1. Introduction
Conductive hearing loss is found in diseased or malformed external or middle ears and can cause a hearing loss up to 60 dB HL [
1]. Conditions like otosclerosis or anatomical anomalies can sometimes be addressed surgically, but technical difficulties or refusal of the patient to undergo an operation can be obstacles to treatment. Historically, tuning forks were used to help in the diagnosis of hearing loss, using the comparison of air and bone sound transmission [
2]. More recently, bone conduction devices and implants have been used to improve the hearing of people suffering from conductive hearing loss, whatever the initial cause of the condition. Clinical experience and research have proved the efficacy of this technology [
3]. However, not many fundamental studies were conducted on the pathways of sound conduction in the skull, a topic relevant to the future optimization of the use of bone implants. Studies have theorized about how the sound itself was transmitted to the basilar membrane of the inner ear through the skull, explaining the basic functioning of bone conduction [
4,
5]. Different stimulation points on the skull with the corresponding response of accelerometers and the cochlea were also studied, but the locations tested (temporal, parietal, and frontal bone) were not compatible with finding new opportunities for implant localization improvement [
6,
7].
This study had two different aims. The first was to identify the location or locations on the skull where bone conduction to the cochlea is optimal by using three different arrangements of implants on each side that could be used in actual practice. The second goal was to determine the frequency, trajectory, and timing properties of the preferential pathways of a sound wave through the skull.
2. Materials and Methods
The experiments were conducted at the Laboratory of Applied Biomechanisms in Aix Marseille University, France. Nine cadaveric heads were acquired and used in the course of this experiment, preserved in Winckler’s solution in a cold room. They were de-identified, and no demographic data were available about the cadavers. Approval for the study was not required in accordance with local and national legislation.
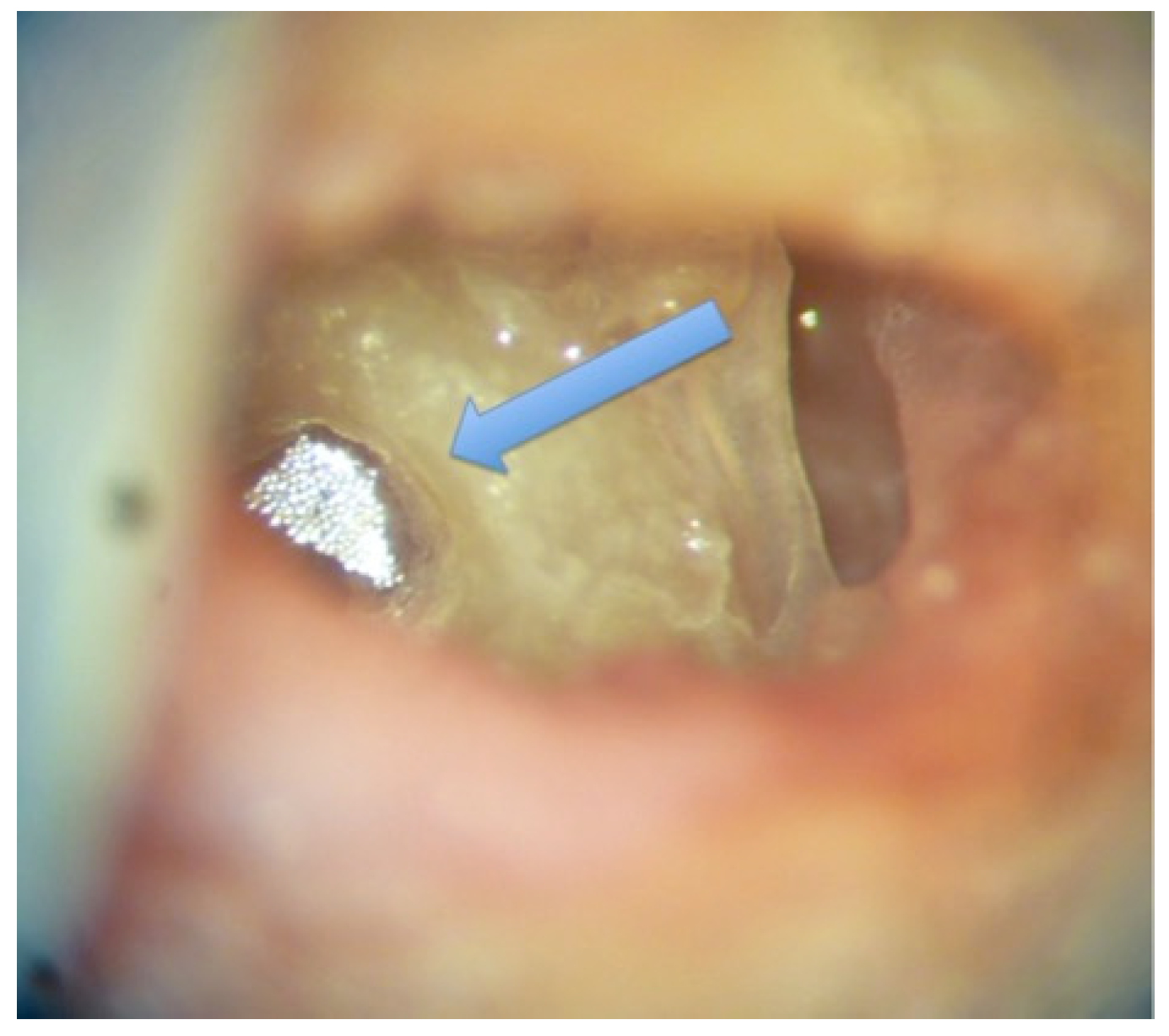
A standard bilateral mastoidectomy, including a facial recess approach to access the round window, was performed on each head. The edge of the round window niche was slightly drilled to have direct access to the round window membrane. A 1 mm
2 reflector for the laser beam of the velocimeter was placed on the round window on one side (
Figure 1).
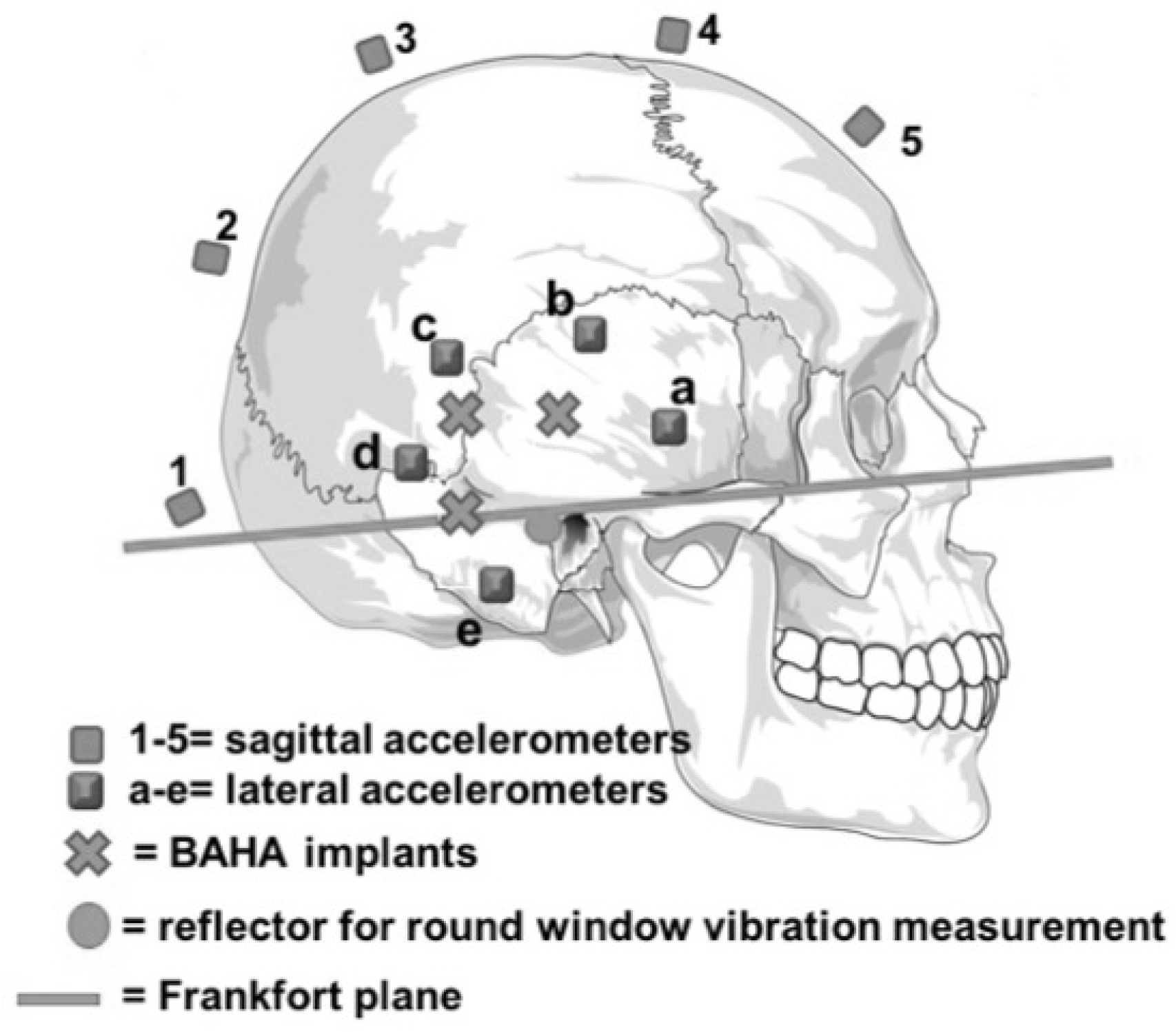
The pinna and the soft tissue behind it were removed on each side to adequately expose the mastoid bone and the space needed for the implants. BAHA™ implants (Cochlear™, Sydney, NSW, Australia) were placed at three different locations bilaterally. They were all set at the same distance (2.5 cm) from the external auditory canal at 0°, 45°, and 90° from the Frankfort plane (
Figure 2), a virtual line passing through the external auditory canal and extending to the inferior limit of the orbital rim.
The implants were fixed in the bone with a measured strength of 45 Newtons. Fifteen linear accelerometers (Bruel and Kjaer 45–17c, Naerum, Denmark) were installed: Five accelerometers were placed at equal distance on the sagittal midline from frontal to occipital, one beside each BAHA™ implant (three on each side) and one in each of the spaces available between the implants (two on each side). To fix all the accelerometers, we exposed the bone by dissecting five squares of soft tissue (2 × 2 cm). The accelerometers were glued directly on the bone for optimal data monitoring. Linear accelerometers, which measure acceleration in only one direction, were used to measure the linear vibration passing through them in the coronal plane from the emitting ear to the other ear. To avoid any damping of the vibrations by external contact and to maintain the head in an upright fixed known position for the duration of the experiment, a stake was placed through the medullar canal of the remaining cervical vertebrae. The microscope, head, and laser were all placed on anti-vibration tables in an anechoic chamber (
Figure 3).
The laser velocimeter (Laser Doppler Vibrometer OFV 534-Polytec, Hudson, MA, USA) was oriented so as to send a signal directly on the reflector on the round window on one side. The laser, accelerometers, and BAHA™ implants interfaced with an automatic Ultrasonic Pulse Velocity (UPV) 8-channels audio analyzer (Rohde-Schwarz, Attleboro, MA, USA). Each BAHA™ implant was tested in sequence. The UPV transmitter covered a frequency range from 100 Hz to 10 kHz per sweep, which are frequencies relevant to human hearing [
8]. The response of each accelerometer and of the laser velocimeter was measured and recorded separately. The UPV transmitter was used to transmit the aforementioned frequency range sweep three times to each implant. Two complete frequency sweep response measurements, in addition to one timing measurement (inter-aural time difference), were recorded. The linear accelerometers’ recordings were done randomly with emission from only one side, followed by the contralateral side. The round window response was measured for both the ipsi and contralateral emissions to get data on bilateral stimulations.
The data from the UPV were normalized over frequency bins corresponding to
1/
3 of an octave per data point by MATLAB scripts (The MatWorks, Natick, MA, USA). An Analysis of Variance (ANOVA) was performed on the data sets collected at 500 and 8000 Hz. The Tukey HSD (honest significant difference) [
9] test that uses the results of the ANOVA to distinguish if the means are different from one another to a significance level
p < 0.05 was applied to all the data sets.
4. Discussion
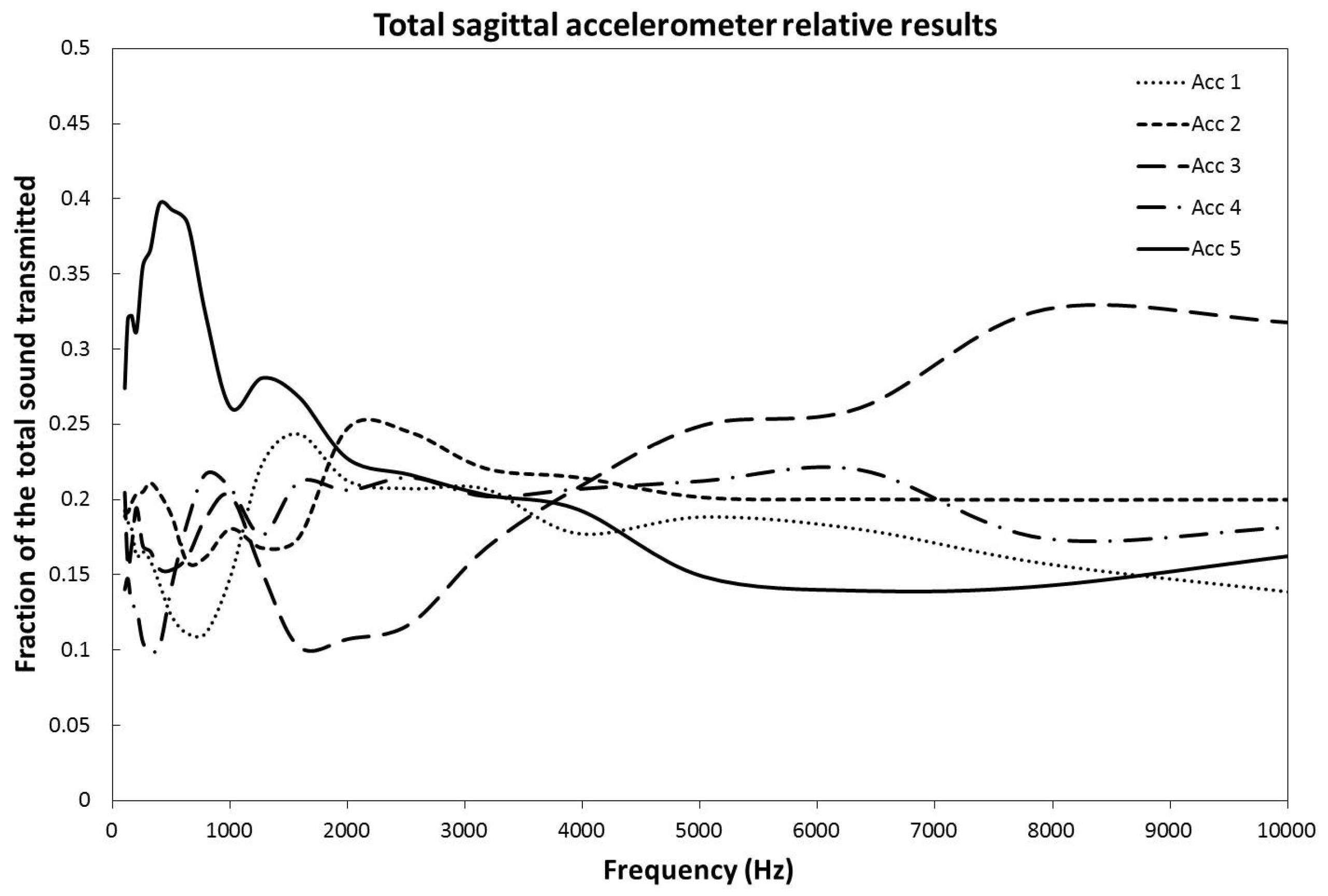
In this study, we have been able to show that the frontal pathway significantly dominates transmission for all implants separately and for the combined locations at lower frequencies. This means that the implant location has no significant effect on side-to-side transmission at those frequencies in a statistically significant manner. However, at higher frequencies, the results on propagation properties were not as clear-cut. Even though we can clearly appreciate, in
Figure 4, that above 7000 Hz there seems to be a clear predominance of accelerator #3, only the 90 degrees and combined signals were transmitting preferentially through the superior part of the skull with a statistically significant
p value of less than 0.05 (
p < 0.001). Taken alone, the 0 and 45 degrees BAHA™ implants seemed to show a tendency to use that pathway, although not in a statistically significant manner.
Figure 4 shows the results for the combination of all implant placements. It is statistically significant due to the very low
p value of the 90 degrees set (
p < 0.001), which influences the mean in a disproportionate way. There is no clear explanation of why the signal transmits that way. We hypothesize that lower frequencies signals adopt a more frontal pathway because the frontal sinus might be creating a less dense region with more resonance, advantaging the transfer of those frequencies. We could argue that the presence of the mastoid posteriorly could play a similar role [
13], but the frontal sinus is more aerated than the mastoid, and all three implants’ locations are on or above the Frankfort plane, therefore above the plane of most of the mastoid region. For the higher frequencies, accelerator #3 is the closest to the vertex, and there is no aeration in the upper skull, optimizing transmission at higher frequencies.
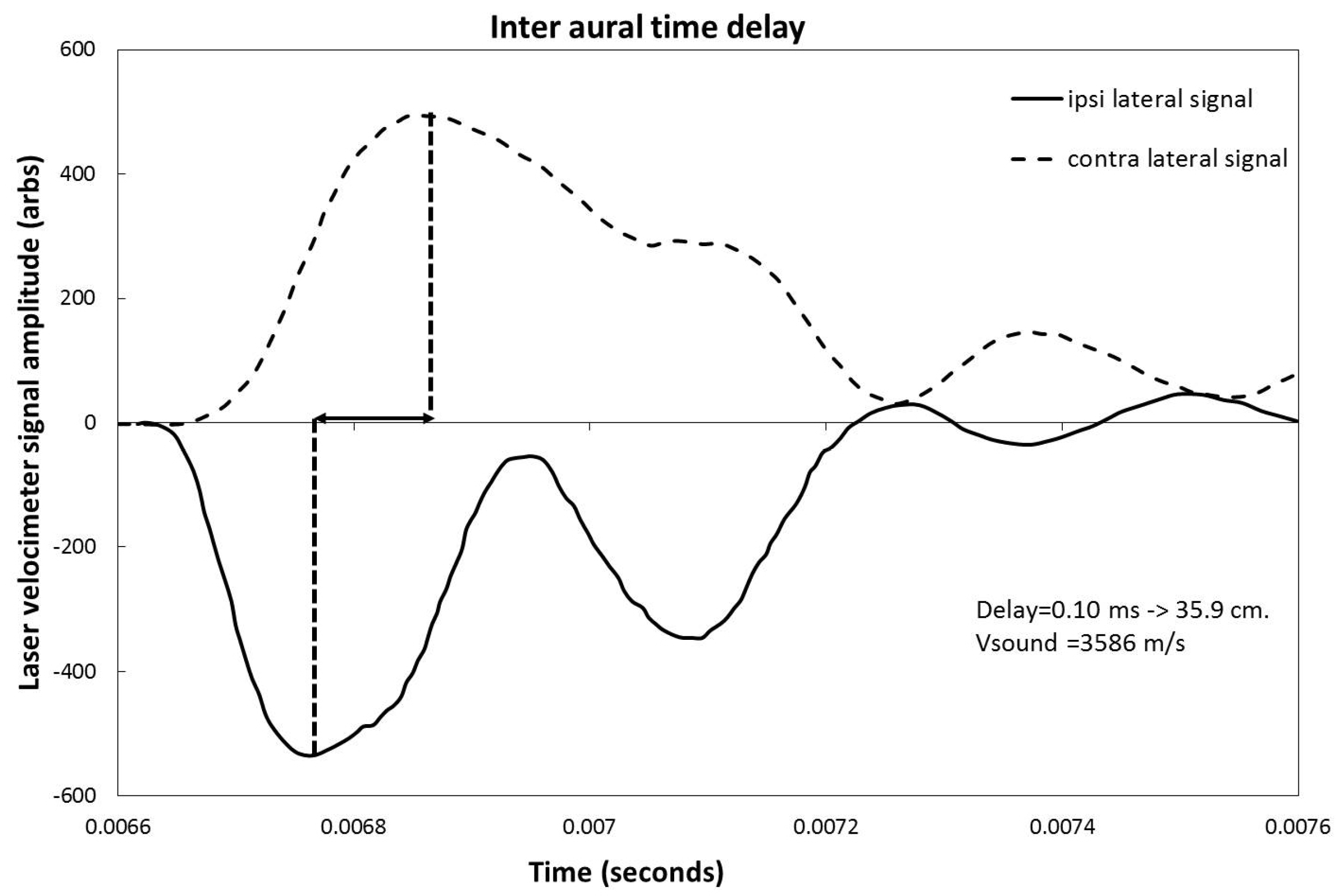
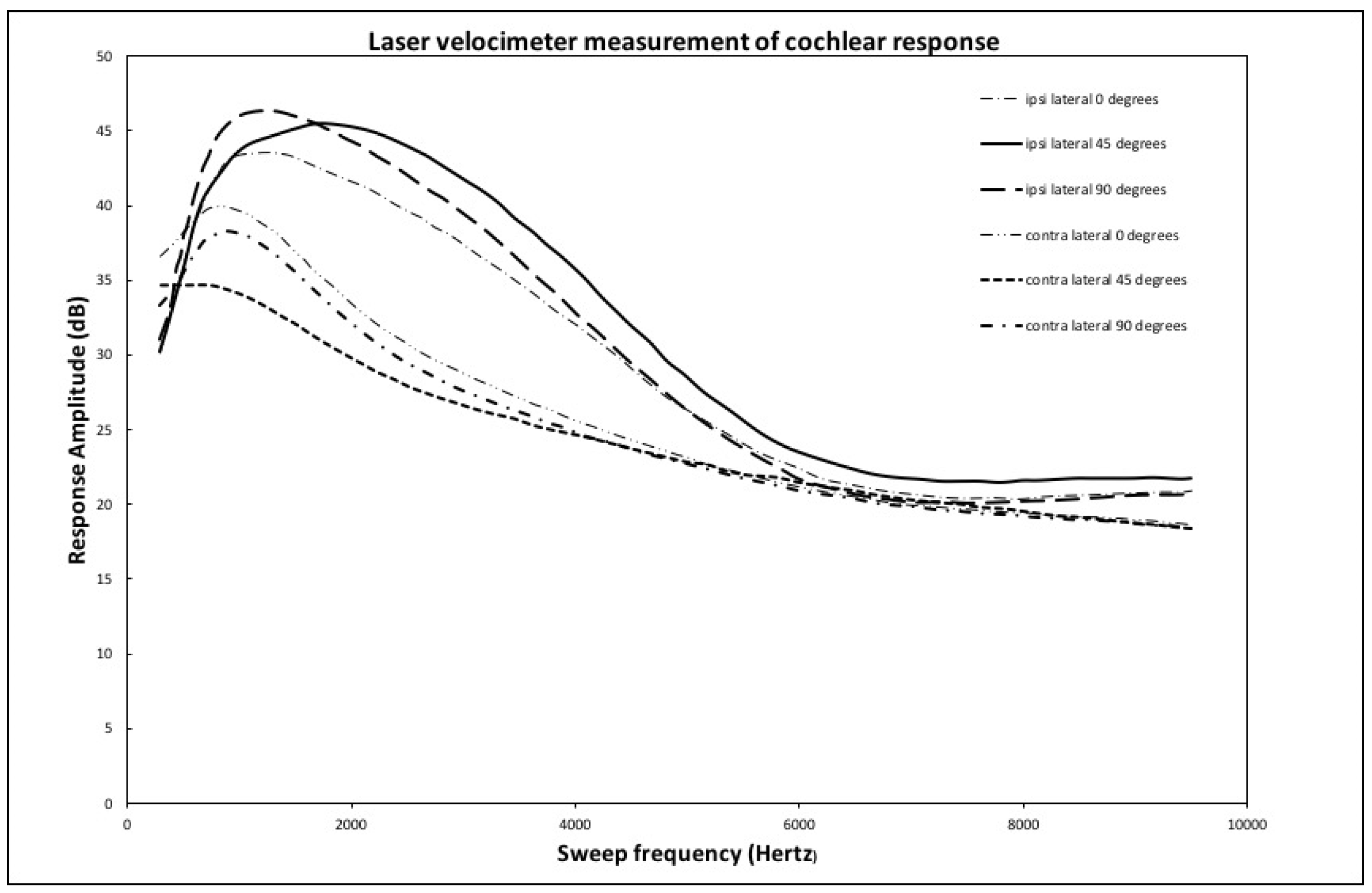
As mentioned in the results section, the laser velocimeter frequency sweep shows a response that peaks in the 1000 to 2500 Hz zone for the ipsilateral case, while this same peak is damped by 5 to 10 dB and shifted to lower frequencies for the contralateral side. This effect is due to the transmission response of the skull that both shifts frequency and damps the signal from the implant. The same effect is also visible in the time response curves shown in
Figure 5. Even though some small differences in average response can be seen between the implant location for both the ipsi and contralateral cases, no statistically significant differences that would favor a particular implant location are shown.
Other studies [
6,
7] tested implant locations not applicable in a clinical setting. This experiment tested potential locations that could be used on patients for surgical implantation. Thus, the data collected could be relevant in the greater aim of improving vibratory implant auditory results.
It is important to note the potential effects of using cadaveric heads. No osseointegration of the implant of the BAHA™ is possible, leaving open the possibility of a slightly weaker and less than optimal sound transmission to the skull from the vibration of the implant. However, the implant is already in firm mechanical contact with the skull by itself, as we could detect from the large signal amplitudes observed in the experiment. The end results should, therefore, be unaffected by this limitation. The second limitation comes from dehydration of the tissues, especially the cochlear fluids. It is very difficult to know or extrapolate the effect of brain dehydration on the transmission in the skull and the cochlea [
14]. In living persons, the brain and its fluid, which are in contact with the whole cranial vault, most probably drive a part of the bone-conducted cues. However, in cadavers, the dehydration of the brain may result in an air interface underneath the skull that may impact or dampen the sound wave transmission. For the cochlea, the limitation is expected to be a weaker transmission to the velocimeter due to less fluid being available to make the round window move when stimulated with sound. If no liquid was present in the cochlea, the velocimeter would have picked-up air displacement, which is similar to liquid displacement although weaker. As with the non-ossification of the BAHA™, this attenuation would not change the relative results but only slightly diminish the signal amplitude. The skin needed to be removed to place the implants and accelerometers. We minimized the skin removed to make sure the pathways taken by the vibrations were mostly intact. Finally, the embalmment and preservation of the head itself is a limitation. Mc Elhaney et al. studied the effect of embalmment on bones and noted generally for all methods a loss of compressive strength and an increase in hardness [
15]. Since the change in property would apply to all the bones, it could affect the raw results numbers but not the interpretation of those numbers.
We compared our results with data observed in a clinical and experimental context [
16]. As noted previously, the interaural attenuation was of 5 to 10 dB, as would be expected in clinic. The time delay response was also compatible when converted into a distance in cm, with the known speed of transmission of sound in bone [
12]. Those parameters confirmed that the data collected are relevant and will be comparable to true clinical features.
While the averaged data presented in the results section show strong regularities, there is still a notable morphology-dependent effect on the different heads. This implies that further studies on the different types of morphologies and what they imply in terms of optimal implant location need to be pursued, using the interaural time signals and the ratio of contra to ipsilateral frequency sweeps to obtain individual skull response functions is an example. In the future, a good understanding of the pathways of transmission and the significant morphological features related to them could lead to the possibility of a tailored selection of device and implantation location for each patient. During the experiment, we also scanned and modelized the heads. The present data set, as it includes both time and frequency response spectra and a CT-scan of each head, could be used in the future to build and verify a finite-element model of the skull in order to propose a virtual benchmark for the development of further bone conductions devices.
Throughout this study, great care was taken to ensure the reproducibility of the results. The work was carried out in the best possible audio conditions to minimize artifact signals. Using an anechoic chamber, anti-vibration tables, and a spine fixation considerably reduced the likelihood of spurious audio signals corrupting the data. This technique ensured reproducibility of the results by guaranteeing consistent and minimal damping of vibrations.
The data were presented and analyzed in a way that would allow other researchers to easily compare their results to ours. An example is the use of fractions in the analysis of the sound transmission pathways through the coronal plane of the skull. With this technique, any type of sound transmitter and vibration receptor could be used as long as they are set in the pattern described in the methods section. The results, when normalized as a fraction of the total sound transmission through the sagittal accelerometers, could be directly compared to the present work.


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}