
Personalized Neonatal Therapy: Application of Magistral Formulas in Therapeutic Orphan Populations

Abstract
1. Introduction
2. Neonatal Pharmacotherapy: Fundamental Concepts
2.1. Pediatric Population
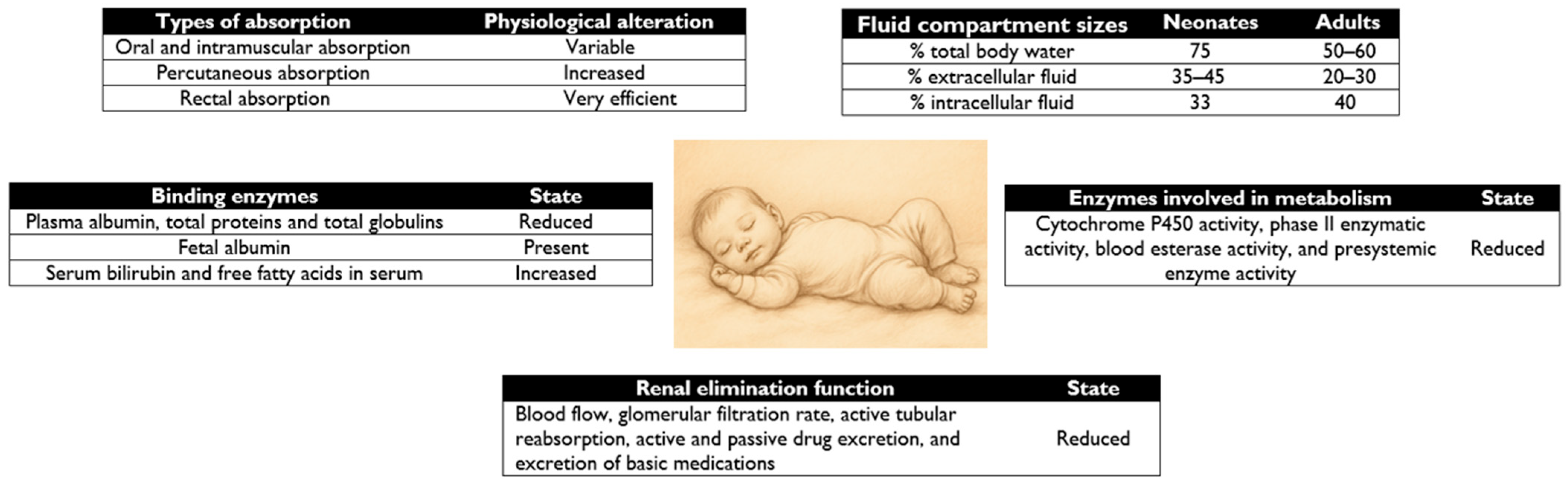
2.2. Principles of Pharmacotherapy in Neonates
2.2.1. Drug Absorption
2.2.2. Distribution of Drugs
2.2.3. Drug Metabolism
2.2.4. Drug Excretion
2.3. Newborns: A Special Group
- -
- Methodological requirements: recruitment of pediatric population for research, pharmacokinetic characteristics different from adults, lack of adequate formulations, insufficient specific indications, and lack of incentives for research.
- -
- Ethical problems: clinical trials in children face significant ethical dilemmas, and there is distrust on the part of parents.
- -
- High costs and limited market: the development of pediatric drugs involves high costs and a small and fragmented market, which reduces the return on investment for laboratories.
2.3.1. Adaptation of Dosage Forms and Routes of Administration
Parenteral Route
Oral Route
Rectal Route
Pulmonary Route
Nasal Route
Transdermal Route
2.3.2. Promoting the Availability of Pediatric Formulations
- -
- Promote and allow research related to pediatric drug design.
- -
- The majority of drugs used in the pediatric population should have specific authorization for use in age-appropriate dosage forms.
- -
- Improve the quality and availability of information on drugs used in the pediatric population.
- -
- Creation of the Pediatric Committee: A committee established by the European Medicines Agency (EMA) that provides advice on issues related to medicines for pediatric use, and performs drug assessment and approval of pediatric investigation plans.
- -
- Pediatric Investigation Plan: This must demonstrate the quality, efficacy, and safety of medicines.
- -
- European Database of Clinical Trials in Pediatrics: This allows access to information on pediatric clinical trials.
- -
- Reward System: Includes a 6-month patent extension and 15 years of validity for certain drugs.
- -
- Free Scientific Advisory Service.
3. Analysis of Magistral Formulas in Neonatal Therapeutics
3.1. Antihypertensives
- -
- Captopril 1 mg/mL oral solution
- -
- Enalapril maleate 1 mg/mL oral solution
3.2. Corticosteroids
- -
- Dexamethasone 1 mg/mL oral solution
- -
- Hydrocortisone 1 mg/mL oral suspension
3.3. Antiepileptics
- -
- Gabapentin 50 mg/mL oral solution
4. Clinical Use and Critical Analysis
4.1. Clinical Use
4.1.1. Use of Off-Label and Unlicensed Medicines in a Neonatal Intensive Care Unit
4.1.2. Use of Off-Label Medicines in Primary Care in European Countries Such as Spain
4.2. Critical Analysis
5. Conclusions
- -
- Specialized formulations are presented as a viable solution for personalized, precise dosing tailored to the specific needs of neonates.
- -
- The importance of understanding the pharmacokinetics and physiological characteristics of neonates to improve the efficacy and safety of treatments is highlighted. Although the field of pharmacokinetics has been studied in recent decades, further research is essential to improve and promote specialized formulations.
- -
- The research and development of new dosage forms that offer ease of administration and accuracy in dosing are points to investigate to improve access and efficacy of treatments.
- -
- Despite advances in pediatric research, neonates remain “therapeutic orphans”. To solve this problem, there is a European regulation to promote research in pediatrics that details, among other aspects, promoting and allowing the design of pediatric drugs.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- E11(R1) Addendum: Clinical Investigation of Medicinal Products in the Pediatric Population Guidance for Industry. Available online: https://www.fda.gov/media/101398/download (accessed on 23 May 2025).
- Broche Candó, R.C.; Trelles Porro, L.; Sosa Palacios, O.; González García, N.E.; Cubero Rego, M.d.l.Á.; Morales Mesa, E. Patrón clínico-epidemiológico de la infección en el recién nacido intervenido quirúrgicamente. Rev. Cuba. Pediatría 2013, 85, 301–310. [Google Scholar]
- Coronell, W.; Pérez, C.; Guerrero, C.; Bustamante, H. Sepsis neonatal. Rev. Enfermedades Infecc. Pediatría 2009, 22, 57–68. [Google Scholar]
- Montes Pérez, L.; Suárez Castro, D. Principales Patologías De Ingreso En Uci Neonatal. Npunto 2022, V, 3–26. [Google Scholar]
- Newborn Mortality. Available online: https://www.who.int/news-room/fact-sheets/detail/newborn-mortality (accessed on 23 May 2025).
- Nacimientos Prematuros. Available online: https://www.who.int/es/news-room/fact-sheets/detail/preterm-birth (accessed on 23 May 2025).
- Metas Mundiales de Nutrición 2025: Documento Normativo Sobre Bajo Peso al Nacer. Available online: https://www.who.int/es/publications/i/item/WHO-NMH-NHD-14.5 (accessed on 23 May 2025).
- Nacimientos por Edad de la Madre y Peso del Nacido. Available online: https://www.ine.es/jaxiT3/Tabla.htm?t=31941&L=0 (accessed on 23 May 2025).
- Gowen, C.W. Nelson. Pediatría Esencial, 9th ed.; Editorial Elsevier: Barcelona, Spain, 2023; pp. 211–262. ISBN 978-84-1382-461-1. [Google Scholar]
- Allegaert, K.; van den Anker, J. Neonatal drug therapy: The first frontier of therapeutics for children. Clin. Pharmacol. Ther. 2015, 98, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Kearns, G.L.; Abdel-Rahman, S.M.; Alander, S.W.; Blowey, D.L.; Leeder, J.S.; Kauffman, R.E. Developmental Pharmacology—Drug Disposition, Action, and Therapy in Infants and Children. N. Engl. J. Med. 2003, 349, 1157–1167. [Google Scholar] [CrossRef] [PubMed]
- Allegaert, K.; Van Den Anker, J.N. Clinical Pharmacology in Neonates: Small Size, Huge Variability. Neonatology 2014, 105, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Sandritter, T.L.; Jones, B.L.; Kearns, G.L.; Lowry, J.A. Principios de la farmacoterapia. In Nelson. Tratado de Pediatría, 21st ed.; Kliegman, R.M., Blum, N.J., Shah, S.S., Geme, J.W.S., Tasker, R.C., Wilson, K.M., Behrman, R.E., Eds.; Elsevier: Barcelona, Spain, 2020; pp. 445–456. ISBN 978-84-9113-684-2. [Google Scholar]
- Bansal, N.; Momin, S.; Bansal, R.; Gurram Venkata, S.K.R.; Ruser, L.; Yusuf, K. Pharmacokinetics of drugs: Newborn perspective. Pediatr. Med. 2024, 7, 18–19. [Google Scholar] [CrossRef]
- Ruggiero, A.; Ariano, A.; Triarico, S.; Capozza, M.A.; Ferrara, P.; Attinà, G. Neonatal pharmacology and clinical implications. Drugs Context 2019, 8, 212608. [Google Scholar] [CrossRef] [PubMed]
- Yapucu Güneş, Ü.; Ceylan, B.; Bayındır, P. Is the ventrogluteal site suitable for intramuscular injections in children under the age of three. J. Adv. Nurs. 2016, 72, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Hansen, T.G.; O’Brien, K.; Morton, N.S.; Rasmussen, S.N. Plasma paracetamol concentrations and pharmacokinetics following rectal administration in neonates and young infants. Acta Anaesthesiol. Scand. 1999, 43, 855–859. [Google Scholar] [CrossRef] [PubMed]
- Linakis, M.W.; Roberts, J.K.; Lala, A.C.; Spigarelli, M.G.; Medlicott, N.J.; Reith, D.M.; Ward, R.M.; Sherwin, C.M.T. Challenges Associated with Route of Administration in Neonatal Drug Delivery. Clin. Pharmacokinet. 2016, 55, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, M.; Sanwatsarkar, S.; Katakwar, M. Pharmacology related to paediatric anaesthesia. Indian J. Anaesth. 2019, 63, 698. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, M.B.; Armijo, J.A. Influencia de los factores genéticos y ambientales, la edad y el embarazo sobre la respuesta a los fármacos. In Farmacología Humana, 6th ed.; Flórez, J., Ed.; Elsevier: Barcelona, Spain, 2014; pp. 121–155. ISBN 978-84-458-2316-3. [Google Scholar]
- Smits, A.; Kulo, A.; N De Hoon, J.; Allegaert, K. Pharmacokinetics of Drugs in Neonates: Pattern Recognition Beyond Compound Specific Observations. Curr. Pharm. Des. 2012, 18, 3119–3146. [Google Scholar] [CrossRef] [PubMed]
- Notarianni, L.J. Plasma Protein Binding of Drugs in Pregnancy and in Neonates. Clin. Pharmacokinet. 1990, 18, 20–36. [Google Scholar] [CrossRef] [PubMed]
- Tayman, C.; Rayyan, M.; Allegaert, K. Neonatal Pharmacology: Extensive Interindividual Variability Despite Limited Size. J. Pediatr. Pharmacol. Ther. 2011, 16, 170–184. [Google Scholar] [CrossRef] [PubMed]
- Piekos, S.; Pope, C.; Ferrara, A.; Zhong, X. Impact of Drug Treatment at Neonatal Ages on Variability of Drug Metabolism and Drug-Drug Interactions in Adult Life. Curr. Pharmacol. Rep. 2017, 3, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Allegaert, K.; Anderson, B.J.; Van Den Anker, J.N.; Vanhaesebrouck, S.; De Zegher, F. Renal Drug Clearance in Preterm Neonates: Relation to Prenatal Growth. Ther. Drug Monit. 2007, 29, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Filler, G.; Bhayana, V.; Schott, C.; Díaz-González De Ferris, M.E. How should we assess renal function in neonates and infants? Acta Paediatr. 2021, 110, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Evaluación de la Función Renal en el Recién Nacido. Asociación Española de Pediatría. Available online: https://www.aeped.es/sites/default/files/documentos/03_renal.pdf (accessed on 23 May 2025).
- Blake, M.J.; Abdel-Rahman, S.M.; Pearce, R.E.; Leeder, J.S.; Kearns, G.L. Effect of Diet on the Development of Drug Metabolism by Cytochrome P-450 Enzymes in Healthy Infants. Pediatr. Res. 2006, 60, 717–723. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, F.; Clapham, D.; Krysiak, K.; Batchelor, H.; Field, P.; Caivano, G.; Pertile, M.; Nunn, A.; Tuleu, C. Making Medicines Baby Size: The Challenges in Bridging the Formulation Gap in Neonatal Medicine. Int. J. Mol. Sci. 2019, 20, 2688. [Google Scholar] [CrossRef] [PubMed]
- Mfoafo, K.A.; Omidian, M.; Bertol, C.D.; Omidi, Y.; Omidian, H. Neonatal and pediatric oral drug delivery: Hopes and hurdles. Int. J. Pharm. 2021, 597, 120296. [Google Scholar] [CrossRef] [PubMed]
- Valverde Molina, E. Farmacia Pediátrica Hospitalaria, 1st ed.; Elsevier Doyma: Madrid, Spain, 2011; ISBN 978-84-8086-926-2. [Google Scholar]
- Sherwin, C.M.T.; Medlicott, N.J.; Reith, D.M.; Broadbent, R.S. Intravenous drug delivery in neonates: Lessons learnt. Arch. Dis. Child. 2014, 99, 590–594. [Google Scholar] [CrossRef] [PubMed]
- Costa, H.T.M.D.L.; Costa, T.X.; Martins, R.R.; Oliveira, A.G. Use of off-label and unlicensed medicines in neonatal intensive care. PLoS ONE 2018, 13, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Perez, M.; Décaudin, B.; Maiguy-Foinard, A.; Barthélémy, C.; Lebuffe, G.; Storme, L.; Odou, P. Dynamic Image Analysis To Evaluate Subvisible Particles During Continuous Drug Infusion in a Neonatal Intensive Care Unit. Sci. Rep. 2017, 7, 9404. [Google Scholar] [CrossRef] [PubMed]
- Kalikstad, B.; Skjerdal, A.; Hansen, T.W.R. Compatibility of drug infusions in the NICU. Arch. Dis. Child. 2010, 95, 745–748. [Google Scholar] [CrossRef] [PubMed]
- Guideline on Pharmaceutical Development of Medicines for Paediatric Use. Available online: https://www.ema.europa.eu/en/pharmaceutical-development-medicines-paediatric-use-scientific-guideline (accessed on 23 May 2025).
- Gurung, K.; Arenas-Lopez, S.; Wei, L.; Tuleu, C. Accuray of enteral syringes for liquid medicines prescribed in children. Arch. Dis. Child. 2014, 99, e3. [Google Scholar] [CrossRef]
- Maier, T.; Scheuerle, R.L.; Markl, D.; Bruggraber, S.; Zeitler, A.; Fruk, L.; Slater, N.K.H. Zinc delivery from non-woven fibres within a therapeutic nipple shield. Int. J. Pharm. 2018, 537, 290–299. [Google Scholar] [CrossRef] [PubMed]
- Hansen, K.; Yee, L.; Lee, J.; Horeczko, T.; Saidinejad, M.; Padlipsky, P.S.; Gausche-Hill, M.; Tanen, D.A. Parent and Nurse Satisfaction Using Pacidose® Oral Medication Delivery Device in the Pediatric Emergency Department: A Pilot Study. J. Pediatr. Nurs. 2018, 42, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Gerrard, S.E.; Baniecki, M.L.; Sokal, D.C.; Morris, M.K.; Urdaneta-Hartmann, S.; Krebs, F.C.; Wigdahl, B.; Abrams, B.F.; Hanson, C.V.; Slater, N.K.; et al. A nipple shield delivery system for oral drug delivery to breastfeeding infants: Microbicide delivery to inactivate HIV. Int. J. Pharm. 2012, 434, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Dr. Brown’sTM PacidoseTM Liquid Medicine Dispenser with Oral Syringe. Available online: https://www.drbrownsbaby.com/product/pacidose-liquid-medicine-dispenser/?highlight=pacidose (accessed on 23 May 2025).
- Greenhalgh, L.L.; Passos, M.M.B.D.; Agrizzi, A.L.; Monteiro, M.S.d.S.B. Compounded medications for cardiovascular use in neonatology: An integrative review. Rev. Paul. Pediatr. 2022, 41, e2021167. [Google Scholar] [CrossRef] [PubMed]
- Demir, N.; Peker, E.; Ece, İ.; Balahoroğlu, R.; Tuncer, O. Efficacy and safety of rectal ibuprofen for patent ductus arteriosus closure in very low birth weight preterm infants. J. Matern.-Fetal Neonatal Med. 2017, 30, 2119–2125. [Google Scholar] [CrossRef] [PubMed]
- MacLoughlin, R.; Telfer, C.; Clark, A.; Fink, J. Aerosol: A Novel Vehicle for Pharmacotherapy in Neonates. Curr. Pharm. Des. 2018, 23, 5928–5934. [Google Scholar] [CrossRef] [PubMed]
- Pohlmann, G.; Iwatschenko, P.; Koch, W.; Windt, H.; Rast, M.; De Abreu, M.G.; Taut, F.J.H.; De Muynck, C. A Novel Continuous Powder Aerosolizer (CPA) for Inhalative Administration of Highly Concentrated Recombinant Surfactant Protein-C (rSP-C) Surfactant to Preterm Neonates. J. Aerosol Med. Pulm. Drug Deliv. 2013, 26, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Valeur, K.S.; Holst, H.; Allegaert, K. Excipients in Neonatal Medicinal Products: Never Prescribed, Commonly Administered. Pharm. Med. 2018, 32, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Charro, M.B.; Guy, R.H. Effective use of transdermal drug delivery in children. Adv. Drug Deliv. Rev. 2014, 73, 63–82. [Google Scholar] [CrossRef] [PubMed]
- Simplified Calculation of Body-Surface Area. N. Engl. J. Med. 1987, 317, 1090–1098. [CrossRef]
- El Edelbi, R.A.; Lindemalm, S.; Nydert, P.; Eksborg, S. Estimation of body surface area in neonates, infants, and children using body weight alone. Int. J. Pediatr. Adolesc. Med. 2021, 8, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Reglamento (CE) n° 1901/2006 del Parlamento Europeo y del Consejo, de 12 de Diciembre de 2006, Sobre Medicamentos para uso Pediátrico y por el que se Modifican el Reglamento (CEE) n° 1768/92, la Directiva 2001/20/CE, la Directiva 2001/83/CE y el Reglamento (CE) n° 726/2004. Available online: https://www.boe.es/buscar/doc.php?id=DOUE-L-2006-82668 (accessed on 23 May 2025).
- The Situation of Pediatric Medicinese in the UE at Ten Years of the Pediatric Regulation, COM/2017/0626 (2017). Available online: https://eur-lex.europa.eu/legal-content/ES/TXT/?uri=CELEX%3A52017DC0626 (accessed on 23 May 2025).
- Real Decreto 175/2001, de 23 de Febrero, por el que se Aprueban las Normas de Correcta Elaboración y Control de Calidad de Fórmulas Magistrales y Preparados Oficinales, Pub. L. No. Real Decreto 175/2001, BOE-A-2001-5185 9746 (2001). Available online: https://www.boe.es/eli/es/rd/2001/02/23/175 (accessed on 23 May 2025).
- Formulario Nacional. Agencia Española de Medicamentos y Productos Sanitarios. Available online: https://www.aemps.gob.es/formulario-nacional/ (accessed on 23 May 2025).
- BOE-A-2006-13554 Ley 29/2006, de 26 de Julio, de Garantías y Uso Racional de los Medicamentos y Productos Sanitarios. Available online: https://www.boe.es/buscar/act.php?id=BOE-A-2006-13554 (accessed on 23 May 2025).
- Flynn, J.T. The hypertensive neonate. Semin. Fetal Neonatal Med. 2020, 25, 101138. [Google Scholar] [CrossRef] [PubMed]
- Asociación Española de Pediatría. Hipertensión Arterial. Protocolos Diagnóstico-Terapéuticos de la AEP. Available online: https://www.aeped.es/sites/default/files/documentos/12_hta.pdf (accessed on 23 May 2025).
- O’Dea, R.F.; Mirkin, B.L.; Alward, C.T.; Sinaiko, A.R. Treatment of neonatal hypertension with captopril. J. Pediatr. 1988, 113, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Tack, E.D.; Perlman, J.M. Renal failure in sick hypertensive premature infants receiving captopril therapy. J. Pediatr. 1988, 112, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Formulario Nacional. FN/2018/FMT/024 Captopril 1 mg/mL Solución Oral. Available online: https://www.aemps.gob.es/formulario-nacional/monografias/formulas-magistrales-tipificadas-pediatricas/fn_2018_fmt_024.pdf (accessed on 23 May 2025).
- CIMA: Centro de Información de Medicamentos. Available online: https://cima.aemps.es/cima/publico/home.html# (accessed on 23 May 2025).
- Lorenzo, P.; Moreno, A.; Leza, C.; Lizasoain, I.; Moro, M.A.; Portolés, A. Velázquez. Farmacología Básica y Clínica, 19th ed.; Editorial Médica Panamericana: Mexico City, Mexico, 2018; pp. 239–676. ISBN 978-607-8546-07-7. [Google Scholar]
- European Medicines Agency. Available online: https://www.ema.europa.eu/en/documents/product-information/aqumeldi-epar-product-information_en.pdf (accessed on 23 May 2025).
- Formulario Nacional. FN/2021/FMT/036 Enalapril Maleato 1 mg/mL Solución Oral. Available online: https://www.aemps.gob.es/formulario-nacional/monografias/formulas-magistrales-tipificadas-pediatricas/fn_2021_fmt_036.pdf (accessed on 23 May 2025).
- Lardón, M.; Uberos, J.; Narbona, E. Does the corticosteroid’s treatment during the pre and postnatal period affect the neurodevelopmental outcome of premature newborns? Biomedica 2016, 37, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Doyle, L.W. Postnatal Corticosteroids to Prevent or Treat Bronchopulmonary Dysplasia. Neonatology 2021, 118, 244–251. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Available online: https://www.ema.europa.eu/en/documents/product-information/neofordex-epar-product-information_en.pdf (accessed on 23 May 2025).
- Formulario Nacional. FN/2020/FMT/030 Dexametasona 1 mg/mL Solución Oral. Available online: https://www.aemps.gob.es/formulario-nacional/monografias/formulas-magistrales-tipificadas-pediatricas/fn_2020_fmt_030.pdf (accessed on 23 May 2025).
- European Medicines Agency. Available online: https://www.ema.europa.eu/en/documents/product-information/efmody-epar-product-information_en.pdf (accessed on 23 May 2025).
- Formulario Nacional. FN/2024/FMT/040 Hidrocortisona 1 mg/mL Suspensión Oral. Available online: https://www.aemps.gob.es/formulario-nacional/monografias/formulas-magistrales-tipificadas-pediatricas/fn_2024_fmt_040.pdf (accessed on 23 May 2025).
- DeLisle, A.; Jones, H.E.; Jansson, L.M. Gabapentin Use During Pregnancy and Lactation With and Without Concurrent Opioid Exposure: Considerations and Future Directions. J. Addict. Med. 2023, 17, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Formulario Nacional. FN/2024/FMT/041 Gabapentina 50 mg/mL Solución Oral. Available online: https://www.aemps.gob.es/formulario-nacional/monografias/formulas-magistrales-tipificadas-pediatricas/fn_2024_fmt_041.pdf (accessed on 23 May 2025).
- Arocas Casañ, V.; Cabezuelo Escribano, B.; Garrido-Corro, B.; De la Cruz Murie, P.; Blázquez Álvarez, M.J.; De la Rubia Nieto, M.A. Off-label and unlicensed drug use in a Spanish Neonatal Intensive Care Unit. Farm. Hosp. 2017, 41, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Turner, S.; Longworth, A.; Nunn, A.J.; Choonara, I. Unlicensed and off label drug use in paediatric wards: Prospective study. BMJ 1998, 316, 343–345. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, M.D.T. Global Pediatric Drug Development. Curr. Ther. Res. Clin. Exp. 2019, 90, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Arenas-López, S.; Stanley, I.M.; Tunstell, P.; Aguado-Lorenzo, V.; Philip, J.; Perkins, J.; Durward, A.; Calleja-Hernández, M.A.; Tibby, S.M. Safe implementation of standard concentration infusions in paediatric intensive care. J. Pharm. Pharmacol. 2017, 69, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Christie-Taylor, S.A.; Tait, P.A. Implementation of standard concentration medication infusions for preterm infants. Infant 2012, 8, 155–159. [Google Scholar]
- Sentinel Event Alert 39: Preventing Pediatric Medication Errors|The Joint Commission. Available online: https://www.jointcommission.org/resources/sentinel-event/sentinel-event-alert-newsletters/sentinel-event-alert-issue-39-preventing-pediatric-medication-errors/ (accessed on 23 May 2025).
- Lizano-Díez, I.; Kargodorian, J.; Piñero-López, M.Á.; Lastra, C.F.; Mariño, E.L.; Modamio, P. Off-label drug use in neonates and infants in Spain: A five-year observational study. Pharmacoepidemiol. Drug Saf. 2022, 31, 270–282. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Category | Postnatal Age |
|---|---|
| Premature newborn | Born before completing the 37th week of gestation, from birth to the expected date of delivery 27 days |
| Term neonates | 0–28 days |
| Infants | 28 days–23 months |
| Children | 2–11 years |
| Teenagers | 11–18 years |
| Birth Weight | Birth Rate in Spain (2022) | Probability of Dying in the Neonatal Period | |
|---|---|---|---|
| Term newborn | ≥2.500 kg | 97.86% | 1× |
| Low birth weight | 2.499–1.500 kg | 6.61% | 40× |
| Very low birth weight | <1.500 kg | 0.82% | 200 |
| Physiological Factors | State |
|---|---|
| Gastric pH | >5 |
| Gastric emptying time | Irregular |
| Gut motility | Reduced |
| Intestinal surface | Reduced |
| Microbial colonization | Reduced |
| Biliary function | Immature |
| Catheter Type | Application | Characteristics | Issues |
|---|---|---|---|
| Peripheral venous catheter | Most intravenous medications, isotonic intravenous fluids, and blood transfusion | Low flow rates; physicochemical irritation with some medications produces phlebitis | Difficult to insert in newborns due to small, difficult to visualize vessels |
| Umbilical venous catheter | For diagnostic and therapeutic purposes: drug infusion, total parental nutrition, hypertonic intravenous fluids, central venous pressure, and venous blood gas monitoring and blood transfusions | It is usually placed within 12 h after birth, if indicated, for parenteral nutrition and/or inotropic support | Suitable only for newborns, as the umbilical vein remains for up to two weeks after birth |
| Peripherally inserted central catheter | Administration of intravenous medications and fluids, total parenteral nutrition, and blood sampling | Suitable for irritating and hyperosmolar drugs; together with the umbilical venous catheter, it helps reduce the risk of drug incompatibilities | Not suitable for the administration of large volumes in emergency situations |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shao, W.; Gomez, A.; Alejano, A.; Gil, T.; Benéitez, M.C. Personalized Neonatal Therapy: Application of Magistral Formulas in Therapeutic Orphan Populations. Pharmaceutics 2025, 17, 963. https://doi.org/10.3390/pharmaceutics17080963
Shao W, Gomez A, Alejano A, Gil T, Benéitez MC. Personalized Neonatal Therapy: Application of Magistral Formulas in Therapeutic Orphan Populations. Pharmaceutics. 2025; 17(8):963. https://doi.org/10.3390/pharmaceutics17080963
Chicago/Turabian StyleShao, Wenwen, Angela Gomez, Alejandra Alejano, Teresa Gil, and María Cristina Benéitez. 2025. "Personalized Neonatal Therapy: Application of Magistral Formulas in Therapeutic Orphan Populations" Pharmaceutics 17, no. 8: 963. https://doi.org/10.3390/pharmaceutics17080963
APA StyleShao, W., Gomez, A., Alejano, A., Gil, T., & Benéitez, M. C. (2025). Personalized Neonatal Therapy: Application of Magistral Formulas in Therapeutic Orphan Populations. Pharmaceutics, 17(8), 963. https://doi.org/10.3390/pharmaceutics17080963