
Theranostic Role of Iron Oxide Nanoparticle for Treating Renal Anemia: Evidence of Efficacy and Significance by MRI, Histology and Biomarkers



Abstract
1. Introduction
2. Materials and Methods
2.1. Reagents
2.2. Animal Procedures
2.3. Hematocrit Measurements
2.4. Iron Parameters
2.5. ELISA
2.6. Histology
2.7. MRI
2.8. Immunohistochemistry
2.9. Statistical Analysis
3. Results
3.1. The Chemical Properties and Stability of IOP Injection
3.2. Changes in Hematopoiesis in Sham and SNx Mice after IOP Injection
3.3. Changes in the Iron Parameters in Sham and SNx Mice after IOP Injection
3.4. Changes in Proinflammatory Cytokines and Oxidative Stress in Sham and SNx Mice after IOP Injection
3.5. MRI Visualization of the Abdomen before and after IOP Injection
3.6. Histological Analysis of the Presence of IOPs
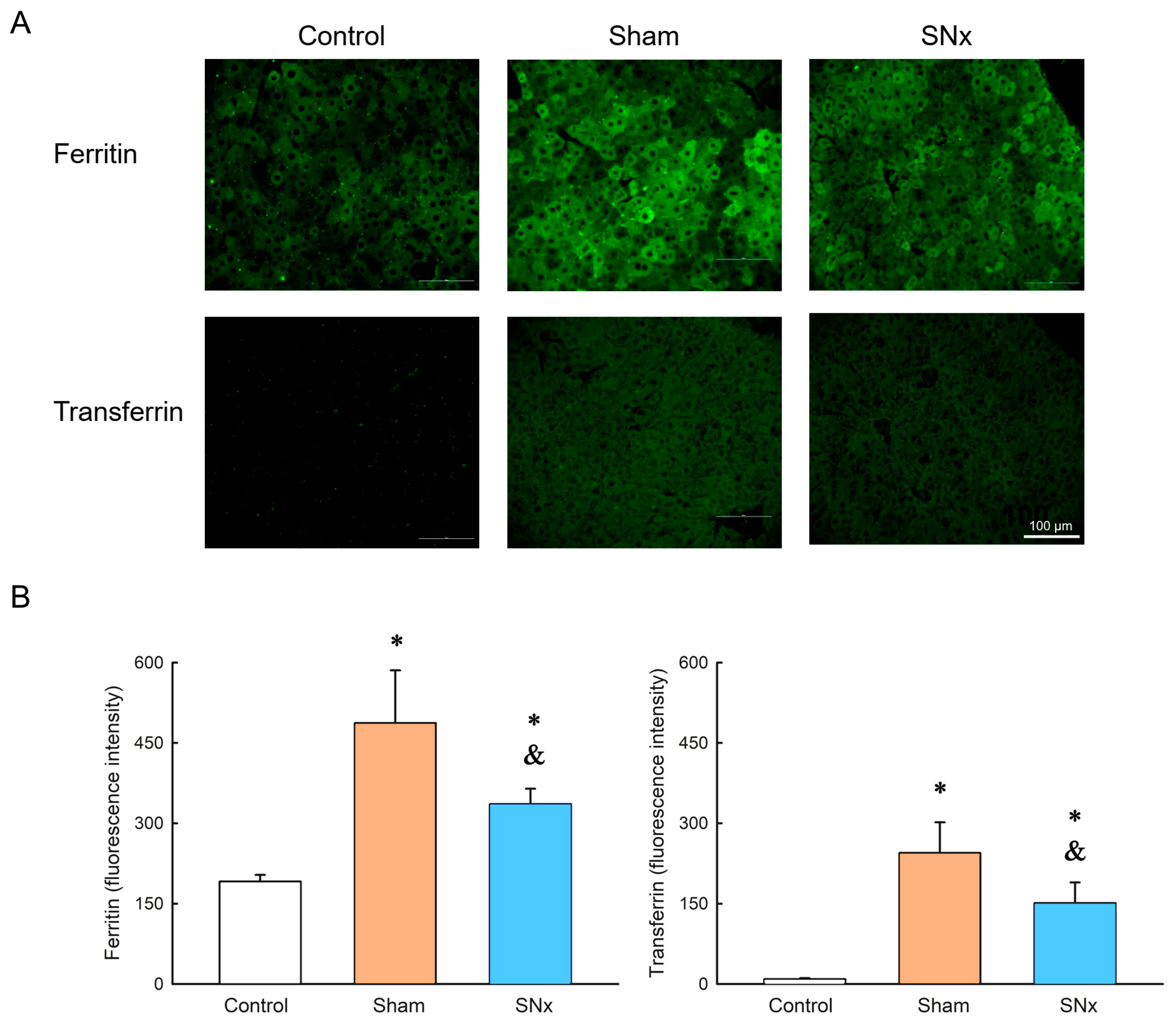
3.7. Ferritin and Transferrin Expression in Liver
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Camaschella, C. Iron-Deficiency Anemia. N. Engl. J. Med. 2015, 372, 1832–1843. [Google Scholar] [CrossRef]
- Cappellini, M.D.; Musallam, K.M.; Taher, A.T. Iron deficiency anaemia revisited. J. Intern. Med. 2020, 287, 153–170. [Google Scholar] [CrossRef]
- DeLoughery, T.G. Iron Deficiency Anemia. Med. Clin. N. Am. 2017, 101, 319–332. [Google Scholar] [CrossRef] [PubMed]
- Bullivant, J.P.; Zhao, S.; Willenberg, B.J.; Kozissnik, B.; Batich, C.D.; Dobson, J. Materials characterization of Feraheme/ferumoxytol and preliminary evaluation of its potential for magnetic fluid hyperthermia. Int. J. Mol. Sci. 2013, 14, 17501–17510. [Google Scholar] [CrossRef] [PubMed]
- Auerbach, M.; Chertow, G.M.; Rosner, M. Ferumoxytol for the treatment of iron deficiency anemia. Expert Rev. Hematol. 2018, 11, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Babitt, J.L.; Lin, H.Y. Mechanisms of anemia in CKD. J. Am. Soc. Nephrol. JASN 2012, 23, 1631–1634. [Google Scholar] [CrossRef]
- Macdougall, I.C.; Tucker, B.; Thompson, J.; Tomson, C.R.; Baker, L.R.; Raine, A.E. A randomized controlled study of iron supplementation in patients treated with erythropoietin. Kidney Int. 1996, 50, 1694–1699. [Google Scholar] [CrossRef]
- Markowitz, G.S.; Kahn, G.A.; Feingold, R.E.; Coco, M.; Lynn, R.I. An evaluation of the effectiveness of oral iron therapy in hemodialysis patients receiving recombinant human erythropoietin. Clin. Nephrol. 1997, 48, 34–40. [Google Scholar]
- Fudin, R.; Jaichenko, J.; Shostak, A.; Bennett, M.; Gotloib, L. Correction of uremic iron deficiency anemia in hemodialyzed patients: A prospective study. Nephron 1998, 79, 299–305. [Google Scholar] [CrossRef]
- Kuo, K.L.; Hung, S.C.; Wei, Y.H.; Tarng, D.C. Intravenous iron exacerbates oxidative DNA damage in peripheral blood lymphocytes in chronic hemodialysis patients. J. Am. Soc. Nephrol. JASN 2008, 19, 1817–1826. [Google Scholar] [CrossRef]
- Kuo, K.L.; Hung, S.C.; Lin, Y.P.; Tang, C.F.; Lee, T.S.; Lin, C.P.; Tarng, D.C. Intravenous ferric chloride hexahydrate supplementation induced endothelial dysfunction and increased cardiovascular risk among hemodialysis patients. PLoS ONE 2012, 7, e50295. [Google Scholar] [CrossRef] [PubMed]
- Kuo, K.L.; Hung, S.C.; Lee, T.S.; Tarng, D.C. Iron sucrose accelerates early atherogenesis by increasing superoxide production and upregulating adhesion molecules in CKD. J. Am. Soc. Nephrol. JASN 2014, 25, 2596–2606. [Google Scholar] [CrossRef] [PubMed]
- Alphandéry, E. Biodistribution and targeting properties of iron oxide nanoparticles for treatments of cancer and iron anemia disease. Nanotoxicology 2019, 13, 573–596. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Liu, Y.; Huang, J.; Chen, K.; Huang, J.; Xiao, K. Uptake, distribution, clearance, and toxicity of iron oxide nanoparticles with different sizes and coatings. Sci. Rep. 2018, 8, 2082. [Google Scholar] [CrossRef]
- Arami, H.; Khandhar, A.; Liggitt, D.; Krishnan, K.M. In vivo delivery, pharmacokinetics, biodistribution and toxicity of iron oxide nanoparticles. Chem. Soc. Rev. 2015, 44, 8576–8607. [Google Scholar] [CrossRef]
- Sakulkhu, U.; Mahmoudi, M.; Maurizi, L.; Salaklang, J.; Hofmann, H. Protein corona composition of superparamagnetic iron oxide nanoparticles with various physico-chemical properties and coatings. Sci. Rep. 2014, 4, 5020. [Google Scholar] [CrossRef]
- Spinowitz, B.S.; Kausz, A.T.; Baptista, J.; Noble, S.D.; Sothinathan, R.; Bernardo, M.V.; Brenner, L.; Pereira, B.J. Ferumoxytol for treating iron deficiency anemia in CKD. J. Am. Soc. Nephrol. JASN 2008, 19, 1599–1605. [Google Scholar] [CrossRef]
- Lu, C.H.; Hsiao, J.K. Diagnostic and therapeutic roles of iron oxide nanoparticles in biomedicine. Tzu Chi Med. J. 2023, 35, 11–17. [Google Scholar] [CrossRef]
- Chen, C.L.; Zhang, H.; Ye, Q.; Hsieh, W.Y.; Hitchens, T.K.; Shen, H.H.; Liu, L.; Wu, Y.J.; Foley, L.M.; Wang, S.J.; et al. A new nano-sized iron oxide particle with high sensitivity for cellular magnetic resonance imaging. Mol. Imaging Biol. 2011, 13, 825–839. [Google Scholar] [CrossRef]
- Liu, L.; Ye, Q.; Wu, Y.; Hsieh, W.Y.; Chen, C.L.; Shen, H.H.; Wang, S.J.; Zhang, H.; Hitchens, T.K.; Ho, C. Tracking T-cells in vivo with a new nano-sized MRI contrast agent. Nanomed. Nanotechnol. Biol. Med. 2012, 8, 1345–1354. [Google Scholar] [CrossRef]
- Chen, C.L.; Siow, T.Y.; Chou, C.H.; Lin, C.H.; Lin, M.H.; Chen, Y.C.; Hsieh, W.Y.; Wang, S.J.; Chang, C. Targeted Superparamagnetic Iron Oxide Nanoparticles for In Vivo Magnetic Resonance Imaging of T-Cells in Rheumatoid Arthritis. Mol. Imaging Biol. 2017, 19, 233–244. [Google Scholar] [CrossRef]
- Hung, S.C.; Kuo, K.L.; Huang, H.L.; Lin, C.C.; Tsai, T.H.; Wang, C.H.; Chen, J.W.; Lin, S.J.; Huang, P.H.; Tarng, D.C. Indoxyl sulfate suppresses endothelial progenitor cell-mediated neovascularization. Kidney Int. 2016, 89, 574–585. [Google Scholar] [CrossRef] [PubMed]
- Kuo, K.L.; Zhao, J.F.; Huang, P.H.; Guo, B.C.; Tarng, D.C.; Lee, T.S. Indoxyl sulfate impairs valsartan-induced neovascularization. Redox Biol. 2020, 30, 101433. [Google Scholar] [CrossRef] [PubMed]
- Vu’o’ng Lê, B.; Khorsi-Cauet, H.; Villegier, A.S.; Bach, V.; Gay-Quéheillard, J. New rat models of iron sucrose-induced iron overload. Exp. Biol. Med. 2011, 236, 790–799. [Google Scholar] [CrossRef]
- Bhandari, S.; Pereira, D.I.A.; Chappell, H.F.; Drakesmith, H. Intravenous Irons: From Basic Science to Clinical Practice. Pharmaceuticals 2018, 11, 82. [Google Scholar] [CrossRef]
- Luo, Y.; Henle, E.S.; Linn, S. Oxidative damage to DNA constituents by iron-mediated fenton reactions. The deoxycytidine family. J. Biol. Chem. 1996, 271, 21167–21176. [Google Scholar] [CrossRef]
- Henle, E.S.; Luo, Y.; Gassmann, W.; Linn, S. Oxidative damage to DNA constituents by iron-mediated fenton reactions. The deoxyguanosine family. J. Biol. Chem. 1996, 271, 21177–21186. [Google Scholar] [CrossRef]
- Kuo, K.L.; Hung, S.C.; Liu, J.S.; Chang, Y.K.; Hsu, C.C.; Tarng, D.C. Iron supplementation associates with low mortality in pre-dialyzed advanced chronic kidney disease patients receiving erythropoiesis-stimulating agents: A nationwide database analysis. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 2015, 30, 1518–1525. [Google Scholar] [CrossRef]
- Kuo, K.L.; Hung, S.C.; Tseng, W.C.; Tsai, M.T.; Liu, J.S.; Lin, M.H.; Hsu, C.C.; Tarng, D.C. Association of Anemia and Iron Parameters With Mortality Among Patients Undergoing Prevalent Hemodialysis in Taiwan: The AIM-HD Study. J. Am. Heart Assoc. 2018, 7, e009206. [Google Scholar] [CrossRef]
- Kuo, K.L.; Liu, J.S.; Lin, M.H.; Hsu, C.C.; Tarng, D.C. Association of anemia and iron parameters with mortality among prevalent peritoneal dialysis patients in Taiwan: The AIM-PD study. Sci. Rep. 2022, 12, 1269. [Google Scholar] [CrossRef] [PubMed]
- Drüeke, T.B.; Massy, Z.A. Oral or intravenous iron for anemia correction in chronic kidney disease? Kidney Int. 2015, 88, 673–675. [Google Scholar] [CrossRef]
- Neiser, S.; Koskenkorva, T.S.; Schwarz, K.; Wilhelm, M.; Burckhardt, S. Assessment of Dextran Antigenicity of Intravenous Iron Preparations with Enzyme-Linked Immunosorbent Assay (ELISA). Int. J. Mol. Sci. 2016, 17, 1185. [Google Scholar] [CrossRef]
- Koskenkorva-Frank, T.S.; Weiss, G.; Koppenol, W.H.; Burckhardt, S. The complex interplay of iron metabolism, reactive oxygen species, and reactive nitrogen species: Insights into the potential of various iron therapies to induce oxidative and nitrosative stress. Free Radic. Biol. Med. 2013, 65, 1174–1194. [Google Scholar] [CrossRef] [PubMed]
- Auerbach, M.; Ballard, H.; Glaspy, J. Clinical update: Intravenous iron for anaemia. Lancet 2007, 369, 1502–1504. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Hsu, J.C.; Koo, H.; Cormode, D.P. Repurposing ferumoxytol: Diagnostic and therapeutic applications of an FDA-approved nanoparticle. Theranostics 2022, 12, 796–816. [Google Scholar] [CrossRef] [PubMed]
- Ling, X.C.; Kuo, K.-L. Oxidative stress in chronic kidney disease. Ren. Replace. Ther. 2018, 4, 53. [Google Scholar] [CrossRef]
- Unterweger, H.; Janko, C.; Folk, T.; Cicha, I.; Kovács, N.; Gyebnár, G.; Horváth, I.; Máthé, D.; Zheng, K.H.; Coolen, B.F.; et al. Comparative in vitro and in vivo Evaluation of Different Iron Oxide-Based Contrast Agents to Promote Clinical Translation in Compliance with Patient Safety. Int. J. Nanomed. 2023, 18, 2071–2086. [Google Scholar] [CrossRef] [PubMed]
- Curcio, A.; Van de Walle, A.; Péchoux, C.; Abou-Hassan, A.; Wilhelm, C. In Vivo Assimilation of CuS, Iron Oxide and Iron Oxide@CuS Nanoparticles in Mice: A 6-Month Follow-Up Study. Pharmaceutics 2022, 14, 179. [Google Scholar] [CrossRef]
- Briley-Saebo, K.; Bjørnerud, A.; Grant, D.; Ahlstrom, H.; Berg, T.; Kindberg, G.M. Hepatic cellular distribution and degradation of iron oxide nanoparticles following single intravenous injection in rats: Implications for magnetic resonance imaging. Cell Tissue Res. 2004, 316, 315–323. [Google Scholar] [CrossRef]
- Dupas, B.; Berreur, M.; Rohanizadeh, R.; Bonnemain, B.; Meflah, K.; Pradal, G. Electron microscopy study of intrahepatic ultrasmall superparamagnetic iron oxide kinetics in the rat. Relation with magnetic resonance imaging. Biol. Cell 1999, 91, 195–208. [Google Scholar] [CrossRef]
- Sibille, J.C.; Kondo, H.; Aisen, P. Interactions between isolated hepatocytes and Kupffer cells in iron metabolism: A possible role for ferritin as an iron carrier protein. Hepatology 1988, 8, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Laskar, A.; Ghosh, M.; Khattak, S.I.; Li, W.; Yuan, X.M. Degradation of superparamagnetic iron oxide nanoparticle-induced ferritin by lysosomal cathepsins and related immune response. Nanomedicine 2012, 7, 705–717. [Google Scholar] [CrossRef] [PubMed]
- Gomi, T.; Nagamoto, M.; Tsunoo, M.; Terada, S.; Terada, H.; Kohda, E. Evaluation of the changes in signals from the spleen using ferucarbotran. Radiat. Med. 2007, 25, 135–138. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Acceptance Criteria | IOP Injection (Batch No.: MPB-1523) | |
| Condition: 5 ± 3 °C | |||
| Testing Interval, Month | |||
| 0 | 12 | ||
| Appearance | Dark brown to black solution | Confirm | Confirm |
| Identification | Corresponds to the reference peaks | Confirm | Confirm |
| Assay | 20.0 ± 2.0 mg/mL | 20.6 mg/mL | 20.2 mg/mL |
| Particle size | Z average: 65 ± 20 nm; (PDI < 0.3) | 60 nm; PDI = 0.2 | 61 nm; PDI = 0.2 |
| Zeta potential | 0~−20 mV | −2 mV | −2 mV |
| Bacterial endotoxin | NMT 6 EU/mL | <6 EU/mL | <6 EU/mL |
| Sterility | Sterile | Sterile | Sterile |
| pH | 5.5–7.5 | 6.3 | 5.7 |
| Impurity | Individual impurity: <0.5% Total impurities: <3.0% | Individual impurity: ND Total impurities: ND 1 | rrt 1.00: 0.4% rrt 1.20: 0.4% rrt 1.24: 0.4% Total impurities: 1.3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsiao, J.-K.; Chen, C.-L.; Hsieh, W.-Y.; Kuo, K.-L. Theranostic Role of Iron Oxide Nanoparticle for Treating Renal Anemia: Evidence of Efficacy and Significance by MRI, Histology and Biomarkers. Pharmaceutics 2023, 15, 1714. https://doi.org/10.3390/pharmaceutics15061714
Hsiao J-K, Chen C-L, Hsieh W-Y, Kuo K-L. Theranostic Role of Iron Oxide Nanoparticle for Treating Renal Anemia: Evidence of Efficacy and Significance by MRI, Histology and Biomarkers. Pharmaceutics. 2023; 15(6):1714. https://doi.org/10.3390/pharmaceutics15061714
Chicago/Turabian StyleHsiao, Jong-Kai, Chih-Lung Chen, Wen-Yuan Hsieh, and Ko-Lin Kuo. 2023. "Theranostic Role of Iron Oxide Nanoparticle for Treating Renal Anemia: Evidence of Efficacy and Significance by MRI, Histology and Biomarkers" Pharmaceutics 15, no. 6: 1714. https://doi.org/10.3390/pharmaceutics15061714
APA StyleHsiao, J.-K., Chen, C.-L., Hsieh, W.-Y., & Kuo, K.-L. (2023). Theranostic Role of Iron Oxide Nanoparticle for Treating Renal Anemia: Evidence of Efficacy and Significance by MRI, Histology and Biomarkers. Pharmaceutics, 15(6), 1714. https://doi.org/10.3390/pharmaceutics15061714