

Y-Site Compatibility Studies of Parenteral Nutrition and Other Intravenous Medications in Neonatal and Pediatric Patients: A Review of the Literature Evidence


Abstract
1. Introduction
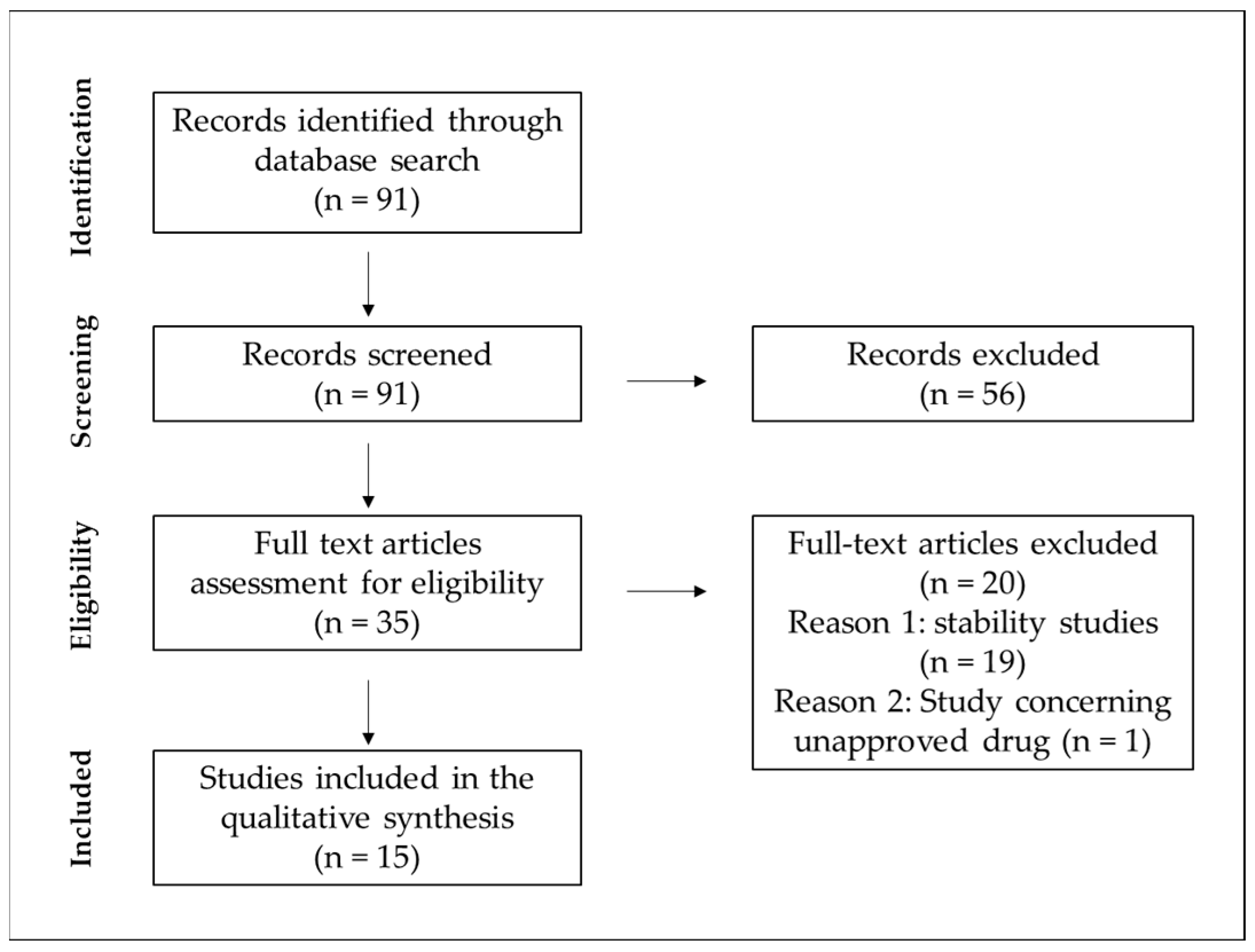
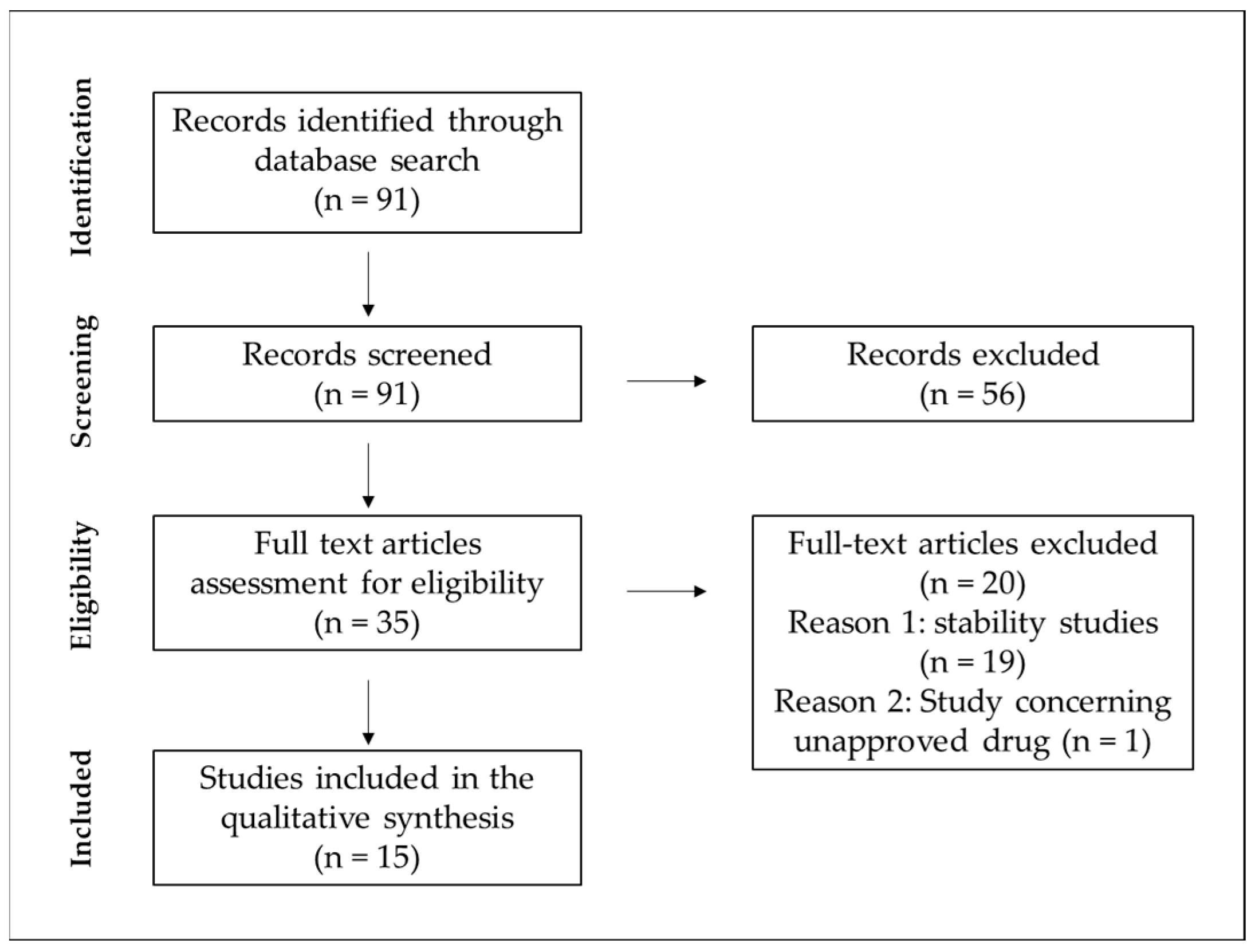
2. Methods
2.1. Research Methodology
2.2. Research Quality Assessment
3. Results and Discussion
3.1. Compatibility Data
3.2. Research Quality Evaluation
3.3. Compatibility Evaluation Methods
3.4. Limitations of Data Extrapolation
4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Groh-Wargo, S.; Barr, S.M. Parenteral Nutrition. Clin. Perinatol. 2022, 49, 355–379. [Google Scholar] [CrossRef] [PubMed]
- Institute for Safe Medication Practices. [High Alert Drug] Institute for Safe Medication Practices List of High-Alert Medications in Acute Care Settings; Institute for Safe Medication Practices: Buttler Pike, PA, USA, 2018. [Google Scholar]
- Riskin, A.; Picaud, J.-C.; Shamir, R.; ESPGHAN/ESPEN/ESPR/CSPEN Working Group on Pediatric Parenteral Nutrition. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Standard versus individualized parenteral nutrition. Clin. Nutr. 2018, 37, 2409–2417. [Google Scholar] [CrossRef]
- Koletzko, B.; Bhutta, Z.A.; Cai, W.; Cruchet, S.; El Guindi, M.; Fuchs, G.J.; Goddard, E.A.; van Goudoever, J.B.; Quak, S.H.; Kulkarny, B.; et al. Compositional requirements of follow-up formula for use in infancy: Recommendations of an international expert group coordinated by the Early Nutrition Academy. Ann. Nutr. Metab. 2013, 62, 44–54. [Google Scholar] [CrossRef]
- Blackmer, A.B.; Partipilo, M.L. Three-in-one parenteral nutrition in neonates and pediatric patients: Risks and benefits. Nutr. Clin. Pract. 2015, 30, 337–343. [Google Scholar] [CrossRef]
- Häni, C.; Vonbach, P.; Fonzo-Christe, C.; Russmann, S.; Cannizzaro, V.; Niedrig, D. Evaluation of Incompatible Co-administration of Continuous Intravenous Infusions in a Pediatric/Neonatal Intensive Care Unit. J. Pediatr. Pharmacol. Ther. 2019, 24, 479–488. [Google Scholar] [CrossRef]
- Benlabed, M.; Perez, M.; Gaudy, R.; Genay, S.; Lannoy, D.; Barthélémy, C.; Odou, P.; Lebuffe, G.; Decaudin, B. Clinical implications of intravenous drug incompatibilities in critically ill patients. Anaesth. Crit. Care Pain Med. 2019, 38, 173–180. [Google Scholar] [CrossRef]
- Leopoldino, R.W.; Costa, H.T.; Costa, T.X.; Martins, R.R.; Oliveira, A.G. Potential drug incompatibilities in the neonatal intensive care unit: A network analysis approach. BMC Pharmacol. Toxicol. 2018, 19, 83. [Google Scholar] [CrossRef]
- Hörmann, K.; Zimmer, A. Drug delivery and drug targeting with parenteral lipid nanoemulsions—A review. J. Control Release 2016, 223, 85–98. [Google Scholar] [CrossRef]
- Ross, E.L.; Petty, K.; Salinas, A.; Her, C.; Carpenter, J.F. Physical compatibility of medications with concentrated neonatal and pediatric parenteral nutrition: A simulated Y-site drug compatibility study. JPEN J. Parenter. Enteral. Nutr. 2023, 47, 372–381. [Google Scholar] [CrossRef]
- Campbell, A.L.; Petrovski, M.; Senarathna, S.G.; Mukadam, N.; Strunk, T.; Batty, K.T. Compatibility of pentoxifylline and parenteral medications. Arch. Dis. Child 2020, 105, 395–397. [Google Scholar] [CrossRef]
- Greenhill, K.; Hornsby, E.; Gorman, G. Investigations of Physical Compatibilities of Commonly Used Intravenous Medications with and without Parenteral Nutrition in Pediatric Cardiovascular Intensive Care Unit Patients. Pharmaceuticals 2019, 12, 67. [Google Scholar] [CrossRef]
- Fox, L.M.; Wilder, A.G.; Foushee, J.A. Physical compatibility of various drugs with neonatal total parenteral nutrient solution during simulated Y-site administration. Am. J. Health Syst. Pharm. 2013, 70, 520–524. [Google Scholar] [CrossRef]
- Sykes, R.; McPherson, C.; Foulks, K.; Wade, J.; Gal, P. Aminophylline compatibility with neonatal total parenteral nutrition. J. Pediatr. Pharmacol. Ther. 2008, 13, 76–79. [Google Scholar] [CrossRef]
- Dice, J.E. Physical Compatibility of Alprostadil with Commonly Used IV Solutions and Medications in the Neonatal Intensive Care Unit. J. Pediatr. Pharmacol. Ther. 2006, 11, 233–236. [Google Scholar] [CrossRef]
- Veltri, M.A.; Conner, K.G. Physical compatibility of milrinone lactate injection with intravenous drugs commonly used in the pediatric intensive care unit. Am. J. Health Syst. Pharm. 2002, 59, 452–454. [Google Scholar] [CrossRef]
- Veltri, M.; Lee, C.K. Compatibility of neonatal parenteral nutrient solutions with selected intravenous drugs. Am. J. Health Syst. Pharm. 1996, 53, 2611–2613. [Google Scholar] [CrossRef]
- Tomczak, S.; Chmielewski, M.; Szkudlarek, J.; Jelińska, A. Antiemetic Drugs Compatibility Evaluation with Paediatric Parenteral Nutrition Admixtures. Pharmaceutics 2023, 15, 2143. [Google Scholar] [CrossRef]
- Nilsson, N.; Storesund, I.; Tho, I.; Nezvalova-Henriksen, K. Co-administration of drugs with parenteral nutrition in the neonatal intensive care unit—Physical compatibility between three components. Eur. J. Pediatr. 2022, 181, 2685–2693. [Google Scholar] [CrossRef]
- Nezvalova-Henriksen, K.; Nilsson, N.; Østerberg, C.T.; Staven Berge, V.; Tho, I. Y-Site Physical Compatibility of Numeta G13E with Drugs Frequently Used at Neonatal Intensive Care. Pharmaceutics 2020, 12, 677. [Google Scholar] [CrossRef] [PubMed]
- Staven, V.; Wang, S.; Grønlie, I.; Tho, I. Physical stability of an all-in-one parenteral nutrition admixture for preterm infants upon mixing with micronutrients and drugs. Eur. J. Hosp. Pharm. Sci. Pract. 2020, 27, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Ross, E.L.; Salinas, A.; Petty, K.; Her, C.; Carpenter, J.F. Compatibility of medications with intravenous lipid emulsions: Effects of simulated Y-site mixing. Am. J. Health Syst. Pharm. 2020, 77, 1980–1985. [Google Scholar] [CrossRef]
- Garcia, J.; Garg, A.; Song, Y.; Fotios, A.; Andersen, C.; Garg, S. Compatibility of intravenous ibuprofen with lipids and parenteral nutrition, for use as a continuous infusion. PLoS ONE 2018, 13, e0190577. [Google Scholar] [CrossRef]
- Staven, V.; Iqbal, H.; Wang, S.; Grønlie, I.; Tho, I. Physical compatibility of total parenteral nutrition and drugs in Y-site administration to children from neonates to adolescents. J. Pharm. Pharmacol. 2017, 69, 448–462. [Google Scholar] [CrossRef]
- Thompson, D.F.; Allen, L.V.; Desai, S.R.; Rao, P.S. Compatibility of furosemide with aminoglycoside admixtures. Am. J. Hosp. Pharm. 1985, 42, 116–119. [Google Scholar] [CrossRef]
- Campos-Baeta, Y.; Saavedra-Mitjans, M.; Garin, N.; Cardenete, J.; Cardona, D.; Riera, P. Physicochemical Compatibility of Dexmedetomidine with Parenteral Nutrition. Nutr. Clin. Pract. 2020, 35, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Mediavilla, M.M.; Molina, A.; Navarro, L.; Grau, L.; Pujol, M.D.; Cardenete, J.; Cardona, D.; Riera, P. Physicochemical Compatibility of Amiodarone with Parenteral Nutrition. J. Parenter. Enter. Nutr. 2019, 43, 298–304. [Google Scholar] [CrossRef]
- Stawny, M.; Gostyńska, A.; Olijarczyk, R.; Jelińska, A.; Ogrodowczyk, M. Stability of high-dose thiamine in parenteral nutrition for treatment of patients with Wernicke’s encephalopathy. Clin. Nutr. 2020, 39, 2929–2932. [Google Scholar] [CrossRef] [PubMed]
- Stawny, M.; Gostyńska, A.; Olijarczyk, R.; Dettlaff, K.; Jelińska, A.; Ogrodowczyk, M. Stability studies of parenteral nutrition with a high dose of vitamin C. J. Oncol. Pharm. Pract. 2020, 26, 1894–1902. [Google Scholar] [CrossRef]
- Gostyńska, A.; Stawny, M.; Dettlaff, K.; Jelińska, A. The Interactions between Ciprofloxacin and Parenteral Nutrition Admixtures. Pharmaceutics 2019, 12, 27. [Google Scholar] [CrossRef]
- Prolla, I.; Tomlinson, C.; Pencharz, P.B.; Porto, B.; Elango, R.; Courtney-Martin, G. Amino acid requirements of total parenteral nutrition (TPN) fed neonates: A narrative review of current knowledge and the basis for a new amino acid solution in neonatal nutrition. Pediatr. Med. 2022, 5, 29. [Google Scholar] [CrossRef]
- Riedijk, M.A.; van Beek, R.H.T.; Voortman, G.; de Bie, H.M.A.; Dassel, A.C.M.; van Goudoever, J.B. Cysteine: A conditionally essential amino acid in low-birth-weight preterm infants? Am. J. Clin. Nutr. 2007, 86, 1120–1125. [Google Scholar] [CrossRef]
- Pencharz, P.B.; House, J.D.; Wykes, L.J.; Ball, R.O. What are the essential amino acids for the preterm and term infant? In Recent Developments in Infant Nutrition: Scheveningen 29 November–2 December 1995; Bindels, J.G., Goedhart, A.C., Visser, H.K.A., Eds.; Springer: Dordrecht, The Netherlands, 1996; pp. 278–296. [Google Scholar] [CrossRef]
- Unger, N.; Holzgrabe, U. Stability and assessment of amino acids in parenteral nutrition solutions. J. Pharm. Biomed. Anal. 2018, 147, 125–139. [Google Scholar] [CrossRef]
- Wang, H.-J.; Hsieh, Y.-T.; Liu, L.-Y.; Huang, C.-F.; Lin, S.-C.; Tsao, P.-N.; Chou, H.-C.; Yen, T.-A.; Chen, C.-Y. Use of sodium glycerophosphate in neonatal parenteral nutrition solutions to increase calcium and phosphate compatibility for preterm infants. Pediatr. Neonatol. 2020, 61, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Bouchoud, L.; Fonzo-Christe, C.; Sadeghipour, F.; Bonnabry, P. Maximizing calcium and phosphate content in neonatal parenteral nutrition solutions using organic calcium and phosphate salts. JPEN J. Parenter. Enteral. Nutr. 2010, 34, 542–545. [Google Scholar] [CrossRef] [PubMed]
- Reber, E.; Neyer, P.; Schönenberger, K.A.; Saxer, C.; Bernasconi, L.; Stanga, Z.; Huber, A.; Hammerer-Lercher, A.; Mühlebach, S. Physicochemical Stability and Compatibility Testing of Voriconazole in All-in-One Parenteral Nutrition Admixtures. Pharmaceutics 2021, 13, 1447. [Google Scholar] [CrossRef] [PubMed]
- Staven, V.; Wang, S.; Grønlie, I.; Tho, I. Development and evaluation of a test program for Y-site compatibility testing of total parenteral nutrition and intravenous drugs. Nutr. J. 2016, 15, 29. [Google Scholar] [CrossRef]
- Trissel, L.A. Everything in a compatibility study is important. Am. J. Health Syst. Pharm. 1996, 53, 2990. [Google Scholar] [CrossRef]
- Mühlebach, S. Basics in clinical nutrition: Drugs and nutritional admixtures. E-SPEN Eur. E-J. Clin. Nutr. Metab. 2009, 4, e134–e136. [Google Scholar] [CrossRef]
- Driscoll, D.F. Clinical issues regarding the use of total nutrient admixtures. DICP Ann. Pharmacother. 1990, 24, 296–303. [Google Scholar] [CrossRef]
- Driscoll, D.F. Physicochemical assessment of total nutrient admixture stability and safety: Quantifying the risk. Nutr. Burbank 1997, 13, 166–167. [Google Scholar] [CrossRef]
- Stawny, M.; Gostyńska, A.; Dettlaff, K.; Jelińska, A.; Główka, E.; Ogrodowczyk, M. Effect of Lipid Emulsion on Stability of Ampicillin in Total Parenteral Nutrition. Nutrients 2019, 11, 559. [Google Scholar] [CrossRef] [PubMed]
- Stawny, M.; Gostyńska, A.; Nadolna, M.; Jelińska, A. Safe Practice of Y-Site Drug Administration: The Case of Colistin and Parenteral Nutrition. Pharmaceutics 2020, 12, 292. [Google Scholar] [CrossRef] [PubMed]
- Gostyńska, A.; Piwowarczyk, L.; Nadolna, M.; Jelińska, A.; Dettlaff, K.; Ogrodowczyk, M.; Popielarz-Brzezinska, M.; Stawny, M. Toward Safe Pharmacotherapy: The Interplay between Meropenem and Parenteral Nutrition Admixtures. Antibiotics 2021, 10, 217. [Google Scholar] [CrossRef]
- Pehlivanli, A.; Eren-Sadioglu, R.; Aktar, M.; Eyupoglu, S.; Sengul, S.; Keven, K.; Erturk, S.; Basgut, B.; Ozcelikay, A.T. Potential drug-drug interactions of immunosuppressants in kidney transplant recipients: Comparison of drug interaction resources. Int. J. Clin. Pharm. 2022, 44, 651–662. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Parenteral Nutrition | Drug Solution | Final Concentration of Drug | Diluent | Mixing Ratio of Drug + PN | Compatibility/Incompatibility (C/I) * | Ref./Grade (A,B,C,D) ** |
|---|---|---|---|---|---|---|
| Two different PN solutions containing the following: Amino acids (TrophAmine, Plenamine) 38.2–58.3 g/L; Cysteine 0–1.5 g/L; Glucose 165–250 g/L; Sodium chloride 26.3–43.7 mmol/L; Sodium acetate 0–19.7 mmol/L; Sodium phosphate 13.2–17.5 mmol/L; Potassium chloride 19.7–14.6 mmol/L; Potassium acetate 13.15–14.6 mmol/L; Calcium gluconate 11.7–16.4 mmol/L; Magnesium sulfate 3.3–4.4 mmol/L; Multivitamin 16.7–21.9 mL/L; Zinc 5263–1167 µg/L; Copper 263–1666 µg/L; Selenium 22–200 µg/L; Heparin 0–1000 units/L; Levocarnitine 263–2333 mg/L | Alprostadil, Pfizer | 0.02 mg/L | Glucose 50 mg/mL | 1 + 1 | C/I | [10] C grade |
| Ampicillin/sulbactam, AuroMedics | 20 mg/mL | NaCl 9 mg/mL | 1 + 1 | C | ||
| Ampicillin, Athenex | 30 mg/mL | NaCl 9 mg/mL | 1 + 1 | C | ||
| Bumetanide, Hospira; Westward | 0.25 mg/mL | NA | 1 + 1 | C | ||
| Cisatracurium, AbbVie | 2 mg/mL | NA | 1 + 1 | C/I | ||
| Dexmedetomidine, Baxter | 0.04 mg/L | NA | 1 + 1 | C | ||
| Furosemide, Novaplus; Hospira | 10 mg/mL | NA | 1 + 1 | C/I | ||
| Heparin, Fresenius Kabi | 500 units/mL | NaCl 9 mg/mL | 1 + 1 | C/I | ||
| Hydromorphone, Teva | 0.5 mg/mL | Glucose 50 mg/mL | 1 + 1 | C | ||
| Ketamine, Mylan | 10 mg/mL | NA | 1 + 1 | C/I | ||
| Lacosamide, UCB | 10 mg/mL | NA | 1 + 1 | C | ||
| Nicardipine, Westward | 0.5 mg/mL | Glucose 50 mg/mL | 1 + 1 | C | ||
| Rocuronium, Sandoz | 10 mg/mL | NA | 1 + 1 | C | ||
| Sildenafil, AuroMedics | 0.8 mg/mL | NA | 1 + 1 | C/I | ||
| Vasopressin, Par Pharmaceutical | 1 unit/mL | Glucose 50 mg/mL | 1 + 1 | C | ||
| Six different PN solutions containing the following: Amino acids (Primene) 23–40 g/L; Glucose 75–120 g/L; Sodium 10–60 mmol/L; Potassium 0–22 mmol/L; Calcium 5–17 mmol/L; Magnesium 1.5 mmol/L; Phosphate 4–13 mmol/L; Acetate 0–34 mmol/L; Chloride 7.6–30.7 mmol/L; Zinc 0–3270 µg/L; Selenium 0–20 µg/L; Iodide 0–8.2 µg/L; Heparin 500 units/L | Pentoxifylline, Trental, Sanofi | 5.0 mg/mL | NaCl 9 mg/mL | 1 + 1 | C | [11] D grade |
| PN solution containing the following: Amino acids (Travasol 10%) 30 g/L; Glucose 250 g/L; Sodium 150 mmol/L; Potassium 80 mmol/L; Calcium 9 mmol/L; Magnesium 2.5 mmol/L, Phosphate 7 mmol/L; Acetate 37.5 mmol/L; Chloride 75 mmol/L; Infuvite Pediatric 5 mL/L; Multitrace-4 1 mL/L; Selenium 10 µg/L; Heparin 1000 units/L | A. Epinephrine hydrochloride, Amphastar B. Milrinone lactate injection, Hikma West-Ward Pharmaceuticals C. Vasopressin, Par Pharmaceutical D. Calcium gluconate, Fresenius Kabi | A. 0.1 mg/L B. 1.0 mg/L C. 1 unit/mL D. 100 mg/mL | A. NaCl 9 mg/mL B. Undiluted C. Glucose 50 mg/mL D. Undiluted | 1 + 1 + 1 + 1 + 1 | C | [12] C grade |
| PN solution containing the following: Amino acids (TrophAmine) 5.7 g/L; Glucose 250 g/L; Sodium 23.1 mmol/L; Potassium 17.1 mmol/L; Calcium 2.9 mmol/L; Magnesium 1.4 mmol/L; Phosphate 3.9 mmol/L; Acetate 11.3 mmol/L; Multivitamin 5.7 mL/L; Trace elements 0.3 mL/L | Amiodarone hydrochloride, Bedford | 16 mg/mL | Sterile water | 1 + 1 | I | [13] C grade |
| Caffeine citrate, Ben Venue | 20 mg/mL | Sterile water | 1 + 1 | C | ||
| Clindamycin phosphate, Hospira | 24 mg/mL | Sterile water | 1 + 1 | C | ||
| Enalaprilat, Baxter | 0.08 mg/mL | Sterile water | C | |||
| Epinephrine hydrochloride, Hospira | 0.0096 mg/mL | Sterile water | 1 + 1 | C | ||
| Fluconazole, Baxter | 2 mg/mL | Sterile water | 1 + 1 | C | ||
| Fosphenytoin sodium, Parke-Davis | 50 mg/mL | Sterile water | 1 + 1 | C | ||
| Hydrocortisone sodium succinate, Pharmacia | 25.6 mg/mL | Sterile water | 1 + 1 | C | ||
| Metoclopramide hydrochloride, Sicor | 0.58 mg/mL | Sterile water | 1 + 1 | C | ||
| Midazolam hydrochloride, Baxter | 0.48 mg/mL | Sterile water | 1 + 1 | C | ||
| Pentobarbital sodium, Abbott | 48 mg/mL | Sterile water | 1 + 1 | I | ||
| Phenobarbital sodium, Baxter | 64 mg/mL | Sterile water | 1 + 1 | I | ||
| Rifampicin, Bedford | 0.3; 7.5; 15; 30 mg/mL | Sterile water | 1 + 1 | I | ||
| Three different PN solutions containing the following: Amino acids (TrophAmine) 28.1–41.7 g/L; Glucose 100–150 g/L; Sodium 10.8–62.5 mmol/L; Potassium 20.1–72.9 mmol/L; Calcium 10.2–24.0 mmol/L; Magnesium 1.2–3.1 mmol/L; Phosphate 8.1–19.2 mmol/L; Pediatric multivitamin 16.1–41.7 mL/L; Pediatric trace elements 1.6–4.2 mL/L; Selenium 24.1–62.5 µg/L; Zinc 1607–4167 µg/L; Molybdenum 2.0–5.2 µg/L; Heparin 500 units/L; Cysteine 1.1–1.7 g/L; Ranitidine 8.0–41.7 mg/L; Levocarnitine 0–416.7 mg/L | Aminophylline solution, Hospira | 2.5 mg/mL | glucose 50 mg/mL | 1 + 1 | C | [14] D grade |
| PN solution containing the following: Amino acids (TrophAmine) 37.5 g/L; Glucose 175 g/L; Sodium 25 mmol/L; Potassium 19 mmol/L; Calcium 9.5 mmol/L; Magnesium 1.9 mmol/L; Phosphate 4.2 mmol/L; Acetate 12.5 mmol/L; MVI- Ped 52 mL/L; Trace Element Injection 4, Pediatric 2.5 mL/L; Ranitidine 73 mg/L | Alprostadil, Bedford | 0.015 mg/mL | Glucose 50 mg/mL; NaCl 9 mg/mL | 1 + 1 | C | [15] D grade |
| Three different PN solutions containing the following: Amino acids (Aminosyn, TrophAmine) 30–40 g/L; Glucose 200 g/L; Sodium 48–93 mmol/L; Potassium 40–60 mmol/L; Calcium 0.7–1.3 mmol/L; Magnesium 2.2–4 mmol/L; Phosphate 7.4–12.9 mmol/L; Multivitamin injection 5 mL/L; Pediatric trace elements 3 mL/L; L-cysteine 0–1.2 g/L; Heparin 500 units/L | Milrinone, Sanofi-Synthelabo | 0.2 mg/mL | Glucose 50 mg/mL; NaCl 9 mg/mL | 1 + 1 | C | [16] D grade |
| Three different PN solutions containing the following: Amino acids (TrophAmine) 20–30 g/L; Glucose 100–200 g/L; Sodium 38–77 mmol/L; Potassium 20–40 mmol/L; Calcium 1.3 mmol/L; Magnesium 1.25 mmol/L; Phosphate 21.4 mmol/L; Acetate 14.5–29 mmol/L; Chloride 38–77 mmol/L; Multivitamin 20 mL/L; Trace elements 2 mL/L; L-cysteine 0.2–0.3 g/L; Heparin 0–500 units/L | Acetazolamide sodium, Lederle | 100 mg/mL | According to SmPC | 1 + 1 | I | [17] D grade |
| Acyclovir sodium, Burroughs Wellcome | 7 mg/mL | 1 + 1 | I | |||
| Amikacin sulfate, Apothecon | 5 mg/mL | 1 + 1 | C | |||
| Aminophylline, American Regent | 5 mg/mL | 1 + 1 | I | |||
| 25 mg/mL | 1 + 1 | I | ||||
| Ampicillin sodium, Apothecon | 100 mg/mL | 1 + 1 | I | |||
| 250 mg/mL | 1 + 1 | I | ||||
| Cefotaxime sodium, Hoechst-Roussel | 60 mg/mL | 1 + 1 | C | |||
| Ceftazidime, Eli Lilly | 60 mg/mL | 1 + 1 | C | |||
| Chlorothiazide sodium, Merck | 28 mg/mL | 1 + 1 | I | |||
| Dexamethasone sodium phosphate, American Regent | 4 mg/mL | 1 + 1 | C | |||
| Dobutamine, Eli Lilly | 5 mg/mL | 1 + 1 | C | |||
| Dopamine, American Regent | 3.2 mg/mL | 1 + 1 | C | |||
| Fentanyl, Elkins-Sinn | 50 µg/mL | 1 + 1 | C | |||
| Furosemide, American Regent | 10 mg/mL | 1 + 1 | C | |||
| Gentamicin sulfate, Elkins-Sinn | 10 mg/mL | 1 + 1 | C | |||
| Metronidazole, Abbott | 5 mg/mL | 1 + 1 | C | |||
| Morphine sulfate, Elkins-Sinn | 1 mg/mL | 1 + 1 | C | |||
| Penicillin G potassium, Marsam | 500.000 units/mL | 1 + 1 | C | |||
| Ranitidine hydrochloride, Glaxo | 25 mg/mL | 1 + 1 | C | |||
| Tobramycin sulfate, Eli Lilly | 10 mg/mL | 1 + 1 | C | |||
| Vancomycin hydrochloride, Eli Lilly | 5 mg/mL | 1 + 1 | C | |||
| Zidovudine, Burroughs Wellcome | 4 mg/mL | 1 + 1 | C |
| Parenteral Nutrition | Drug Solution | Final Concentration of Drug | Diluent | Selected Mixing Ratio of Drug + PN | Compatibility/Incompatibility (C/I) * | Ref./Grade (A,B,C,D) ** |
|---|---|---|---|---|---|---|
| Eight different PN admixtures containing the following: Amino acids (Aminoplasmal Paed/Primene) 19.8 g/L; Glucose 142.9 g/L; Lipids (Lipidem/ClinOleic/SMOFlipid/Intralipid) 39.7 g/L; Sodium 27.7 mmol/L; Potassium 19.9 mmol/L; Magnesium 2.0 mmol/L; Calcium 3.96 mmol/L; Phosphate 4.0 mmol/L; Cernevit 0.5 mL/L; Peditrace 1.0 mL/L | Ondansetron, Accord Healthcare | 0.02 mg/mL | NaCl 9 mg/mL | 1 + 1, 2 + 1 | C | [18] C grade |
| Hydrocortisone, Bausch Health Ireland Limited | 0.98 mg/mL | 1 + 1, 4 + 1 | C | |||
| Dexamethasone, Bausch Health Ireland Limited | 0.08 mg/mL | 1 + 1, 2 + 1 | C | |||
| PN admixture: Numeta G13E; Calcium gluconate 11.7 mmol/L; Phosphate 8.3 mmol/L; Soluvit 10 vials/L; Vitlipid N Infant 100 mL/L; Peditrace 33.3 mL/L | Morphine hydrochloride, Orione | 0.2 mg/mL | Glucose 50 mg/mL | 1 + 1, 1 + 7, 1 + 39 | C | [19] B grade |
| Dopamine hydrochloride, Takeda | 2 mg/mL | Undiluted | 1 + 1, 1 + 6, 1 + 56 | C | ||
| Cefotaxime, Villerton and MIP Pharma | 40 mg/mL | Glucose 50 mg/mL | 1 + 1, 9 + 1, 1 + 20 | C | ||
| PN admixture: Numeta G13E; Soluvit 10 vials/L; Vitlipid N Infant 100 mL/L; Peditrace 33.3 mL/L | Paracetamol, B. Braun | 10 mg/mL | Undiluted | 1 + 1, 1 + 10, 3 + 2 | C | [20] B grade |
| Vancomycin, MIP Pharma | 5 mg/mL | Glucose 50 mg/mL | 1 + 1, 1 + 2, 1 + 5 | C | ||
| Fentanyl, Hameln | 10 µg/mL | Glucose 50 mg/mL | 1 + 1, 1 + 10, 1 + 20 | C | ||
| PN admixture containing the following: Amino acids (Vaminolact) 26.4–27.5 g/L; Glucose 54.2–56.4 g/L; Lipids (SMOFlipid) 23.6 g/L Sodium 16.0 mmol/L; Potassium 15.4–16.0 mmol/L; Calcium 4.5–4.6 mmol/L; Magnesium 1.9–2.0 mmol/L; Phosphate 8.0–10.3 mmol/L; Chloride 24.3–25.3 mmol/L; Sulfate 1.9–2.0 mmol/L; Soluvit 0–2.9 vials/L; Vitlipid N Infant 0–33.4 mL/L; Peditrace 8.0–14.5 mL/L | Ampicillin sodium, Bristol Myers Squibb | 50 mg/mL | NaCl 9 mg/mL | 1 + 10, 1 + 1, 2 + 1 | C/I | [21] B grade |
| Ceftazidime pentahydrate, Fresenius Kabi | 40 mg/mL | Glucose 50 mg/mL | 1 + 10, 1 + 1, 1 + 2 | C/I | ||
| Fluconazole, B. Braun | 2 mg/mL | Undiluted | 1 + 10, 1 + 1, 9 + 1 | C/I | ||
| Fosphenytoin sodium, Pfizer | 10 mg/mL | Glucose 50 mg/mL | 1 + 50, 1 + 1, 5 + 1 | C/I | ||
| Furosemide, Nycomed; Takeda | 2 mg/mL | NaCl 9 mg/mL | 1 + 100, 1 + 1, 2 + 1 | C/I | ||
| Metronidazole, B. Braun | 5 mg/mL | Undiluted | 1 + 10, 1 + 1, 5 + 1 | C/I | ||
| Paracetamol, B. Braun; Fresenius Kabi | 10 mg/mL | Undiluted | 1 + 10, 1 + 1, 1 + 2 | C/I | ||
| Lipid emulsions: Intralipid; Nutrilipid; SMOFlipid | Alprostadil, Pfizer | 20 µg/mL | Glucose 50 mg/mL | 1 + 1 | C/I | [22] C grade |
| Ampicillin/sulbactam, West-Ward | 20 mg/mL | Undiluted | 1 + 1 | C | ||
| Ampicillin, Sandoz | 30 mg/mL | NaCl 9 mg/mL | 1 + 1 | C | ||
| Bumetanide, West-Ward | 0.25 mg/mL | Undiluted | 1 + 1 | C | ||
| Cisatracurium, AbbVie | 2 mg/mL | Undiluted | 1 + 1 | C/I | ||
| Dexmedetomidine, Baxter | 0.004 mg/mL | Undiluted | 1 + 1 | C | ||
| Furosemide, Hospira | 10 mg/mL | Undiluted | 1 + 1 | C | ||
| Gentamicin, Baxter | 2 mg/mL | Undiluted | 1 + 1 | C/I | ||
| Heparin, Fresenius Kabi | 500 units/mL | Undiluted | 1 + 1 | C | ||
| Hydromorphone, Hospira | 2.5 mg/mL | Glucose 50 mg/mL | 1 + 1 | C | ||
| Ketamine, Mylan | 10 mg/mL | Undiluted | 1 + 1 | C | ||
| Lacosamide, UCB | 10 mg/mL | Undiluted | 1 + 1 | C | ||
| Levocarnitine, Leadiant | 50 mg/mL | NaCl 9 mg/mL | 1 + 1 | C | ||
| Milrinone, Hospira | 0.2 mg/mL | Undiluted | 1 + 1 | C | ||
| Ondansetron, Accord | 2 mg/mL | Undiluted | 1 + 1 | C | ||
| Rocuronium, Hospira | 10 mg/mL | Undiluted | 1 + 1 | C/I | ||
| Sildenafil, AuroMedics | 0.8 mg/mL | Undiluted | 1 + 1 | C | ||
| Famotidine, APP Pharmaceuticals | 2.5 mg/mL, 0.25 mg/mL | NaCl 9 mg/mL | 1 + 1 1 + 1 | C/I C | ||
| Three different PN admixtures containing the following: Amino acids (Primene) 30.0–33.0 g/L; Glucose 75.0–100.0 g/L; Sodium 15–33 mmol/L; Potassium 0–1.0 mmol/L; Calcium 12.0 mmol/L; Magnesium 1.5 mmol/L; Phosphate 10.0 mmol/L; Acetate 5.0–40.0 mmol/L; Chloride 9.3–13.5 mmol/L; Zinc 0–326 µg/L; Selenium 0–2 µg/L; Iodide 0–0.8 µg/L; Heparin 500 units/L and Lipid emulsion (SMOFlipid); Soluvit N Infant 50 mL/L; Vitlipid N Infant 200 mL/L | Ibuprofen lysine, BOSC Sciences | 1.25 mg/mL to 5 mg/mL | NaCl 9 mg/mL, RO water | 1 + 1 mixtures of ibuprofen lysine and PN/glucose/IV SMOFlipid | C | [23] C grade |
| Two different PN admixtures: Olimel N5E; Soluvit 0–5.4 vials/L; Vitlipid N Adult 0–9.9 mL/L; Tracel 10 mL/L and Numeta G16E; Soluvit 0–5.4 vials/L; Vitlipid N Infant 0–57.1 mL/L; Peditrace 50 mL/L; | Ampicillin sodium, Bristol Myers Squibb; APP Pharmaceuticals; SAGENT | 50 mg/mL | NaCl 9 mg/mL | Olimel: 1 + 1, 1 + 10, 2 + 1 | I | [24] B grade |
| Numeta: 1 + 1, 1 + 10, 2 + 1 | I | |||||
| Ceftazidime, Fresenius Kabi | 40 mg/mL | Glucose 50 mg/mL | Olimel: 1 + 10, 1 + 1, 2 + 1 | C | ||
| Numeta: 1 + 10, 1 + 1, 1 + 2 | C | |||||
| Clindamycin, Villerton; Pfizer; Stragen | 10 mg/mL | Glucose 50 mg/mL | Olimel: 1 + 25, 1 + 1, 4 + 1 | C | ||
| Numeta: 1 + 33, 1 + 1, 2 + 1 | C | |||||
| Dexamethasone, GALEN | 0.5 mg/mL | Glucose 50 mg/mL | Olimel: 1 + 100, 1 + 1, 2 + 1 | C | ||
| Numeta: 1 + 50, 1 + 1, 1 + 2 | C | |||||
| Fluconazole, B. Braun | 2 mg/mL | Undiluted | Olimel: 1 + 5, 1 + 1, 4 + 1 | C | ||
| Numeta: 1 + 10, 1 + 1, 11 + 1 | C | |||||
| Fosphenytoin sodium, Pfizer | 10 mg/mL | Glucose 50 mg/mL | Olimel: 1 + 25, 1 + 1, 7 + 1 | I | ||
| Numeta: 1 + 33, 1 + 1, 6 + 1 | I | |||||
| Furosemide, Nycomed; Takeda | 2 mg/mL | NaCl 9 mg/mL | Olimel: 1 + 100, 1 + 1, 4 + 1 | C | ||
| Numeta: 1 + 100, 1 + 1, 9 + 4 | I | |||||
| Metronidazole, B. Braun | 5 mg/mL | Undiluted | Olimel: 1 + 5, 1 + 1, 3 + 1 | C | ||
| Numeta: 1 + 8, 1 + 1, 6 + 1 | C | |||||
| Ondansetron hydrochloride, Copyfarm, Fresenius Kabi; Accord | 0.2 mg/mL | Glucose 50 mg/mL | Olimel: 3 + 10, 1 + 1, 2 + 1 | C | ||
| Numeta: 1 + 4, 1 + 1, 1 + 2 | C | |||||
| Paracetamol, Bristol Myers Squibb; Actavis | 10 mg/mL | Undiluted | Olimel: 3 + 5, 1 + 1, 3 + 1 | C | ||
| Numeta: 1 + 4, 1 + 1, 2 + 1 | C |
| Scope of Assessment | Method | Apparatus | References |
|---|---|---|---|
| Visible precipitation, color change, gas production | Visual assessment under white light and against a dark background | Not applied | [10,12,13,14,16,17,23] |
| Fluorescent lighting (not specified) | [15] | ||
| Polarized light viewer | Apollo I, Adelphi Manufacturing Co., Haywards Heath, Sussex, England | [11] | |
| Tyndall beam effect | Light scattering | Intravenous Solution Visual/Clarity Inspection Station Contamination Control Laboratories, Livonia, MI, USA | [16,17] |
| Fiber optic Tyndall beam (Schott KL 1600 LED, Germany) and red laser pen (630–650 nm, P 3010 RoHS, Chongqing, China) | [19,20,21,24] | ||
| Sub-visual particle counting | Light obscuration | AccuSizer 780 Optical Particle Sizer; Nicomp PSS, Santa Barbara, CA, USA | [19,20,21,24] |
| HIAC 9703+, Beckman-Coulter, Indianapolis, IN, USA | [10] | ||
| Backgrounded membrane imaging (BMI) | Horizon Subvisible Particle Analysis Instrument, Halo Labs, Burlingame, CA, USA | [10] | |
| Flow imaging microscopy | FlowCam VS, Yokogawa Fluid-Imaging Technologies Inc., Scarborough, ME, USA | [10] | |
| Turbidity | Nephelometric | Model 2100N, Hach Company, Loveland, CO, USA | [13] |
| 2100Q Turbidimeter, Hach, Loveland, CO, USA | [12] | ||
| TU52000 Laboratory Laser Turbidimeter (Hach Company, Loveland, CO, USA) | [18] | ||
| Formazin nephelometric | 2100Qis Turbidimeter, Hach Lange GmbH, Duesseldorf, Germany | [19,20,21,24] | |
| pH | Potentiometry | Seven Compact, Mettler Toledo, Greifensee, Switzerland | [19,20] |
| Metrohm 744 pH Meter, Metrohm AG, Herisau, Switzerland | [21,24] | ||
| Ohaus Starter pH Meter, Parsippany, NJ, USA | [23] | ||
| Drug concentration | HPLC | Not specified | [11] |
| Scope of Assessment | Method | Apparatus | References |
|---|---|---|---|
| Visible precipitation, color change, gas production | Microscopy | Olympus BX51 Microscope, Olympus America, Melville, NY, USA | [23] |
| Particle size (mean droplet diameter, MDD) | Dynamic light scattering | Zetasizer Nano ZS, Malvern Instruments, Worcestershire, UK | [18,19,20,23] |
| Laser diffraction | Mastersizer 2000 and Hydro 2000G Sample Dispersion Unit, Malvern Instruments, Worcestershire, UK | [21,24] | |
| Particle size (percentage of fat residing in globules larger than 5 µm, PFAT5) | Light obscuration | AccuSizer 780 Optical Particle Sizer; Nicomp PSS, Santa Barbara, CA, USA | [19,20,21,24] |
| HIAC 9703+ Liquid Particle Counting System, Beckman-Coulter Life Sciences | [22] | ||
| pH | Potentiometry | Seven Compact, Mettler Toledo, Greifensee, Switzerland | [18,19,20] |
| Metrohm 744 pH Meter, Metrohm AG, Herisau, Switzerland | [21,24] | ||
| Osmolality | Freezing point depression | Osmometer 800CLG, TridentMed, Warsaw, Poland | [18] |
| Zeta potential | Electrophoretic light scattering | Zetasizer Nano ZS, Malvern Instruments, Worcestershire, UK | [18] |
| Drug concentration | HPLC | Shimadzu LC-20 AD Prominence Liquid Chromatogram connected to a DGU-20AS Prominence Degasser, SIL-20A HT Prominence Autosampler, and SPD-M2DA Prominence Diode Array Detector, Shimadzu Scientific Instruments, Kyoto, Japan | [23] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gostyńska, A.; Przybylski, T.; Ogrodowczyk, M. Y-Site Compatibility Studies of Parenteral Nutrition and Other Intravenous Medications in Neonatal and Pediatric Patients: A Review of the Literature Evidence. Pharmaceutics 2024, 16, 264. https://doi.org/10.3390/pharmaceutics16020264
Gostyńska A, Przybylski T, Ogrodowczyk M. Y-Site Compatibility Studies of Parenteral Nutrition and Other Intravenous Medications in Neonatal and Pediatric Patients: A Review of the Literature Evidence. Pharmaceutics. 2024; 16(2):264. https://doi.org/10.3390/pharmaceutics16020264
Chicago/Turabian StyleGostyńska, Aleksandra, Tomasz Przybylski, and Magdalena Ogrodowczyk. 2024. "Y-Site Compatibility Studies of Parenteral Nutrition and Other Intravenous Medications in Neonatal and Pediatric Patients: A Review of the Literature Evidence" Pharmaceutics 16, no. 2: 264. https://doi.org/10.3390/pharmaceutics16020264
APA StyleGostyńska, A., Przybylski, T., & Ogrodowczyk, M. (2024). Y-Site Compatibility Studies of Parenteral Nutrition and Other Intravenous Medications in Neonatal and Pediatric Patients: A Review of the Literature Evidence. Pharmaceutics, 16(2), 264. https://doi.org/10.3390/pharmaceutics16020264