Outcomes of IncobotulinumtoxinA Injection on Myalgia and Arthralgia in Patients Undergoing Temporomandibular Joint Arthroscopy: A Randomized Controlled Trial



Abstract
1. Introduction
2. Results
2.1. Pre and Post-Treatment Measurements
2.1.1. Pre-Treatment Phase
2.1.2. Post-Treatment T1 (5 Weeks)
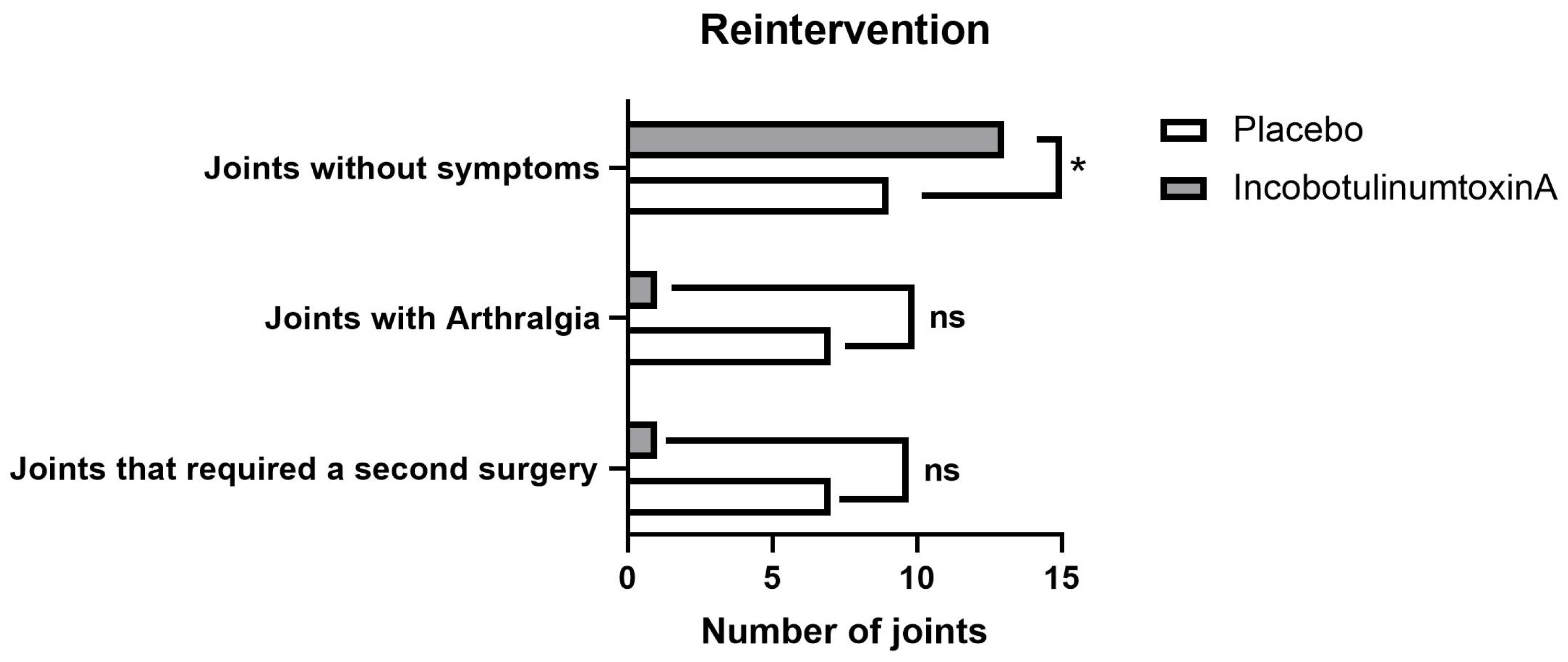
2.1.3. Post-Treatment T2 (6 Months)
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Study Design
5.2. Outcomes Evaluation
5.3. Myalgia and Arthralgia Assessment
5.4. Randomization
5.5. Treatment Protocol
5.5.1. Masticatory Muscles Injection
5.5.2. TMJ Arthroscopy
5.6. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ulmner, M.; Weiner, C.K.; Lund, B. Predictive factors in temporomandibular joint arthroscopy: A prospective cohort short-term outcome study. Int. J. Oral Maxillofac. Surg. 2020, 49, 614–620. [Google Scholar] [CrossRef]
- Schiffman, E.L.; Ohrbach, R.; Truelove, E.L.; Tai, F.; Anderson, G.C.; Pan, W.; Gonzalez, Y.M.; John, M.T.; Sommers, E.; List, T.; et al. The Research Diagnostic Criteria for Temporomandibular Disorders. V: Methods used to establish and validate revised Axis I diagnostic algorithms. J. Orofac. Pain 2010, 24, 63–78. [Google Scholar]
- Ângelo, D.F.; Mota, B.; João, R.S.; Sanz, D.; Cardoso, H.J. Prevalence of Clinical Signs and Symptoms of Temporomandibular Joint Disorders Registered in the EUROTMJ Database: A Prospective Study in a Portuguese Center. J. Clin. Med. 2023, 12, 3553. [Google Scholar] [CrossRef] [PubMed]
- Martin Granizo, R.; Correa Muñoz, D.C.; Varela Reyes, E. Rearthroscopy of the temporomandibular joint: A retrospective study of 600 arthroscopies. J. Cranio-Maxillo-Facial Surg. Off. Publ. Eur. Assoc. Cranio-Maxillo-Facial Surg. 2018, 46, 1555–1560. [Google Scholar] [CrossRef]
- Ângelo, D.F.; Araújo, R.A.D.; Sanz, D. Surgical complications related to temporomandibular joint arthroscopy: A prospective analysis of 39 single-portal versus 43 double-portal procedures. Int. J. Oral Maxillofac. Surg. 2021, 50, 1089–1094. [Google Scholar] [CrossRef]
- Golanska, P.; Saczuk, K.; Domarecka, M.; Kuć, J.; Lukomska-Szymanska, M. Temporomandibular Myofascial Pain Syndrome-Aetiology and Biopsychosocial Modulation. A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 7807. [Google Scholar] [CrossRef]
- Machado, D.; Martimbianco, A.L.C.; Bussadori, S.K.; Pacheco, R.L.; Riera, R.; Santos, E.M. Botulinum Toxin Type A for Painful Temporomandibular Disorders: Systematic Review and Meta-Analysis. J. Pain 2020, 21, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.W.; Lee, S.K.; Ahnn, J. Botulinum Toxin as a Pain Killer: Players and Actions in Antinociception. Toxins 2015, 7, 2435–2453. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.W.; Chiu, Y.W.; Chen, C.Y.; Chuang, S.K. Botulinum toxin therapy for temporomandibular joint disorders: A systematic review of randomized controlled trials. Int. J. Oral Maxillofac. Surg. 2015, 44, 1018–1026. [Google Scholar] [CrossRef]
- Thambar, S.; Kulkarni, S.; Armstrong, S.; Nikolarakos, D. Botulinum toxin in the management of temporomandibular disorders: A systematic review. Br. J. Oral Maxillofac. Surg. 2020, 58, 508–519. [Google Scholar] [CrossRef]
- Al-Moraissi, E.A.; Conti, P.C.R.; Alyahya, A.; Alkebsi, K.; Elsharkawy, A.; Christidis, N. The hierarchy of different treatments for myogenous temporomandibular disorders: A systematic review and network meta-analysis of randomized clinical trials. Oral Maxillofac. Surg. 2022, 26, 519–533. [Google Scholar] [CrossRef] [PubMed]
- Walter, S.D.; Han, H.; Guyatt, G.H.; Bassler, D.; Bhatnagar, N.; Gloy, V.; Schandelmaier, S.; Briel, M. A systematic survey of randomised trials that stopped early for reasons of futility. BMC Med. Res. Methodol. 2020, 20, 10. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, G.; Gonçalves, D.A.G.; Conti, P. Musculoskeletal Disorders. Dent. Clin. North Am. 2018, 62, 553–564. [Google Scholar] [CrossRef]
- Ernberg, M.; Hedenberg-Magnusson, B.; List, T.; Svensson, P. Efficacy of botulinum toxin type A for treatment of persistent myofascial TMD pain: A randomized, controlled, double-blind multicenter study. Pain 2011, 152, 1988–1996. [Google Scholar] [CrossRef]
- Pellett, S.; Tepp, W.H.; Whitemarsh, R.C.; Bradshaw, M.; Johnson, E.A. In vivo onset and duration of action varies for botulinum neurotoxin A subtypes 1-5. Toxicon Off. J. Int. Soc. Toxinology 2015, 107, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Benoliel, R.; Svensson, P.; Heir, G.M.; Sirois, D.; Zakrzewska, J.; Oke-Nwosu, J.; Torres, S.R.; Greenberg, M.S.; Klasser, G.D.; Katz, J.; et al. Persistent orofacial muscle pain. Oral Dis. 2011, 17 (Suppl. S1), 23–41. [Google Scholar] [CrossRef]
- Reis, P.H.F.; Laxe, L.A.C.; Lacerda-Santos, R.; Münchow, E.A. Distribution of anxiety and depression among different subtypes of temporomandibular disorder: A systematic review and meta-analysis. J. Oral Rehabil. 2022, 49, 754–767. [Google Scholar] [CrossRef]
- Rodrigues, A.L.P.; Cardoso, H.J.; Ângelo, D.F. Patient experience and satisfaction with different temporomandibular joint treatments: A retrospective study. J. Cranio-Maxillo-Facial Surg. Off. Publ. Eur. Assoc. Cranio-Maxillo-Facial Surg. 2023, 51, 44–51. [Google Scholar] [CrossRef]
- Song, P.C.; Schwartz, J.; Blitzer, A. The emerging role of botulinum toxin in the treatment of temporomandibular disorders. Oral Dis. 2007, 13, 253–260. [Google Scholar] [CrossRef]
- Patel, A.A.; Lerner, M.Z.; Blitzer, A. IncobotulinumtoxinA Injection for Temporomandibular Joint Disorder. Ann. Otol. Rhinol. Laryngol. 2017, 126, 328–333. [Google Scholar] [CrossRef]
- Kurtoglu, C.; Gur, O.H.; Kurkcu, M.; Sertdemir, Y.; Guler-Uysal, F.; Uysal, H. Effect of botulinum toxin-A in myofascial pain patients with or without functional disc displacement. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2008, 66, 1644–1651. [Google Scholar] [CrossRef]
- Ramos-Herrada, R.M.; Arriola-Guillén, L.E.; Atoche-Socola, K.J.; Bellini-Pereira, S.A.; Castillo, A.A. Effects of botulinum toxin in patients with myofascial pain related to temporomandibular joint disorders: A systematic review. Dent. Med. Probl. 2022, 59, 271–280. [Google Scholar] [CrossRef]
- De la Torre Canales, G.; Poluha, R.L.; Pinzón, N.A.; Da Silva, B.R.; Almeida, A.M.; Ernberg, M.; Manso, A.C.; Bonjardim, L.R.; Rizzatti-Barbosa, C.M. Efficacy of Botulinum Toxin Type-A I in the Improvement of Mandibular Motion and Muscle Sensibility in Myofascial Pain TMD Subjects: A Randomized Controlled Trial. Toxins 2022, 14, 441. [Google Scholar] [CrossRef]
- Fleckenstein, J.; Zaps, D.; Rüger, L.J.; Lehmeyer, L.; Freiberg, F.; Lang, P.M.; Irnich, D. Discrepancy between prevalence and perceived effectiveness of treatment methods in myofascial pain syndrome: Results of a cross-sectional, nationwide survey. BMC Musculoskelet. Disord. 2010, 11, 32. [Google Scholar] [CrossRef]
- von Lindern, J.J. Type A botulinum toxin in the treatment of chronic facial pain associated with temporo-mandibular dysfunction. Acta Neurol. Belg. 2001, 101, 39–41. [Google Scholar] [PubMed]
- Aurora, S.K.; Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia Int. J. Headache 2010, 30, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.C.; Seet, R.C. Use of botulinum toxin in the neurology clinic. Nat. Rev. Neurol. 2010, 6, 624–636. [Google Scholar] [CrossRef] [PubMed]
- Montori, V.M.; Devereaux, P.J.; Adhikari, N.K.; Burns, K.E.; Eggert, C.H.; Briel, M.; Lacchetti, C.; Leung, T.W.; Darling, E.; Bryant, D.M.; et al. Randomized trials stopped early for benefit: A systematic review. Jama 2005, 294, 2203–2209. [Google Scholar] [CrossRef] [PubMed]
- Dimitroulis, G. A new surgical classification for temporomandibular joint disorders. Int. J. Oral Maxillofac. Surg. 2013, 42, 218–222. [Google Scholar] [CrossRef]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Goiato, M.C.; Zuim, P.R.J.; Moreno, A.; Dos Santos, D.M.; da Silva, E.V.F.; de Caxias, F.P.; Turcio, K.H.L. Does pain in the masseter and anterior temporal muscles influence maximal bite force? Arch. Oral Biol. 2017, 83, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Lian, Y.; Xie, N.; Chen, C.; Zheng, Y. Single-dose botulinum toxin type a compared with repeated-dose for treatment of trigeminal neuralgia: A pilot study. J. Headache Pain 2017, 18, 81. [Google Scholar] [CrossRef]
- Guarda-Nardini, L.; Manfredini, D.; Salamone, M.; Salmaso, L.; Tonello, S.; Ferronato, G. Efficacy of Botulinum Toxin in Treating Myofascial Pain in Bruxers: A Controlled Placebo Pilot Study. CRANIO® 2008, 26, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.H.; Lee, H.J.; Hur, H.W.; Seo, K.K.; Kim, H.J. Guidelines for Botulinum Neurotoxin Injection for Facial Contouring. Plast. Reconstr. Surg. 2022, 150, 562e–571e. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total (n = 15) (30 Joints) | Placebo (n = 8) (16 Joints) | Incobotulinumtoxin A (n = 7) (14 Joints) | p Value | |
|---|---|---|---|---|
| Demographic data | ||||
| Age, A ± SD | 26.5 ± 6.1 (18–39) | 29.3 ± 5.4 (24–39) | 23.4 ± 5.5 (18–30) | 0.058 |
| Sex (F) | 93.3% (14) | 100% (8) | 85.7% (7) | 0.467 |
| Joint Diagnosis T (B, R, L) | ||||
| DDwoR | 15 (5, 8, 7) | 8 (3, 4, 4) | 7 (2, 4, 3) | 0.694 |
| DDwR | 12 (2, 5, 7) | 6 (2, 3, 3) | 6 (1, 2, 4) | 0.417 |
| Osteoarthrosis | 13 (4, 7, 6) | 5 (2, 2, 3) | 8 (2, 5, 3) | 0.999 |
| Arthralgia | 27 (13, 14, 13) | 14 (7, 7, 7) | 13 (6, 7, 6) | 0.457 |
| Disc Perforation | 1 (0, 0, 1) | 0 (0, 0, 0) | 1 (0, 0, 1) | 0.999 |
| Osteophytes | 1 (0, 1, 0) | 1 (0, 1, 0) | 0 (0, 0, 0) | 0.999 |
| Placebo (n = 8) (16 Joints) | Inco-BoNT/A (n = 7) (14 Joints) | Placebo vs. Inco-BoNT/A p Value | |
|---|---|---|---|
| Pre-treatment measurements | |||
| TMJ arthralgia (VAS, 0–10), A ± SD | 6 ± 3.6 | 5.4 ± 1.9 | 0.487 |
| MMO (mm), A ± SD | 33.9 ± 10.1 | 35.1 ± 12.8 | 0.953 |
| Myalgia degree (0–3), A ± SD | 2.8 ± 0.3 | 2.3 ± 0.6 | 0.072 |
| Joint clicks T (B,R,L) | 8 (4, 4, 4) | 5 (1, 2, 3) | 0.484 |
| Post-treatment measurements (5 weeks) | |||
| TMJ arthralgia (VAS, 0–10), A ± SD | 0.9 ± 1.6 | 0.9 ± 1.3 | 0.753 |
| MMO (mm), A ± SD | 35.9 ± 2.2 | 36.3 ± 3.3 | 0.683 |
| Myalgia degree (0–3), A ± SD | 0.9 ± 1.0 | 1.1 ± 1.1 | 0.815 |
| Joint clicks T (B,R,L) | 1 (0, 1, 0) | 0 (0, 0, 0) | 0.999 |
| Post-treatment measurements (6 months) | |||
| TMJ arthralgia (VAS, 0–10), A ± SD | 2.4 ± 2.1 | 0.14 ± 0.4 | 0.036 * |
| MMO (mm), A ± SD | 39.9 ± 4.4 | 41.0 ± 3.9 | 0.728 |
| Myalgia degree (0–3), A ± SD | 1.2 ± 1.1 | 0.14 ± 0.4 | 0.023 * |
| Joint clicks T (B,R,L) | 3 (0, 1, 2) | 3 (1,1,0) | 0.999 |
| Intragroup analysis (p-value) | |||
| TMJ arthralgia | 0.055 | 0.002 ** | |
| MMO | 0.079 | 0.368 | |
| Myalgia degree | 0.002 ** | 0.003 ** | |
| Joint clicks | 0.020 * | 0.042 * | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ângelo, D.F.; Sanz, D.; Maffia, F.; Cardoso, H.J. Outcomes of IncobotulinumtoxinA Injection on Myalgia and Arthralgia in Patients Undergoing Temporomandibular Joint Arthroscopy: A Randomized Controlled Trial. Toxins 2023, 15, 376. https://doi.org/10.3390/toxins15060376
Ângelo DF, Sanz D, Maffia F, Cardoso HJ. Outcomes of IncobotulinumtoxinA Injection on Myalgia and Arthralgia in Patients Undergoing Temporomandibular Joint Arthroscopy: A Randomized Controlled Trial. Toxins. 2023; 15(6):376. https://doi.org/10.3390/toxins15060376
Chicago/Turabian StyleÂngelo, David Faustino, David Sanz, Francesco Maffia, and Henrique José Cardoso. 2023. "Outcomes of IncobotulinumtoxinA Injection on Myalgia and Arthralgia in Patients Undergoing Temporomandibular Joint Arthroscopy: A Randomized Controlled Trial" Toxins 15, no. 6: 376. https://doi.org/10.3390/toxins15060376
APA StyleÂngelo, D. F., Sanz, D., Maffia, F., & Cardoso, H. J. (2023). Outcomes of IncobotulinumtoxinA Injection on Myalgia and Arthralgia in Patients Undergoing Temporomandibular Joint Arthroscopy: A Randomized Controlled Trial. Toxins, 15(6), 376. https://doi.org/10.3390/toxins15060376