-12-803394-4. [Google Scholar]
- Almeida, T.; Valverde, T.; Martins-Júnior, P.; Ribeiro, H.; Kitten, G.; Carvalhaes, L. Morphological and quantitative study of collagen fibers in healthy and diseased human gingival tissues. Rom. J. Morphol. Embryol. 2015, 56, 33–40. Available online: https://pubmed.ncbi.nlm.nih.gov/25826485/ (accessed on 30 May 2020). [PubMed]
- Janjić, K.; Cvikl, B.; Schädl, B.; Moritz, A.; Agis, H. The impact of collagen membranes on 3D gingival fibroblast toroids. BMC Oral Heal. 2019, 19, 48. [Google Scholar] [CrossRef]
- Soni, N.; Sikri, P.; Kapoor, D.; Soni, B.W.; Jain, R. Evaluation of the efficacy of 100% Type-I collagen membrane of bovine origin in the treatment of human gingival recession: A clinical study. Indian J. Dent. 2014, 5, 132–138. [Google Scholar] [CrossRef]
- Marrelli, M.; Maletta, C.; Inchingolo, F.; Alfano, M.; Tatullo, M. Three-point bending tests of zirconia core/veneer ceramics for dental restorations. Int. J. Dent. 2013, 2013, 831976. [Google Scholar] [CrossRef]
- Ausenda, F.; Rasperini, G.; Acunzo, R.; Gorbunkova, A.; Pagni, G. New perspectives in the use of biomaterials for periodontal regeneration. Materials 2019, 12, 2197. [Google Scholar] [CrossRef]
- Marrazzo, P.; Paduano, F.; Palmieri, F.; Marrelli, M.; Tatullo, M. Highly efficient in vitro reparative behaviour of dental pulp stem cells cultured with standardised platelet lysate supplementation. Stem Cells Int. 2016, 2016, 7230987. [Google Scholar] [CrossRef]
- Tóth, B.B.; Arianti, R.; Shaw, A.; Vámos, A.; Veréb, Z.; Póliska, S.; Győry, F.; Bacsó, Z.; Fésüs, L.; Kristóf, E. FTO intronic SNP strongly influences human neck adipocyte browning determined by tissue and PPARγ specific regulation: A transcriptome analysis. Cells 2020, 9, 987. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef]
- Grewal, A.; Kataria, H.; Dhawan, I. Literature search for research planning and identification of research problem. Indian J. Anaesth. 2016, 60, 635–639. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Savović, J.; Page, M.J.; Sterne, J.A. Revised Cochrane Risk of Bias Tool for Randomized Trials (RoB 2.0). 2016, pp. 1–52. Available online: https://www.unisa.edu.au/contentassets/72bf75606a2b4abcaf7f17404af374ad/rob2-0_indiv_main_guidance.pdf (accessed on 6 July 2020).
- Ashworth, J.C.; Mehr, M.; Buxton, P.G.; Best, S.M.; Cameron, R.E. Optimising collagen scaffold architecture for enhanced periodontal ligament fibroblast migration. J. Mater. Sci. Mater. Med. 2018, 29, 1–66. [Google Scholar] [CrossRef] [PubMed]
- Cole, D.J.; Payne, M.C.; Ciacchi, L.C. Water structuring and collagen adsorption at hydrophilic and hydrophobic silicon surfaces. Phys. Chem. Chem. Phys. 2009, 11, 11395–11399. [Google Scholar] [CrossRef] [PubMed]
- Soheilifar, S.; Bidgoli, M.; Faradmal, J.; Soheilifar, S. Effect of periodontal dressing on wound healing and patient satisfaction following periodontal flap surgery. J. Dent. (Tehran Iran) 2015, 12, 151–156. [Google Scholar]
- Khoswanto, C.; Arijani, E.; Soesilawati, P. Cytotoxicity test of 40, 50 and 60% citric acid as dentin conditioner by using MTT assay on culture cell line. Dent. J. (Majalah Kedokt. Gigi) 2008, 41, 103–106. [Google Scholar] [CrossRef]
- Ma, L.; Gao, C.; Mao, Z.; Zhou, J.; Shen, J.; Hu, X.; Han, C. Collagen/chitosan porous scaffolds with improved biostability for skin tissue engineering. Biomaterials 2003, 24, 4833–4841. [Google Scholar] [CrossRef]
- Raita, Y.; Komatsu, K.; Hayakawa, T. Pilot study of gingival connective tissue responses to 3-dimensional collagen nanofiber-coated dental implants. Dent. Mater. J. 2015, 34, 847–854. [Google Scholar] [CrossRef]
- Chen, C.-Y. Novel Nano-Engineered Titanium Surface for Direct Connective Tissue Attachment. Bachelor’s Thesis, Harvard School of Dental Medicine, Boston, MA, USA, 25 April 2019. [Google Scholar]
- Das, S.; Gurav, S.; Soni, V.; Ingle, A.; Mohanty, B.S.; Chaudhari, P.; Bendale, K.; Dholam, K.; Bellare, J.R. Osteogenic nanofibrous coated titanium implant results in enhanced osseointegration: In vivo preliminary study in a rabbit model. Tissue Eng. Regen. Med. 2018, 15, 231–247. [Google Scholar] [CrossRef]
- Polo-Corrales, L.; Latorre-Esteves, M.; Ramirez-Vick, J.E. Scaffold design for bone regeneration. J. Nanosci. Nanotechnol. 2014, 14, 15–56. [Google Scholar] [CrossRef]
- Nakada, A.; Shigeno, K.; Sato, T.; Kobayashi, T.; Wakatsuki, M.; Uji, M.; Nakamura, T. Manufacture of a weakly denatured collagen fiber scaffold with excellent biocompatibility and space maintenance ability. Biomed. Mater. 2013, 8, 45010. [Google Scholar] [CrossRef]
- Thoma, D.S.; Zeltner, M.; Hilbe, M.; Hämmerle, C.H.F.; Hüsler, J.; Jung, R.E. Randomized controlled clinical study evaluating effectiveness and safety of a volume-stable collagen matrix compared to autogenous connective tissue grafts for soft tissue augmentation at implant sites. J. Clin. Periodontol. 2016, 43, 874–885. [Google Scholar] [CrossRef] [PubMed]
- Madaghiele, M.; Calò, E.; Salvatore, L.; Bonfrate, V.; Pedone, D.; Frigione, M.; Sannino, A. Assessment of collagen crosslinking and denaturation for the design of regenerative scaffolds. J. Biomed. Mater. Res. Part A 2015, 104, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Wang, X.; Zhou, H.; Zhang, C.; Wang, Y.; Huang, J.; Liu, M.; Yang, P.; Song, A. Enhancement of periodontal tissue regeneration by conditioned media from gingiva-derived or periodontal ligament-derived mesenchymal stem cells: A comparative study in rats. Stem Cell Res. Ther. 2020, 11, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Menicanin, D.; Gronthos, S.; Bartold, P. Stem cells, tissue engineering and periodontal regeneration. Aust. Dent. J. 2013, 59, 117–130. [Google Scholar] [CrossRef]
- Yoo, S.-Y.; Lee, J.-S.; Cha, J.-K.; Kim, S.-K.; Kim, C.-S. Periodontal healing using a collagen matrix with periodontal ligament progenitor cells in a dehiscence defect model in beagle dogs. J. Periodontal Implant. Sci. 2019, 49, 215–227. [Google Scholar] [CrossRef]
- Seciu, A.-M.; Craciunescu, O.; Zărnescu, O. Advanced regenerative techniques based on dental pulp stem cells for the treatment of periodontal disease. In Periodontology and Dental Implantology; Manakil, J., Ed.; IntechOpen: London, UK, 2019; ISBN 978-1-83881-785-5. [Google Scholar]
- Masci, V.L.; Taddei, A.R.; Gambellini, G.; Giorgi, F.; Fausto, A.M. Ultrastructural investigation on fibroblast interaction with collagen scaffold. J. Biomed. Mater. Res. Part A 2015, 104, 272–282. [Google Scholar] [CrossRef]
- Milinkovic, I.; Aleksic, Z.; Jankovic, S.; Popović, O.; Bajic, M.; Cakic, S.; Lekovic, V. Clinical application of autologous fibroblast cell culture in gingival recession treatment. J. Periodontal Res. 2014, 50, 363–370. [Google Scholar] [CrossRef]
- Schmitt, C.M.; Moest, T.; Lutz, R.; Wehrhan, F.; Neukam, F.W.; Schlegel, K.A. Long-term outcomes after vestibuloplasty with a porcine collagen matrix (Mucograft®) versus the free gingival graft: A comparative prospective clinical trial. Clin. Oral Implants Res. 2016, 27, e125–e133. [Google Scholar] [CrossRef]
- Schmitt, C.M.; Tudor, C.; Kiener, K.; Wehrhan, F.; Schmitt, J.; Eitner, S.; Agaimy, A.; Schlegel, K.A. Vestibuloplasty: Porcine collagen matrix versus free gingival graft: A clinical and histologic study. J. Periodontol. 2013, 84, 914–923. [Google Scholar] [CrossRef]
- Cieślik-Wegemund, M.; Wierucka-Młynarczyk, B.; Tanasiewicz, M.; Gilowski, Ł. Tunnel technique with collagen matrix compared with connective tissue graft for treatment of periodontal recession: A randomized clinical trial. J. Periodontol. 2016, 87, 1436–1443. [Google Scholar] [CrossRef]
- O’Brien, F.J. Biomaterials & scaffolds for tissue engineering. Mater. Today 2011, 14, 88–95. [Google Scholar] [CrossRef]
- Waddington, R.J.; Jones, S.Q.; Moseley, R. Assessing the potential of Mesenchymal stem cells in craniofacial bone repair and regeneration. In Tissue Engineering and Regeneration in Dentistry: Current Strategies; Waddington, R.J., Sloan, A.J., Eds.; Wiley-Blackwell: Wales, UK, 2016; ISBN 9781118741078. [Google Scholar]
- Fraley, S.I.; Feng, Y.; Krishnamurthy, R.; Kim, D.-H.; Celedon, A.; Longmore, G.D.; Wirtz, D. A distinctive role for focal adhesion proteins in three-dimensional cell motility. Nat. Cell Biol. 2010, 12, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, R.S.; Awwadi, M.R.; Moatazed, S.; Rezaei, F.; Hajisadeghi, S. Comparison of acidic and neutral PH root conditioners prior to a coronally positioned flap to treat gingival recession. Dent. Res. J. (Isfahan) 2014, 11, 309–315. [Google Scholar]
- Murray, P. Biocompatibility of biomaterials for dental tissue repair. In Biocompatibility of Dental Biomaterials; Shelton, R., Ed.; Woodhead: West Midlands, UK, 2017; pp. 41–62. ISBN 9780081009437. [Google Scholar]
- Antoine, E.E.; Vlachos, P.P.; Rylander, M.N. Review of collagen I hydrogels for bioengineered tissue microenvironments: Characterization of mechanics, structure, and transport. Tissue Eng. Part B:Rev. 2014, 20, 683–696. [Google Scholar] [CrossRef] [PubMed]
- Zaky, S.H.; Yoshizawa, S.; Sfeir, C. Nanomaterials for dental and craniofacial tissue engineering. In Nanomaterials in Tissue Engineering: Fabrication and Applications; Gaharwar, A.K., Sant, S., Hancock, M.J., Hacking, S.A., Eds.; Woodhead Publishing: Waltham, MA, USA, 2013; pp. 415–432. ISBN 9780857095961. [Google Scholar]
- Brauer, E.; Lippens, E.; Klein, O.; Nebrich, G.; Schreivogel, S.; Korus, G.; Duda, G.N.; Petersen, A. Collagen fibrils mechanically contribute to tissue contraction in an in vitro wound healing scenario. Adv. Sci. 2019, 6, 1801780. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, J.; Blume, M.; Barbeck, M.; Teiler, A.; Kirkpatrick, C.J.; Sader, R.A.; Ghanaati, S. Expansion of the peri-implant attached gingiva with a three-dimensional collagen matrix in head and neck cancer patients–results from a prospective clinical and histological study. Clin. Oral Investig. 2016, 21, 1103–1111. [Google Scholar] [CrossRef]
- Castillo-Briceño, P.; Bihan, D.; Nilges, M.; Hamaia, S.; Meseguer, J.; García-Ayala, A.; Farndale, R.W.; Mulero, V. A role for specific collagen motifs during wound healing and inflammatory response of fibroblasts in the teleost fish gilthead seabream. Mol. Immunol. 2011, 48, 826–834. [Google Scholar] [CrossRef]
- Boilard, E.; Nigrovic, P.A.; Larabee, K.; Watts, G.F.M.; Coblyn, J.S.; Weinblatt, M.E.; Massarotti, E.M.; Remold-O’Donnell, E.; Farndale, R.W.; Ware, J.; et al. Platelets amplify inflammation in arthritis via collagen-dependent microparticle production. Science 2010, 327, 580–583. [Google Scholar] [CrossRef]
- Huang, J.-P.; Liu, J.-M.; Wu, Y.-M.; Chen, L.-L.; Ding, P.-H. Efficacy of xenogeneic collagen matrix in the treatment of gingival recessions: A systematic review and meta-analysis. Oral Dis. 2018, 25, 996–1008. [Google Scholar] [CrossRef]
- Mariani, E.; Lisignoli, G.; Borzì, R.M.; Pulsatelli, L. Biomaterials: Foreign bodies or tuners for the immune response? Int. J. Mol. Sci. 2019, 20, 636. [Google Scholar] [CrossRef]
- Spagnuolo, G.; De Vito, D.; Rengo, S.; Tatullo, M. COVID-19 outbreak: An overview on dentistry. Int. J. Environ. Res. Public Heal. 2020, 17, 2094. [Google Scholar] [CrossRef] [PubMed]
- Bhanushali, P.; Katge, F.; Deshpande, S.; Chimata, V.K.; Shetty, S.; Pradhan, D. COVID-19: Changing trends and its impact on future of dentistry. Int. J. Dent. 2020, 2020, 8817424. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Aim | Study Design | Type of Subject | Findings | Conclusion |
|---|---|---|---|---|---|
| Rosdiani et al. [11] | To develop a Col-chitosan-glycerol scaffold for gingival recession | In vitro | Not applicable | -Scaffold thickness ranges from 0.412 mm to 0.515 mm. -Scaffold pore size ranges from 102.4 μm to 143.5 μm. -Tensile strength of the scaffold ranges from 0.46 MPa to 2.36 MPa. -The swelling ratio of the scaffold was recorded at 413.9%, 801.91%, 1021.78%, and 1354.04%. -Addition of Col contributes to the increase of tensile strength. | The developed Col-based scaffold can be used as alternative treatment in means of biomaterial for gingival recession thanks to its excellent physical properties. |
| Nurfriana et al. [12] | To test the effect of Col-chitosan-glycerol scaffold for gingival recession | In vitro | Not applicable | -The scaffold thickness ranges from 0.51 mm to 0.65 mm. -The pore size of the scaffold ranges from 66.29 μm to 191.7 μm. -Swelling ratio achieved equilibrium point at the 7th minute and starts to reduce from the 8th day onwards. -100% of degradation of the scaffold was observed on day 14. -Addition of Col decreases the tensile value. -Low cytotoxicity level was seen with BHK-21 fibroblast cells. ->50% of cell viability was observed. | The developed scaffold meets the criteria for gingival recession application. |
| Author | Aim | Study Design | Type of Subject | Findings | Conclusion |
|---|---|---|---|---|---|
| Hatayama et al. [13] | To evaluate the efficacy of Col scaffold with different pH for gingival tissue regeneration | In vivo | 9 beagle dogs | -Absence signs of inflammation at the wound site. -Increase thickness of submucosal and epithelial tissue was seen upon implanting Col scaffold. -Col scaffold with pH 7.4 shows the highest rate of tissue regeneration. | Col scaffold with a pH of 7.4 is well suited for gingival tissue regeneration. |
| Schmitt et al. [14] | To compare the effectiveness of porcine Col matrix with a subepithelial connective tissue graft (SCTG) for thickening of gingival | In vivo | 8 beagle dogs | -Thickness of CT was recorded in the mean range of 1.06 mm ± 0.27 mm for Col matrix group, while at 1.32 mm ± 0.44 mm for the SCTG group. -Papillary indentation was deeper in the SCTG group compared with the Col matrix group. -Expression of Col-I and VEGF for Col matrix group was 30.57% ± 7.83% and 37.15% ± 9.80%, respectively, while for SCTG, it was 32.64% ± 7.09% and 39.06% ± 7.27%, respectively. | Col matrix is inferior for thickening of gingival soft tissue compared with SCTG. |
| Shirakata et al. [15] | To compare the effectiveness of coronally advanced flap and porcine acellular dermal matrix (PADM) in GR | In vivo | 12 beagle dogs | -PADM shows complete healing with absence of adverse effects in five sites with -PADM shows an increase in soft tissue thickness and height, dense Col fibers, and formation of bone. | PADM is effective in treating Miller class II GR. |
| Cha et al. [16] | To assess the effectiveness of fibroblast growth factor 2 (FGF-2) incorporated with porcine Col matrix | In vivo | 5 mongrel dogs | -After 16 weeks, the recession area was 4.92 ± 1.05 mm2. -40% of complete root coverage was seen in the test group. -Increase in soft tissue thickness and formation of bone and cementum was observed in the treated group. | The combination promotes rapid healing of GR. |
| Author | Aim | Study Design | Type of Subject | Follow Up Duration | Findings | Conclusion |
|---|---|---|---|---|---|---|
| Barakat et al. [17] | To evaluate the outcome of Col matrix integrated with coronally advanced flap for treating Miller class II GR | Clinical trial | 20 patients | 3 month, 6 month, and 12 month | -Mean reduction in recession depth was 0.20 ± 0.37 in the test group. -Increased of probing depth and width of keratinised tissue was 1.42 ± 0.41 and 3.53 ± 0.82, respectively, in the test group. | Combination of Col matrix with coronally advanced flap effective in treating GR and integration of Col matrix prevent the need for secondary surgery. |
| Matoh et al. [18] | To compare the clinical outcome between CTG and Col matrix in GR patients | Clinical trial | 10 patients | 6 month and 12 month | -The mean root closure in Col matrix group was 85% ± 24%, while it was 100 in CTG group. -Increase in height of keratinised tissue height is lower in Col matrix compared with the CTG group. | Col matrix is less effective in treating GR compared with the CTG. |
| Cosgarea et al. [19] | To assess the effectiveness of PADM in Miller class I, II, and III GR | Clinical trial | 12 patients | 6 month and 12 month | -Improvement of mean root coverage of 73.20 ± 27.71%. -Complete root coverage was >40%. -Reduction in recession depth in maxilla and mandible was 2.51 ± 1.15 and 1.57 ± 1.02, respectively. -Reduction in recession width was 2.92 ± 1.68 and 1.23 ± 1.16 in maxilla and mandible, respectively. -Increase of 0.82 ± 0.72 and 0.87 ± 0.75 for maxilla and mandible, respectively, in attached gingiva was seen. -Keratinised tissue deposition was increase in maxilla and mandible was 0.76 ± 0.51 and 0.62 ± 0.49, respectively. -Probing depth was 1.00 ± 0.00 and 1.20 ± 0.05 for maxilla and mandible, respectively. | PADM is effective for treating Miller class I, II, and III GR. |
| Rotundo et al. [20] | To evaluate the outcome in combination of Col matrix and coronally advanced flap for GR | Clinical trial | 24 patients | 3 month, 6 month, 12 month, and 1 year | -Mean reduction in the recession depth was 2.0 ± 0.8 mm in the test group, while it was 2.0 ± 1.1 mm in the control group. -63% of complete root coverage was achieved in the test group. -> 95% increase in gingival thickness was seen in the test group. | -Combination of Col matrix with coronally advanced flap proven effective in treating GR. |
| Wiench et al. [21] | To evaluate the effectiveness of Col matrix incorporation with coronally advanced flap for Miller class I and II GR | Clinical trial | 12 patients | 3 month and 6 month | -Mean reduction in recession depth and width was 0.5 ± 0.6 and 1.4 ± 1.2. -Mean reduction in recession area was 0.6 ± 0.8. -Mean increase of 3.4 ± 0.9 in keratinised tissue width. -The mean reduction between cement enamel junction and mucogingival junction was 4.4 ± 1.1. -Average root coverage was 87% with a complete root coverage of 47%. | Col matrix incorporated with coronally advanced flap is effective in treating Miller class I and II GR. |
| Nahas et al. [22] | To evaluate the outcome of Col matrix vs. CTG in Miller class I GR | Clinical trial | 15 patients | 3 month, 6 month, and 12 month | -The mean decrease in recession depth and probing depth was 2.7 mm ± 1.1 mm and 1.1 mm ± 0.4 mm, respectively. -The mean increase of keratinised tissue width was 2.2 mm ± 1.0 mm. -Root coverage was >77% with 60% of complete root coverage. | Both Col matrix and CTG promote healing in GR. |
| Tarquini [23] | To test the efficacy of equine Col matrix incorporated with coronally advanced flap for gingival recession | Clinical trial | 50 patients | 1 year | -The probing depth, recession depth, and width of keratinized tissue for both are 1.00 mm ± 0.40 mm, 0.15 mm ± 0.37 mm, and 3.38 mm ± 0.57 mm, respectively, for the equine Col matrix group. -For recession type I, the Col matrix group shows keratinized tissue width of 3.56 mm ± 3.50 mm, probing depth of 0.94 mm ± 0.42 mm, and a recession depth of 0.11 mm ± 0.12 mm. -For recession type II, the Col matrix group shows keratinized tissue width of 3.00 mm ± 0.53 mm, probing depth of 1.13 mm ± 0.35 mm, and a recession depth of 0.25 mm ± 0.46 mm. -Average root coverage for equine Col matrix group was 94.2% ± 14.7% with a complete root coverage of 84.6%. | Equine Col matrix can be used to treat GR. |
| Stefanini et al. [24] | To test the efficiency of volume stable Col matrix (VCMX) in addition of coronally advanced flap for gingival recession | Clinical trial | 10 patients | 6 month and 12 month | -VCMX possesses the ability to soak up blood with a high elasticity. -20% of the subjects showed incomplete wound closure. -96.7 ± 10.4% of root coverage was recorded. -Recession depth shows a mean range of 0.1 mm ± 0.3 mm. -Recession width was recorded in the mean range of 0.3 mm ± 0.9 mm. -Probing depth mean was seen in the mean range of 1.9 mm ± 0.6 mm. -Keratinized tissue width was observed in the mean range of 2.2 mm ± 0.6 mm. -Thickness of gingival was seen in the mean range of 1.3 mm ± 0.4 mm. -Increase in the VCMX dimension contributes to the closure of the wound. -Absence of bleeding, pus, abscess, and fistula was observed. | Volume stable Col matrix is an effective method to treat gingival recession. |
| Pietruska et al. [25] | To compare the effectiveness of coronal tunnel technique that has been modified with subepithelial connective tissue (SCTG) and Col matrix for gingival recession | Clinical trial | 20 patients | 6 month and 12 month | -Gingival recession height in Col matrix side was reduced from 1.95 mm ± 0.76 mm to 0.95 mm ± 0.79 mm, while for SCTG, it was from 1.94 mm ± 0.66 mm to 0.40 mm ± 0.69mm. -Mean root coverage for Col matrix was 53.2%, while for SCTG, it was 83.1%. -20% of complete root coverage was achieved with Col matrix, while it was 67% with SCTG. -Col matrix shows a reduction in recession width from 2.97 mm ± 0.75 mm to 2.08 mm ± 1.30 mm, while in SCTG, it was from 0.76 mm ± 0.31 mm to 1.86 mm ± 0.48 mm. -Col matrix exhibits a statistical different of 1.1 mm with clinical attachment level, compared with SCTG, which is 1.54 mm. -Increased keratinized tissue was seen with Col matrix, from 1.38 mm ± 0.68 mm to 1.91 mm ± 0.84 mm, while for SCTG, it was from 1.28 mm ± 0.72 mm to 4.06 mm ± 1.59 mm. -Gingival thickness for Col matrix side was 1.10 mm ± 0.37 mm, while for SCTG, it was 1.86 mm ± 0.48 mm. -No changes seen in probing depth in either procedure. -10% complete coverage of gingival recession was achieved with Col matrix, while it was 45% for SCTG. -Signs of inflammation with extended healing were seen in two patients. | Col matrix is less effective compared with SCTG for gingival recession. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naomi, R.; Ardhani, R.; Hafiyyah, O.A.; Fauzi, M.B. Current Insight of Collagen Biomatrix for Gingival Recession: An Evidence-Based Systematic Review. Polymers 2020, 12, 2081. https://doi.org/10.3390/polym12092081
Naomi R, Ardhani R, Hafiyyah OA, Fauzi MB. Current Insight of Collagen Biomatrix for Gingival Recession: An Evidence-Based Systematic Review. Polymers. 2020; 12(9):2081. https://doi.org/10.3390/polym12092081
Chicago/Turabian StyleNaomi, Ruth, Retno Ardhani, Osa Amila Hafiyyah, and Mh Busra Fauzi. 2020. "Current Insight of Collagen Biomatrix for Gingival Recession: An Evidence-Based Systematic Review" Polymers 12, no. 9: 2081. https://doi.org/10.3390/polym12092081
APA StyleNaomi, R., Ardhani, R., Hafiyyah, O. A., & Fauzi, M. B. (2020). Current Insight of Collagen Biomatrix for Gingival Recession: An Evidence-Based Systematic Review. Polymers, 12(9), 2081. https://doi.org/10.3390/polym12092081