1. Introduction
Repairing three-dimensional (3D) defects is a challenging part in maxillofacial surgery. Such defects can occur for many reasons, e.g., after surgical resections of pathological lesions such as cysts or tumors or after traumatic events such as traffic accidents or violent crimes. In this context, with about 40%, the lower jaw represents the highest occurrence of all facial fractures in the maxillofacial field [
1]. In Germany, more than 10,000 facial mouth/jaw surgeries are operated annually, and treatment times are up to 14 h [
2]. The reconstruction of maxillofacial defects is clinically important because if they are not restored, defects variable in size and form remain and might cause disfigurements and/or functional impairments. Such reconstructions always involve surgery and a patient-specific treatment plan [
3].
The use of autologous bone is still the first choice in the restoration of any kind of bone defect. Autologous bone can be harvested as a vascularized or non-vascularized graft from a donor site in the same surgical procedure with the defect reconstruction. Although the autologous bone is regarded as the reconstruction gold standard for bone defects, the harvesting procedure can be time-consuming, adding additional operation time and a donor site morbidity that can cause surgery-related complications, which are exhausting for the surgeon and the patient. Furthermore, autologous bone harvesting can be impossible in medical cases where a donor site offering an adequate amount of bone is absent or simply not accessible because of general medical reasons such as bad health conditions of the patient [
4]. As an alternative to autologous bone grafts, alloplastic (synthetic) materials can be used to reconstruct defects. Alloplastic materials can be formed as implants intraoperatively by the surgeon or virtually planned and customized, manufactured preoperatively according to patient-specific aspects. Commonly used alloplastic materials include metals such as titanium and titanium alloys, ceramics such as hydroxyapatite (HA) or polymers such as polyetheretherketone (PEEK) [
5]. Although titanium and titanium alloys are basically biocompatible, they are relatively stiff compared to human bone. However, a bone-like modulus of elasticity is important to prevent stress shielding and/or osteolysis [
6]. Additionally, metal implants are generally highly heat conducting, and thus can cause pain if patients are exposed to environmental temperature variations [
7]. PEEK, on the other hand, provides low heat conduction, but also has a limited accumulation potential for cells: the surrounding bone tissue does not stay entirely healthy on implant surfaces (“halo-effect”) [
8,
9]. Bulk hydroxyapatite, although highly cell-friendly, is not suitable for high load bearing conditions due to its poor mechanical traits [
10].
Since the discipline of maxillofacial surgery, in particular, has undergone a remarkable rate of technological innovation associated with computer assistance in the last two decades [
11], patient-specific implants designed and manufactured using computer-aided design (CAD) and computer-aided manufacturing (CAM) have become a highly clinically relevant part in routine and complex individual surgical cases [
12,
13]. Based on a computer tomography scan (CT) or cone beam computer tomography scan (CBCT) of the patient, implants can be virtually designed using CAD software [
14] and consecutively manufactured. Those services are usually clinic-externally supplied by subtractive manufacturing like milling or by additive manufacturing (AM) like powder bed fusion [
7]. In contrast to AM, the cost- and material-intensive subtractive process employs milling of the 3D model from a material block in a computer numerical controlled (CNC) milling machine. Furthermore, the freedom of implant design for successful milling is limited [
7].
Although the reconstruction of complex bone defects is challenging due to the unique anatomy and the variety of deficits [
4,
5], recent improvements in the field of CAD in combination with a compact and efficient AM could lead to precise patient-specific implants in a very short production time [
11]. Thus, shorter operation times by a clinic-internal, maybe intra-operative implementation of CAD/AM would lead to less patient stress and faster healing. In addition, time-related changes in the bone structure and the extent of the lesion (bone growth) can be addressed. A material adaption to specific patient needs could also be addressed by the surgeon. For the latter demand, the extrusion-based additive manufacturing (“material extrusion” by EN ISO/ASTM 52900, edition 2017) is very promising because of the intrinsic material flexibility. At present, clinical tests of extrusion-based implants, especially internally implemented as an intra-operative option, are still in the early stages. Nevertheless, the research group MAM—Medical Additive Manufacturing, located at the University of Basel, Switzerland, has evaluated the medical approach as very promising [
15,
16,
17]. In contrast, Vaezi et al. [
18] displayed extrusion-based additive manufacturing as still not ready for clinical entry because of insufficient print results.
Hence, the goal of this study was to face the specific problems of the established maxillofacial alloplastic materials (stress shielding, heat conduction, halo-effect, mechanical performance) with an adapted material selection and to combine those materials with the extrusion-based additive manufacturing (on a filament basis) to prove the basic ability of this fabrication approach for the CAD-based reconstruction of maxillofacial defects. This study is based on the preliminary work of additive manufacturing of biofunctional implants for craniomaxillofacial surgery [
7].
2. Materials and Methods
2.1. Material Selection
The implant materials were selected regarding melt flowability, mechanical toughness, mechanical stiffness, and biotoxicity. Enough flowability should allow reliable extrusion and mechanical toughness should deliver filament flexibility. Mechanical stiffness should ensure the form stability of the implant under load. The lack of biotoxicity should avoid inflammation reactions in vivo.
Optimal flowability, displayed by the melt flow rate (MFR), was determined by the evaluation of commercial filament technical data sheets [
19]. The optimal MFR for material extrusion was evaluated between 5 g/10 min and 50 g/10 min. The implant requirement of the mechanical toughness and the mechanical stiffness were investigated for different polymers in previous works of Katschnig et al. [
7,
20]. The main results suggested a composite of a rigid and stiff polymer and a soft and tough polymer. This material hybrid delivered a synergy effect in mechanical tests, especially in the non-linear increase in the impact energy [
7]. These findings can result in a stiff and at the same time tough implant. These data are given in
Table 1. The bioactivity of PETG and TPU was also examined by Katschnig [
7] and is given in
Table 2. Moreover, the positive cell-impact of polyurethane polymers was proposed by J.A. de La Peña-Salcedo et al. [
21]. Following these preliminary works, the final material choice fell on the (hard) thermoplastic polyethylene terephthalate glycol (PETG) as base polymer and the (soft) thermoplastic elastomer polyurethane (TPU) as bioactive polymer. The PETG Mimesis DP300 was supplied by Selenis (Selenis S.A, Portalegre Portugal) and the TPU Polyflex TPU95 was purchased from Polymaker (Polymaker BV, Shanghai, China).
This selection promoted the idea of using TPU outer layers (soft shell) as crack stoppers for PETG-filled (stiff core) implants in the maxillofacial area. At the same time, a TPU shell could have a cell-activating effect. The potential combination of enhanced mechanical performance and bioactive shell forms the potential biofunctionality of the fabricated implant. Extrusion-based AM opens the possibility of producing these biofunctional hybrids in one process step by dual printing.
An Acrylester–Styrol–Acrylnitril (ASA) named ApolloX Natural from Formfutura (Formfutura BV, Nijmegen, The Netherlands) was used for all printed ex-vivo bone models. The material was chosen because of the bone-like colour and good printability.
2.2. Filament Preparation
TPU was purchased in filament form, but PETG was only available as pellets and had to be prepared for filament-based material extrusion by filament extrusion. Payr described important influencing factors in the extrusion of high-quality filaments [
22]. For a polyethylene (PE), a polypropylene (PP) and for a polycarbonate (PC) it was proven that optimal settings for high quality filaments include slow and uniform cooling of the extruded filaments. As a result, filaments could be produced in the range of 1.75 mm ± 0.05 mm in diameter, ±0.05 mm in ovality and without vacuoles. Slow and uniform filament cooling can be done with symmetrical air cooling and a slow draw-off speed. This is achieved, for example, by the table-top 3devo Advanced 1.0 filament extruder (3devo B.V., Utrecht, The Netherlands), which was therefore used for the extrusion of PETG filaments. A further advantage was the easy processing of small raw material batches below 5 kg. The 3devo Advanced 1.0 is equipped with an optical filament diameter measurement, thus has an automated quality control during production.
Table 3 lists the machine specifications.
2.3. Clinical Data Preparation
The anatomical defect localizations were chosen to be clinically relevant and comparable to the surgical routine, e.g., after the surgical resection of tumors and pathologic bone lesions or after expanded traumatic injuries including heavy bone loss.
2.3.1. Maxillofacial Defect Data Source
A physiologically preserved anonymous human cadaver mandible, donated within the “anatomical body donation program” of the Institute for Macroscopic and Clinical Anatomy at the Medical University of Graz, was used to create two comprehensible bone defects in the lower chaw.
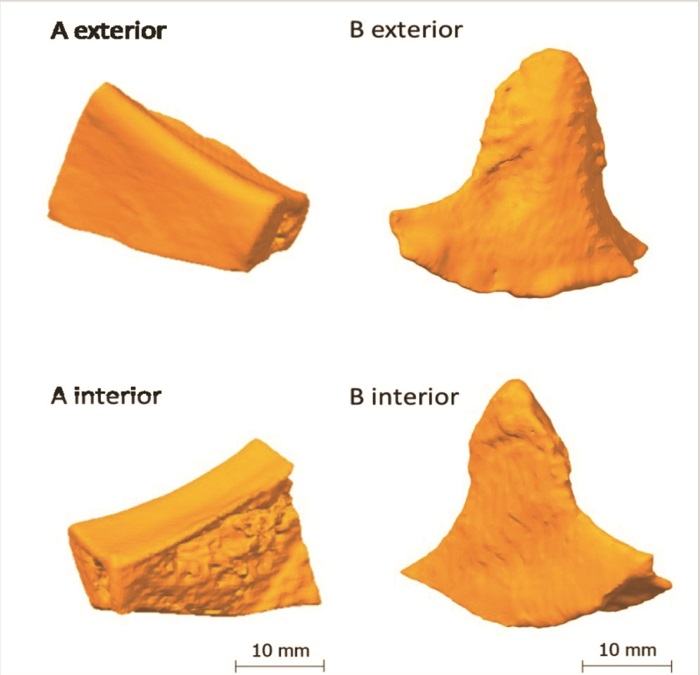
A first bone defect (implant A) was created in the anatomical area of the right mandibular angle (approx. 3.0 cm × 2.0 cm × 1.0 cm), including the right oblique line, cortical bone and the infra-alveolar nerve, as it often occurs after the resection of neoplastic processes that infiltrate the bone. The aim was to digitally scan the defect and the previously resected defect positive. The aim was to achieve the subsequent surgical filling of the defect with a printed replication of the defect positive.
A second bone defect (implant B) was created by the resection of the muscular process (pterygoid process) on the left side of the human mandible (approx. 3.5 cm × 3.0 cm × 1.0 cm), as a potential result of a pathological bone lesion resection or of a congenital missing or malformed anatomical hard tissue structure. The aim was to replicate the second defect, i.e., to “model” the defect positive digitally and then to print the implant.
All defect preparations were done with a commercially available oscillating bone saw and a blade width of 0.8 mm, using water cooling to secure further structures in the mandible cadaver bone.
Regarding the localization of the reconstruction sites for implant A and B, the mandible was chosen for both defect creations because it provided highly complex geometry for additive manufactured implants, a bone to be subject to naturally occurring strong biomedical forces and clinical highly relevant fracture sites [
1,
2,
3].
2.3.2. Imaging of Anatomical Structures
All defects were scanned using the CT scanner Siemens Sensation 64 (Siemens Medical Solutions, Malvern, PA, USA). The scanners are regularly subjected to quality control evaluations; scanning procedures were done with a standard scanning protocol. High-resolution images with an in-plane resolution of 0.98 × 0.98 mm2 of the craniomaxillofacial area and a slice thickness of 1 mm were provided by the Department of Oral and Maxillofacial Surgery (Medical University of Graz, Graz, Austria) in digital imaging and communications in medicine(DICOM) file format.
2.3.3. Segmentation and STL Model Creation
All defects were converted and segmented with the help of Invesalius v3.1 (Campinas, Brazil) a free medical open source software used to generate virtual reconstructions of structures in the human body [
23]. The segmentation was done by bi-level thresholding. The additional modeling of implant B was done with Meshmixer 3.5 (Autodesk Inc., San Rafael, CA, USA).
2.3.4. Post-Processing of the STL Models
Any post-processing of the STL models was performed using 3D Builder (Microsoft Corporation, Redmond, WA, USA) and Meshmixer 3.5 (Autodesk Inc., San Rafael, CA, USA).
2.4. Material Extrusion Machines
For all single extrusion prints, the cartesian industrial printer HAGE3D medmex (HAGE3D GmbH, Graz, Austria) was used. All dual extrusion prints were carried out with the cartesian industrial printer HAGE3D 84L-A (HAGE3D GmbH, Austria).
Table 4 shows the machine specifications.
The medmex machine used an air-cooled direct drive printhead (abbr. SDK) with synchronized profile wheels and mosquito hotends (Slice Engineering, Gainesville, FL, USA). The 84L-A machine used a water-cooled high friction feeding system printhead (abbr. HFFS) with shortened aluminium hot ends for precise melt control.
2.5. Slicing and Print Parameters
All implants and ex-vivo bone models were sliced using the software Simplify3D Version 4.0 (Simplify3D Inc., Cincinnati, OH, USA) with a brass nozzle of 0.4 mm diameter using the settings summarized in
Table 5,
Table 6 and
Table 7. Those settings were based on a previous process development by the author [
7]. The heatable print bed was covered by polyetherimide (PEI) foil. For dual printing, an additional value setting and a tool change script were required and are shown in
Table 8 and
Table 9.
After finalizing the printing job, the printed parts were detached from the cooled down print bed with a spatula and stored under standardized conditions for more than 72 h before subsequent tests were conducted.
2.6. Clinical Evaluation
Defect reconstructions were done ex-vivo with conventional surgical methods as they are also routinely used intraoperatively. The fixation of each implant was done with commercially available osteosynthesis microplates and screws (MedArtis AG, Basel, Switzerland). These plates and screws are also used intraoperatively in the clinical routine in facial reconstructive and bone fixation procedures and can generally remain in the patient without the need of second operation for their removal.
4. Discussion
The main task in this work was to search for alternatives to the established alloplastic implant materials with an adapted material selection and combine those new materials with the extrusion-based additive manufacturing on a filament basis to produce ready-to-use reconstructions of maxillofacial defects. From a manufacturing perspective, this can be affirmed based on the achieved results.
The (STL-) models “implant A” and “implant B”, made by semi-automatic segmentation and defect reconstruction with open source software, delivered a precise adaptation to the region of implantation. The three-dimensional bone contour was well reconstructed. The models had no mesh defects and the slicing was performed smoothly. The model quality was comparable to already presented CAD-based mandible reconstructions [
24,
25].
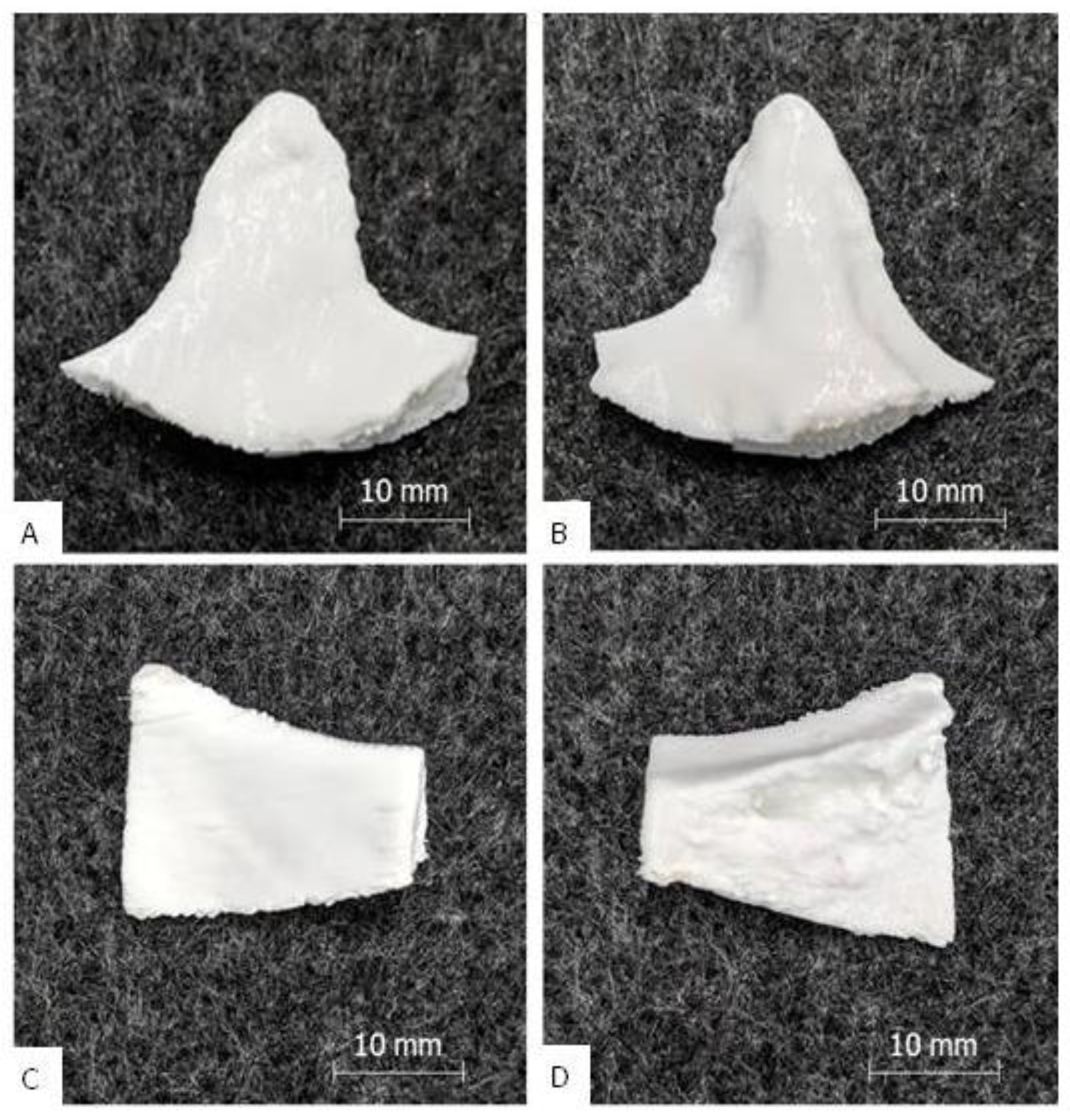
A clean and complete extrusion process could be carried out for both the standard and performance implants. The optimized printing parameters derived from [
7] could be confirmed. In dual printing, the adhesion between the TPU shell and the PETG core seems to be good. The surfaces are homogeneous and have a process-specific resolution (±0.1 mm [
26]). The exceptions were slightly frayed areas on the supported surfaces of the performance implants, which had to be smoothed in post-processing. The reason for the surface damage was probably the good adhesion between the PETG support and the TPU shell, if the defined offsets of 0.3 mm are bypassed by extrusion errors. TPU is known for its increased adhesiveness [
27], so if there is any offset bridging of extruded material, the contact adhesion tends to be strong. In addition, slight traces of overheating in the TPU shell were found. The reason for this may have been a local overheating by tool path-enforced low layer times (<10 s) [
28].
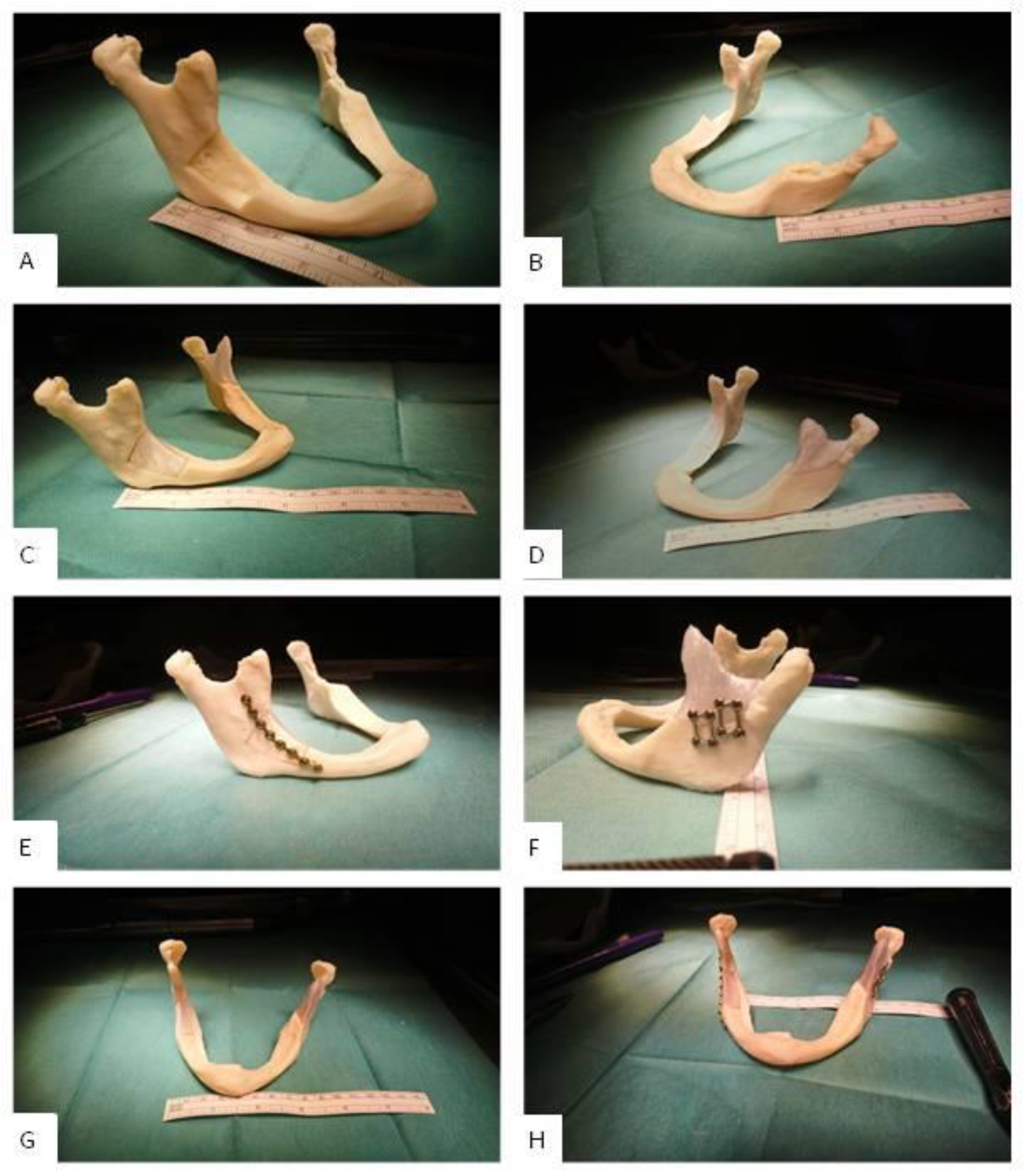
The assembly ability of implant A and B was clinically proven in a printed ex-vivo bone model.
Figure 7 shows a qualitative comparison between an already published result of fitted and mounted PEEK implants that are conventionally available for a clinical use and a fitted and mounted PETG implant A. One can see that the clinical fixation with osteosynthesis microplates and screws possibly does not harm the implants and leads to aesthetically good results. Furthermore, the implant fits to the three-dimensional bone contour.
Every new AM-based patient-specific implant (PSI) fabrication effort must compete with the already established (and often commercialized) technologies and materials. Looking at extrusion-based AM with thermoplastics, the benchmark material is PEEK. PEEK PSIs are used clinically in a wide medical field [
30]. Various studies conducted with PEEK in the reconstruction of maxillofacial defects have shown good postoperative aesthetic and functional results without any complications [
31,
32,
33,
34].
However, there are also reports of PEEK post-operative complications and implant failures [
35,
36], although with better performance compared to titanium meshes [
36], for example, and the difficulty to print PEEK [
37]. From a clinical point of view PEEK PSIs may cause local infection and increased soft tissue scarring due to a limited biocompatible surface, especially in anatomical areas where strong muscles are crossing and moving strong bones, for example in the lower jaw. Furthermore, PEEK is not ideal for dual printing due its high extrusion temperature and consecutively beneficial material composites like hard–soft-combinations, for example, rib replacements and fixtures are not easy to achieve. Moreover, producing compounds with PEEK and bioactive fillers like HA is difficult [
7]. Those disadvantages should motivate researchers to establish other thermoplastics and thermoplastic elastomers as alternatives.
Figure 8 depicts a visual comparison between a maxillofacial PEEK implant and a standard/performance implant B. With the results of this publication and preliminary works of the authors in mind, PETG or TPU as mono material implant or PETG/TPU as material composite are potentially a promising substitute for PEEK.
However, there are some drawbacks in using PETG and TPU instead of PEEK, such as the non-eligibility for autoclave sterilization (ultraviolet radiation sterilization or ethylene oxide sterilization could be alternatives) or the minor load-bearing capability, which must be addressed in further studies. Maxillofacial reconstructions need high-strength implants, especially if there is not enough supporting biological bone structure. This is especially true in the mandible, where the highest forces of the whole maxillofacial complex can occur that are punctually at a maximum average of 700 N in a healthy human. These high-strength forces result from bite forces that influence the bone. However, clinically, for as long as 6 weeks after an operation, bite forces are typically between 0 N and 100 N for incisal edge front loading and between 0 N and 200 N for molar edge rear loading [
38,
39]. Thus, those value ranges represent clinically relevant load limits for the mechanical testing of implants in the maxillofacial complex [
40]. After 6 weeks, the bone healing is known to be biologically stable enough and thus, together with the implant, a biological stability can be achieved [
41,
42]. Another important aspect that needs to be investigated further is the technology-specific mechanical anisotropy in printed parts. This means the part is normally strongest in the direction of the extruding tool path and relatively weaker in the two remaining part axes, vertically to the extruding tool path (layer bonding regions). This anisotropy should be addressed in the slicing strategy considering the in-vivo implant orientation
5. Conclusions and Future Work
The presented technical approach proved to be sufficiently fast, clean, and precise to exactly reconstruct maxillofacial structures ex-vivo. If an intraoperative fabrication is considered or if non-risk patients are clinically involved, a fast in-house printed PETG standard implant could potentially serve as an alternative for maxillofacial bone reconstruction. For patients who are either at risk of implant rejection or high impact stress, the TPU/PETG performance implant is a potential implant solution. It has a TPU shell that is biofunctional and crack-stopping and a PETG core that gives strength. The impact strength is synergistically increased; the risk of fracture and splintering is low. The disadvantage of performance implants is the longer manufacturing time. In summary, standard implants could make second operations obsolete by manufacturing them during surgery and performance implants could compensate for the disadvantages of currently used implant materials such as casual rejection reactions (titanium alloys etc.) or fracture susceptibility (HA etc.).
Concerning the study design, a pre-clinical ex-vivo defect creation and evaluation was done because new fabrication strategies and material combinations (PETG/TPU) were used. An in-vivo study within a clinical setting is planned as a following future work project. However, to reduce this ex-vivo limitation in our study design, we used a physiologically preserved high quality human cadaver (Institute for Macroscopic and Clinical Anatomy, Medical University of Graz), which completely consists of human cellular tissue and naturally simulates a clinical setting regarding geometry and mechanical behavior. The study design of this work was chosen according to previously successfully performed investigations of new methods for a clinical use that suggest a first pre-clinical assessment when new materials or technologies should be introduced as routine procedures in maxillofacial surgery [
1,
40,
43].
In general, the new requirements of the standards ISO 13485:2016 (introduction to quality management for medical devices), VDI 3405 (additive manufacturing processes) and ISO 5832 (implant certification) will pose questions in particular for the additive manufacturing of implants, which need to be answered. The focus of those requirements is on the clinical evaluation of medical devices, post-market surveillance systems and quality management for in-house production in hospitals. The current standards also attach great importance to questions of approval and liability for printed implants [
44]. The central question here will be whether the risk of implant failure due to manufacturing errors can be internalized, i.e., ultimately borne by the medical facility and its employees or whether the risk will continue to be externalized by external service manufacturing. A possible way out would be the separation into emergency medical operations, which require the time savings and flexibility of in-house manufacturing, and standard procedures, which make standardized external manufacturing appear reasonable. Extrusion-based AM, more precisely filament-based material extrusion, will support the flexible, fast and low-cost ready-to-use in-house manufacturing with a compact and clean printing process and the possibility of patient-specific material design. The authors therefore recommend a systematic evaluation of the complete benefit chain from data generating to clinical study of the presented technology including quality documentation and risk management. A successful result would be a relevant and vital step towards the clinical acceptance and potential use of filament-based material extrusion for patient-specific implants in maxillofacial defect reconstruction.

 ,
, 












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}