

Discovery and Potential Utility of a Novel Non-Invasive Ocular Delivery Platform

Abstract
:1. Introduction
2. Materials and Methods
2.1. Compounds
2.2. Formulations
2.3. Non-Invasive Ocular Delivery Platform (NIODP)
2.4. Choice of Animals for Eye Drop and NIODP Ocular Biodisposition Studies
2.5. Biodisposition of JV-DE1 Eye Drops in New Zealand Rabbits
2.6. Biodisposition of JV-DE1 and JV-MD2 Delivered via NIODP in Non-Human Primates
2.7. LC-MS/MS Methods for JV-DE1 in Rabbit Plasma and Ocular Tissues
2.8. LC-MS/MS Methods for JV-DE1 and JV-MD2 in Monkey Plasma and Ocular Tissues
3. Results
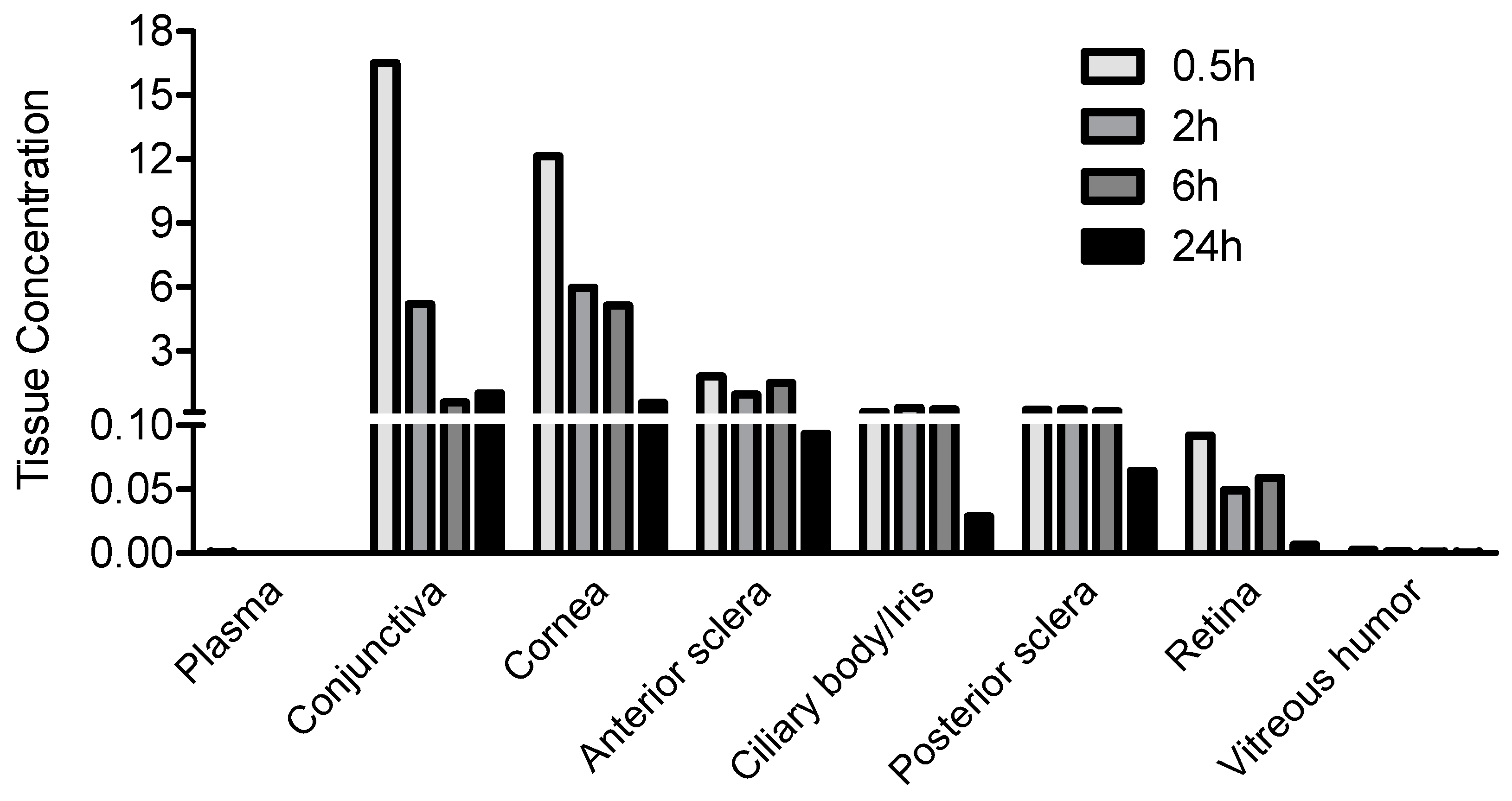
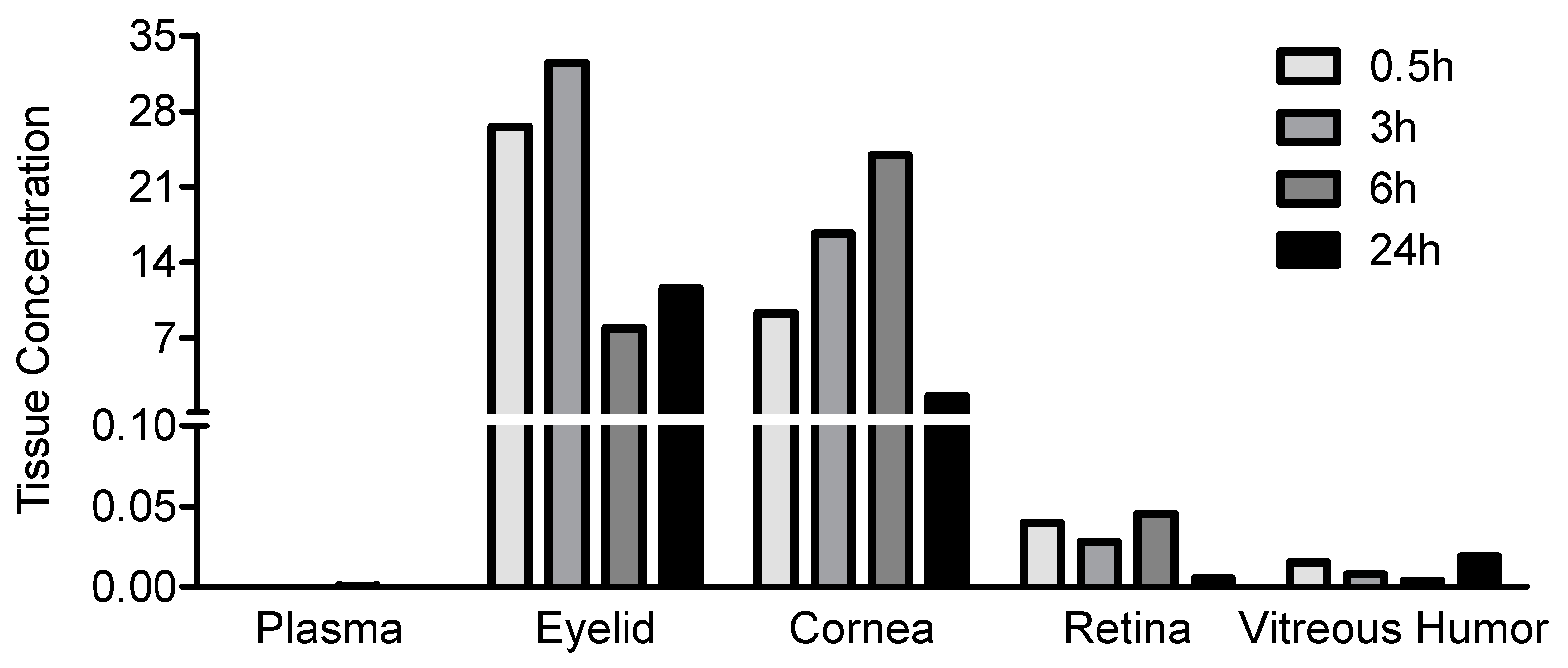
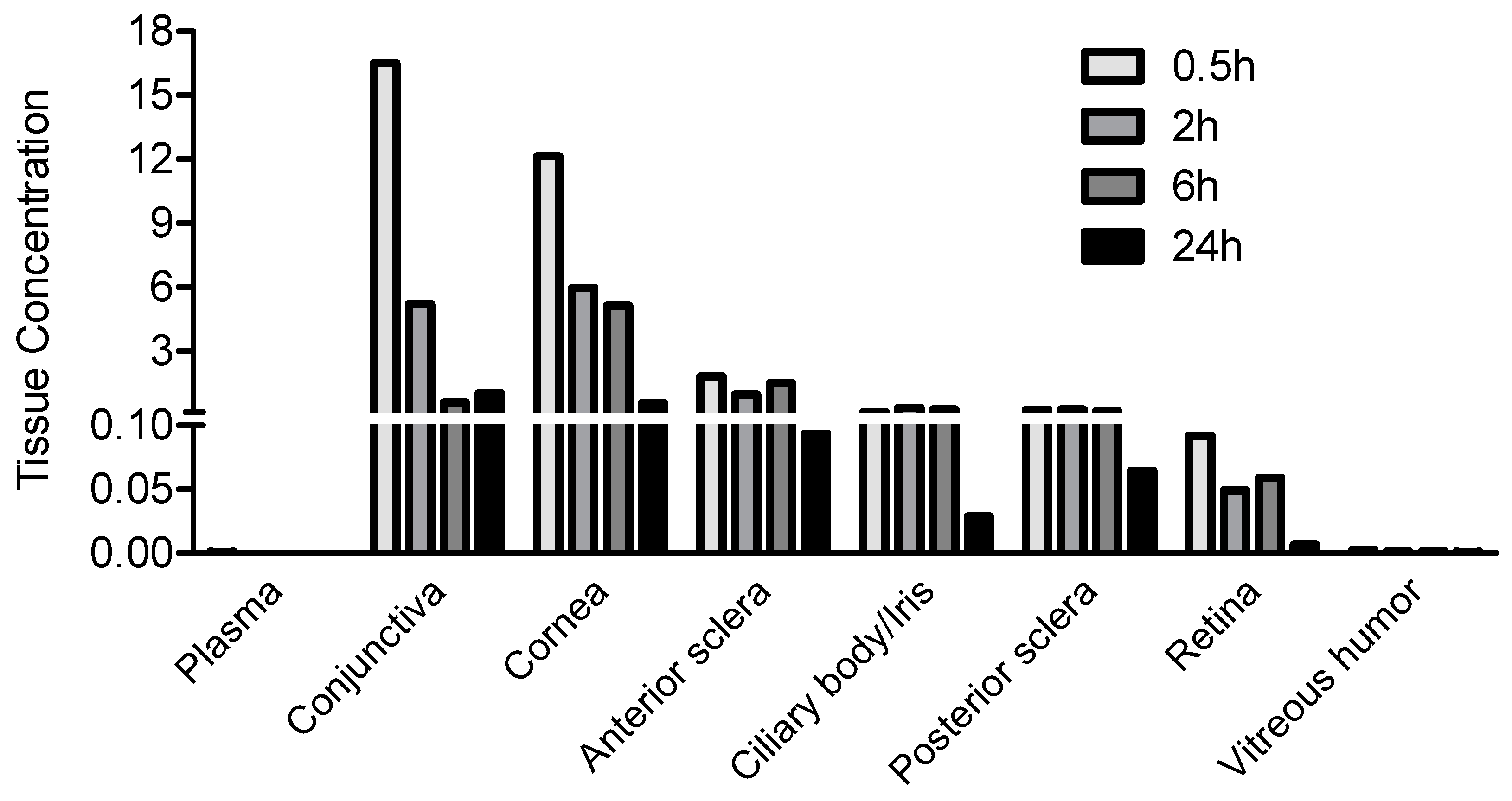
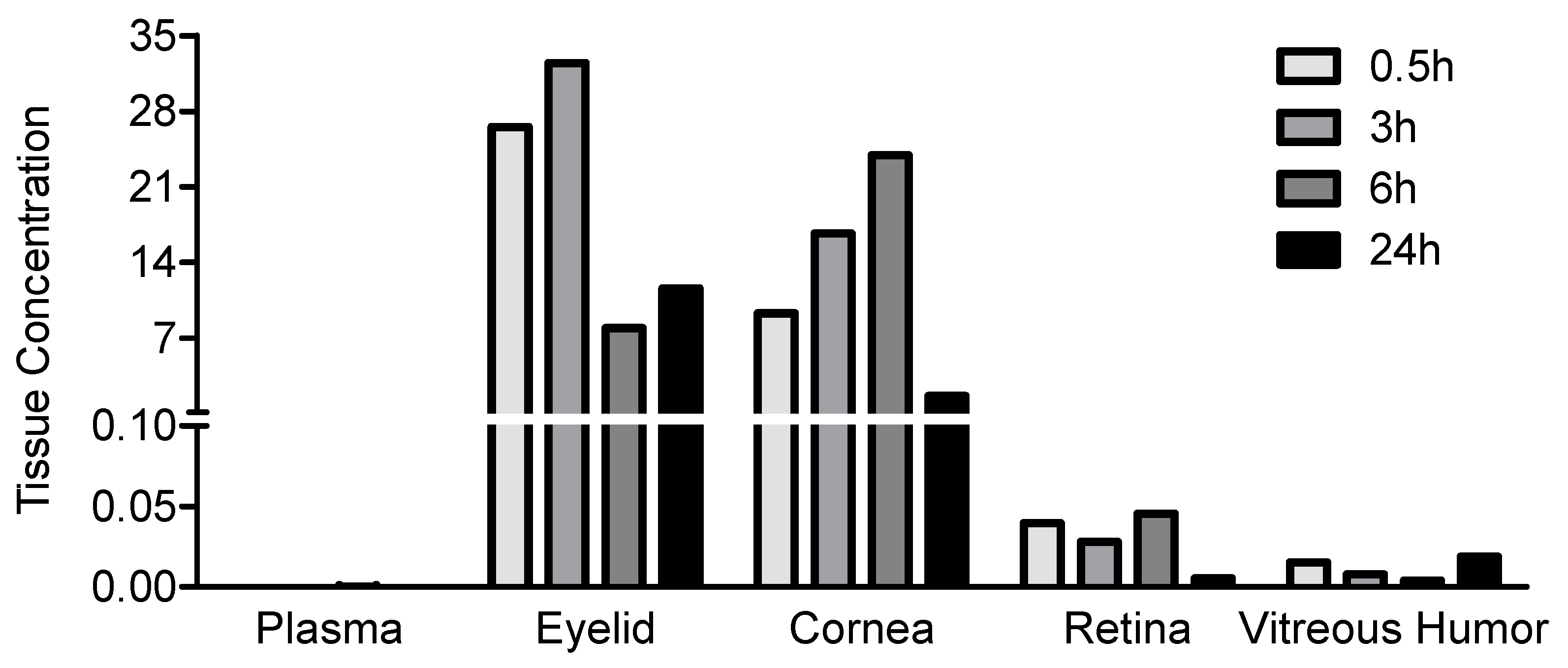
3.1. JV-DE1 Ocular and Plasma Bioavailability Delivered by Eye Drops in New Zealand Rabbits: The Evolution of Eye Drop Administration to Glaucoma Drug Periorbital Skin Delivery, to the Discovery of the Non-Invasive Ocular Delivery Platform (NIODP)
3.2. JV-DE1 Ocular and Plasma Bioavailability after a Single-Dose NIODP Application in Non-Human Primates
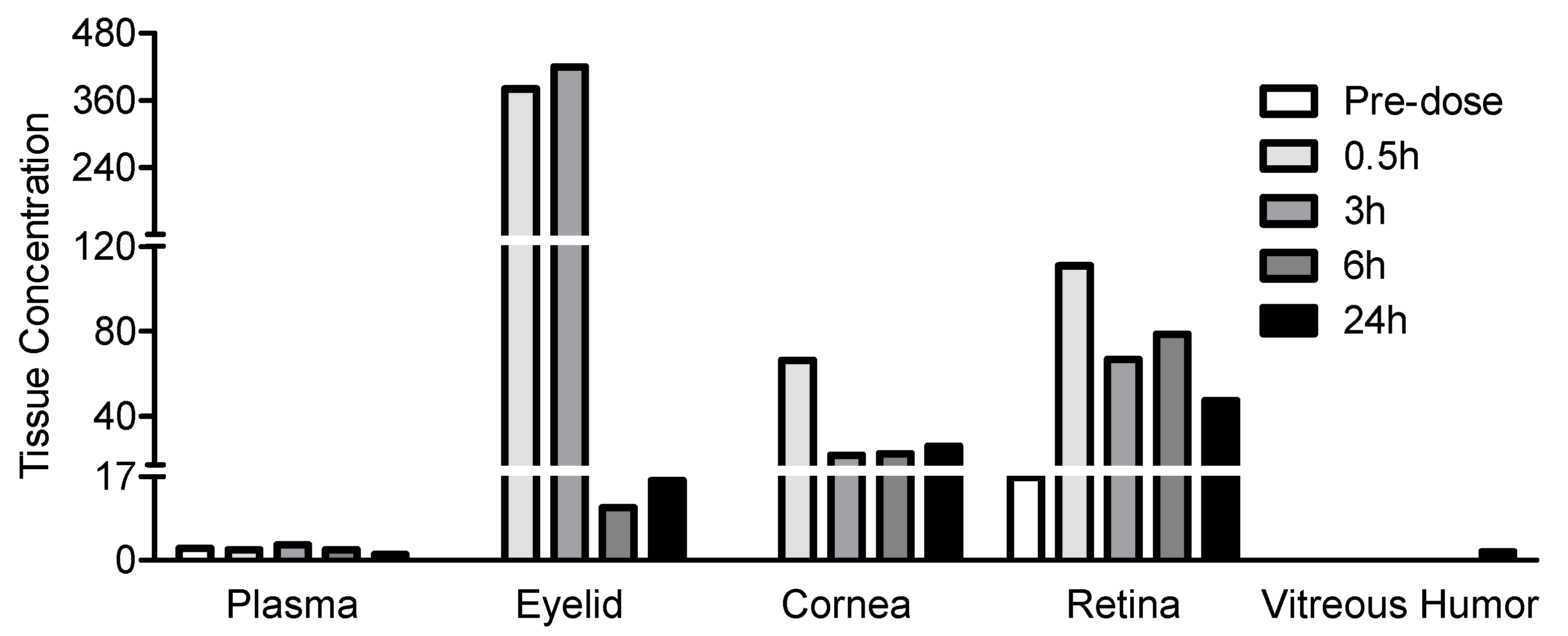
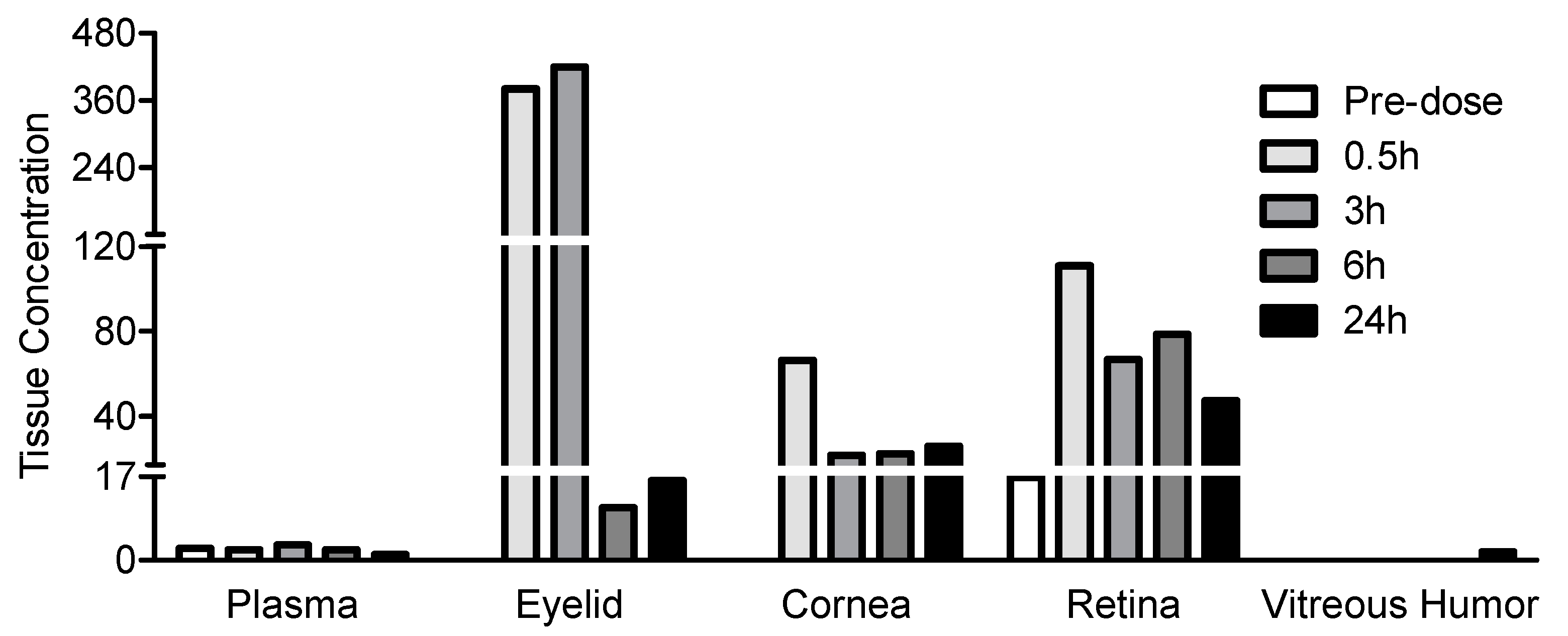
3.3. JV-MD2 Ocular and Plasma Bioavailability via NIODP in Non-Human Primates
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mosteller, M.W.; Gebhardt, B.M.; Hamilton, A.M.; Kaufman, H.E. Penetration of topical cyclosporine into the rabbit cornea, aqueous humor, and serum. Arch. Ophthalmol. 1985, 103, 101–102. [Google Scholar] [CrossRef] [PubMed]
- Said, T.; Dutot, M.; Christon, R.; Beaudeux, J.L.; Martin, C.; Warnet, J.M.; Rat, P. Benefits and side effects of different vegetable oil vectors on apoptosis, oxidative stress, and P2X7 cell death receptor activation. Investig. Ophthalmol. Vis. Sci. 2007, 48, 5000–5006. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, P.; Craig, J.P.; Rupenthal, I.D. Formulation Considerations for the Management of Dry Eye Disease. Pharmaceutics 2021, 13, 207. [Google Scholar] [CrossRef] [PubMed]
- Agrahari, V.; Mandal, A.; Agrahari, V.; Trinh, H.M.; Joseph, M.; Ray, A.; Hadji, H.; Mitra, R.; Pal, D.; Mitra, A.K. A comprehensive insight on ocular pharmacokinetics. Drug Deliv. Transl. Res. 2016, 6, 735–754. [Google Scholar] [CrossRef] [PubMed]
- Sarkadi-Nagy, E.; Wijendran, V.; Diau, G.Y.; Chao, A.C.; Hsieh, A.T.; Turpeinen, A.; Nathanielsz, P.W.; Brenna, J.T. The influence of prematurity and long chain polyunsaturate supplementation in 4-week adjusted age baboon neonate brain and related tissues. Pediatr. Res. 2003, 54, 244–252. [Google Scholar] [CrossRef]
- Sarkadi-Nagy, E.; Wijendran, V.; Diau, G.Y.; Chao, A.C.; Hsieh, A.T.; Turpeinen, A.; Lawrence, P.; Nathanielsz, P.W.; Brenna, J.T. Formula feeding potentiates docosahexaenoic and arachidonic acid biosynthesis in term and preterm baboon neonates. J. Lipid Res. 2004, 45, 71–80. [Google Scholar] [CrossRef]
- Sripetch, S.; Loftsson, T. Topical drug delivery to the posterior segment of the eye: Thermodynamic considerations. Int. J. Pharm. 2021, 597, 120332. [Google Scholar] [CrossRef]
- Hughes, P.M.; Olejnik, O.; Chang-Lin, J.E.; Wilson, C.G. Topical and systemic drug delivery to the posterior segments. Adv. Drug Deliv. Rev. 2005, 57, 2010–2032. [Google Scholar] [CrossRef]
- Tsai, C.H.; Wang, P.Y.; Lin, I.C.; Huang, H.; Liu, G.S.; Tseng, C.L. Ocular Drug Delivery: Role of Degradable Polymeric Nanocarriers for Ophthalmic Application. Int. J. Mol. Sci. 2018, 19, 2830. [Google Scholar] [CrossRef]
- Lakhani, P.; Patil, A.; Majumdar, S. Recent advances in topical nano drug-delivery systems for the anterior ocular segment. Ther. Deliv. 2018, 9, 137–153. [Google Scholar] [CrossRef]
- Molokhia, S.A.; Thomas, S.C.; Garff, K.J.; Mandell, K.J.; Wirostko, B.M. Anterior eye segment drug delivery systems: Current treatments and future challenges. J. Ocul. Pharm. Ther. 2013, 29, 92–105. [Google Scholar] [CrossRef] [PubMed]
- Varela-Fernandez, R.; Diaz-Tome, V.; Luaces-Rodriguez, A.; Conde-Penedo, A.; Garcia-Otero, X.; Luzardo-Alvarez, A.; Fernandez-Ferreiro, A.; Otero-Espinar, F.J. Drug Delivery to the Posterior Segment of the Eye: Biopharmaceutic and Pharmacokinetic Considerations. Pharmaceutics 2020, 12, 269. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, G.A.; Lutz, D.; Shen, J.; Yuan, X.; Shen, H.; Cunningham, J.; Rivers, H.M. Topical Drug Delivery to the Posterior Segment of the Eye: Addressing the Challenge of Preclinical to Clinical Translation. Pharm. Res. 2018, 35, 245. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.M.; Woo, S.J. Ocular Drug Delivery to the Retina: Current Innovations and Future Perspectives. Pharmaceutics 2021, 13, 108. [Google Scholar] [CrossRef]
- Gote, V.; Sikder, S.; Sicotte, J.; Pal, D. Ocular Drug Delivery: Present Innovations and Future Challenges. J. Pharm. Exp. Ther. 2019, 370, 602–624. [Google Scholar] [CrossRef] [PubMed]
- Nomoto, H.; Shiraga, F.; Kuno, N.; Kimura, E.; Fujii, S.; Shinomiya, K.; Nugent, A.K.; Hirooka, K.; Baba, T. Pharmacokinetics of bevacizumab after topical, subconjunctival, and intravitreal administration in rabbits. Invest. Ophthalmol. Vis. Sci. 2009, 50, 4807–4813. [Google Scholar] [CrossRef]
- Davis, B.M.; Normando, E.M.; Guo, L.; Turner, L.A.; Nizari, S.; O’Shea, P.; Moss, S.E.; Somavarapu, S.; Cordeiro, M.F. Topical delivery of Avastin to the posterior segment of the eye in vivo using annexin A5-associated liposomes. Small 2014, 10, 1575–1584. [Google Scholar] [CrossRef]
- De Cogan, F.; Hill, L.J.; Lynch, A.; Morgan-Warren, P.J.; Lechner, J.; Berwick, M.R.; Peacock, A.F.A.; Chen, M.; Scott, R.A.H.; Xu, H.; et al. Topical Delivery of Anti-VEGF Drugs to the Ocular Posterior Segment Using Cell-Penetrating Peptides. Investig. Ophthalmol. Vis. Sci. 2017, 58, 2578–2590. [Google Scholar] [CrossRef]
- Sigurdsson, H.H.; Konraethsdottir, F.; Loftsson, T.; Stefansson, E. Topical and systemic absorption in delivery of dexamethasone to the anterior and posterior segments of the eye. Acta Ophthalmol. Scand. 2007, 85, 598–602. [Google Scholar] [CrossRef]
- Hartman, R.R.; Kompella, U.B. Intravitreal, Subretinal, and Suprachoroidal Injections: Evolution of Microneedles for Drug Delivery. J. Ocul. Pharm. Ther. 2018, 34, 141–153. [Google Scholar] [CrossRef]
- Del Amo, E.M.; Rimpela, A.K.; Heikkinen, E.; Kari, O.K.; Ramsay, E.; Lajunen, T.; Schmitt, M.; Pelkonen, L.; Bhattacharya, M.; Richardson, D.; et al. Pharmacokinetic aspects of retinal drug delivery. Prog. Retin. Eye Res. 2017, 57, 134–185. [Google Scholar] [CrossRef] [PubMed]
- Karti, O.; Saatci, A.O. Intravitreal Dexamethasone Implant in the Treatment of Non-Infectious Uveitic Macular Edema. Med. Hypothesis Discov. Innov. Ophthalmol. 2018, 7, 169–175. [Google Scholar] [PubMed]
- Villegas, V.M.; Gold, A.S.; Wildner, A.; Latiff, A.; Murray, T.G. Intravitreal triamcinolone acetonide: A “real world” analysis of visual acuity, pressure and outcomes. Int. J. Ophthalmol. 2016, 9, 789–791. [Google Scholar] [PubMed]
- Cao, L.; Weetall, M.; Bombard, J.; Qi, H.; Arasu, T.; Lennox, W.; Hedrick, J.; Sheedy, J.; Risher, N.; Brooks, P.C.; et al. Discovery of Novel Small Molecule Inhibitors of VEGF Expression in Tumor Cells Using a Cell-Based High Throughput Screening Platform. PLoS ONE 2016, 11, e0168366. [Google Scholar] [CrossRef]
- Roskoski, R., Jr. The role of small molecule platelet-derived growth factor receptor (PDGFR) inhibitors in the treatment of neoplastic disorders. Pharm. Res. 2018, 129, 65–83. [Google Scholar] [CrossRef]
- Kaiser, P.K. Retina Pipeline 2021 Ongoing Innovation Wet AMD. Available online: https://retinatoday.com/images/retina-pipeline/retina-pipeline-2021/pdfs-for-download/Wet-AMD-Retina-Pipeline-Poster.pdf (accessed on 20 January 2022).
- Kaiser, P.K. Retina Pipeline 2021 Ongoing Innovation Dry AMD. Available online: https://retinatoday.com/images/retina-pipeline/retina-pipeline-2021/pdfs-for-download/Dry-AMD-Retina-Pipeline-Poster.pdf (accessed on 20 January 2022).
- Woodward, D.F.; Wang, J.W.; Coleman, R.A.; Woodrooffe, A.J.; Clark, K.L.; Stamer, W.D.; Tao, G.; Fan, S.; Toris, C.B. A Highly Effective and Ultra-Long-Acting Anti-Glaucoma Drug, with a Novel Periorbital Delivery Method. J. Ocul. Pharm. Ther. 2019, 35, 265–277. [Google Scholar] [CrossRef]
- Dilbeck, M.D.; Spahr, Z.R.; Nanjappa, R.; Economides, J.R.; Horton, J.C. Columnar and Laminar Segregation of Retinal Input to the Primate Superior Colliculus Revealed by Anterograde Tracer Injection Into Each Eye. Investig. Ophthalmol. Vis. Sci. 2022, 63, 9. [Google Scholar] [CrossRef]
- Zarbin, M.A.; Novack, G. N-of-1 Clinical Trials: A Scientific Approach to Personalized Medicine for Patients with Rare Retinal Diseases Such as Retinitis Pigmentosa. J. Ocul. Pharm. Ther. 2021, 37, 495–501. [Google Scholar] [CrossRef]
- Woodward, D.F.; Wenthur, S.L.; Rudebush, T.L.; Fan, S.; Toris, C.B. Prostanoid Receptor Antagonist Effects on Intraocular Pressure, Supported by Ocular Biodisposition Experiments. J. Ocul. Pharm. Ther. 2016, 32, 606–622. [Google Scholar] [CrossRef]
- Zernii, E.Y.; Baksheeva, V.E.; Iomdina, E.N.; Averina, O.A.; Permyakov, S.E.; Philippov, P.P.; Zamyatnin, A.A.; Senin, I.I. Rabbit Models of Ocular Diseases: New Relevance for Classical Approaches. CNS Neurol. Disord. Drug Targets 2016, 15, 267–291. [Google Scholar] [CrossRef]
- Bley, K.R.; Bhattacharya, A.; Daniels, D.V.; Gever, J.; Jahangir, A.; O’Yang, C.; Smith, S.; Srinivasan, D.; Ford, A.P.; Jett, M.F. RO1138452 and RO3244794: Characterization of structurally distinct, potent and selective IP (prostacyclin) receptor antagonists. Br. J. Pharm. 2006, 147, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Watsky, M.A.; Jablonski, M.M.; Edelhauser, H.F. Comparison of conjunctival and corneal surface areas in rabbit and human. Curr. Eye Res. 1988, 7, 483–486. [Google Scholar] [CrossRef] [PubMed]
- Chiang, B.; Jung, J.H.; Prausnitz, M.R. The suprachoroidal space as a route of administration to the posterior segment of the eye. Adv. Drug Deliv. Rev. 2018, 126, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Tyagi, P.; Kadam, R.S.; Kompella, U.B. Comparison of suprachoroidal drug delivery with subconjunctival and intravitreal routes using noninvasive fluorophotometry. PLoS ONE 2012, 7, e48188. [Google Scholar] [CrossRef]
- Scheive, M.; Yazdani, S.; Hajrasouliha, A.R. The utility and risks of therapeutic nanotechnology in the retina. Ther. Adv. Ophthalmol. 2021, 13, 25158414211003381. [Google Scholar] [CrossRef]
- Tornquist, P.; Alm, A.; Bill, A. Permeability of ocular vessels and transport across the blood-retinal-barrier. Eye 1990, 4, 303–309. [Google Scholar] [CrossRef]
- Hammadi, S.; Tzoumas, N.; Ferrara, M.; Meschede, I.P.; Lo, K.; Harris, C.; Lako, M.; Steel, D.H. Bruch’s Membrane: A Key Consideration with Complement-Based Therapies for Age-Related Macular Degeneration. J. Clin. Med. 2023, 12, 2870. [Google Scholar] [CrossRef]
- Clark, S.J.; McHarg, S.; Tilakaratna, V.; Brace, N.; Bishop, P.N. Bruch’s Membrane Compartmentalizes Complement Regulation in the Eye with Implications for Therapeutic Design in Age-Related Macular Degeneration. Front. Immunol. 2017, 8, 1778. [Google Scholar] [CrossRef]
- Ambati, J.; Atkinson, J.P.; Gelfand, B.D. Immunology of age-related macular degeneration. Nat. Rev. Immunol. 2013, 13, 438–451. [Google Scholar] [CrossRef]
- Cheng, S.Y.; Cipi, J.; Ma, S.; Hafler, B.P.; Kanadia, R.N.; Brush, R.S.; Agbaga, M.P.; Punzo, C. Altered photoreceptor metabolism in mouse causes late stage age-related macular degeneration-like pathologies. Proc. Natl. Acad. Sci. USA 2020, 117, 13094–13104. [Google Scholar] [CrossRef]
- Casciano, F.; Zauli, E.; Rimondi, E.; Mura, M.; Previati, M.; Busin, M.; Zauli, G. The role of the mTOR pathway in diabetic retinopathy. Front. Med. 2022, 9, 973856. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, G.C.; Accardi, G.; Monastero, R.; Nicoletti, F.; Libra, M. Ageing: From inflammation to cancer. Immun. Ageing 2018, 15, 1. [Google Scholar] [CrossRef] [PubMed]
- Zou, Z.; Tao, T.; Li, H.; Zhu, X. mTOR signaling pathway and mTOR inhibitors in cancer: Progress and challenges. Cell Biosci. 2020, 10, 31. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Gao, S.; Zhang, Y.; Xin, M.; Zuo, C.; Yan, N.; Xia, Q.; Zhang, M. Dihydroartemisinin Inhibits Laser-Induced Choroidal Neovascularization in a Mouse Model of Neovascular AMD. Front. Pharm. 2022, 13, 838263. [Google Scholar] [CrossRef]
- Gutierrez, S.; Svahn, S.L.; Johansson, M.E. Effects of Omega-3 Fatty Acids on Immune Cells. Int. J. Mol. Sci. 2019, 20, 5028. [Google Scholar] [CrossRef]
- Department of Ophthalmology, H.M.S. AMD Treatment Guidelines. Available online: https://eye.hms.harvard.edu/eyeinsights/2015-january/age-related-macular-degeneration-amd#:~:text=Ninety%20percent%20of%20all%20people,legal%20blindness%20from%20the%20disease (accessed on 27 July 2023).
- Nielsen, M.K. Geographic Atrophy. Available online: https://eyewiki.aao.org/Geographic_Atrophy#:~:text=It%20starts%20typically%20in%20the,of%20all%20individuals%20with%20AMD (accessed on 27 July 2023).
- Georgiou, T.; Prokopiou, E. The New Era of Omega-3 Fatty Acids Supplementation: Therapeutic Effects on Dry Age-Related Macular Degeneration. J. Stem Cells 2015, 10, 205–215. [Google Scholar]
- Prokopiou, K.; Kolovos, P.; Tsangari, H.; Bandello, F.; Rossetti, L.M.; Mastropasqua, L.; Mohand-Said, S.; Georgiou, T. A prospective, multicentre, randomised, double-blind study designed to assess the potential effects of omega-3 fatty acids supplementation in dry age-related macular degeneration or Stargardt disease. Investig. Ophthalmol. Vis. Sci. 2022, 63, 377-F0208. [Google Scholar]
- Souied, E.H.; Delcourt, C.; Querques, G.; Bassols, A.; Merle, B.; Zourdani, A.; Smith, T.; Benlian, P.; Nutritional, A.M.D.T.S.G. Oral docosahexaenoic acid in the prevention of exudative age-related macular degeneration: The Nutritional AMD Treatment 2 study. Ophthalmology 2013, 120, 1619–1631. [Google Scholar] [CrossRef]
- Souied, E.H.; Aslam, T.; Garcia-Layana, A.; Holz, F.G.; Leys, A.; Silva, R.; Delcourt, C. Omega-3 Fatty Acids and Age-Related Macular Degeneration. Ophthalmic Res. 2015, 55, 62–69. [Google Scholar] [CrossRef]
- Edelhauser, H.F.; Rowe-Rendleman, C.L.; Robinson, M.R.; Dawson, D.G.; Chader, G.J.; Grossniklaus, H.E.; Rittenhouse, K.D.; Wilson, C.G.; Weber, D.A.; Kuppermann, B.D.; et al. Ophthalmic drug delivery systems for the treatment of retinal diseases: Basic research to clinical applications. Investig. Ophthalmol. Vis. Sci. 2010, 51, 5403–5420. [Google Scholar] [CrossRef]
- Khoo, H.E.; Ng, H.S.; Yap, W.S.; Goh, H.J.H.; Yim, H.S. Nutrients for Prevention of Macular Degeneration and Eye-Related Diseases. Antioxidants 2019, 8, 85. [Google Scholar] [CrossRef]
- Querques, G.; Forte, R.; Souied, E.H. Retina and omega-3. J. Nutr. Metab. 2011, 2011, 748361. [Google Scholar] [CrossRef]
- Calder, P.C. Omega-3 fatty acids and inflammatory processes. Nutrients 2010, 2, 355–374. [Google Scholar] [CrossRef]
- German, O.L.; Monaco, S.; Agnolazza, D.L.; Rotstein, N.P.; Politi, L.E. Retinoid X receptor activation is essential for docosahexaenoic acid protection of retina photoreceptors. J. Lipid Res. 2013, 54, 2236–2246. [Google Scholar] [CrossRef]
- Lengqvist, J.; Mata De Urquiza, A.; Bergman, A.C.; Willson, T.M.; Sjovall, J.; Perlmann, T.; Griffiths, W.J. Polyunsaturated fatty acids including docosahexaenoic and arachidonic acid bind to the retinoid X receptor alpha ligand-binding domain. Mol. Cell Proteom. 2004, 3, 692–703. [Google Scholar] [CrossRef]
- Itoh, T.; Yamamoto, K. Peroxisome proliferator activated receptor gamma and oxidized docosahexaenoic acids as new class of ligand. Naunyn Schmiedebergs Arch. Pharm. 2008, 377, 541–547. [Google Scholar] [CrossRef]
- Calder, P.C. Omega-3 polyunsaturated fatty acids and inflammatory processes: Nutrition or pharmacology? Br. J. Clin. Pharm. 2013, 75, 645–662. [Google Scholar] [CrossRef]
- Li, X.; Yu, Y.; Funk, C.D. Cyclooxygenase-2 induction in macrophages is modulated by docosahexaenoic acid via interactions with free fatty acid receptor 4 (FFA4). FASEB J. 2013, 27, 4987–4997. [Google Scholar] [CrossRef]
- Iverson, C.; Bacong, A.; Liu, S.; Baumgartner, S.; Lundstrom, T.; Oscarsson, J.; Miner, J.N. Omega-3-carboxylic acids provide efficacious anti-inflammatory activity in models of crystal-mediated inflammation. Sci. Rep. 2018, 8, 1217. [Google Scholar] [CrossRef]
- Mirnikjoo, B.; Brown, S.E.; Kim, H.F.; Marangell, L.B.; Sweatt, J.D.; Weeber, E.J. Protein kinase inhibition by omega-3 fatty acids. J. Biol. Chem. 2001, 276, 10888–10896. [Google Scholar] [CrossRef]
- Djebli, N.; Khier, S.; Griguer, F.; Coutant, A.L.; Tavernier, A.; Fabre, G.; Leriche, C.; Fabre, D. Ocular Drug Distribution After Topical Administration: Population Pharmacokinetic Model in Rabbits. Eur. J. Drug Metab. Pharmacokinet. 2017, 42, 59–68. [Google Scholar] [CrossRef]
- Bos, J.D.; Meinardi, M.M. The 500 Dalton rule for the skin penetration of chemical compounds and drugs. Exp. Dermatol. 2000, 9, 165–169. [Google Scholar] [CrossRef]
- Schramlova, J.; Blazek, K.; Bartackova, M.; Otova, B.; Mardesicova, L.; Zizkovsky, V.; Hulinska, D. Electron microscopic demonstration of the penetration of liposomes through skin. Folia Biol. 1997, 43, 165–169. [Google Scholar]
- Souto, E.B.; Macedo, A.S.; Dias-Ferreira, J.; Cano, A.; Zielinska, A.; Matos, C.M. Elastic and Ultradeformable Liposomes for Transdermal Delivery of Active Pharmaceutical Ingredients (APIs). Int. J. Mol. Sci. 2021, 22, 9743. [Google Scholar] [CrossRef]
- Bisht, R.; Mandal, A.; Jaiswal, J.K.; Rupenthal, I.D. Nanocarrier mediated retinal drug delivery: Overcoming ocular barriers to treat posterior eye diseases. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2018, 10, e1473. [Google Scholar] [CrossRef]
- Ghasemiyeh, P.; Mohammadi-Samani, S. Potential of Nanoparticles as Permeation Enhancers and Targeted Delivery Options for Skin: Advantages and Disadvantages. Drug Des. Dev. Ther. 2020, 14, 3271–3289. [Google Scholar] [CrossRef]
- Shah, S.M.; Ashtikar, M.; Jain, A.S.; Makhija, D.T.; Nikam, Y.; Gude, R.P.; Steiniger, F.; Jagtap, A.A.; Nagarsenker, M.S.; Fahr, A. LeciPlex, invasomes, and liposomes: A skin penetration study. Int. J. Pharm. 2015, 490, 391–403. [Google Scholar] [CrossRef]
- NanoSense Lesson 2: Scale of Objects, Student Materials. Available online: https://nanosense.sri.com/activities/sizematters/sizeandscale/SM_Lesson2Student.pdf (accessed on 27 July 2023).
- Duangjit, S.; Opanasopit, P.; Rojanarata, T.; Ngawhirunpat, T. Characterization and In Vitro Skin Permeation of Meloxicam-Loaded Liposomes versus Transfersomes. J. Drug Deliv. 2011, 2011, 418316. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Test Article | JV-DE1 (0.24% w/v) | |||||
|---|---|---|---|---|---|---|
| Dosing site | Topical eye drop (OD) | |||||
| Rabbit ID | All | 2036281 | 2036282 | 2036283 | 2036284 | |
| Time (h) | 0 | 0.5 | 3 | 6 | 24 | |
| Dose level (μg/eye) | 0 | 120 | 120 | 120 | 120 | |
| Drug in plasma (μg/mL) | BLQ | 0.0010 | 0.0003 | 0.0001 | BLQ | |
| Drug in vitreous humor (μg/mL) | NF * | 0.0026 | 0.0017 | 0.0012 | 0.0004 | |
| Drug in OD Tissues (μg/g) | Conjunctiva | NF * | 16.4919 | 5.1781 | 0.5660 | 0.9937 |
| Cornea | NF * | 12.1249 | 5.9526 | 5.1255 | 0.5422 | |
| Anterior sclera | NF * | 1.7856 | 0.9263 | 1.4785 | 0.0932 | |
| Ciliary body/iris | NF * | 0.1054 | 0.3049 | 0.2314 | 0.0289 | |
| Posterior sclera | NF * | 0.2090 | 0.2395 | 0.1512 | 0.0645 | |
| Retina | NF * | 0.0920 | 0.0491 | 0.0589 | 0.0068 | |
| Vitreous humor (μg/mL) | NF * | 0.0026 | 0.0017 | 0.0012 | 0.0004 | |
| % Administered Dose | Conjunctiva | 1.3929 | 0.4477 | 0.1288 | 0.1467 | |
| Cornea | 0.8622 | 0.4239 | 0.3709 | 0.0254 | ||
| Anterior sclera | 0.2982 | 0.1068 | 0.2139 | 0.0127 | ||
| Ciliary body/iris | 0.0084 | 0.0174 | 0.0137 | 0.0021 | ||
| Posterior sclera | 0.0153 | 0.0323 | 0.0197 | 0.0088 | ||
| Retina | 0.0047 | 0.0036 | 0.0037 | 0.0004 | ||
| Vitreous humor | 0.0023 | 0.0012 | 0.0007 | 0.0004 | ||
| Test Article | JV-DE1 (0.53% w/w) | |||||
|---|---|---|---|---|---|---|
| Dosing site | Periorbital skin (OD) | |||||
| Animal no. | 101 | 101 | 102 | 103 | 104 | |
| Time (h) | 0 | 0.5 | 3 | 6 | 24 | |
| Dose level (μg/eye) | 0 | 179.1 | 160.6 | 162.2 | 159.3 | |
| Drug in plasma (μg/mL) | BLQ | 0.0001 | 0.0002 | 0.0003 | BLQ | |
| Drug in OD Tissues (μg/g) | Eyelid/periorbital skin | NF * | 26.5354 | 32.4547 | 7.9456 | 11.5978 |
| Cornea | NF * | 9.2993 | 16.6887 | 23.9295 | 1.6213 | |
| Retina | NF * | 0.0396 | 0.0279 | 0.0455 | 0.0055 | |
| Vitreous humor (μg/mL) | NF * | 0.0152 | 0.0079 | 0.0039 | 0.0190 | |
| % Administered Dose | Eyelid/periorbital skin | 0.6370 | 1.4956 | 0.3477 | 0.7501 | |
| Cornea | 0.1921 | 0.3430 | 0.5900 | 0.0326 | ||
| Retina | 0.0004 | 0.0004 | 0.0005 | 0.0002 | ||
| Vitreous humor | 0.0047 | 0.0029 | 0.0031 | 0.0018 | ||
| Test Article | JV-MD2 (DHA (21.5% w/w) | |||||
|---|---|---|---|---|---|---|
| Dosing site | Periorbital skin (OS) | |||||
| Animal no. | 101 | 101 | 102 | 103 | 104 | |
| Time (h) | 0 | 0.5 | 3 | 6 | 24 | |
| Dose level (μg/eye) | 0 | 6568 | 6768 | 7018 | 6747 | |
| Drug in plasma (µg/mL) | 2 | 2 | 3 | 2 | 1 | |
| Drug in OS Tissues (µg/g) | Eyelid/periorbital skin | BLQ * | 381 | 420 | 11 | 16 |
| Cornea | BLQ * | 66 | 22 | 22 | 26 | |
| Retina | 17 * | 111 | 67 | 79 | 47 | |
| Vitreous humor | BLQ * | 0 | 0 | 0 | 2 | |
| % Administered Dose | Eyelid/periorbital skin | 0.4288 | 0.3844 | 0.0149 | 0.0197 | |
| Cornea | 0.0283 | 0.0109 | 0.0149 | 0.0173 | ||
| Retina ** | 0.0343 | 0.0264 | 0.0228 | 0.0175 | ||
| Vitreous humor | 0.0000 | 0.0000 | 0.0000 | 0.0236 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, W.; Snider, N. Discovery and Potential Utility of a Novel Non-Invasive Ocular Delivery Platform. Pharmaceutics 2023, 15, 2344. https://doi.org/10.3390/pharmaceutics15092344
Wang W, Snider N. Discovery and Potential Utility of a Novel Non-Invasive Ocular Delivery Platform. Pharmaceutics. 2023; 15(9):2344. https://doi.org/10.3390/pharmaceutics15092344
Chicago/Turabian StyleWang, Weizhen (Jenny), and Nonna Snider. 2023. "Discovery and Potential Utility of a Novel Non-Invasive Ocular Delivery Platform" Pharmaceutics 15, no. 9: 2344. https://doi.org/10.3390/pharmaceutics15092344
APA StyleWang, W., & Snider, N. (2023). Discovery and Potential Utility of a Novel Non-Invasive Ocular Delivery Platform. Pharmaceutics, 15(9), 2344. https://doi.org/10.3390/pharmaceutics15092344