
Audiological Performance of ADHEAR Systems in Simulated Conductive Hearing Loss: A Case Series with a Review of the Existing Literature

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects and Test Device
2.2. Hearing Tests
2.3. Statistical Analysis
3. Results
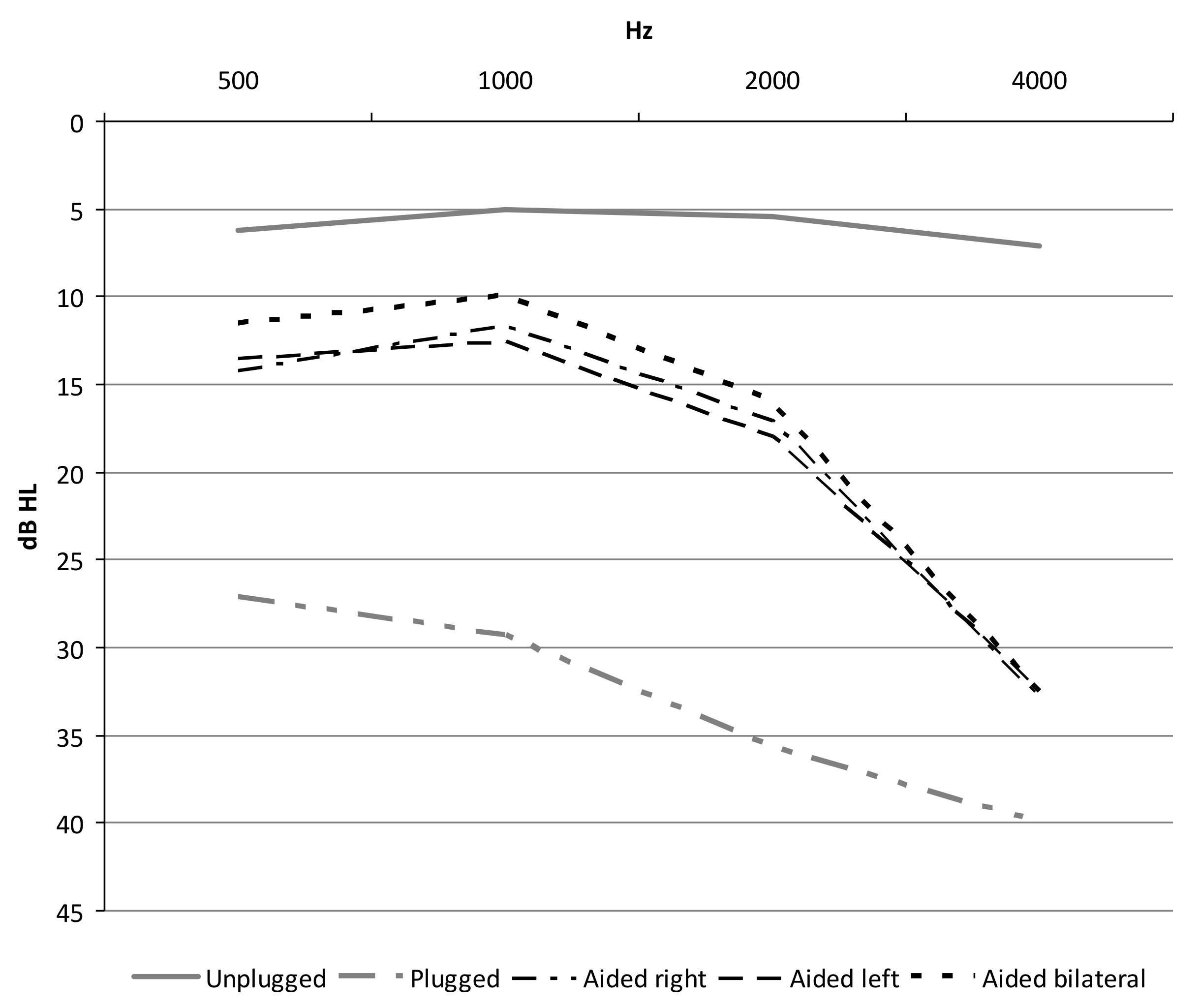
3.1. Free Field Average Hearing Threshold
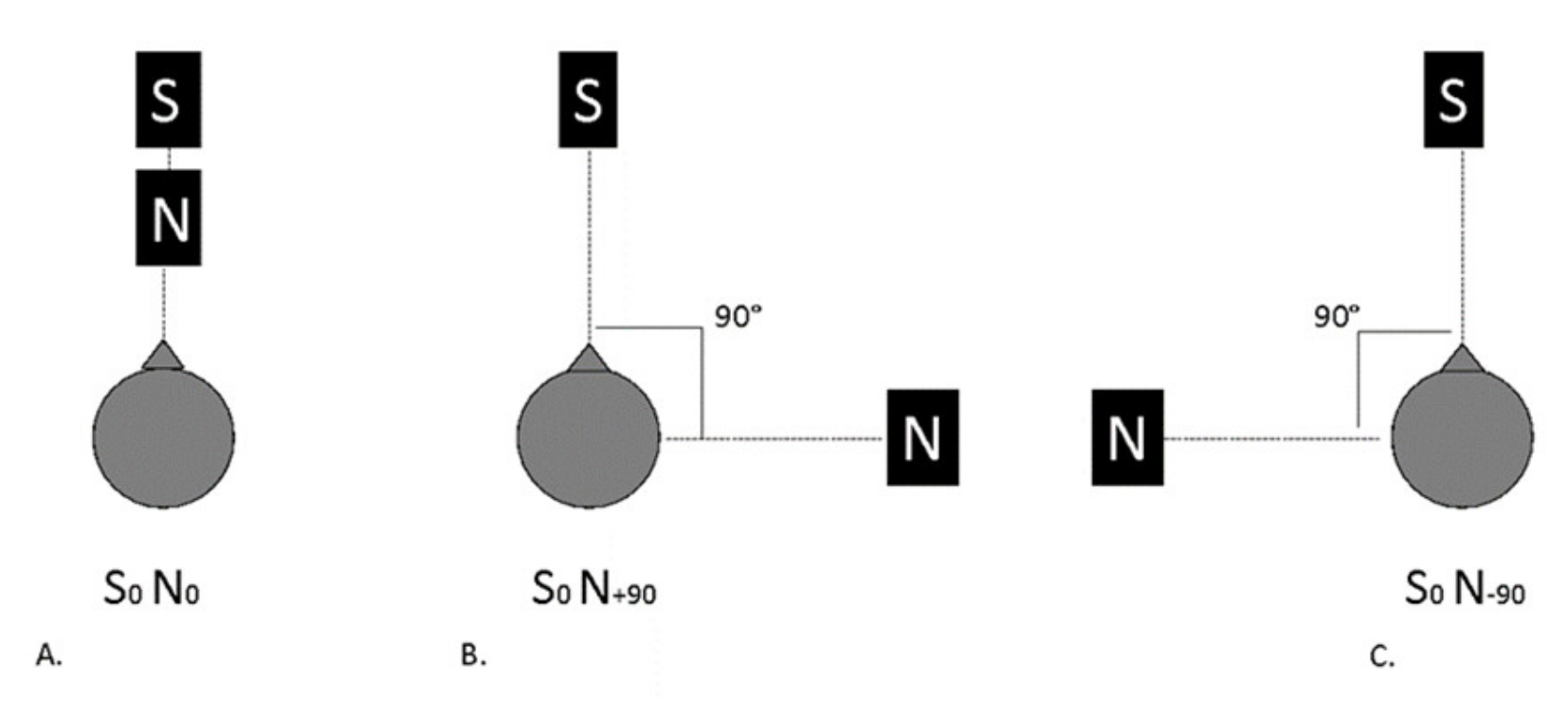
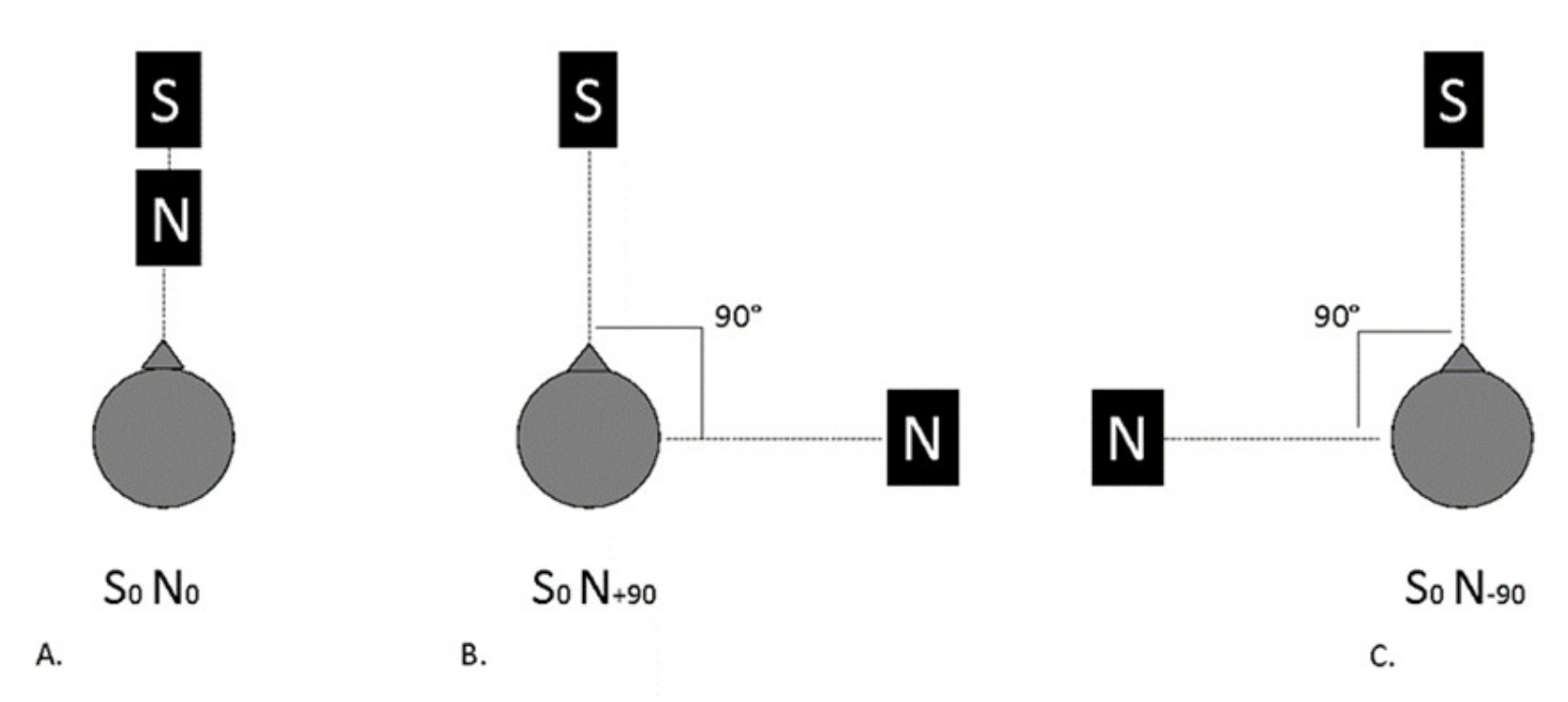
3.2. Binaural Hearing in Noise (Loudness Summation and Squelch Effect)
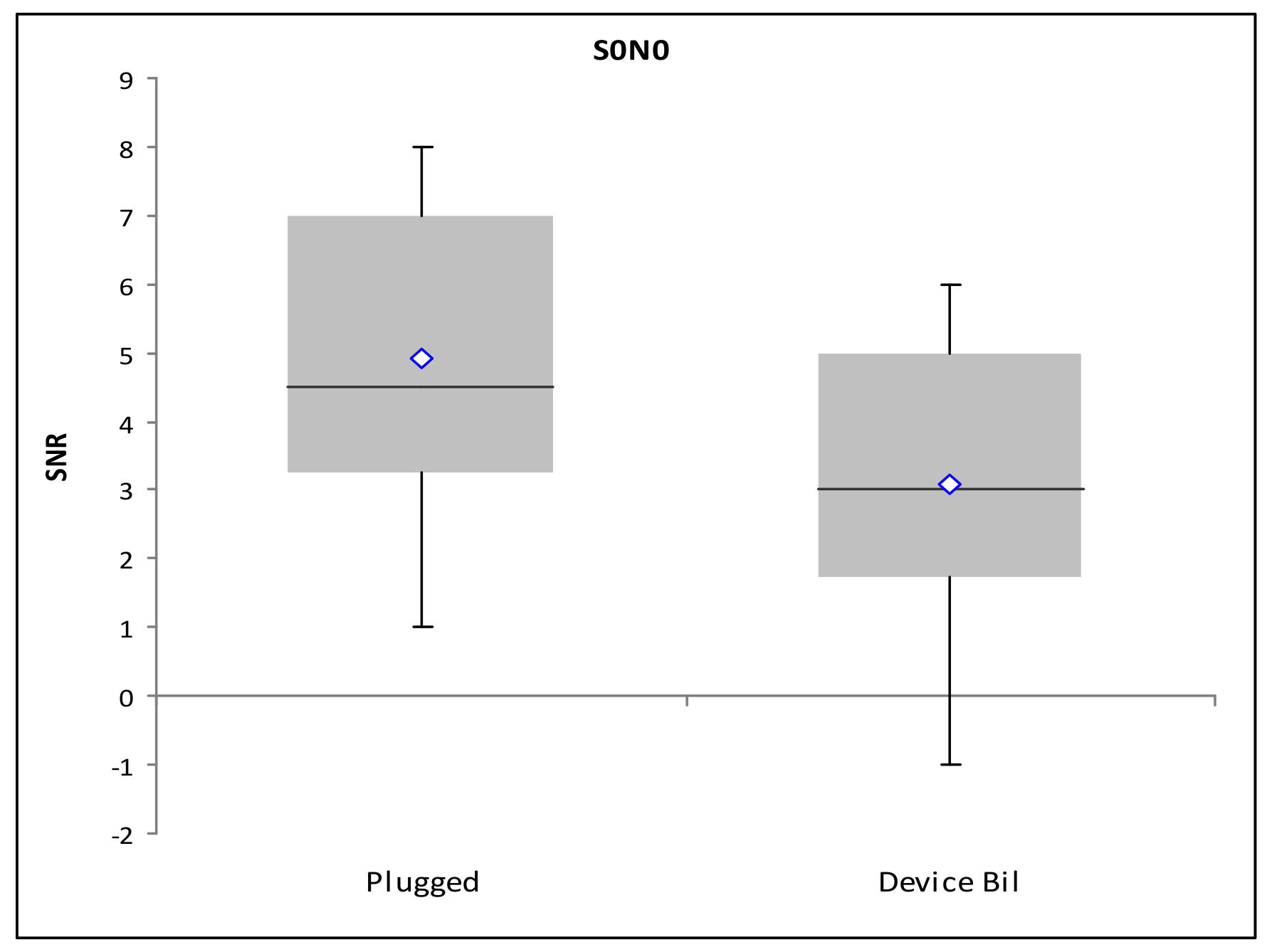
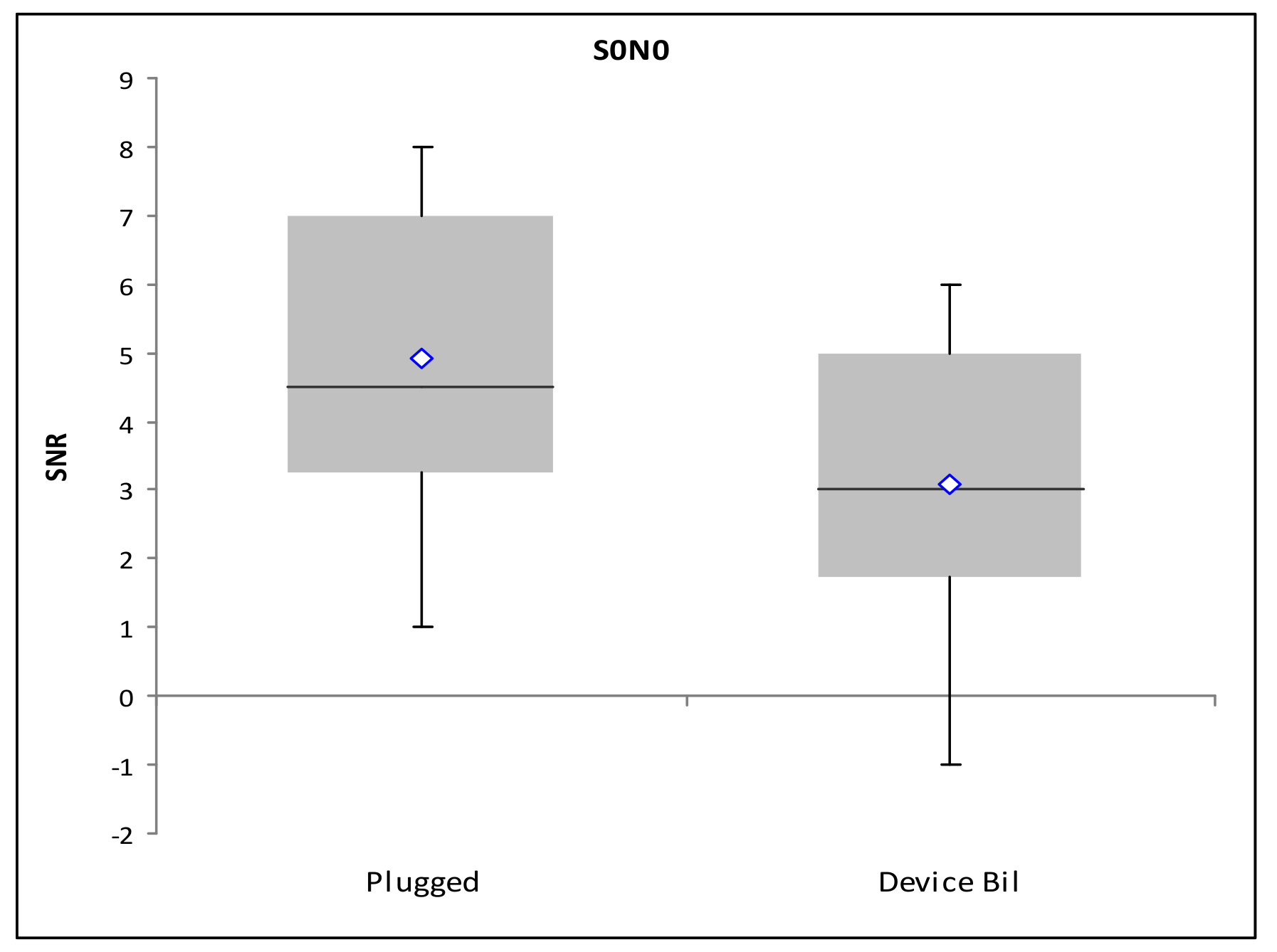
3.2.1. Loudness Summation S0N0
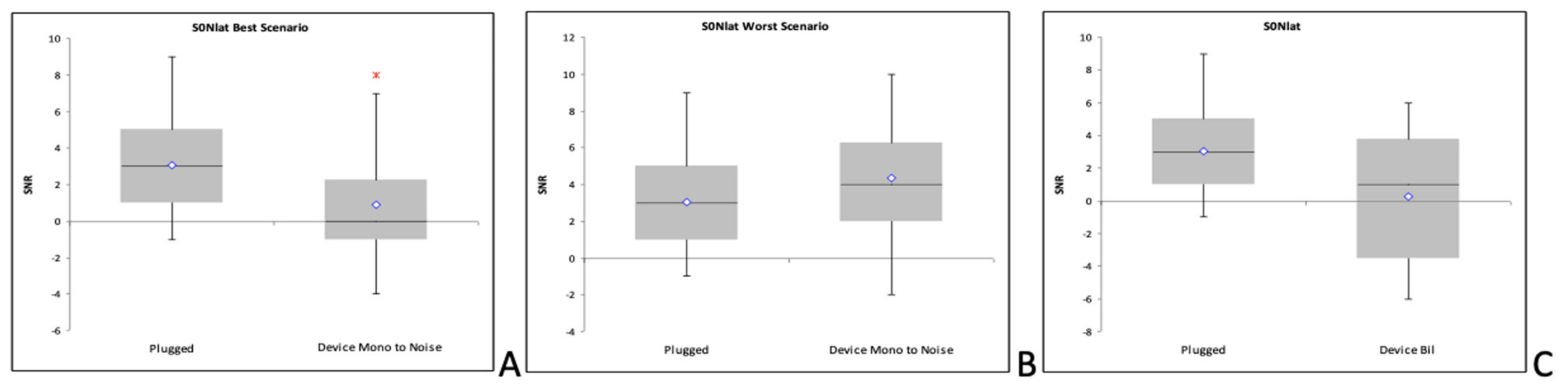
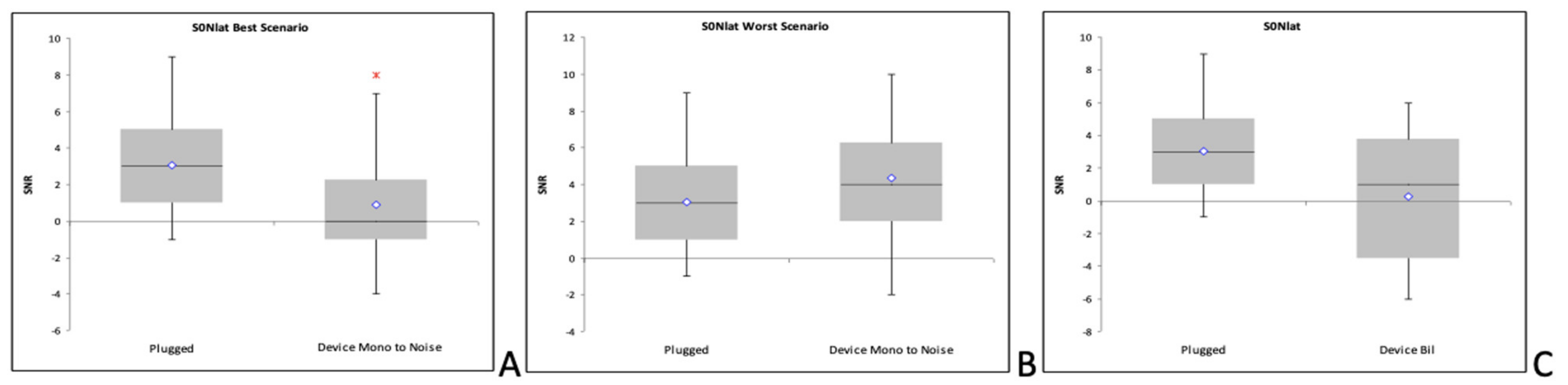
3.2.2. Squelch Effect (S0N+90)
3.2.3. Squelch Effect (S0N−90)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rosenfeld, R.M.; Culpepper, L.; Doyle, K.J.; Grundfast, K.M.; Hoberman, A.; Kenna, M.A.; Lieberthal, A.S.; Mahoney, M.; Wahl, R.A.; Woods, C.R.; et al. Clinical Practice Guideline: Otitis Media with Effusion. Otolaryngol. Neck Surg. 2004, 130, S95–S118. [Google Scholar] [CrossRef] [PubMed]
- Ebert, C.S.; Pillsbury, H.C. Otitis Media: Background and Science. In Managing the Allergic Patient; Elsevier: Amsterdam, The Netherlands, 2008; pp. 175–191. [Google Scholar]
- Robb, M.P.; Psak, J.L.; Pang-Ching, G.K. Chronic otitis media and early speech development: A case study. Int. J. Pediatr. Otorhinolaryngol. 1993, 26, 117–127. [Google Scholar] [CrossRef]
- Rach, G.H.; Zielhuis, G.A.; Broek, P.V.D. The influence of chronic persistent otitis media with effusion on language development of 2- to 4-year-olds. Int. J. Pediatr. Otorhinolaryngol. 1988, 15, 253–261. [Google Scholar] [CrossRef]
- Boudewyns, A.; Declau, F.; Ende, J.V.D.; Van Kerschaver, E.; Dirckx, S.; Brandt, A.H.-V.D.; Van de Heyning, P. Otitis Media With Effusion. Otol. Neurotol. 2011, 32, 799–804. [Google Scholar] [CrossRef] [PubMed]
- Cai, T.; McPherson, B. Hearing loss in children with otitis media with effusion: A systematic review. Int. J. Audiol. 2016, 56, 65–76. [Google Scholar] [CrossRef] [PubMed]
- O’Niel, M.B.; Runge, C.L.; Friedland, D.R.; Kerschner, J.E. Patient Outcomes in Magnet-Based Implantable Auditory Assist Devices. JAMA Otolaryngol. Neck Surg. 2014, 140, 513–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turrini, M.; Cutugno, F.; Maturi, P.; Prosser, S.; Leoni, F.A.; Arslan, E. Bisyllabic words for speech audiometry: A new italian material. Acta Otorhinolaryngol. Ital. 1993, 13, 63–77. [Google Scholar] [PubMed]
- Koopmans, W.J.A.; Goverts, S.T.; Smits, C. Speech Recognition Abilities in Normal-Hearing Children 4 to 12 Years of Age in Stationary and Interrupted Noise. Ear Heart 2018, 39, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- Cai, T.; McPherson, B.; Li, C.; Yang, F. Hearing Loss in Children With Otitis Media With Effusion: Actual and Simulated Effects on Speech Perception. Ear Heart 2018, 39, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Dahm, V.; Baumgartner, W.-D.; Liepins, R.; Arnoldner, C.; Riss, D. First Results with a New, Pressure-free, Adhesive Bone Conduction Hearing Aid. Otol. Neurotol. 2018, 39, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Kuthubutheen, J.; Broadbent, C.; Marino, R.; Távora-Vieira, D. The Use of a Novel, Nonsurgical Bone Conduction Hearing Aid System for the Treatment of Conductive Hearing Loss. Otol. Neurotol. 2020, 41, 948–955. [Google Scholar] [CrossRef] [PubMed]
- Snapp, H.; Vogt, K.; Agterberg, M.J. Bilateral bone conduction stimulation provides reliable binaural cues for localization. Heart Res. 2020, 388, 107881. [Google Scholar] [CrossRef] [PubMed]
- Neumann, K.; Thomas, J.P.; Voelter, C.; Dazert, S. A new adhesive bone conduction hearing system effectively treats conductive hearing loss in children. Int. J. Pediatr. Otorhinolaryngol. 2019, 122, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Dahm, V.; Auinger, A.B.; Liepins, R.; Baumgartner, W.-D.; Riss, D.; Arnoldner, C. A Randomized Cross-over Trial Comparing a Pressure-free, Adhesive to a Conventional Bone Conduction Hearing Device. Otol. Neurotol. 2019, 40, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Favoreel, A.; Heuninck, E.; Mansbach, A.-L. Audiological benefit and subjective satisfaction of children with the ADHEAR audio processor and adhesive adapter. Int. J. Pediatr. Otorhinolaryngol. 2020, 129, 109729. [Google Scholar] [CrossRef] [PubMed]
- Gawliczek, T.; Munzinger, F.; Anschuetz, L.; Caversaccio, M.; Kompis, M.; Wimmer, W. Unilateral and Bilateral Audiological Benefit With an Adhesively Attached, Noninvasive Bone Conduction Hearing System. Otol. Neurotol. 2018, 39, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- Mertens, G.; Gilles, A.; Bouzegta, R.; Van de Heyning, P. A Prospective Randomized Crossover Study in Single Sided Deafness on the New Non-Invasive Adhesive Bone Conduction Hearing System. Otol. Neurotol. 2018, 39, 940–949. [Google Scholar] [CrossRef] [PubMed]
- Brill, I.T.; Brill, S.; Stark, T. Neue Möglichkeiten der Rehabilitation bei Schallleitungsschwerhörigkeit. HNO 2019, 67, 698–705. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.; Loth, A.; Leinung, M.; Balster, S.; Hirth, D.; Stöver, T.; Helbig, S.; Kramer, S. A new adhesive bone conduction hearing system as a treatment option for transient hearing loss after middle ear surgery. Eur. Arch. Oto-Rhino-Laryngol. 2019, 277, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Almuhawas, F.; Alzhrani, F.; Saleh, S.; AlSanosi, A.; Yousef, M. Auditory Performance and Subjective Satisfaction with the ADHEAR System. Audiol. Neurotol. 2021, 26, 1–10. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 500 Hz | 1000 Hz | 2000 Hz | 4000 Hz | |
|---|---|---|---|---|
| Unplugged | 6.25 ± 2.26 | 5 ± 3 | 5.42 ± 3.96 | 7.08 ± 3.34 |
| Plugged | 28.3 ± 6.85 | 27.14 ± 7.48 | 36.25 ± 6.9 | 42.5 ± 6.9 |
| Aided right | 14.17 ± 2.8 | 11.67 ± 3.25 | 17.08 ± 3.96 | 32.92 ± 4.98 |
| Aided left | 13.5 ± 2.4 | 12.5 ± 3.5 | 18 ± 3.5 | 32.5 ± 5.9 |
| Aided bil | 11.5 ± 3.37 | 10 ± 2.35 | 16 ± 5.6 | 32.5 ± 4.24 |
| Loudness Summation S0N0 | Squelch Effect (S0N+90) | Squelch Effect (S0N–90) | |
|---|---|---|---|
| Unplugged | 2 dB (0; 2.3) | –5 dB (–7; –2) | –2 dB (–3.5; –1) |
| Plugged | 4.5 dB (3.8; 7) | 3 dB (2; 5) | 3 dB (0.75; 5) |
| Aided right | 3 dB (3; 6.3) | 4 dB (3; 6) | 0 dB (–1; 1.5) |
| Aided left | 5.5 dB (4; 7.8) | 0 dB (0; 2), | 5 dB (2.25; 5.75) |
| Aided bil | 3 dB (2.3; 4.8) | 0 dB (–4; 3) | 1 dB (–1.5; 3.5) |
| Authors | Subjects | Aided Condition Tested | Tests | Results |
|---|---|---|---|---|
| Brill et al. 2019 [19] | N = 12 Age = Adult Simulated with bilateral conductive hearing loss with a foam earplug | Unilateral ABCD. |
|
|
| Weiss et al. 2019 [20] | N = 11 Age = 18 years of age or older. Transient conductive hearing loss due to auditory canal tamponade after middle ear surgery. | Unilateral ABCD at the tamponade side, with contralateral ear plugged and covered. |
|
|
| Almuhawas et al. 2020 [21] | N = 12 Age = between 5 and 53 years. Conductive hearing loss (different etiologies). | Unilateral ABCD with the contralateral ear occluded with specific earplugs. |
|
|
| Dahm et al. 2018 [11] | N = 12 Age = between 14 to 74 years. Bilateral or unilateral conductive hearing loss (different etiologies). | Unilateral ABCD, with the contralateral ear covered with a circumaural earmuff or with the application of a masking signal. |
|
|
| Dahm et al. 2019 [15] | N = 13 Age = between 12 to 63 years Unilateral or bilateral conductive hearing loss | Unilateral ABCD, with the application in the contralateral ear of a masking signal Unilateral BCHA, with the application in the contralateral ear of a masking signal. |
|
|
| Favoreel et al. 2020 [16] | N = 10 Age = between 4 to 17 years. Unilateral or bilateral conductive hearing loss. | Unilateral ABCD with contralateral ear closed with an earplug and headphones. Unilateral BCHA with contralateral ear closed with an earplug and headphones. |
|
|
| Kuthubutheen et al. 2020 [12] | N = 12 Age = between 11 to 70 years. Unilateral conductive hearing loss. | Unilateral ABCD. Unilateral BCHA. |
|
|
| Neumann et al. 2019 [14] | N = 10 Age = between 3 months to 10 years. Unilateral or bilateral conductive hearing loss. | Unilateral ABCD, with the application in the contralateral ear of a masking signal. Unilateral BCHA with the application in the contralateral ear of a masking signal. |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muzzi, E.; Gambacorta, V.; Lapenna, R.; Pizzamiglio, G.; Ghiselli, S.; Caregnato, I.; Marchi, R.; Ricci, G.; Orzan, E. Audiological Performance of ADHEAR Systems in Simulated Conductive Hearing Loss: A Case Series with a Review of the Existing Literature. Audiol. Res. 2021, 11, 537-546. https://doi.org/10.3390/audiolres11040048
Muzzi E, Gambacorta V, Lapenna R, Pizzamiglio G, Ghiselli S, Caregnato I, Marchi R, Ricci G, Orzan E. Audiological Performance of ADHEAR Systems in Simulated Conductive Hearing Loss: A Case Series with a Review of the Existing Literature. Audiology Research. 2021; 11(4):537-546. https://doi.org/10.3390/audiolres11040048
Chicago/Turabian StyleMuzzi, Enrico, Valeria Gambacorta, Ruggero Lapenna, Giulia Pizzamiglio, Sara Ghiselli, Igor Caregnato, Raffaella Marchi, Giampietro Ricci, and Eva Orzan. 2021. "Audiological Performance of ADHEAR Systems in Simulated Conductive Hearing Loss: A Case Series with a Review of the Existing Literature" Audiology Research 11, no. 4: 537-546. https://doi.org/10.3390/audiolres11040048
APA StyleMuzzi, E., Gambacorta, V., Lapenna, R., Pizzamiglio, G., Ghiselli, S., Caregnato, I., Marchi, R., Ricci, G., & Orzan, E. (2021). Audiological Performance of ADHEAR Systems in Simulated Conductive Hearing Loss: A Case Series with a Review of the Existing Literature. Audiology Research, 11(4), 537-546. https://doi.org/10.3390/audiolres11040048