
Physicochemical Properties of Demineralized Bone Matrix and Calcium Hydroxide Composites Used as Bone Graft Material

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Fabrication of DBM-Ca(OH)2
2.2. X-Ray Diffraction (XRD)
2.3. Atomic Absorption Spectroscopy (AAS)
2.4. Fourier Transform Infrared (FTIR) Spectroscopy
2.5. Scanning Electron Microscope (SEM)—Energy-Dispersive X-Ray Spectroscopy (EDS)
2.6. Statistical Analysis
3. Results
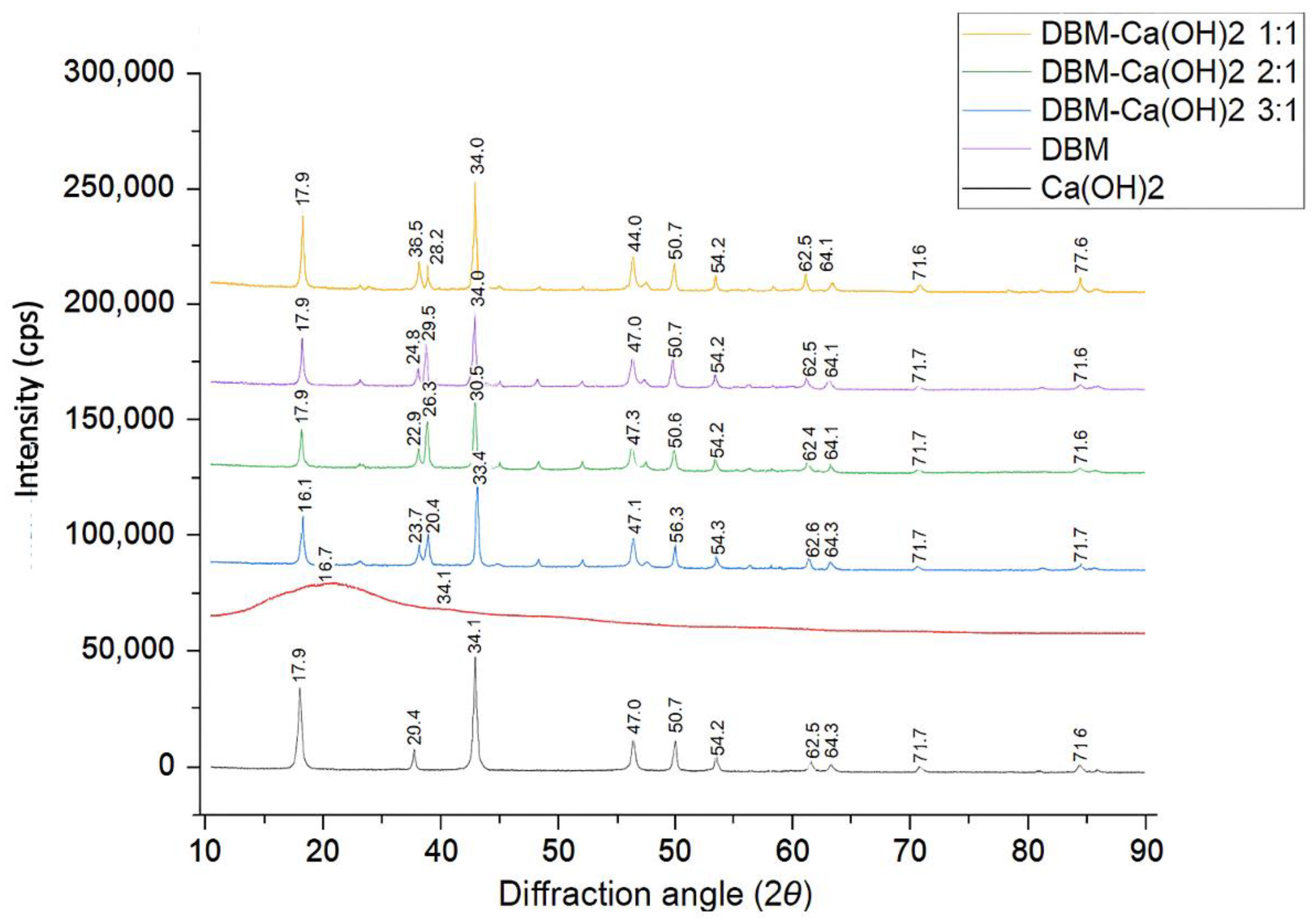
3.1. X-Ray Diffraction (XRD)
3.2. Atomic Absorption Spectroscopy (AAS)
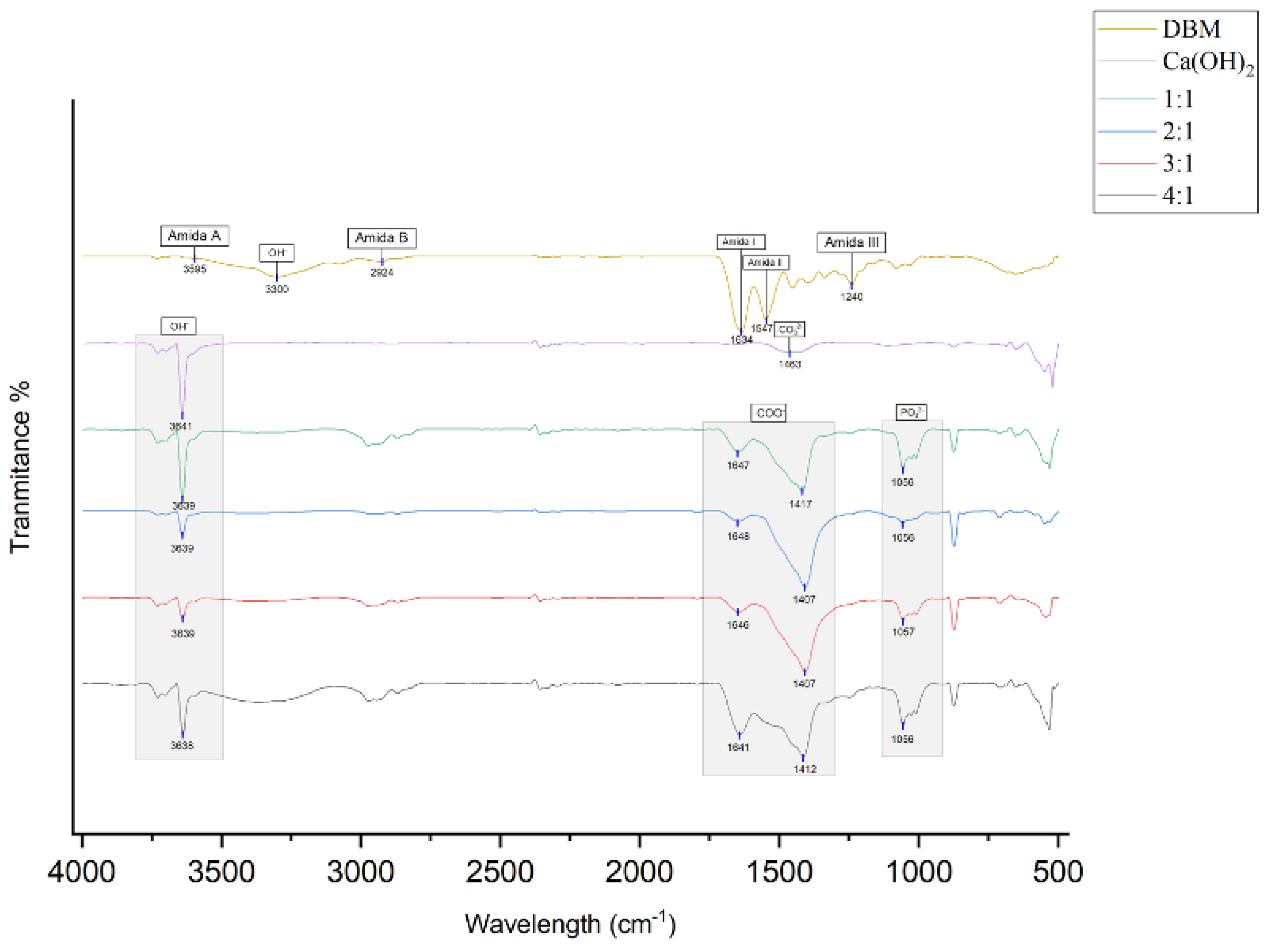
3.3. Fourier Transform Infrared (FTIR) Spectroscopy
- ▪ Amide A (N–H stretching) at 3595 cm−1;
- ▪ Amide B (C–H stretching) at 2924 cm−1;
- ▪ Amide I (C=O stretching) at 1634 cm−1;
- ▪ Amide II (N–H bending) at 1547 cm−1;
- ▪ Amide III (C–N stretching) at 1240 cm−1;
- ▪ OH− at 3300 cm−1.
- ▪ PO43− was detected at ~1056 cm−1 (1057 cm−1 in 3:1 group);
- ▪ COO− bands were observed in the ranges of 1407–1417 cm−1 and 1641–1648 cm−1 across all composite groups, suggesting ionic interaction between Ca2+ and the carboxyl groups in collagen;
- ▪ OH− stretching was present at 3638–3639 cm−1 in all composites.
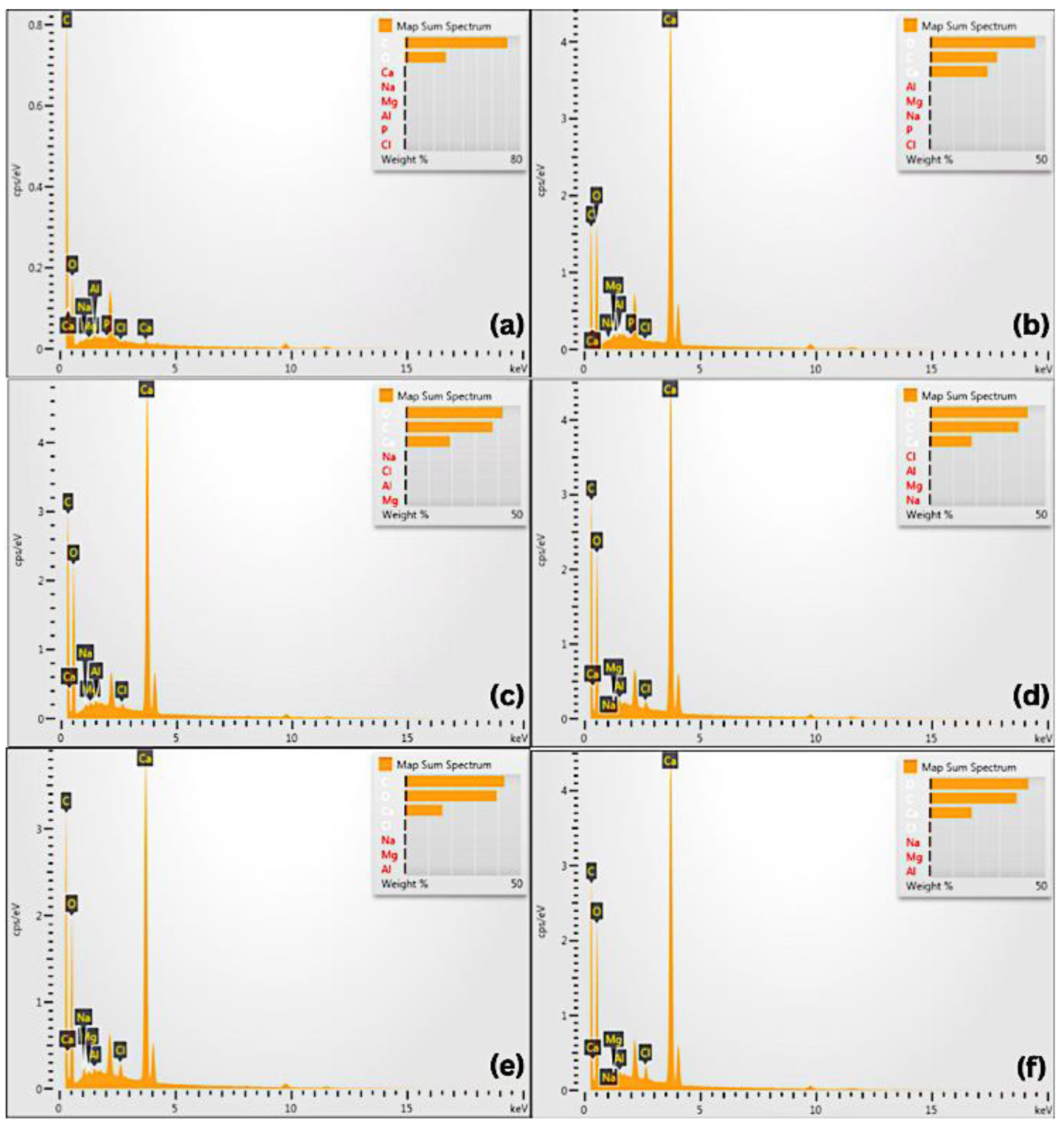
3.4. Scanning Electron Microscope (SEM)—Energy-Dispersive X-Ray Spectroscopy (EDS)
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Nibali, L.; Sultan, D.; Arena, C.; Pelekos, G.; Lin, G.; Tonetti, M. Periodontal infrabony defects: Systematic review of healing by defect morphology following regenerative surgery. J. Clin. Periodontonl. 2021, 48, 100–113. [Google Scholar] [CrossRef] [PubMed]
- Tsuchida, S.; Nakayama, T. Recent clinical treatment and basic research on the alveolar bone. Biomedicines 2023, 11, 843. [Google Scholar] [CrossRef] [PubMed]
- Boehm, T.K.; Clara, S.K. An Overview of Periodontal Surgical Procedures; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Ciszyński, M.; Dominiak, S.; Dominiak, M.; Gedrange, T.; Hadzik, J. Allogenic bone graft in dentistry: A review of current trends and developments. Int. J. Mol. Sci. 2023, 24, 16598. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Q.; Wang, Z.; Zhou, W.; Zhang, L.; Liu, Y.; Xu, Z.; Li, Z.; Zhu, C.; Zhang, X. Bone regeneration materials and their application over 20 years: A bibliometric study and systematic review. Front. Bioeng. Biotechnol. 2022, 10, 921092. [Google Scholar] [CrossRef]
- Wibowo, A.R.; Octarina, O.; Munadziroh, E.; Handharyani, E. The effect of application bovine amniotic membrane on ssteoblasts, osteocytes, and collagen. Padjajaran J. Dent. 2023, 35, 163–169. [Google Scholar] [CrossRef]
- Veremeev, A.; Bolgarin, R.; Nesterenko, V.; Andreev-Andrievskiy, A.; Kutikhin, A. Native bovine hydroxyapatite powder, demineralised bone matrix powder, and purified bone collagen membranes are efficient in repair of critical-sized rat calvarial defects. Materials 2020, 13, 3393. [Google Scholar] [CrossRef]
- Zhang, H.; Yang, L.; Yang, X.-G.; Wang, F.; Feng, J.; Hua, K.; Li, Q.; Hu, Y. Demineralized bone matrix carriers and their clinical applications: An overview. Orthop. Surg. 2019, 11, 725–737. [Google Scholar] [CrossRef] [PubMed]
- Chen, I.-C.; Su, C.-Y.; Lai, C.-C.; Tsou, Y.-S.; Zheng, Y.; Fang, H.-W. Preparation and characterization of moldable demineralized bone matrix/calcium sulfate composite bone graft materials. J. Funct. Biomater. 2021, 12, 56. [Google Scholar] [CrossRef] [PubMed]
- Wen, B.; Freilich, M.; Kuhn, L. Bone Tissue Engineering Around Dental Implants. Stem Cell Biol. Tissue Eng. Dent. Sci. 2015, 55, 749–764. [Google Scholar]
- Cho, H.; Bucciarelli, A.; Kim, W.; Jeong, Y. Natural Sources and Applications of Demineralized Bone Matrix in the Field of Bone and Cartilage Tissue Engineering. Adv. Exp. Med. Biol. 2020, 1249, 3–14. [Google Scholar]
- Sawkins, M.; Bowen, W.; Dhadda, P.; Markides, H.; Sidney, L.; Taylor, A.; Rose, F.; Badylak, S.; Shakesheff, K.; White, L. Hydrogels derived from demineralized and decellularized bone extracellular matrix. Acta Biomater. 2013, 9, 7865–7873. [Google Scholar] [CrossRef] [PubMed]
- Verboket, R.D.; Irrle, T.; Busche, Y.; Schaible, A.; Schröder, K.; Brune, J.C.; Marzi, I.; Nau, C.; Henrich, D. Fibrous demineralized bone matrix (DBM) improves bone marrow mononuclear cell (BMC)-supported bone healing in large femoral bone defects in rats. Cells 2021, 10, 1249. [Google Scholar] [CrossRef] [PubMed]
- Khosropanah, H.; Lashkarizadeh, N.; Ayatollahi, M.; Kaviani, M.; Mostafavipour, Z. The impact of calcium hydroxide on the osteoinductive capacity of demineralized freeze-dried bone allograft: An in-vitro study. J. Dent. Shiraz. Univ. Med. Sci. 2018, 19, 19–27. [Google Scholar]
- Mahajan, A.; Kedige, S. Periodontal bone regeneration in intrabony defects using osteoconductive bone graft versus combination of osteoconductive and osteostimulative bone graft: A comparative study. J. Dent. Res. 2015, 12, 25–30. [Google Scholar] [CrossRef]
- Khorshidi, H.; Raoofi, S.; Sabagh, S.; Behboud, Z.; Mozafari, G.; Ashraf, M. Effect of combined calcium hydroxide and accelerated portland cement on bone formation and soft tissue healing in dog bone lesions. J. Dent. Biomater. 2015, 2, 97–102. [Google Scholar]
- Dhruvakumar, D.; Gupta, C. Role of combination therapy/composite graft in periodontal regeneration: A mini review. Tanta Dent. J. 2017, 14, 169. [Google Scholar] [CrossRef]
- Barus, L.; Septianingtyas, V.; Febriadi, P.B.; Hendra, I.M.; Annis, A.F.; Satria, R.M.H.; Wibisono, N.I.; Pratiwi, E.S.; Rasyida, A.Z.; Mulyawan, I.; et al. Demineralized Freeze-Dried Bovine Bone Xenograft Granules as Alveolar Bone Substitutes: A Profile Study. 2021. Available online: http://www.jidmr.com (accessed on 8 June 2025).
- Coathup, M.; Campion, C.; Blunn, G. A carboxymethyl cellulose bone graft carrier delays early bone healing in an ovine model. J. Biomed. Mater. Res.-Part B Appl. Biomater. 2020, 108, 612–618. [Google Scholar] [CrossRef]
- Chauhan, N.; Lakhkar, N.; Chaudhari, A. Development and physicochemical characterization of novel porous phosphate glass bone graft substitute and in vitro comparison with xenograft. J. Mater. Sci. Mater. Med. 2021, 32, 60. [Google Scholar] [CrossRef]
- Kurniawan, F.L.; Tjandrawinata, R.; Marpaung, C.; Pratiwi, D.; Komariah, K. The effect of horn beetle nanochitosan (Xylotrupes gideon) addition on the hardness of glass-ionomer cement. J. Indones. Dent. Assoc. 2022, 5, 27–31. [Google Scholar] [CrossRef]
- Livia, F.; Tjandrawinata, R.; Marpaung, C.D.; Pratiwi, D.; Komariah, K. The effect of horn beetle nano chitosan (Xylotrupes gideon) on the surface roughness of glass-ionomer cement. Mater. Sci. Forum. 2022, 1069, 161–166. [Google Scholar] [CrossRef]
- Ali, A.; Chiang, Y.W.; Santos, R.M. X-ray diffraction techniques for mineral characterization: A review for engineers of the fundamentals, applications, and research firections. Minerals 2022, 12, 205. [Google Scholar] [CrossRef]
- Khan, H.; Yerramilli, A.S.; D’Oliveira, A.; Alford, T.L.; Boffito, D.C.; Patience, G.S. Experimental methods in chemical engineering: X-ray diffraction spectroscopy—XRD. Can. J. Chem. Eng. 2020, 98, 1255–1266. [Google Scholar] [CrossRef]
- Filio, P.; Octarina, F.; Komariah, F. Characterization of fabricated bovine hydroxyapatite crystal as socket preservation material: An SEM-EDX and x-ray diffraction study. World J. Dent. 2022, 13 (Suppl. S2), S175–S181. [Google Scholar] [CrossRef]
- Filho, H.J.I.; Salazar, R.F.S.; Capri, M.R.; Neto, A.C.; Alcantara, M.A.K.; Peixoto, A.L.C. State-of-the-art and trends in atomic absorption spectrometry. In Atomic Absorption Spectroscopy; InTech: Houston, TX, USA, 2012; pp. 13–36. [Google Scholar]
- Berna, F. Encyclopedia of Geoarchaeology; Springer: Dordrecht, The Netherlands, 2017. [Google Scholar]
- Nam, J.-W.; Kim, M.-Y.; Han, S.-J. Cranial Bone Regeneration According to Different Particle Sizes and Densities of Demineralized Dentin Matrix in The Rabbit Model. Maxillofac. Plast. Reconstr. Surg. 2016, 38, 27. [Google Scholar] [CrossRef]
- Charlena, C.; Maddu, A.; Hidayat, T. Synthesis and Characterization of hydroxyapatite from green mussel shell with sol-gel method. J. Kim. Val. 2022, 8, 269–279. [Google Scholar] [CrossRef]
- Widjonarko, N.E. Introduction to advanced x-ray diffraction techniques for polymeric thin films. Coatings 2016, 6, 54. [Google Scholar] [CrossRef]
- Dozza, B.; Lesci, I.G.; Duchi, S.; Della Bella, E.; Martini, L.; Salamanna, F.; Falconi, M.; Cinotti, S.; Fini, M.; Lucarelli, E.; et al. When size matters: Differences in demineralized bone matrix particles affect collagen structure, mesenchymal stem cell behaviour, and osteogenic potential. J. Biomed. Mater. Res. 2017, 105, 1019–1033. [Google Scholar] [CrossRef]
- Nicoletti, A.; Torricelli, P.; Bigi, A.; Fornasari, P.; Fini, M.; Moroni, L. Incorporation of nanostructured hydroxyapatite and poly(N-isopropylacrylamide) in demineralized bone matrix enhances osteoblast and human mesenchymal stem cell activity. Biointerphases 2015, 10, 041001. [Google Scholar] [CrossRef]
- Chacón, V.P.G.; Habibovic, P. Deconvoluting the bioactivity of calcium phosphate-based bone graft substitutes: Strategies to understand the role of individual material properties. Adv. Healthc. Mater. 2017, 6, 1601478. [Google Scholar] [CrossRef]
- Mohammadi, M.; Shaegh, S.A.M.; Alibolandi, M.; Ebrahimzadeh, M.H.; Tamayol, A.; Jaafari, M.R.; Ramezani, M. Micro and nanotechnologies for bone regeneration: Recent advances and emerging designs. J. Control. Release 2018, 274, 35–55. [Google Scholar] [CrossRef]
- Manalu, J.L.; Soegijono, B.; Indrani, D.J. Characterization of hydroxyapatite derived from bovine bone. Asian J. Appl. Sci. 2015, 3, 758–765. [Google Scholar]
- Ovrebo, O.; Orlando, L.; Rubenis, K.; Ciriello, L.; Ma, Q.; Giorgi, Z.; Tognoni, S.; Loca, D.; Villa, T.; Nogueira, L.P.; et al. The role of collagen and crystallinity in the physicochemical properties of naturally derived bone grafts. Regen. Biomater. 2024, 11, rbae093. [Google Scholar] [CrossRef] [PubMed]
- Hong, K. Analysis of crystal structure of bone graft material using analyses of x-Ray diffraction and scanning electron microscope image. Int. J. Clin. Prev. Dent. 2019, 15, 215–219. [Google Scholar] [CrossRef]
- Park, M.; Mah, Y.J.; Kim, D.H.; Kim, E.S.; Park, E.J. Demineralized deciduous tooth as a source of bone graft material: Its biological and physicochemical characteristics. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 307–314. [Google Scholar] [CrossRef]
- Haugen, H.J.; Lyngstadaas, S.P.; Rossi, F.; Perale, G. Bone grafts: Which is the ideal biomaterial. J. Clin. Periodontol. 2019, 46 (Suppl. S21), 92–102. [Google Scholar] [CrossRef]
- Montazerian, M.; Shearer, A.; Mauro, J.C. Perspectives on the impact of crystallization in bioactive glasses and glass-ceramics. Int. J. Ceram. Eng. Sci. 2023, 6, e10194. [Google Scholar] [CrossRef]
- Kuzmenka, D.; Sewohl, C.; König, A.; Flath, T.; Hahnel, S.; Schulze, F.P.; Hacker, M.C.; Schulz-Siegmund, M. Sustained calcium(II)-release to impart bioactivity in hybrid glass scaffolds for bone tissue engineering. Pharmaceutics 2020, 12, 1192. [Google Scholar] [CrossRef]
- Berberi, A.; Samarani, A.; Nader, N.; Noujeim, Z.; Dagher, M.; Kanj, W.; Mearawi, R.; Salemeh, Z.; Badran, B. Physicochemical characteristics of bone substitutes used in oral surgery in comparison to autogenous bone. BioMed Res. Int. 2014, 2014, 320790. [Google Scholar] [CrossRef]
- Sunarso; Rahmawati, D.; Irawan, B.; Pangesty, A.I. A novel method to fabricate monetite granules for bone graft applications. Dent. Mater. J. 2024, 43, 67–73. [Google Scholar] [CrossRef]
- Roldan, L.; Isaza, C.; Ospina, J.; Montoya, C.; Domínguez, J.; Orrego, S.; Correa, S. A Comparative Study of HA/DBM Compounds Derived from Bovine and Porcine for Bone Regeneration. J. Funct. Biomater. 2023, 14, 439. [Google Scholar] [CrossRef]
- Suptijah, P.; Indriani, D.; Wardoyo, S.E. Isolasi dan karakterisasi kolagen dari kulit ikan patin (Pangasius sp.). J. Sains Nat. 2018, 8, 8–23. [Google Scholar] [CrossRef]
- Kiefer, J.; Stärk, A.; Kiefer, A.; Glade, H. Infrared Spectroscopic Analysis of the Inorganic Deposits from Water in Domestic and Technical Heat Exchangers. Energies 2018, 11, 798. [Google Scholar] [CrossRef]
- Riaz, T.; Zeeshan, R.; Zarif, F.; Ilyas, K.; Muhammad, N.; Safi, S.Z.; Rahim, A.; Rizvi, S.A.A.; Rehman, I.U. FTIR analysis of natural and synthetic collagen. Appl. Spectrosc. Rev. 2018, 53, 703–746. [Google Scholar] [CrossRef]
- Idiawati, N.; Novita, I.; Nurdiansyah, S.I.; Minsas, S.; Siregar, S. Identifikasi kolagen dari cangkang bulu babi (Diadema setosum) asal perairan Pulau Lemukutan. Marinade 2022, 5, 136–141. [Google Scholar] [CrossRef]
- Sizeland, K.H.; Hofman, K.A.; Hallett, I.C.; Martin, D.E.; Potgieter, J.; Kirby, N.M.; Hawley, A.; Mudie, S.T.; Ryan, T.M.; Haverkamp, R.G.; et al. Nanostructure of electrospun collagen: Do electrospun collagen fibers form native structures? Materialia 2018, 3, 90–96. [Google Scholar] [CrossRef]
- Hossain, M.S.; Ahmed, S. FTIR spectrum analysis to predict the crystalline and amorphous phases of hydroxyapatite: A comparison of vibrational motion to reflection. RSC Adv. 2023, 13, 14625–14630. [Google Scholar] [CrossRef]
- Nandiyanto, A.B.D.; Oktiani, R.; Ragadhita, R. How to Read and Interpret FTIR Spectroscope of Organic Material. Indones. J. Sci. Technol. 2019, 4, 97. [Google Scholar] [CrossRef]
- Febri, W.; Astuti, E.; Trisnawati, P. Uji Hidrolisis Parasetamol dalam Larutan pH 2,0; 5,0; dan 7,0 Pada Suhu 37 °C. Bachelor’s Thesis, Program Studi Farmasi, Fakultas Sains dan Teknologi, Universitas Peradaban, 2022. Available online: http://repository.peradaban.ac.id/id/eprint/1076 (accessed on 8 June 2025).
- Bariyah, N.; Pascawinata, A.; Firdaus, F. Gambaran Karakteristik Scaffold Hidroksiapatit Gigi Manusia Dengan Metode Planetary Ball Mill Menggunakan Uji Scanning Electron Microscope (Sem). B-Dent. Kedokt. Gigi Univ. Baiturrahmah 2016, 3, 131–138. [Google Scholar] [CrossRef]
- Munadziroh, E.; Razak, F.A.; Abbas, B.; Soekartono, H.; Agustantina, T.H.; Surboyo, M.D. Characterization of bovine sponge amnion (BSA) by a novel process for dental treatment. J. Int. Dent. Med. Res. 2022, 15, 479–484. [Google Scholar]
- O’Connor, D.; Sexton, B.; Smart, R. Surface Analysis Methods in Materials Science; Springer Series in Surface Sciences; Springer Nature: Dordrecht, The Netherlands, 2013. [Google Scholar]
- Dewi, M.; Peornomo, H. The Effect of Zirconia Material for Dental Implant to Osseointegrated Process. SONDE (Sound Dent.) 2020, 5, 39–53. [Google Scholar] [CrossRef]
- Le Guéhennec, L.; Soueidan, A.; Layrolle, P.; Amouriq, Y. Surface treatments of titanium dental implants for rapid osseointegration. Dent. Mater. 2007, 23, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Engbrecht, D.C.; Hirschfeld, D. Thermal analysis of calcium sulfate dihydrate sources used to manufacture gypsum wallboard. Thermochim. Acta 2016, 639, 173–185. [Google Scholar] [CrossRef]
- Grawish, M.E. Demineralized dentin matrix for dental and alveolar bone tissues regeneration: An innovative scope review. Tissue Eng. Regen. Med. 2022, 19, 687–701. [Google Scholar] [CrossRef] [PubMed]
- Li, Q. Demineralized bone matrix-based microcarrier scaffold favors vascularized large bone regeneration in vivo in a rat model. J. Biomater. Appl. 2018, 33, 182–195. [Google Scholar] [CrossRef]
- Leni, A.; Hariyani, N.A. Hidroksiapatit sebagai salah satu bahan yang paling umum digunakan pada cangkok tulang. J. Kedokt. Gigi Univ. Baiturrahmah 2021, 8, 172–178. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample * | Crystal Phase | Degree of Crystallinity |
|---|---|---|
| DBM–Ca(OH)2 1:1 | Ca(OH)2 | 58.6% |
| DBM–Ca(OH)2 2:1 | Ca(OH)2 | 51.6% |
| DBM–Ca(OH)2 3:1 | Ca(OH)2 | 48.5% |
| DBM–Ca(OH)2 4:1 | Ca(OH)2 | 48.1% |
| DBM | - | - |
| Ca(OH)2 | Ca(OH)2 | 63.1% |
| Sample | Number of Sample | Calcium Ion Concentration (mg/L) (x ± SD) | p-Value |
|---|---|---|---|
| DBM–Ca(OH)2 1:1 | 3 | 218.56 ± 1.37 | <0.001 * |
| DBM–Ca(OH)2 2:1 | 3 | 214.71 ± 1.53 | |
| DBM–Ca(OH)2 3:1 | 3 | 209.65 ± 0.80 | |
| DBM–Ca(OH)2 4:1 | 3 | 205.11 ± 0.99 | |
| DBM | 3 | 2.31 ± 0.32 | |
| Ca(OH)2 | 3 | 229.60 ± 1.94 |
| Compound | Functional Group | Infrared Wavelength |
|---|---|---|
| Amide I | Stretching C=O | 1600–1700 cm−1 |
| Amide II | Stretching C-N Bending N-H | 1480–1575 cm−1 |
| Amide III | Stretching C-N Bending N-H | 1200–1300 cm−1 |
| Amide A | Stretching N-H | 3300–3500 cm−1 |
| Amide B | Stretching N-H | 2900–3100 cm−1 |
| PO43− | Asymmetry Stretching P-O | 1030–1090 cm−1 |
| CO32− | Asymmetry Stretching C-O | 1400–1500 cm−1 |
| COO− | Symmetry Stretching C-O-O Asymmetry Stretching C-O-O | 1300–1420 cm−1 1550–1650 cm−1 |
| OH− | Stretching O-H | 3300–3650 cm−1 |
| Sampel | Smallest Particle (μm) | Largest Particle (μm) | Average Particle Size (μm) | ± SD |
|---|---|---|---|---|
| DBM * | - | - | - | - |
| Ca(OH)2 | 0.01 | 350.68 | 6.34 | 6.34 ± 29.56 |
| DBM-Ca(OH)2 1:1 | 0.01 | 248.38 | 4.37 | 4.37 ± 13.42 |
| DBM-Ca(OH)2 2:1 | 0.01 | 149.67 | 4.50 | 4.50 ± 13.28 |
| DBM-Ca(OH)2 3:1 | 0.01 | 146.75 | 3.65 | 3.65 ± 9.35 |
| DBM-Ca(OH)2 4:1 | 0.01 | 197.28 | 5.00 | 5.00 ± 15.49 |
| Element | DBM | Ca(OH)2 | DBM-Ca(OH)2 1:1 | DBM-Ca(OH)2 2:1 | DBM-Ca(OH)2 3:1 | DBM-Ca(OH)2 4:1 |
|---|---|---|---|---|---|---|
| Wt% | Wt% | Wt% | Wt% | Wt% | Wt% | |
| C | 71.14 | 29.04 | 37.7 | 38.47 | 42.89 | 37.60 |
| O | 28.51 | 45.55 | 42.13 | 42.35 | 39.66 | 42.70 |
| Na | 0 | 0 | 0.28 | 0.21 | 0.48 | 0.52 |
| Mg | 0 | 0.23 | 0.14 | 0.23 | 0.16 | 0.20 |
| Al | 0 | 0.24 | 0.2 | 0.23 | 0.15 | 0.19 |
| Cl | 0 | 0 | 0.25 | 0.31 | 0.53 | 0.6 |
| Ca | 0.35 | 24.94 | 19.3 | 18.2 | 16.12 | 18.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Octarina; Kurniawan, F.L.; Larosa, F.A.; Komala, O.N.; Surboyo, M.D.C. Physicochemical Properties of Demineralized Bone Matrix and Calcium Hydroxide Composites Used as Bone Graft Material. Crystals 2025, 15, 564. https://doi.org/10.3390/cryst15060564
Octarina, Kurniawan FL, Larosa FA, Komala ON, Surboyo MDC. Physicochemical Properties of Demineralized Bone Matrix and Calcium Hydroxide Composites Used as Bone Graft Material. Crystals. 2025; 15(6):564. https://doi.org/10.3390/cryst15060564
Chicago/Turabian StyleOctarina, Florencia Livia Kurniawan, Firda Amalia Larosa, Olivia Nauli Komala, and Meircurius Dwi Condro Surboyo. 2025. "Physicochemical Properties of Demineralized Bone Matrix and Calcium Hydroxide Composites Used as Bone Graft Material" Crystals 15, no. 6: 564. https://doi.org/10.3390/cryst15060564
APA StyleOctarina, Kurniawan, F. L., Larosa, F. A., Komala, O. N., & Surboyo, M. D. C. (2025). Physicochemical Properties of Demineralized Bone Matrix and Calcium Hydroxide Composites Used as Bone Graft Material. Crystals, 15(6), 564. https://doi.org/10.3390/cryst15060564