Abstract
Small bowel evaluation is warranted in all newly diagnosed cases of Crohn’s disease (CD) as small bowel is involved in two-thirds of CD patients at diagnosis and the involvement can be discontinuous. Endoscopic evaluation of the small bowel in suspected or established CD can be done by video capsule endoscopy (VCE), device assisted enteroscopy (DAE) (which includes single and double balloon enteroscopy, novel motorized spiral enteroscopy (NMSE) and balloon guided endoscopy (BGE)) and intra-operative enteroscopy (IOE). In suspected CD with a negative ileo-colonoscopy, VCE is the preferred initial diagnostic modality in the absence of obstructive symptoms or known stenosis. VCE should be preceded by cross-sectional imaging or patency capsule testing if obstruction is suspected given with high retention risk. In established cases, small bowel cross-sectional imaging (magnetic resonance or computed tomography enterography) is preferred over VCE as it can assess transmural and extra-luminal involvement. VCE is indicated subsequently if necessary to assess disease extent, unexplained symptoms (e.g., anemia, malnutrition) or mucosal healing. Pan-enteric capsule endoscopy (PCE) and the use of artificial intelligence are the recent developments with VCE. DAE with small bowel biopsy can provide definitive evidence of CD including the extent and severity. A final diagnosis of CD is based on the constellation of clinical, radiologic, histologic and endoscopic features. Newer technologies like NMSE and BGE can help with deeper and faster small bowel evaluation. DAE has also allowed endoscopic treatment of small bowel strictures, small bowel bleeding and retrieval of retained capsule or foreign bodies. Endoscopic balloon dilation (EBD), endoscopic electro-incision, strictureplasty and stenting have shown promising results in CD related small bowel strictures. In conclusion, endoscopic evaluation of the small bowel is rapidly evolving field that has a major role in diagnosis and management of small bowel CD and can alter treatment outcomes in properly selected patients.
1. Introduction
Crohn’s disease (CD) is a chronic idiopathic, inflammatory bowel disease that can involve any part of the gastrointestinal tract. It is characterized by mucosal and transmural inflammation and even extra-mural involvement in the form of abscess and fistula [1]. Therefore, apart from cross-sectional imaging modalities, gastrointestinal mucosal assessment is necessary. This is traditionally done by ileo-colonoscopy as the terminal ileum is the most common site involved. Upper gastrointestinal endoscopy is warranted if upper GI symptoms are present. However, CD can affect the intestine in a discontinuous manner and isolated involvement of proximal small intestine can occur in up to one third of cases. A negative ileo-colonoscopy thus does not rule out CD and the small bowel should be assessed in both suspected and established CD [2].
There are various modalities of small bowel assessment that are evolving rapidly. Traditionally, this was done by radiological imaging that has evolved from small bowel follow through (SBFT) to dedicated cross sectional imaging modalities like computed tomography (CT) enterography/enteroclysis and more recently magnetic resonance enterography (MRE).
Direct endoscopic visualization of small bowel mucosa has today shifted the paradigm of diagnosis providing histopathologic evidence to rule out infective and neoplastic causes of small bowel ulcerations. This can be done by flexible endoscopes that are advanced through the small intestine assisted by balloon (single balloon enteroscopy (SBE) and double balloon enteroscopy (DBE)) and more recently, balloon guided enteroscopy (BGE) and motorized spiral enteroscopy (NMSE) [3,4,5]. Faster and deeper small bowel endoscopic assessment can now be done by new and evolving advances in small bowel endoscopy with an increase in therapeutic enteroscopy [6]. Video Capsule Endoscopy (VCE) enables visualization of the entire small bowel mucosa less invasively than flexible endoscopes. With the evolution of technology, pan-enteric capsule endoscopy (PCE), which can enable visualization of both small and large bowel mucosa, can become the ideal noninvasive diagnostic tool. However, careful patient selection and cross-sectional imaging or patency capsule testing is warranted before proceeding to VCE in case of suspected or established CD given the higher risk of capsule retention than in the general population [7].
In fact, with the advent of VCE and dedicated small bowel cross-sectional imaging (CTE/MRE), the role of small bowel enteroscopy in suspected or established CD is primarily histological confirmation and therapeutic interventions. In this review, we have critically evaluated the current role of the various small bowel endoscopic modalities for evaluation and management of suspected or established small bowel CD. This review comprehensively sums up the existing, emerging, and ever-expanding literature in this field and highlights areas of future study.
2. Endoscopic Evaluation of Small Bowel Crohn’s Disease
2.1. Indications of Small Bowel Endoscopy in CD
- (1)
- Suspected isolated small bowel CD [8];
- (2)
- Small bowel evaluation in patients with confirmed CD [9];
- (3)
- Assessment for post-operative CD recurrence in small bowel after ileo-colonic resection [10];
- (4)
- Small bowel evaluation in IBD-unclassified and disease reclassification [8];
- (5)
- Therapeutic interventions in small bowel CD (stricture dilatation, retained capsule or foreign body retrieval, hemostasis for small bowel bleed) [8].
2.2. Role of Small Bowel Endoscopy in Suspected and Established CD
Small bowel involvement is seen in two thirds of CD patients and among them 90% have the involvement of terminal ileum [11]. Hence, in suspected small bowel CD, ileo-colonoscopy is the first line of investigation [12]. VCE is the next diagnostic modality in cases with suspected CD and negative ileo-colonoscopy in the absence of obstructive symptoms or known stenosis (Figure 1). In the presence of obstructive symptoms or known stenosis, MRE/CTE should be preferred over VCE given the high risk of capsule retention. In isolated small bowel involvement in suspected CD on VCE or MRE/CTE, DAE with a small bowel biopsy can provide definitive evidence of CD. This is particularly important in resource limited countries where infections (e.g., tuberculosis) still predominate and need to be excluded prior to initiation of therapy [13].
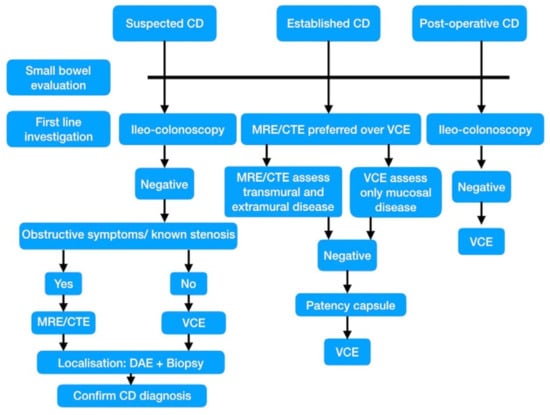
Figure 1.
Algorithm for small bowel evaluation in a suspected, established and post-operative Crohn’s disease (CD). DAE—Device assisted enteroscopy, MRE—Magnetic resonance enteroclysis, CTE—computed tomography enteroclysis, VCE—video capsule endoscopy.
Small bowel evaluation is warranted in every case of established CD, as the small bowel is involved in two thirds of CD, which can be discontinuous. In established CD, CTE/MRE is preferred over VCE due to its potential to assess transmural and extra-luminal disease. VCE is indicated subsequently if cross-sectional imaging is non-contributory preferably after patency capsule testing. VCE can better evaluate mucosal healing, unexplained pain/anemia, malabsorption and early post-operative recurrence compared to cross-sectional imaging, especially in non-stricturing CD [8]. In established CD, DAE is indicated for endoscopic treatment of small bowel strictures (balloon dilatation, stricturoplasty and stenting), small bowel bleed and foreign bodies/retained capsule retrieval [9].
2.3. VCE in Small Bowel CD
VCE is highly sensitive but not specific for detection of mucosal inflammation in small bowel CD (Figure 2). Hence, in suspected CD, VCE is useful in ruling out the diagnosis especially if ileo-colonoscopy and cross-sectional imaging are negative. In established CD, VCE can help in detecting precise disease location, disease severity and monitoring response to therapy [7]. VCE can better detect subtle mucosal abnormalities in both suspected and established CD (Figure 2B–E) [14]. The major drawback of VCE in small bowel CD are false positive diagnosis and high risk of capsule retention (Figure 2F). The later can be reduced by prior cross-sectional imaging and use of patency capsule [7].

Figure 2.
Video capsule endoscopy (VCE) for small bowel Crohn’s disease (CD). (A) Video capsule endoscope for small bowel (PillCam, Given imaging Ltd., Yokñeam Illit, Israel); (B) Aphthous ulcer seen on VCE in a case of suspected small bowel CD; (C) Small ulcer seen on VCE in CD; (D) Hyperemia, superficial ulcers and edematous mucosa on VCE in a case of CD. (E) Ulcerated stricture in CD; (F) Retained capsule removed at laparotomy.
2.3.1. Comparison of VCE with Other Diagnostic Modalities
VCE has a distinct advantage over cross-sectional imaging (CTE/MRE) in small bowel CD as it directly visualizes the small bowel mucosa and can detect subtle mucosal abnormalities [7]. In a meta-analysis of 12 studies including more than 400 patients, VCE had better diagnostic yield compared to small bowel radiology, CTE and ileo-colonoscopy in suspected CD and was a better diagnostic modality in established CD as well [14]. However, the majority of this incremental diagnostic yield could be attributed to false positives in VCE as the positive predictive value of positive VCE finings such as “more than 3 ulcers” reported to be only 50% at 12 months [15]. Moreover, these studies have significant selection bias. The only prospective blinded study comparing these modalities showed that diagnostic yield of VCE (83%) was not different from others including CTE (83%). The specificity of VCE was quite low (53%) [16]. This, combined with need for prior small bowel cross-sectional imaging, precluded the use of VCE as a first line diagnostic test in suspected CD. In a retrospective study comparing MRE and VCE, VCE detected more small bowel lesions compared to MRE, especially proximal and superficial lesions [17]. Meta-analyses have shown that VCE, MRE and small intestinal contrast ultrasound (SICUS) have similar diagnostic yield, except in the proximal bowel where VCE performs better than MRE. However, risk of capsule retention should be kept in mind [18]. In a prospective blinded study of 93 patients, the sensitivity and specificity of VCE (100% and 91%) were higher than that of CTE (76% and 85%) and MRE (81% and 86%). Proximal small bowel lesions were detected in 16 patients in VCE compared to only two patients with MRE/CTE. Only two patients had additional small bowel stenosis who did not have obstructive symptoms and underwent complete ileo-colonoscopy [19]. Therefore, it was concluded that CE is the first line modality for detecting small bowel CD in the absence of clinical suspicion of stenosis.
2.3.2. VCE in Suspected Small Bowel CD
VCE has high sensitivity (93%) for the diagnosis of small bowel CD with a high negative predictive value (96%) [20,21]. However, due to high false positive rates and consequent low specificity, VCE should be used for exclusion of CD rather than for confirmation of diagnosis [7]. Non-steroidal into-inflammatory drugs (NSAIDs) and other drug induced enteropathy, infections (e.g., small intestinal tuberculosis), autoimmune enteropathy, radiation enteritis and immunodeficiency can mimic CD on VCE [22,23]. Hence, NSAIDs should be discontinued for at least 4 weeks prior to VCE. In this regard, disease biomarkers such as fecal calprotectin could be useful in selecting patients for CE in suspected CD, as it helps exclude non-inflammatory small bowel lesions. A recent meta-analysis has identified that a fecal calprotectin cut off of more than 100 µg/g has highest diagnostic accuracy (sensitivity and specificity 73% and diagnostic odd ratio 7.89) [24]. Hence, fecal calprotectin can be used as a tool for selecting patients with suspected small bowel CD for VCE. Therefore, in suspected CD with negative ileo-colonoscopy, VCE is indicated in the absence of obstructive symptoms and known stenosis [25].
2.3.3. VCE in Established Small Bowel CD
Assessing Distribution and Monitoring Disease Activity: The VCE Scores
Measuring the extent and severity of inflammation is important in established small bowel CD as a “Treat to target” strategy based on mucosal healing can reduce disease related complications leading to surgery and hospitalization [26]. Criteria of more than three ulcers proposed by Mow et al. has modest positive predictive value of 50–70% to diagnose small bowel CD but does not give any idea on the extent and severity of mucosal inflammation [27]. The Lewis score (LS) and capsule endoscopy Crohn’s disease activity index (CECDAI) assess the disease extent, severity of mucosal inflammation and presence of stenosis (Table 1 and Table 2) [28,29]. The scores are based on a similar principle but differ in the way they are measured. CECDAI is simpler to use and was shown to be more reflective of small bowel inflammation, according to a comparative study [30]. There is strong correlation between the two scores as an LS of 135–790 was shown be equivalent to a CECDAI score of 4.9–6.9 [30,31]. There is moderate correlation with biomarkers such as fecal calprotectin. Although incorporation of these scores in clinical practice can improve clinical outcomes and larger prospective, validation is warranted [7].

Table 1.
Lewis Score for the assessment of small bowel lesions using small bowel capsule endoscopy.
Table 2.
The capsule endoscopy Crohn’s disease activity index (CECDAI) for the assessment of small bowel lesions using video Capsule Endoscopy.
VCE can be useful for detecting occult small bowel inflammation in patients with irritable bowel syndrome (IBS) type symptoms in CD with normal ileo-colonoscopy and cross-sectional imaging [32,33]. Fecal calprotectin as a measure of small bowel inflammatory activity is uncertain in this regard [34]. However, the potential of VCE to over diagnose CD should be borne in mind.
VCE have been shown to diagnose jejunal lesions in more than half of the patients with CD. Jejunal lesions were associated with relapsing disease [35].
Although proximal and superficial small bowel lesions are better identified by VCE than MRE, the risk of capsule retention especially in presence of strictures and frequent incomplete bowel examinations should be kept in mind [36].
Mucosal Healing and Treat to Target
As mentioned above, mucosal healing as treatment target in small bowel CD can improve long term outcomes. A sequential capsule endoscopy study in CD has shown a poor correlation between endoscopic mucosal healing and clinical disease activity scores/inflammatory markers [37]. Deep remission rates of 42% can be achieved with anti-tumor necrosis factor (TNF) therapy or thiopurines, which is comparable to deep remission rates in colon and terminal ileum [38]. There is insufficient information on the temporal relationship and differences between healing of colonic and small bowel lesions. Incomplete VCE examinations, risk of capsule retention especially in the presence of strictures and routine requirement of prior patency capsule testing are the drawbacks of VCE in monitoring small bowel disease [36]. Capsule endoscopes with longer battery life and pan-enteric capsules can overcome the existing drawbacks. Nevertheless, VCE is an emerging tool for surveillance of small bowel CD.
Evaluation of Unexplained Anemia or Obscure GI Bleed in CD
Meta-analysis has shown that VCE has highest diagnostic yield while investigating obscure GI bleed compared to small bowel radiology, CTE and push enteroscopy [39].
Assessment of Postoperative CD Recurrence
Bowel resection is eventually required in 75% of CD patients over 20 years of follow up. On the other hand, post-resection recurrent CD affects 70% patients 20 years post-surgery. Ileo-colonoscopy is the test of choice to diagnose post-operative recurrence of CD. The sensitivity of VCE is lower than ileo-colonoscopy in detecting recurrence in the neo-terminal ileum. Two thirds of the lesions beyond the reach of ileo-colonoscopy can be detected by VCE [40]. Emerging data shows that VCE have incremental diagnostic yield compared to ileo-colonoscopy especially for proximal lesions and can lead to a change in management in more than half of the patients [41]. According to a recent study, ileal recurrence is more likely to predict long term outcomes in CD compared to anastomotic recurrence [42]. Hence, VCE could have the potential to improve clinical outcomes in postoperative CD beyond the scope of ileo-colonoscopy. Moreover, patient acceptance is usually better for VCE than ileo-colonoscopy in this regard due to its non-invasiveness.
Classification of IBD-Unclassified (IBD-U)
IBD-U refers to inflammatory colitis that cannot be classified into UC or Crohn’s colitis. This is important as surgical management differs between the two. Small, uncontrolled studies have demonstrated that VCE can detect new small bowel lesions compatible with CD in 29–40% patients of IBD-U [43,44]. This can impact management especially in pediatric IBD [45]. Although VCE has high sensitivity to rule out small bowel involvement, up to 20% IBD-U patients with normal VCE can develop new small bowel lesions suggestive of CD on follow up [46].
Mimics of Crohn Disease on Capsule Endoscopy
NSAID induced enteropathy is the most common CD mimic on VCE. On VCE, the most common finding is mucosal breaks, and presence of diaphragms (circumferential thin membrane) is characteristic. Most of the cases are asymptomatic but iron deficiency anemia due to acute and chronic gastrointestinal hemorrhage and intestinal obstruction are the main complications. Other presentations are protein losing enteropathy and malabsorption syndrome. Risk of capsule retention is high in NSAID induced enteropathy. Treatment with enteroscopy guided dilation carries a low risk of perforation as the diaphragms do not include muscularis propria [47].
Differentiating small bowel tuberculosis (SBTB) from small bowel CD could be a diagnostic challenge in a tuberculosis endemic area. In prospective study on VCE, ileo-cecal valve involvement was more common in SBTB whereas aphthous ulcers were less frequent compared to CD. Proximal small bowel involvement was seen only in SBTB, although it was not statistically significant [48].
Cryptogenic multifocal ulcerating stenosing enteropathy (CMUSE) presents with chronic abdominal pain and GI blood loss due to idiopathic strictures in the absence of systemic inflammation. VCE carries very high risk of retention and small bowel endoscopy shows shallow, superficial ulcers. Biopsy shows non-specific inflammation limited to submucosa. Although termed cryptogenic, genetic defects in prostaglandin function (e.g., solute carrier organic anion transporter family, member 2A1-SLCO2A1 gene) have been identified [49].
Radiation enteritis presenting with chronic abdominal pain, anemia and VCE showing erythema and mucosal enema can resemble small bowel CD. History of radiation and histology could be helpful in differentiation [50]. Eosinophilic enteritis can show ulcerations and even strictures mimicking CD, which can be differentiated on histology [51]. Autoimmune enteropathy presenting with sprue like diarrhea and malabsorption without dietary triggers can show villous blunting and scalloping on VCE and the histopathology is diagnostic [52]. Behcet’s disease and malignancy of the small bowel (e.g., lymphoma, adenocarcinoma) can also present as small bowel strictures [53].
Capsule Retention
Risk of capsule retention in the general population, suspected CD and established CD are 1–2.5%, 2.6% and 13%, respectively, in the pre-patency capsule era [54]. Current meta-analysis reports retention rates of 2.45% and 4.63% in suspected and established CD, respectively. The retention rates are 2.32% and 2.68%, respectively, when prior cross-sectional imaging and patency capsule testing has been done [55].
Retained capsule should be treated with an observant, conservative approach followed by medical therapy with steroids and biologics failing which endoscopic retrieval or surgery should be attempted [56].
Patency Capsule
Patients with suspected CD at risk of capsule retention (obstructive symptoms or known stenosis) and all patients with established CD should undergo either cross-sectional imaging or patency capsule testing prior to VCE [57]. The two currently available patency capsules (Given and Agile) differ in the number of timer plugs (Given 1 and Agile 2), dissolution start time (Given 40–100 h and Agile 30 h) and composition (Given capsule: lactose, Agile capsules: dissolvable compounds surrounding radio frequency identification tag detectable by X-ray) [58]. Symptomatic intestinal obstruction due to patency capsule is rare and mostly managed conservatively [59]. Drawbacks of patency capsule testing is false positive rates that can be reduced by low dose, spot computed tomography (CT), which determines precise location of capsule. False positive results are common due to colonic retention as a result of prolonged transit time. This can markedly reduce false positive patency testing [60].
Pan-Enteric Capsules
Pan-enteric capsules can evaluate both small bowel and colon. Better diagnostic yield than ileo-colonoscopy (69.7%) have been reported with pan-enteric capsule endoscopy (83.3%) [61]. In pediatric CD, pan-enteric capsules can have comparable sensitivity to ileo-colonoscopy and MRE according to preliminary data [62].
Application of Deep Learning Technology for VCE in CD
Substantial progress has been made in the application of deep learning technology using an artificial neural network for VCE in CD. Automated, fast detection of CD related ulcers and strictures have been reported with high accuracy in recent studies [63,64]. Convolutional neural networks for grading CD ulcerations have shown high accuracy in grading of CD ulcers specifically identifying severe CD related ulcers [65].
2.4. Enteroscopy in CD
Device assisted enteroscopy (DAE) techniques include double balloon enteroscopy (DBE), single balloon enteroscopy (SBE), balloon guided enteroscopy (BGE) and novel motorized spiral enteroscopy (NMSE).
2.4.1. SBE/DBE
SBE is technically easier due to the absence of any balloon at the tip of the enteroscope, unlike DBE. However, DBE has relatively higher depth of insertion, advantageous in presence of adhesions and is less prone to backward slippage during retrograde enteroscopy than SBE [66]. The majority of the studies on DAE in CD are based on DBE than SBE.
2.4.2. BGE
Balloon guided enteroscopy (BGE) is a novel through the scope (TTS), on-demand balloon assisted enteroscopy performed by the push pull technique with the help of a disposable advancing balloon through the working channel (diameter 3.7 mm) of a colonoscope. Therapeutic procedures can be performed through the working channel after removing the balloon. Shorter procedure time, easier learning curve and obviating need for enteroscope and over-tube are the advantages while a relative lack of stability is the disadvantage. This was circumvented by integration of a latex free balloon at the bending section of the colonoscope. The safety and feasibility has been proven in adults as well as in a pediatric group [4,67]. Depth of insertion from trans-oral and trans-anal routes were 158 cm (50–350 cm) and 89 cm (20–150 cm), respectively, and the average procedure time was 15.5 min in adult multi-center study [67]. In the pediatric population, reported depth of insertion were 138 cm (range 100–190 cm) and 143 cm (range 100–170 cm) via antegrade and retrograde routes, respectively. Average procedure time was very low (21.9 min and 12.8 min in the antegrade and retrograde routes, respectively) [4].
2.4.3. NMSE
Conventional spiral enteroscopy uses over-tube with raised spiral edges that is rotated clockwise for advancement of enteroscope pleating small bowel loops. NMSE is composed of a reusable endoscope with an integrated motor, which permits rotation of a short spiral over-tube in the insertion tube portion of the endoscope. Short procedure time, larger working channel (3.2 mm), high diagnostic yield (>80%), greater depth of insertion and higher total enteroscopy rates (>60% with combined antegrade and retrograde approach) are the advantages of NMSE [5].
In a recent large, single center, retrospective study, out of 61 cases of NMSE, the majority were inflammatory lesions (41%) including CD, TB and CMUSE. Therapeutic interventions were done in one quarter of patients, which included stricture dilatation and retrieval of retained capsule [5,68]. NMSE is not suitable in pediatric patients due to large diameter of the over-tube and is technically difficult in post-operative patients due to adhesions.
2.4.4. DAE in Suspected CD
DAE is indicated for confirmation of diagnosis when CD is suspected based on cross sectional imaging (Figure 3A–D) or VCE (Table 3). DAE not only helps in diagnosing CD, it also helps in excluding CD, diagnosing alternate conditions such as NSAID enteropathy leading to NSAID discontinuation and making a surgical decision if a tight stricture is found [69]. The prevalence of new diagnosis of CD in patients with suspected CD varied from 25–75% [4,69,70,71,72,73,74,75,76,77,78]. This wide range is due to variable pre-DAE investigations done in various studies. When CD was suspected based on both MRE and VCE, the prevalence of CD was as high as 75% [78]. Hence, proper patient selection is the key to higher diagnostic yield with DAE. Diagnostic yield for DAE in suspected CD is based on the likelihood that DAE provides information on establishing or refuting a diagnosis. Only a few studies addressed this issue in the true sense. Two studies are worth mentioning in this regard [69,71].
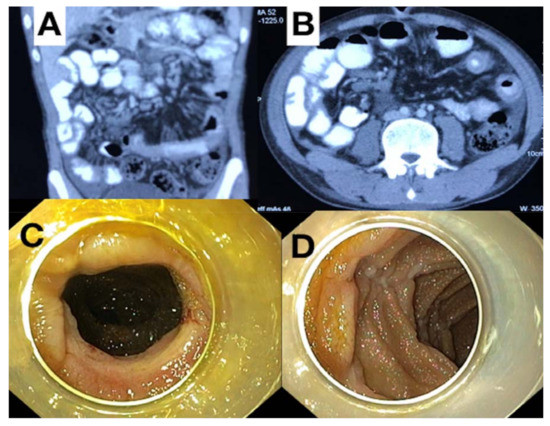
Figure 3.
Cross sectional imaging and enteroscopic images in small bowel Crohn’s disease (CD). (A) Computed tomography (CT) enterography coronal section image showing long segment jejunal thickening with prominent vasa recta in a suspected case of CD; (B) CT enterography image of the same patient showing wall thickening in axial section; (C) Single balloon enteroscopy (SBE) done trans-orally showing a stricture with features of mild inflammation, (D) SBE image of the same patient showing linear ulcers with skip areas in jejunum.
Table 3.
Summary of studies based on device assisted enteroscopy (DAE) in suspected Crohn’s disease (CD) [4,69,70,71,72,73,74,75,76,77,78].
Rahman et al. studied 43 patients with suspected CD, 39.5% were diagnosed as new CD. Diagnostic yield was 79%. DAE altered existing management in 77%. In 17% cases, DBE failed to reach target lesion. Only 1% had perforation. Although CD was diagnosed based on endoscopy and histology, precise histopathological findings were not mentioned [69]. This was addressed in a larger retrospective study of 100 patients with suspected CD by Tun et al. that included follow up data as well. In that study, the proportion of new CD was 38% and diagnostic yield was 71%. Histology was diagnostic in 8%, suggestive in 15%, but in total 45% was initiated on CD treatment based on clinical, VCE and DAE findings. On median follow up of 27 months, 38% were finally diagnosed to have CD. Additionally, two patients each were diagnosed to have small bowel malignancy and tuberculosis on DAE guided biopsy. Two patients with normal DBE developed CD on follow up. This result suggests that histological yield of DAE guided biopsy is low and treatment based on macroscopic findings on DAE can help initiate CD treatment in a substantial number of patients. Moreover, alternate diagnosis of TB and small bowel malignancy can be made on histology [71].
Therefore, DAE is helpful in establishing diagnosis of small bowel CD whereas VCE is more useful in ruling out small bowel CD. Cross sectional imaging like MRE is better for assessment of transmural and extra-luminal disease, whereas luminal disease is better assessed by DAE with additional advantage of histologic sampling [79].
2.4.5. AE in Established CD
DAE can be helpful in established CD to diagnose active small bowel disease that is suspected based on cross-sectional imaging (CTE/MRE) or VCE (Table 4), alteration in medical management, assess requirement of surgical intervention and direct therapeutic interventions like endoscopic therapy for small bowel strictures/bleed and retrieval of retained capsule/foreign body [69]. In a study by Mensink et al., therapy adjustment based on DBE resulted in a decrease in the Crohn’s disease activity index (CDAI) score on follow up [80].
Table 4.
Summary of studies based on device assisted enteroscopy (DAE) in established Crohn’s disease (CD) [4,69,70,75,76,77,78,80].
DAE could be important in evaluation of small bowel activity in CD as VCE and cross-sectional imaging have their own drawbacks in this regard. Incomplete small bowel examination, risk of capsule retention, requirement of patency capsule testing, inability to take biopsy and poor correlation with enteroscopic findings are drawbacks of VCE. VCE is otherwise relatively non-invasive and better tolerated. Nearly one third of patients with abnormal VCE findings had normal DBE results and one fourth with abnormal VCE had different lesions in a study by Rahman et al. Therefore, results of VCE should be interpreted with caution. DAE can also be useful to evaluate small bowel mass in the small bowel CD for ruling out adenocarcinoma on DAE guided biopsy amd may obviate the need for laparotomy [69].
The diagnostic yield of DAE for established CD is higher (77–100%) than in cases of suspected CD (25–75%) [75,76,77,78,79,80,81,82]. However, DAE can be technically difficult leading to inability to reach target lesion in up to 17% cases. Fixation of a mobile small bowel due to active CD or adhesions from stricture or previous surgery can hinder deep enteroscopy. Moreover, complications like transient pain, bleeding and perforation can occur [69].
There is increasing evidence that small bowel mucosal healing may not correspond to colonic mucosal healing. In a post hoc analysis of CD patients treated with anti-TNF, small bowel ulcers detected by DAE were more difficult to heal (36%) than colonic ulcers (79%) and were associated with complicated CD [83]. In a retrospective study, endoscopic evaluation of the deep small bowel was an independent predictor of relapse in CD on clinical remission whereas evaluation of terminal ileum was not. This highlights the importance of deep small bowel evaluation in CD even if in clinical remission to prevent future relapses [84].
2.4.6. DAE Guided Therapeutic Intervention
Small Bowel Strictures
Treatment of small bowel strictures is challenging. Treatment with anti-inflammatory drugs improve obstructive symptoms in symptomatic small bowel strictures but 40% require surgery/EBD within 1 year and 50% require surgery in 4 years [85]. Most of the data on EBD for CD strictures is on ileal and anastomotic strictures is done with ileo-colonoscopy; however, data on EBD for small bowel strictures with DAE is limited [86].
Endoscopic Balloon Dilatation (EBD)
EBD is recommended for symptomatic, de novo or anastomotic, small bowel strictures (less than four closely situated strictures) less than 5 cm in size with minimal inflammatory activity (Figure 4). For asymptomatic small bowel strictures, risk of complications with EBD should be balanced with the benefits of halting progression of asymptomatic stenosis. Cross-sectional imaging (CTE/MRE), or more recently small bowel ultrasound, is being used for evaluation of stricture prior to EBD. Wall thickening, luminal narrowing and pre-stenotic dilatation should be noted prior to EBD using these modalities [87]. Monitored /general anesthesia, fluoroscopic guidance and in-patient admission are not mandatory but should be used if complex strictures and a long procedure time is contemplated in a patient with significant co-morbidity. Carbon dioxide insufflation and prophylactic antibiotics are recommended and warfarin/thienopyridines should be discontinued for 5 days (aspirin could be continued).
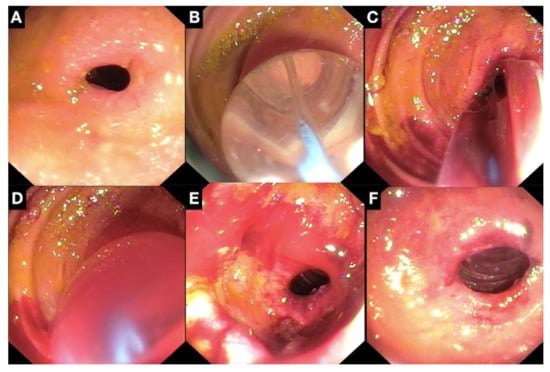
Figure 4.
Endoscopic balloon dilation (EBD) of fibrotic proximal jejunal stricture done. (A) Symptomatic proximal jejunal stricture detected on single balloon enteroscopy reached by pediatric colonoscope; (B) Graded dilatation was done with controlled radial expansion (CRE) balloon up to 13.5 mm, direct through the balloon visualization done to detect endoscopic tearing during balloon dilation; (C) Post dilatation bleeding noted at dilation site; (D) Mechanical pressure applied by balloon tamponade with CRE balloon. (E) Post balloon tamponade, mild ooze noted from structure; (F) Complete hemostasis achieved after hypertonic glucose spray at dilation site with no delayed bleed on follow up, remains asymptomatic for 6 months post dilation.
Outcomes of EBD for Small Bowel Strictures
The most common therapeutic intervention in small bowel Crohn’s disease is endoscopic balloon dilatation (EBD). Table 5 summarizes the published literature on EBD for small bowel strictures in CD. In a recent meta-analysis, data of 218 patients and 384 EBD were analyzed. It showed high technical success rate (95%) that is comparable to that for ileo-cecal (90%) and gastroduodenal (100%) strictures. Short term clinical efficacy (82.3%) was also comparable to clinical success rates of EBD for ileo-cecal (80.8%) and gastroduodenal (87%) strictures. Recurrent symptoms were seen in half of the patients (48.3%) compared to recurrence rate of 47.5% and 70.5% for ileo-cal and gastro-duodenal strictures over 2 years follow up. Repeat dilatation or surgery were required in 38.8% and 27.4% patients, respectively [88]. Surgery rates in ileo-cecal and gastroduodenal strictures post EBD were 28.6% and 30.8%, respectively. Although a technical success, clinical success and long term success were similar to other strictures, complication rates of small bowel stricture was higher (5.3%) compared to ileo-cecal (2.8%) and gastroduodenal (2.9%) strictures [89,90]. This finding is due to the technically challenging procedure with DAE compared to that with endoscope or colonoscope.
Table 5.
Summary of published literature on endoscopic balloon dilatation (EBD) for small bowel strictures in Crohn’s disease with device assisted enteroscopy (DAE); SBE—single balloon enteroscopy, DBE—double balloon enteroscopy, BGE—balloon guided enteroscopy [70,73,81,91,92,93,94,95,96,97,98,99,100,101].
Intra-procedural bleed (Figure 4C–F) with hemodynamic instability and post-procedure bleeding requiring hospitalization or blood transfusion should be tried with volume resuscitation and rescue endoscopy and hemostasis with clips/mechanical pressure/epinephrine injection or hypertonic glucose spraying failing which angiographic embolization or surgery may be required in rare instances. For intra-procedural perforation, endoscopic closure could be attempted failing which surgical intervention is warranted.
Factors Predicting Outcomes of EBD
According to the meta-analysis, fibrotic strictures, absence of inflammatory disease elsewhere, higher body mass index (BMI) and use of anti-inflammatory drugs lower the risk of re-intervention following EBD [88]. Deep ulcers in a strictured segment increases risk of bleeding and perforation; however, superficial ulcers should not preclude EBD [91]. Concomitant use of steroids (prednisolone ≥20 mg/day) but not biologics is associated with increased risk of complications with EBD [89]. Advanced disease usually leads to weight loss that could be the explanation of better outcome in patients with a high BMI. Pre-stenotic dilatation signifying long standing disease and stricture length > 5 cm were significant risk factors for failure of EBD and future surgery. Every 1 cm increase in stricture size increases the risk of future surgery by 8% [90]. Adjacent abscess and fistula are contraindications to EBD [91]. De novo CD strictures have low short-term clinical efficacy compared to anastomotic strictures, although long term outcomes are not different. EBD is safe and effective for less than four strictures in close proximity to each other compared to more than equal to four strictures located far away [91]. Asian ethnicity was associated with low short term clinical efficacy, lower recurrence and a higher risk of surgery that could be related to protocol for EBD, different disease phenotype and a lower threshold for surgery. Disease located in jejunum or proximal ileum were associated with higher risk of re-dilatation or surgery [88]. Concurrent intra-lesional steroid injection is not recommended and there is no definite benefit of intra-lesional anti-TNF therapy [91].
Graded Versus One Step Dilation
It is not clear whether a graded dilatation is better than one time dilatation, although generally graded dilatation is recommended to reduce chances of bleeding and perforation. Usually, graded dilation is done up to 18–20 mm, but smaller balloon sizes are preferred for small bowel strictures [91]. Graded dilatation was associated with higher short term efficacy but 65% higher risk of recurrent symptoms. Although complication rates (3.2%) were higher with graded dilatation compared to one-step dilatation (0.7%), it was not statistically significant due to overall low complication rates. Balloon size (15.8 mm) was lower with graded compared to one-step dilatation (17.2 mm) [88]. Future studies are warranted in this regard.
Endoscopic Techniques Other Than EBD for Small Bowel Strictures
Endoscopic stricturotomy (horizontal or radial incision in strictures) and stricturectomy (endoscopic electro-incision along with clip placement) can be used as rescue therapies for CD related short strictures (<3 cm) where EBD has failed. Delayed bleeding may occur in a higher frequency than in EBD although the risk of perforation is lower. Full covered removal metal stents have been used successfully as rescue therapy for terminal ileal and ileo-colonic short, fibrostenotic stricture [91]. However, data is scarce on the effect of these modalities in small bowel strictures. Risk of migration, perforation and fistula formation are drawbacks of metal stents, which can be circumvented in future by biodegradable stents specifically designed for CD [102,103]. In the recent meta-analysis of EBD of small bowel strictures, 0.54% and 2.7% patients were treated with electro-incision and stents, respectively [88].
2.4.7. DAE in Pediatric Patients
DAE is technically difficult in children due to small abdominal cavity, thin abdominal wall and narrow lumen. DAE is feasible in children more than 3 years old and with a body weight of more than 14 kg. Single or double balloon enteroscopy and balloon guided enteroscopy have been used extensively in pediatric CD (Table 3 and Table 4). IBD-U reclassification is more relevant for pediatric population. DAE is safe according to large DBE and SBE series [75,76,77,104,105]. Currently available motorized spiral enteroscopy is not feasible in children due to the large diameter of the scope.
2.5. Intra-Operative Enteroscopy (IOE) in CD
Although the role of IOE is becoming limited with current advances in small bowel endoscopy, IOE has been shown to be useful in surgical decision of small bowel CD. IOE can help in assessment of severity of stricture (severe strictures do not allow passage of enteroscope) and deciding the extent of surgical resection. Supposedly mild stricture on inspection and palpation at laparotomy could turn out to be severe, non-passable stricture on IOE altering surgical extent [106,107].
3. Conclusions
Direct endoscopic evaluation of the small bowel has revolutionized diagnostic and therapeutic management of small bowel CD. Small bowel endoscopy is useful for diagnosing small bowel CD with normal ileo-colonoscopy. In this scenario, VCE in the absence of known stenosis or obstructive symptoms carries low risk of capsule retention. DAE with endoscopic biopsy may help rule out mimics of small bowel CD; however, histological yield is poor in small bowel CD. Small bowel endoscopy could also be helpful in IBD-U. In post-operative small bowel disease, VCE may be helpful to evaluate recurrence. In established CD, small bowel disease extent, severity and mucosal healing can be assessed by both VCE and DAE. VCE has high risk of retention in established CD and hence should be preceded by cross sectional imaging or patency capsule testing. The indications of small bowel therapeutic enteroscopy are expanding and include treatment of small bowel stricture/bleeding and removal of retained capsule or foreign body. EBD has been extensively used in treatment of small bowel stricture. Newer techniques for treatment of strictures in CD like electro-incision, stricturoplasty and stenting need to be evaluated in small bowel strictures.
Author Contributions
All authors have contributed to the concept and writing of paper. Conceptualization: R.B. and P.P.; Writing—Original Draft Preparation, P.P.; Writing—Review and Editing, R.B. and P.P.; Visualization, P.P.; Supervision, R.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study as it was a review article that did not constitute human subject research.
Informed Consent Statement
Informed consent was taken from all the subjects involved in the study for use of anonymized images of small bowel endoscopy.
Acknowledgments
We acknowledge Pradeep Rebala for providing intra-operative photos of retained capsule endoscope removal at laparotomy.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Farmer, R.G.; Hawk, W.A.; Turnbull, R.B., Jr. Clinical patterns in Crohn’s disease: A statistical study of 615 cases. Gastroenterology 1975, 68, 627–635. [Google Scholar] [CrossRef]
- Valle, J.; Alcantara, M.; Perez-Grueso, M.J.; Navajas, J.; Muñoz-Rosas, C.; Legaz, M.L.; Cuena, R.; Carrobles, J.M. Clinical features of patients with negative results from traditional diagnostic work-up and Crohn’s disease findings from capsule endoscopy. J. Clin. Gastroenterol. 2006, 40, 692–696. [Google Scholar] [CrossRef] [PubMed]
- Doherty, G.A.; Moss, A.C.; Cheifetz, A.S. Capsule endoscopy for small-bowel evaluation in Crohn’s disease. Gastrointest. Endosc. 2011, 74, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Broide, E.; Shalem, T.; Richter, V.; Matalon, S.; Shirin, H. The safety and feasibility of a new through-the-scope balloon-assisted enteroscopy in children. J. Pediatr. Gastroenterol. Nutr. 2020, 71, e6–e11. [Google Scholar] [CrossRef] [PubMed]
- Ramchandani, M.; Rughwani, H.; Inavolu, P.; Singh, A.P.; Tevethia, H.V.; Jagtap, N.; Sekaran, A.; Kanakagiri, H.; Darishetty, S.; Reddy, D.N. Diagnostic yield and therapeutic impact of novel motorized spiral enteroscopy in small-bowel disorders: A single-center, real-world experience from a tertiary care hospital (with video). Gastrointest. Endosc. 2021, 93, 616–626. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.R.; Kim, J.O.; Byeon, J.S.; Yang, D.H.; Ko, B.M.; Goong, H.J.; Jang, H.J.; Park, S.J.; Kim, E.R.; Hong, S.N.; et al. Korean Association for the study of intestinal disease (KASID). Enteroscopy in Crohn’s disease: Are there any changes in role or outcomes over time? A KASID multicenter study. Gut Liver 2020, 6. [Google Scholar] [CrossRef]
- McCain, J.D.; Pasha, S.F.; Leighton, J.A. Role of capsule endoscopy in inflammatory bowel disease. Gastrointest. Endosc. Clin. N. Am. 2021, 31, 345–361. [Google Scholar] [CrossRef]
- Pennazio, M.; Spada, C.; Eliakim, R.; Keuchel, M.; May, A.; Mulder, C.J.; Rondonotti, E.; Adler, S.N.; Albert, J.; Baltes, P.; et al. Small-bowel capsule endoscopy and device-assisted enteroscopy for diagnosis and treatment of small-bowel disorders: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2015, 47, 352–376. [Google Scholar] [CrossRef]
- Bourreille, A.; Ignjatovic, A.; Aabakken, L.; Loftus, E.V., Jr.; Eliakim, R.; Pennazio, M.; Bouhnik, Y.; Seidman, E.; Keuchel, M.; Albert, J.G.; et al. Role of small-bowel endoscopy in the management of patients with inflammatory bowel disease: An international OMED-ECCO consensus. Endoscopy 2009, 41, 618–637. [Google Scholar] [CrossRef]
- Condino, G.; Calabrese, E.; Onali, S. Small bowel capsule endoscopy for assessing early postoperative recurrence of Crohn’s disease: A prospective longitudinal study. Gastroenterology 2013, 144, S425. [Google Scholar] [CrossRef]
- Van Assche, G.; Dignass, A.; Panes, J.; Beaugerie, L.; Karagiannis, J.; Allez, M.; Ochsenkühn, T.; Orchard, T.; Rogler, G.; Louis, E.; et al. European Crohn’s and Colitis Organisation (ECCO). The second European evidence based consensus on the diagnosis and management of Crohn’s disease: Definitions and diagnosis. J. Crohns Colitis 2010, 4, 7–27. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.D.; Nathan, T.; Rafaelsen, S.R.; Kjeldsen, J. Ileoscopy reduces the need for small bowel imaging in suspected Crohn’s disease. Dan. Med. J. 2012, 59, A4491. [Google Scholar] [PubMed]
- Banerjee, R.; Pal, P.; Mak, J.W.Y.; Ng, S.C. Challenges in the diagnosis and management of inflammatory bowel disease in resource-limited settings in Asia. Lancet Gastroenterol. Hepatol. 2020, 5, 1076–1088. [Google Scholar] [CrossRef]
- Dionisio, P.M.; Gurudu, S.R.; Leighton, J.A.; Leontiadis, G.I.; Fleischer, D.E.; Hara, A.K.; Heigh, R.I.; Shiff, A.D.; Sharma, V.K. Capsule endoscopy has a significantly higher diagnostic yield in patients with suspected and established small-bowel Crohn’s disease: A meta-analysis. Am. J. Gastroenterol. 2010, 105, 1240–1248. [Google Scholar] [CrossRef] [PubMed]
- Tukey, M.; Pleskow, D.; Legnani, P.; Cheifet, A.S.; Moss, A.C. The utility of capsule endoscopy in patients with suspected Crohn′s disease. Am. J. Gastroenterol. 2009, 104, 2734–2739. [Google Scholar] [CrossRef]
- Solem, C.A.; Loftus, E.V., Jr.; Fletcher, J.G.; Baron, T.H.; Gostout, C.J.; Petersen, B.T.; Tremaine, W.J.; Egan, L.J.; Faubion, W.A.; Schroeder, K.W.; et al. Small-bowel imaging in Crohn’s disease: A prospective, blinded, 4-way comparison trial. Gastrointest. Endosc. 2008, 68, 255–266. [Google Scholar] [CrossRef] [PubMed]
- González-Suárez, B.; Rodriguez, S.; Ricart, E.; Ordás, I.; Rimola, J.; Díaz-González, Á.; Romero, C.; de Miguel, C.R.; Jáuregui, A.; Araujo, I.K.; et al. Comparison of capsule endoscopy and magnetic resonance enterography for the assessment of small bowel lesions in Crohn’s disease. Inflamm. Bowel Dis. 2018, 24, 775–780. [Google Scholar] [CrossRef] [PubMed]
- Kopylov, U.; Yung, D.E.; Engel, T.; Vijayan, S.; Har-Noy, O.; Katz, L.; Oliva, S.; Avni, T.; Battat, R.; Eliakim, R.; et al. Diagnostic yield of capsule endoscopy versus magnetic resonance enterography and small bowel contrast ultrasound in the evaluation of small bowel Crohn’s disease: Systematic review and meta-analysis. Dig. Liver Dis. 2017, 49, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.D.; Nathan, T.; Rafaelsen, S.R.; Kjeldsen, J. Diagnostic accuracy of capsule endoscopy for small bowel Crohn’s disease is superior to that of MR enterography or CT enterography. Clin. Gastroenterol. Hepatol. 2011, 9, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Girelli, C.M.; Porta, P.; Malacrida, V.; Barzaghi, F.; Rocca, F. Clinical outcome of patients examined by capsule endoscopy for suspected small bowel Crohn’s disease. Dig. Liver Dis. 2007, 39, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Hall, B.; Holleran, G.; Costigan, D.; McNamara, D. Capsule endoscopy: High negative predictive value in the long term despite a low diagnostic yield in patients with suspected Crohn’s disease. United Eur. Gastroenterol. J. 2013, 1, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Dilauro, S.; Crum-Cianflone, N.F. Ileitis: When it is not Crohn’s disease. Curr. Gastro. Enterol. Rep. 2010, 12, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, J.L.; Eisen, G.M.; Lewis, B.; Gralnek, I.M.; Zlotnick, S.; Fort, J.G. Investigators. Video capsule endoscopy to prospectively assess small bowel injury with celecoxib, naproxen plus omeprazole, and placebo. Clin. Gastroenterol. Hepatol. 2005, 3, 133–141. [Google Scholar] [CrossRef]
- Jung, E.S.; Lee, S.P.; Kae, S.H.; Kim, J.H.; Kim, H.S.; Jang, H.J. Diagnostic accuracy of fecal calprotectin for the detection of small bowel Crohn’s disease through capsule endoscopy: An updated meta-analysis and systematic review. Gut Liver 2020, 24. [Google Scholar] [CrossRef]
- Pal, P.; Reddy, D.N.; Nabi, Z. Role of Small Bowel Endoscopy in Diagnosis and Management of Inflammatory Bowel Disease: Current Perspective, Endoscopy in Small Bowel Diseases; IntechOpen: London, UK, 2021. [Google Scholar] [CrossRef]
- Bouguen, G.; Levesque, B.G.; Feagan, B.G.; Kavanaugh, A.; Peyrin-Biroulet, L.; Colombel, J.F.; Hanauer, S.B.; Sandborn, W.J. Treat to target: A proposed new paradigm for the management of Crohn’s disease. Clin. Gastroenterol. Hepatol. 2015, 13, 1042–1050.e2. [Google Scholar] [CrossRef]
- Mow, W.S.; Lo, S.K.; Targan, S.R.; Dubinsky, M.C.; Treyzon, L.; Abreu-Martin, M.T.; Papadakis, K.A.; Vasiliauskas, E.A. Initial experience with wireless capsule enteroscopy in the diagnosis and management of inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2004, 2, 31–40. [Google Scholar] [CrossRef]
- Gralnek, I.M.; Defranchis, R.; Seidman, E.; Leighton, J.A.; Legnani, P.; Lewis, B.S. Development of a capsule endoscopy scoring index for small bowel mucosal inflammatory change. Aliment. Pharmacol. Ther. 2008, 27, 146–154. [Google Scholar] [CrossRef]
- Gal, E.; Geller, A.; Fraser, G.; Levi, Z.; Niv, Y. Assessment and validation of the new capsule endoscopy Crohn’s disease activity index (CECDAI). Dig. Dis. Sci. 2008, 53, 1933–1937. [Google Scholar] [CrossRef]
- Omori, T.; Kambayashi, H.; Murasugi, S.; Ito, A.; Yonezawa, M.; Nakamura, S.; Tokushige, K. Comparison of lewis score and capsule endoscopy Crohn’s disease activity index in patients with Crohn’s disease. Dig. Dis. Sci. 2020, 65, 1180–1188. [Google Scholar] [CrossRef]
- Yablecovitch, D.; Lahat, A.; Neuman, S.; Levhar, N.; Avidan, B.; Ben-Horin, S.; Eliakim, R.; Kopylov, U. The Lewis score or the capsule endoscopy Crohn’s disease activity index: Which one is better for the assessment of small bowel inflammation in established Crohn’s disease? Ther. Adv. Gastroenterol. 2018, 11, 1756283X17747780. [Google Scholar] [CrossRef]
- Fairbrass, K.M.; Costantino, S.J.; Gracie, D.J.; Ford, A.C. Prevalence of irritable bowel syndrome-type symptoms in patients with inflammatory bowel disease in remission: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 1053–1062. [Google Scholar] [CrossRef]
- Niv, Y. Diagnostic value of capsule endoscopy during relapse in co-morbid irritable bowel syndrome and Crohn’s disease. Eur. J. Gastroenterol. Hepatol. 2004, 16, 1073–1074. [Google Scholar] [CrossRef] [PubMed]
- Sipponen, T.; Haapamäki, J.; Savilahti, E.; Alfthan, H.; Hämäläinen, E.; Rautiainen, H.; Koskenpato, J.; Nuutinen, H.; Färkkilä, M. Fecal calprotectin and S100A12 have low utility in prediction of small bowel Crohn’s disease detected by wireless capsule endoscopy. Scand. J. Gastroenterol. 2012, 47, 778–784. [Google Scholar] [CrossRef] [PubMed]
- Flamant, M.; Trang, C.; Maillard, O.; Sacher-Huvelin, S.; Rhun, M.L.; Galmiche, J.P.; Bourreille, A. The prevalence and outcome of jejunal lesions visualized by small bowel capsule endoscopy in Crohn’s disease. Inflamm. Bowel Dis. 2013, 19, 1390–1396. [Google Scholar] [CrossRef] [PubMed]
- Annese, V.; Manetti, N. Capsule endoscopy in Crohn’s disease: Is there enough light in the tunnel? J. Crohns Colitis 2014, 8, 1598–1600. [Google Scholar] [CrossRef] [PubMed]
- Niv, E.; Fishman, S.; Kachman, H.; Arnon, R.; Dotan, I. Sequential capsule endoscopy of the small bowel for follow-up of patients with known Crohn’s disease. J. Crohns Colitis Mar. 2014, 22, 1616–1623. [Google Scholar] [CrossRef] [PubMed]
- Hall, B.; Holleran, G.; Chin, J.L.; Smith, S.; Ryan, B.; Mahmud, N.; Smith, S.; Ryan, B.; Mahmud, N.; McNamara, D. A prospective 52 week mucosal healing assessment of small bowel Crohn’s disease as detected by capsule endoscopy. J. Crohns Colitis Sep. 2014, 22, 1601–1609. [Google Scholar] [CrossRef]
- Leighton, J.A.; Triester, S.L.; Sharma, V.K. Capsule endoscopy: A meta-analysis for use with obscure gastrointestinal bleeding and Crohn’s disease. Gastrointest. Endosc. Clin. N. Am. 2006, 16, 229–250. [Google Scholar] [CrossRef]
- Bourreille, A.; Jarry, M.; D’Halluin, P.N.; Ben-Soussan, E.; Maunoury, V.; Bulois, P.; Sacher-Huvelin, S.; Vahedy, K.; Lerebours, E.; Heresbach, D. Wireless capsule endoscopy versus ileocolonoscopy for the diagnosis of postoperative recurrence of Crohn’s disease: A prospective study. Gut 2006, 55, 978–983. [Google Scholar] [CrossRef]
- Beltrán, V.P.; Nos, P.; Bastida, G.; Bastida, G.; Beltrán, B.; Argüello, L.; Aguas, M.; Rubín, A.; Pertejo, V.; Sala, T. Evaluation of postsurgical recurrence in Crohn’s disease: A new indication for capsule endoscopy? Gastrointest. Endosc. 2007, 66, 533–540. [Google Scholar] [CrossRef]
- Hammoudi, N.; Auzolle, C.; Minh, M.L.T.; Boschetti, G.; Bezault, M.; Buisson, A.; Pariente, B.; Treton, X.; Seksik, P.; Fumery, M.; et al. Postoperative endoscopic recurrence on the neoterminal ileum but not on the anastomosis is mainly driving long-term outcomes in Crohn’s disease. Am. J. Gastroenterol. 2020, 115, 1084–1093. [Google Scholar] [CrossRef]
- Lo, S.; Zaidel, O.; Tabibzadeh, S.; Papadakis, K.A.; Leo, T.; Kimble, J.; Vasiliauskas, E. Utility of wireless capsule enteroscopy (WCE) and IBD serology in reclassifying indeterminate colitis (IC). Gastroenterology 2003, 124, A192. [Google Scholar] [CrossRef]
- Kalla, R.; McAlindon, M.E.; Drew, K.; Sidhu, R. Clinical utility of capsule endoscopy in patients with Crohn’s disease and inflammatory bowel disease unclassified. Eur. J. Gastroenterol. Hepatol. 2013, 25, 706–713. [Google Scholar] [CrossRef]
- Min, S.B.; Le-Carlson, M.; Singh, N.; Nylund, C.M.; Gebbia, J.; Haas, K.; Lo, S.; Mann, N.; Melmed, G.Y.; Rabizadeh, S.; et al. Video capsule endoscopy impacts decision making in pediatric IBD: A single tertiary care center experience. Inflamm. Bowel Dis. 2013, 19, 2139–2145. [Google Scholar] [CrossRef]
- Maunoury, V.; Sovoye, G.; Bourreille, A.; Bouhnik, Y.; Jarry, M.; Sacher-Huvelin, S.; Ben Soussan, E.; Lerebours, E.; Galmiche, J.P.; Colombel, J.F. Value of wireless capsule endoscopy in patients with indeterminate colitis (inflammatory bowel disease type unclassified). Inflamm. Bowel Dis. 2007, 13, 152–155. [Google Scholar] [CrossRef]
- Lim, Y.J.; Yang, C.-H. Non-steroidal anti-inflammatory drug-induced enteropathy. Clin. Endosc. 2012, 45, 138–144. [Google Scholar] [CrossRef]
- Rana, S.S.; Sharma, V.; Sharma, R.; Nada, R.; Gupta, R.; Bhasin, D.K. Capsule endoscopy in small bowel Crohn’s disease and tuberculosis. Trop. Doct. 2017, 47, 113–118. [Google Scholar] [CrossRef]
- Singh, A. Cryptogenic multifocal ulcerating stenosing enteropathy(CMUSE) and/or chronic non-specific multiple ulcers of the small intestine(CNSU) and non-granulomatous ulcerating jejunoileitis (NGUJI). Curr. Gastroenterol. Rep. 2019, 10, 53. [Google Scholar] [CrossRef]
- Kim, H.M.; Kim, Y.J.; Kim, H.J.; Park, S.W.; Bang, S.; Song, S.Y. A pilot study of capsule endoscopy for the diagnosis of radiation enteritis. Hepatogastroenterology 2011, 58, 459–464. [Google Scholar]
- Okuda, K.; Daimon, Y.; Iwase, T.; Mitsufuji, S. Novel findings of capsule endoscopy and double-balloon enteroscopy in a case of eosinophilic gastroenteritis. Clin. J. Gastroenterol. 2013, 6, 16–19. [Google Scholar] [CrossRef]
- Akram, S.; Murray, J.A.; Pardi, D.S.; Alexander, G.L.; Schaffner, J.A.; Russo, P.A.; Abraham, S.C. Adult autoimmune enteropathy: Mayo Clinic Rochester experience. Clin. Gastroenterol. Hepatol. 2007, 5, 1282–1290. [Google Scholar] [CrossRef] [PubMed]
- Durmush, D.; Kaffes, A.J. Small bowel strictures. Curr. Opin. Gastroenterol. 2019, 35, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Cheifetz, A.S.; Kornbluth, A.A.; Legnani, P.; Schmelkin, I.; Brown, A.; Lichtiger, S.; Lewis, B.S. The risk of retention of the capsule endoscope in patients with known or suspected Crohn’s disease. Am. J. Gastroenterol. 2006, 101, 2218–2222. [Google Scholar] [CrossRef] [PubMed]
- Pasha, S.F.; Pennazio, M.; Rondonotti, E.; Wolf, D.; Buras, M.R.; Albert, J.G.; Cohen, S.A.; Cotter, J.; D’Haens, G.; Eliakim, R.; et al. Capsule retention in Crohn’s disease: A meta-analysis. Inflamm. Bowel Dis. 2020, 26, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Rondonotti, E. Capsule retention: Prevention, diagnosis and management. Ann. Transl. Med. 2017, 5, 198. [Google Scholar] [CrossRef] [PubMed]
- Yadav, A.; Heigh, R.I.; Hara, A.K.; Decker, G.A.; Crowell, M.D.; Gurudu, S.R.; Pasha, S.F.; Fleischer, D.E.; Harris, L.A.; Post, J.; et al. Performance of the patency capsule compared with nonenteroclysis radiologic examinations in patients with known or suspected intestinal strictures. Gastrointest. Endosc. 2011, 74, 834–839. [Google Scholar] [CrossRef]
- Caunedo-Alvarez, A.; Romero-Vazquez, J.; Herrerias-Gutierrez, J.M. Patency and agile capsules. World J. Gastroenterol. 2008, 14, 5269–5273. [Google Scholar] [CrossRef]
- Rasmussen, B.; Nathan, T.; Jensen, M.D. Symptomatic patency capsule retention in suspected Crohn’s disease. J. Crohns Colitis 2016, 10, 1445–1447. [Google Scholar] [CrossRef][Green Version]
- Silva, M.; Cardoso, H.; Cunha, R.; Peixoto, A.; Gaspar, R.; Gomes, S.; Santos, A.L.; Lopes, S.; Macedo, G. Evaluation of small-bowel patency in Crohn’s disease: Prospective study with a patency capsule and computed tomography. GE Port. J. Gastroenterol. 2019, 26, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Leighton, J.A.; Helper, D.J.; Gralnek, I.M.; Dotan, I.; Fernandez-Urien, I.; Lahat, A.; Malik, P.; Mullin, G.E.; Rosa, B. Comparing diagnostic yield of a novel pan-enteric video capsule endoscope with ileocolonoscopy in patients with active Crohn’s disease: A feasibility study. Gastrointest. Endosc. 2017, 85, 196–205. [Google Scholar] [CrossRef]
- Oliva, S.; Aloi, M.; Viola, F.; Mallardo, S.; Civitelli, F.; Maccioni, F.; Hassan, C.; Papoff, P.; Cucchiara, S.; Cohen, S.A. A Treat to Target Strategy Using Panenteric Capsule Endoscopy in Pediatric Patients With Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2019, 17, 2060–2067. [Google Scholar] [CrossRef]
- Klang, E.; Barash, Y.; Margalit, R.Y.; Soffer, S.; Shimon, O.; Albshesh, A.; Ben-Horin, S.; Amitai, M.M.; Eliakim, R.; Kopylov, U. Deep learning algorithms for automated detection of Crohn’s disease ulcers by video capsule endoscopy. Gastrointest. Endosc. 2020, 91, 606–613.e2. [Google Scholar] [CrossRef]
- Klang, E.; Grinman, A.; Soffer, S.; Margalit Yehuda, R.; Barzilay, O.; Amitai, M.M.; Konen, E.; Ben-Horin, S.; Eliakim, R.; Barash, Y.; et al. Automated detection of Crohn’s disease intestinal strictures on capsule endoscopy images using deep neural networks. J. Crohns Colitis 2020, 20, 749–756. [Google Scholar]
- Barash, Y.; Azaria, L.; Soffer, S.; Yehuda, R.M.; Shlomi, O.; Ben-Horin, S.; Eliakim, R.; Klang, E.; Kopylov, U. Ulcer severity grading in video capsule images of patients with Crohn’s disease: An ordinal neural network solution. Gastrointest. Endosc. 2021, 93, 187–192. [Google Scholar] [CrossRef]
- Nardo, G.D.; Esposito, G.; Ziparo, C.; Micheli, F.; Masoni, L.; Villa, M.P.; Parisi, P.; Manca, M.B.; Baccini, F.; Corleto, V.D. Enteroscopy in children and adults with inflammatory bowel disease. World J. Gastroenterol. 2020, 21, 5944–5958. [Google Scholar] [CrossRef]
- Ali, R.; Wild, D.; Shieh, F.; Diehl, D.L.; Fischer, M.; Tamura, W.; Rubin, D.T.; Kumbhari, V.; Okolo, P.; Storm, A. Deep enteroscopy with a conventional colonoscope: Initial multicenter study by using a through-the-scope balloon catheter system. Gastrointest. Endosc. 2015, 82, 855–860. [Google Scholar] [CrossRef]
- Inavolu, P.; Singh, A.P.; Kanakagiri, H.; Reddy, D.N.; Ramchandani, M. Motorized spiral enteroscope-assisted retrieval of video capsule in a patient with Crohn’s disease. VideoGIE 2020, 22, 488–491. [Google Scholar] [CrossRef]
- Rahman, A.; Ross, A.; Leighton, J.A.; Schembre, D.; Gerson, L.; Lo, S.K.; Waxman, I.; Dye, C.; Semrad, C. Double-balloon enteroscopy in Crohn’s disease: Findings and impact on management in a multicenter retrospective study. Gastrointest. Endosc. 2015, 82, 102–107. [Google Scholar] [CrossRef]
- Holleran, G.; Valerii, G.; Tortora, A.; Scaldaferri, F.; Conti, S.; Amato, A.; Gasbarrini, A.; Costamagna, G.; Riccioni, M.E. The use of single balloon enteroscopy in Crohn’s disease and its impact on clinical outcome. Scand. J. Gastroenterol. 2018, 53, 925–929. [Google Scholar] [CrossRef]
- Tun, G.S.; Rattehalli, D.; Sanders, D.S.; McAlindon, M.E.; Drew, K.; Sidhu, R. Clinical utility of double-balloon enteroscopy in suspected Crohn’s disease: A single-centre experience. Eur. J. Gastroenterol. Hepatol. 2016, 28, 820–825. [Google Scholar] [CrossRef]
- Christian, K.E.; Kapoor, K.; Goldberg, E.M. Performance characteristics of retrograde single-balloon endoscopy: A single center experience. World J. Gastrointest. Endosc. 2016, 8, 501–507. [Google Scholar] [CrossRef]
- Navaneethan, U.; Vargo, J.J.; Menon, K.V.; Sanaka, M.R.; Tsai, C.J. Impact of balloon-assisted enteroscopy on the diagnosis and management of suspected and established small-bowel Crohn’s disease. Endosc. Int. Open 2014, 2, E201–E206. [Google Scholar] [CrossRef]
- Schulz, C.; Mönkemüller, K.; Salheiser, M.; Bellutti, M.; Schütte, K.; Malfertheiner, P. Double-balloon enteroscopy in the diagnosis of suspected isolated Crohn’s disease of the small bowel. Dig. Endosc. 2014, 26, 236–242. [Google Scholar] [CrossRef]
- Urs, A.N.; Martinelli, M.; Rao, P.; Thomson, M.A. Diagnostic and therapeutic utility of double-balloon enteroscopy in children. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 204–212. [Google Scholar] [CrossRef]
- Uchida, K.; Yoshiyama, S.; Inoue, M.; Koike, Y.; Yasuda, H.; Fujikawa, H.; Okita, Y.; Araki, T.; Tanaka, K.; Kusunoki, M. Double balloon enteroscopy for pediatric inflammatory bowel disease. Pediatr. Int. 2012, 54, 806–809. [Google Scholar] [CrossRef]
- Ridder, L.D.; Mensink, P.B.; Lequin, M.H.; Aktas, H.; de Krijger, R.R.; van der Woude, C.J.; Escher, J.C. Single- balloon enteroscopy, magnetic resonance enterography, and abdominal US useful for evaluation of small-bowel disease in children with (suspected) Crohn’s disease. Gastrointest. Endosc. 2012, 75, 87–94. [Google Scholar] [CrossRef]
- Nardo, G.D.; Oliva, S.; Aloi, M.; Rossi, P.; Casciani, E.; Masselli, G.; Ferrari, F.; Mallardo, S.; Stronati, L.; Cucchiara, S. Usefulness of single-balloon enteroscopy in pediatric Crohn’s disease. Gastrointest. Endosc. 2012, 75, 80–86. [Google Scholar] [CrossRef]
- Seiderer, J.; Herrmann, K.; Diepolder, H.; Schoenberg, S.O.; Wagner, A.C.; Göke, B.; Ochsenkühn, T.; Schäfer, C. Double-balloon enteroscopy versus magnetic resonance enteroclysis in diagnosing suspected small-bowel Crohn’s disease: Results of a pilot study. Scand. J. Gastroenterol. 2007, 42, 1376–1385. [Google Scholar] [CrossRef]
- Mensink, P.B.; Groenen, M.J.; Van Buuren, H.R.; Kuipers, E.J.; Van der Woude, C.J. Double-balloon enteroscopy in Crohn’s disease patients suspected of small bowel activity: Findings and clinical impact. J. Gastroenterol. 2009, 44, 271–276. [Google Scholar] [CrossRef]
- Kondo, J.; Iijima, H.; Abe, T.; Komori, M.; Hiyama, S.; Ito, T.; Nakama, A.; Tominaga, K.; Kubo, M.; Suzuki, K.; et al. Roles of double-balloon endoscopy in the diagnosis and treatment of Crohn’s disease: A multicenter experience. J. Gastroenterol. 2010, 45, 713–720. [Google Scholar] [CrossRef]
- Möschler, O.; May, A.; Müller, M.K.; Ell, C. German DBE Study group. Complications in and performance of double-balloon enteroscopy (DBE): Results from a large prospective DBE database in Germany. Endoscopy 2011, 43, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, K.; Fujii, T.; Suzuki, K.; Shimizu, H.; Motobayashi, M.; Hibiya, S.; Saito, E.; Nagahori, M.; Watanabe, M.; Ohtsuka, K. Small bowel healing detected by endoscopy in patients with Crohn’s disease After treatment with antibodies against tumor necrosis factor. Clin. Gastroenterol. Hepatol. 2020, 18, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Takabayashi, K.; Hosoe, N.; Kato, M.; Hayashi, Y.; Nanki, K.; Fukuhara, K.; Mikami, Y.; Mizuno, S.; Sujino, T.; Mutaguchi, M.; et al. Significance of endoscopic deep small bowel evaluation using balloon-assisted enteroscopy for Crohn’s disease in clinical remission. J. Gastroenterol. 2021, 56, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Bouhnik, Y.; Carbonnel, F.; Laharie, D.; Stefanescu, C.; Hébuterne, X.; Abitbol, V.; Nachury, M.; Brixi, H.; Bourreille, A.; Picon, L.; et al. Efficacy of adalimumab in patients with Crohn’s disease and symptomatic small bowel stricture: A multicentre, prospective, observational cohort (CREOLE) study. Gut 2018, 67, 53–60. [Google Scholar] [CrossRef]
- Bettenworth, D.; Lopez, R.; Hindryckx, P.; Levesque, B.G. Heterogeneity in endoscopic treatment of Crohn’s disease-associated strictures: An international inflammatory bowel disease specialist survey. J. Gastroenterol. 2016, 51, 939–948. [Google Scholar] [CrossRef]
- Bruining, D.H.; Zimmermann, E.M.; Loftus, E.V., Jr.; Sandborn, W.J.; Sauer, C.G.; Strong, S.A.; Society of Abdominal Radiology Crohn’s Disease-Focused Panel. Consensus recommendations for evaluation, interpretation, and utilisation of computed tomography and magnetic resonance enterography in patients with small bowel Crohn’s disease. Gastroenterology 2018, 154, 1172–1194. [Google Scholar] [CrossRef]
- Bettenworth, D.; Bokemeyer, A.; Kou, L.; Lopez, R.; Bena, J.F.; El Ouali, S.; Mao, R.; Kurada, S.; Bhatt, A.; Beyna, T.; et al. Systematic review with meta-analysis: Efficacy of balloon-assisted enteroscopy for dilation of small bowel Crohn’s disease strictures. Aliment Pharmacol. Ther. 2020, 52, 1104–1116. [Google Scholar] [CrossRef]
- Bettenworth, D.; Mucke, M.M.; Lopez, R.; Singh, A.; Zhu, W.; Guo, F.; Matsui, T.; James, T.W.; Herfarth, H.; Goetz, M.; et al. Efficacy of endoscopic dilation of gastroduodenal Crohn’s disease strictures: A systematic review and meta-analysis of individual patient data. Clin. Gastroenterol. Hepatol. 2019, 17, 2514–2522.e8. [Google Scholar] [CrossRef]
- Bettenworth, D.; Gustavsson, A.; Atreja, A.; Lopez, R.; Tysk, C.; van Assche, G.; Rieder, F. A pooled analysis of efficacy, safety, and long-term outcome of endoscopic balloon dilation therapy for patients with stricturing Crohn’s disease. Inflamm. Bowel Dis. 2017, 23, 133–142. [Google Scholar] [CrossRef]
- Shen, B.; Kochhar, G.; Navaneethan, U.; Farraye, F.A.; Schwartz, D.A.; Iacucci, M.; Bernstein, C.N.; Dryden, G.; Cross, R.; Bruining, D.H.; et al. Practical guidelines on endoscopic treatment for Crohn’s disease strictures: A consensus statement from the Global Interventional Inflammatory Bowel Disease Group. Lancet Gastroenterol. Hepatol. 2020, 5, 393–405. [Google Scholar] [CrossRef]
- Hirai, F.; Andoh, A.; Ueno, F.; Watanabe, K.; Ohmiya, N.; Nakase, H.; Kato, S.; Esaki, M.; Endo, Y.; Yamamoto, H.; et al. Efficacy of Endoscopic Balloon Dilation for Small Bowel Strictures in Patients With Crohn’s Disease: A Nationwide, Multi-centre, Open-label, Prospective Cohort Study. J Crohns Colitis. 2018, 12, 394–401. [Google Scholar] [CrossRef]
- Nishida, Y.; Hosomi, S.; Yamagami, H.; Yukawa, T.; Nagami, Y.; Tanaka, F.; Kamata, N.; Tanigawa, T.; Shiba, M.; Watanabe, T.; et al. Analysis of the Risk Factors of Surgery after Endoscopic Balloon Dilation for Small Intestinal Strictures in Crohn’s Disease Using Double-balloon Endoscopy. Intern. Med. 2017, 56, 2245–2252. [Google Scholar] [CrossRef]
- Sunada, K.; Shinozaki, S.; Nagayama, M.; Yano, T.; Takezawa, T.; Ino, Y.; Sakamoto, H.; Miura, Y.; Hayashi, Y.; Sato, H.; et al. Long-term Outcomes in Patients with Small Intestinal Strictures Secondary to Crohn’s Disease After Double-balloon Endoscopy-assisted Balloon Dilation. Inflamm. Bowel Dis. 22, 380–386. [CrossRef]
- Hirai, F.; Beppu, T.; Takatsu, N.; Yano, Y.; Ninomiya, K.; Ono, Y.; Hisabe, T.; Matsui, T. Long-term outcome of endoscopic balloon dilation for small bowel strictures in patients with Crohn’s disease. Dig. Endosc. 2014, 26, 545–551. [Google Scholar] [CrossRef]
- Gill, R.S.; Kaffes, A.J. Small bowel stricture characterization and outcomes of dilatation by double-balloon enteroscopy: A single-centre experience. Therap. Adv. Gastroenterol. 2014, 7, 108–114. [Google Scholar] [CrossRef]
- Hirai, F.; Beppu, T.; Sou, S.; Seki, T.; Yao, K.; Matsui, T. Endoscopic balloon dilatation using double-balloon endoscopy is a useful and safe treatment for small intestinal strictures in Crohn’s disease. Dig. Endosc. 2010, 22, 200–204. [Google Scholar] [CrossRef]
- Despott, E.J.; Gupta, A.; Burling, D.; Tripoli, E.; Konieczko, K.; Hart, A.; Fraser, C. Effective dilation of small-bowel strictures by double-balloon enteroscopy in patients with symptomatic Crohn’s disease (with video). Gastrointest. Endosc. 2009, 70, 1030–1036. [Google Scholar] [CrossRef]
- Ohmiya, N.; Arakawa, D.; Nakamura, M.; Honda, W.; Shirai, O.; Taguchi, A.; Itoh, A.; Hirooka, Y.; Niwa, Y.; Maeda, O.; et al. Small-bowel obstruction: Diagnostic comparison between double-balloon endoscopy and fluoroscopic enteroclysis, and the outcome of enteroscopic treatment. Gastrointest. Endosc. 2009, 69, 84–93. [Google Scholar] [CrossRef]
- Pohl, J.; May, A.; Nachbar, L.; Ell, C. Diagnostic and therapeutic yield of push-and-pull enteroscopy for symptomatic small bowel Crohn’s disease strictures. Eur. J. Gastroenterol. Hepatol. 2007, 19, 529–534. [Google Scholar] [CrossRef]
- Fukumoto, A.; Tanaka, S.; Yamamoto, H.; Yao, T.; Matsui, T.; Iida, M.; Goto, H.; Sakamoto, C.; Chiba, T.; Sugano, K. Diagnosis and treatment of small-bowel stricture by double balloon endoscopy. Gastrointest. Endosc. 2007, 66, S108–S112. [Google Scholar] [CrossRef]
- Karstensen, J.G. Biodegradable stents for the treatment of bowel strictures in Crohn’s disease: Technical results and challenges. Endosc. Int. Open 2016, 4, E296–E300. [Google Scholar] [CrossRef]
- Das, R.; Singh, R.; Din, S.; Lund, J.; Krishnamoorthy, R.; Hearing, S.; Norton, B.; Williams, J.; Fraser, C.; Goddard, A.; et al. Therapeutic resolution of focal, predominantly anastomotic Crohn’s disease strictures using removable stents: Outcomes from a single-center case series in the United Kingdom. Gastrointest. Endosc. 2020, 92, 344–352. [Google Scholar] [CrossRef]
- Yokoyama, K.; Yano, T.; Kumagai, H.; Mizuta, K.; Ono, S.; Imagawa, T.; Yamamoto, H.; Yamagata, T. Double-balloon enteroscopy for pediatric patients: Evaluation of safety and efficacy in 257 cases. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 34–40. [Google Scholar] [CrossRef]
- Reddy, P.M.; Kulkarni, S.; Nabi, Z.; Kasle, S.; Chavan, R.; Pal, P.; Shrimal, P.; Choudhary, H.; Sayyed, M.; Reddy, D.N. Single balloon enteroscopy in children for evaluation of small bowel diseases in children: A large, tertiary center study. J. Pediatr. Surg. 2020. [Google Scholar] [CrossRef]
- Hotokezaka, M.; Jimi, S.I.; Hidaka, H.; Maehara, N.; Eto, T.A.; Chijiiwa, K. Role of intraoperative enteroscopy for surgical decision making with Crohn’s disease. Surg. Endosc. 2007, 21, 1238–1242. [Google Scholar] [CrossRef]
- Esaki, M.; Matsumoto, T.; Hizawa, K.; Aoyagi, K.; Mibu, R.; Iida, M.; Fujishima, M. Intraoperative enteroscopy detects more lesions but is not predictive of postoperative recurrence in Crohn’s disease. Surg. Endosc. 2001, 15, 455–459. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).