
Regeneration of Articular Cartilage Using Membranes of Polyester Scaffolds in a Rabbit Model

 ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
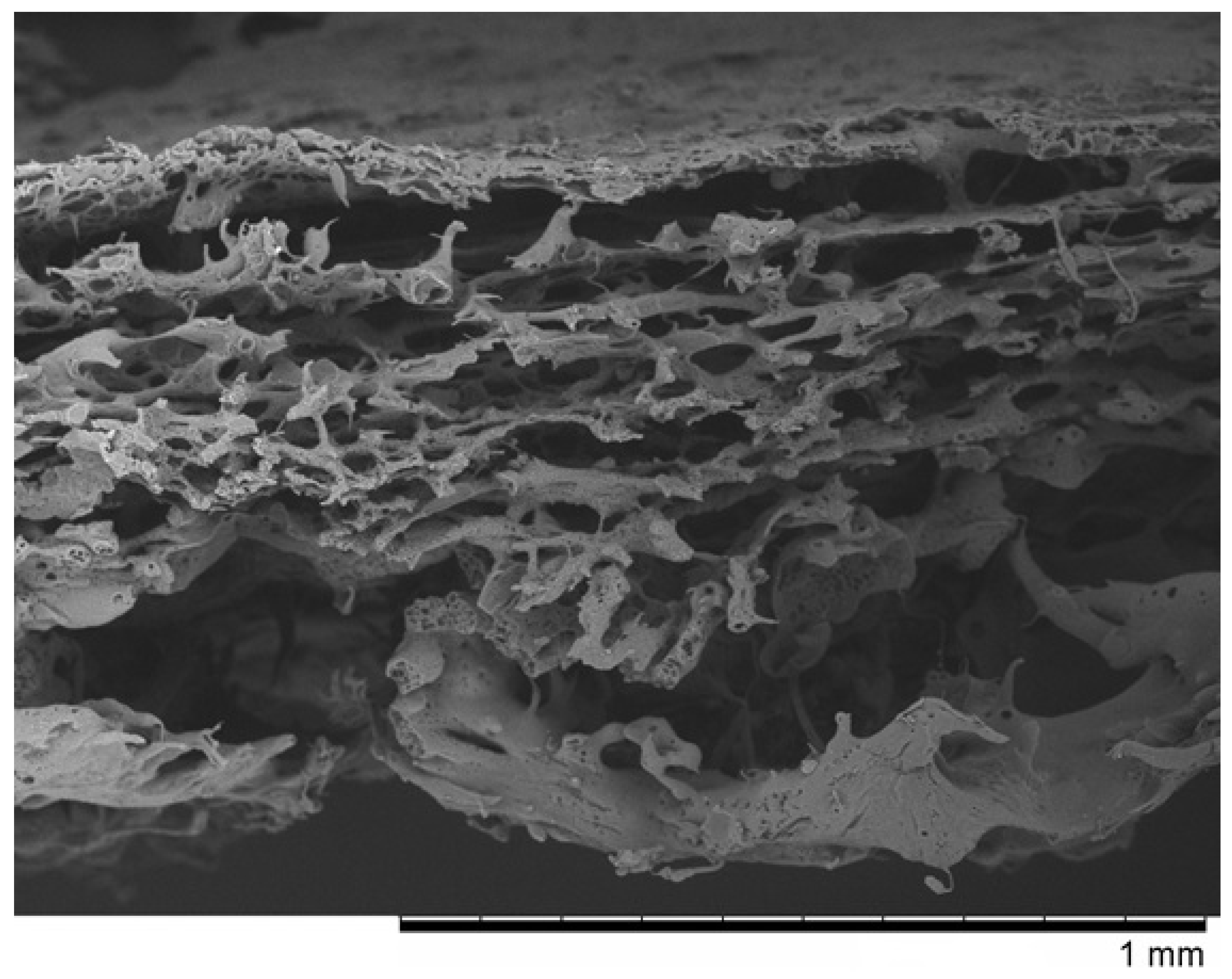
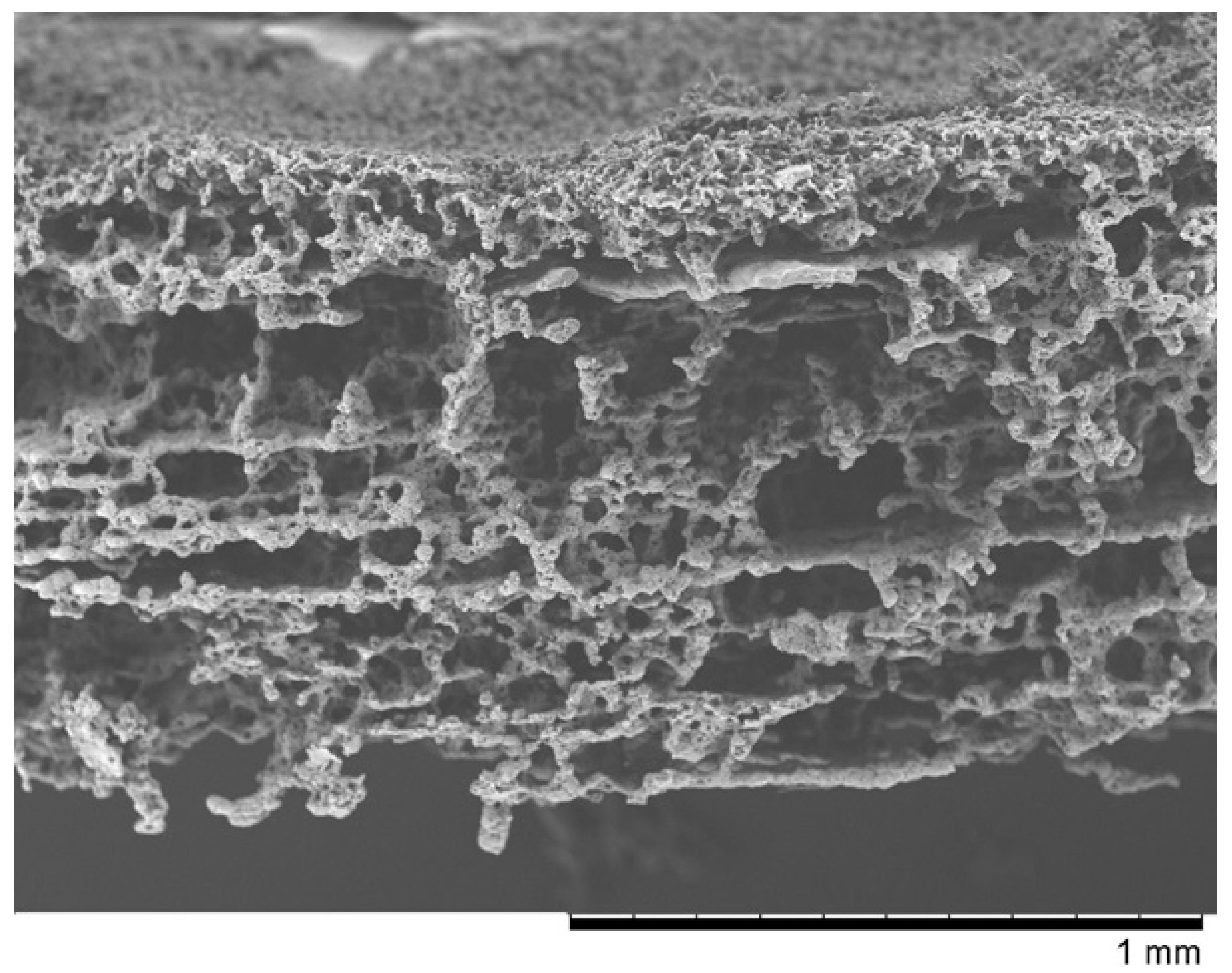
2.1.1. Membranes
2.1.2. Rabbits
2.2. Methods
2.2.1. Implantation
- (a)
- We administered general anesthesia intramuscularly (xylazine and ketamine—dose calculated according to the animal’s body weight; ketamine—0.4 mg/kg, xylazine 0.5 mg/kg).
- (b)
- We shaved the area to be operated.
- (c)
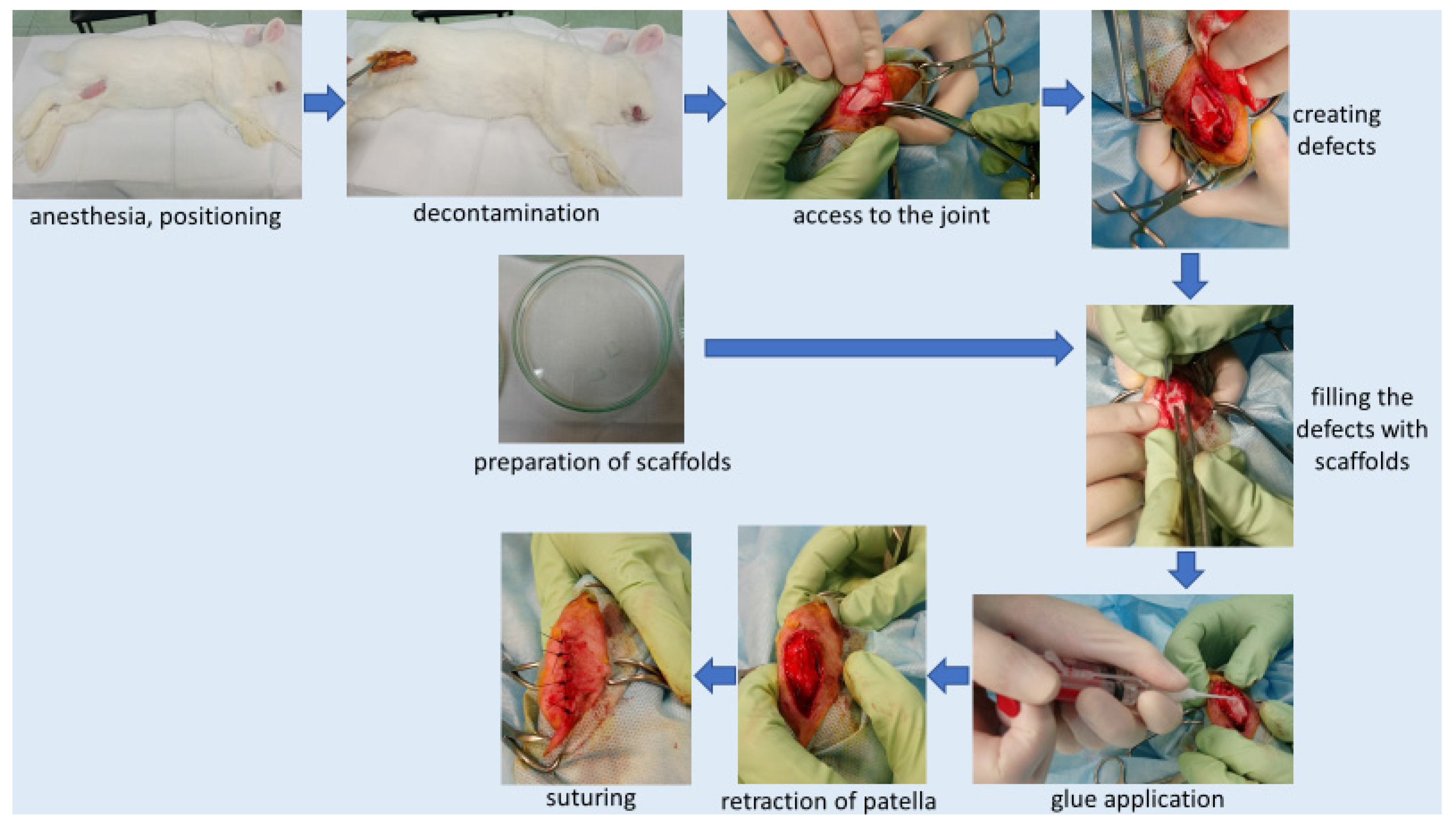
- We placed the animal on the side opposite the one to be operated, with the limb in abduction. Skin decontamination with iodine solution. We covered the operating area with sterile drapes, which were attached to the skin.
- (d)
- We prepared the scaffold (membrane “PVP” or “Z”—depending on group). Under sterile conditions, we removed the membrane immersed in alcohol in transport packaging and placed the membrane in sterile petri dishes filled with a 0.9% NaCl solution. Rinsed the membranes twice at 10-min intervals with a 0.9% NaCl solution (to get rid of alcohol). For each animal, membranes were prepared in a separate petri dish. This point was omitted in the control group (where no membrane was used).
- (e)
- Skin incision on the lateral side at the level of the knee joint, then the incision of subcutaneous tissue and the joint capsule. Dislocation of the kneecap to the medial side, providing access to the articular surface of the femur. We created 2 defects located symmetrically at both condyles (each condyle had one defect) of the femur (load bearing area), using a chisel (Figure 3). Defect (0.1 cm2) of cartilage and bone to a depth of 3 mm. Confirming a full-depth defect penetrating the bone marrow by the occurrence of bleeding from the base of the defects.
- (f)
- We rinsed the defects with sterile 0.9% NaCl solution and dried them (to get rid of any debris). We cut a scaffold to the size of the defect and inserted a scaffold inside the defect so that the more porous surface of the membrane was in direct contact with the bone marrow.
- (g)
- After filling the defects with membranes, we applied the tissue glue (TisselLyo) to the surface of the defects according to the manufacturer’s instructions.
- (h)
- We waited for the adhesive to bond with the surrounding tissues. We moved back the kneecap into the correct position. We sutured the articular capsule with a Vicryl 3/0 suture, subcutaneous suture—Vicryl 4/0, skin suture—Ethilon 4/0 (to be removed in 14 days). We covered the postoperative wound with iodoform. Sterile dressing. We applied soft dressing from the ankle to the groin for 24 h.
- (i)
- Postoperative administration of antibiotics (Enrofloxacin) and analgesics (Metamizole) for 2 days.
- (j)
- Due to animal welfare reasons, we operated the second knees of the animals after the previously planned time (8 or 16 weeks, depending on the group).
2.2.2. Aftercare
2.2.3. Termination
- (a)
- We administered general anesthesia intramuscularly (dose calculated according to the animal’s body weight—ketamine—0.4 mg/kg, xylazine 0.5 mg/kg).
- (b)
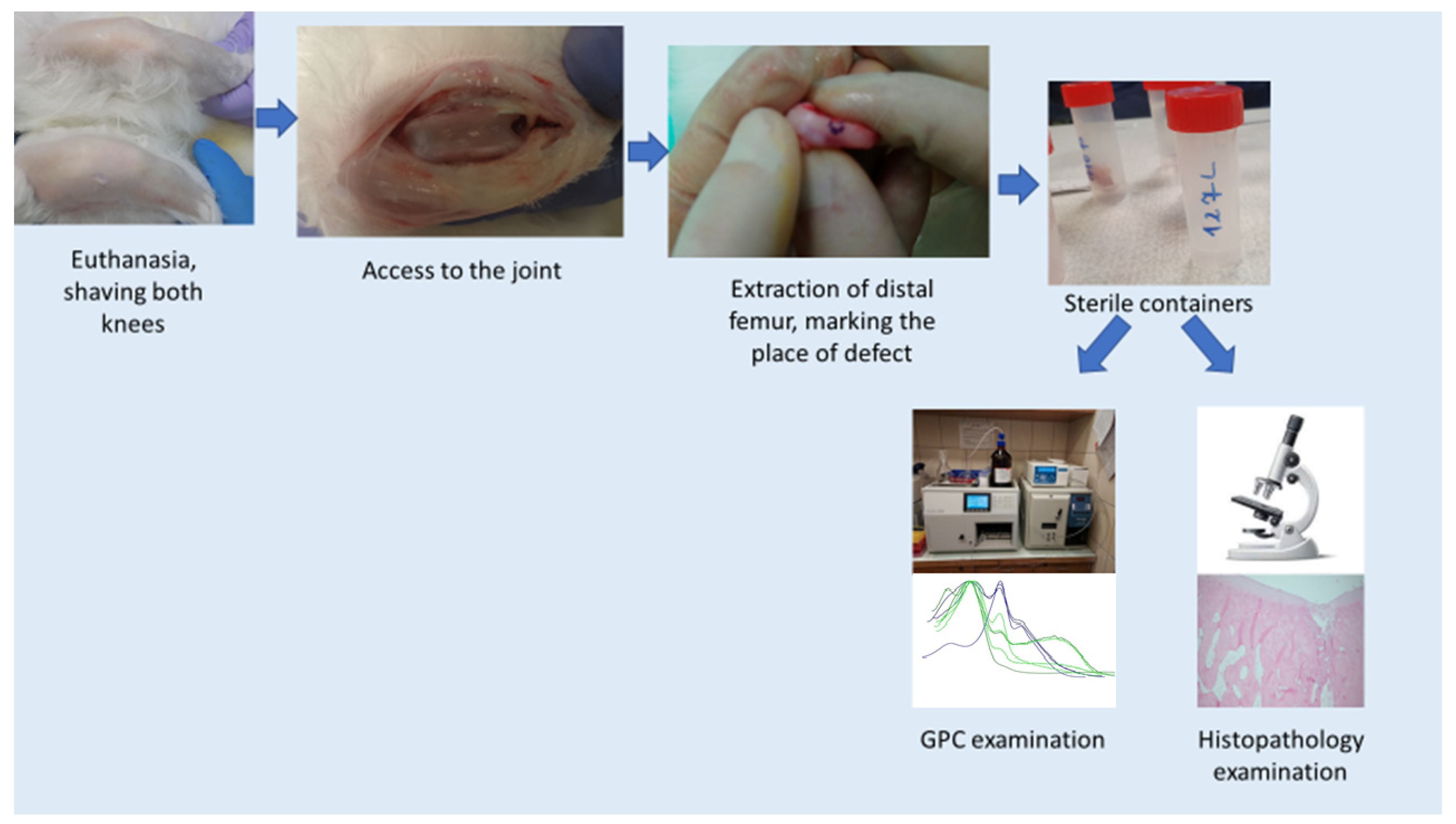
- Euthanasia by intravenous administration of Morbital.
- (c)
- We shaved the knee for surgery; disinfection of shaved areas.
- (d)
- Access to the knee joint (skin and deeper tissues were cut, as in the case of surgery). Extraction of the distal femur. Marked the place of defects/membrane insertion with ink. Cut the condyles from the rest of the bone and placed in a sterile transport container for further examination. Lateral condyle was taken to the histopathology examination, medial condyle to GPC.
2.2.4. Gel Permeation Chromatography (GPC)
- (a)
- Scraping and cutting only cavities from previously taken specimens;
- (b)
- Flushing in a physiological saline solution—flushing out physiological fluids;
- (c)
- Rinsing in hexane to extract fats;
- (d)
- Washing in CDCl3 (deuterated chloroform)—deproteinization;
- (e)
- Rinsing in methylene chloride—extraction of membranes (membrane residues);
- (f)
- Filter through a syringe filter with a PTFE membrane, with a porosity of 0.2 μm to get rid of bits of remaining cartilage (insoluble parts).
2.2.5. Histopathology
- (a)
- Collected condyles were immersed in 10% formalin.
- (b)
- Descaling—while waiting for the descaling, checks were made on the degree of descaling by trying to puncture the tissue with a needle every few weeks. After decalcification, the damaged areas were more visible.
- (c)
- The decalcified sections were dehydrated and embedded in paraffin (Paraplast sigma).
- (d)
- The material was cut into pieces with a thickness of 4 μm.
- (e)
- Paraffin sections were stained by the routine hematoxylin–eosin method.
- (f)
- The regenerates were evaluated (ICRS microscopic scoring system) under a light microscope by two trained and blinded observers. Each observer rated 1 regenerate 3 times at weekly intervals. The final score is the average of 3 measurements [60].
2.2.6. Statistics
3. Results
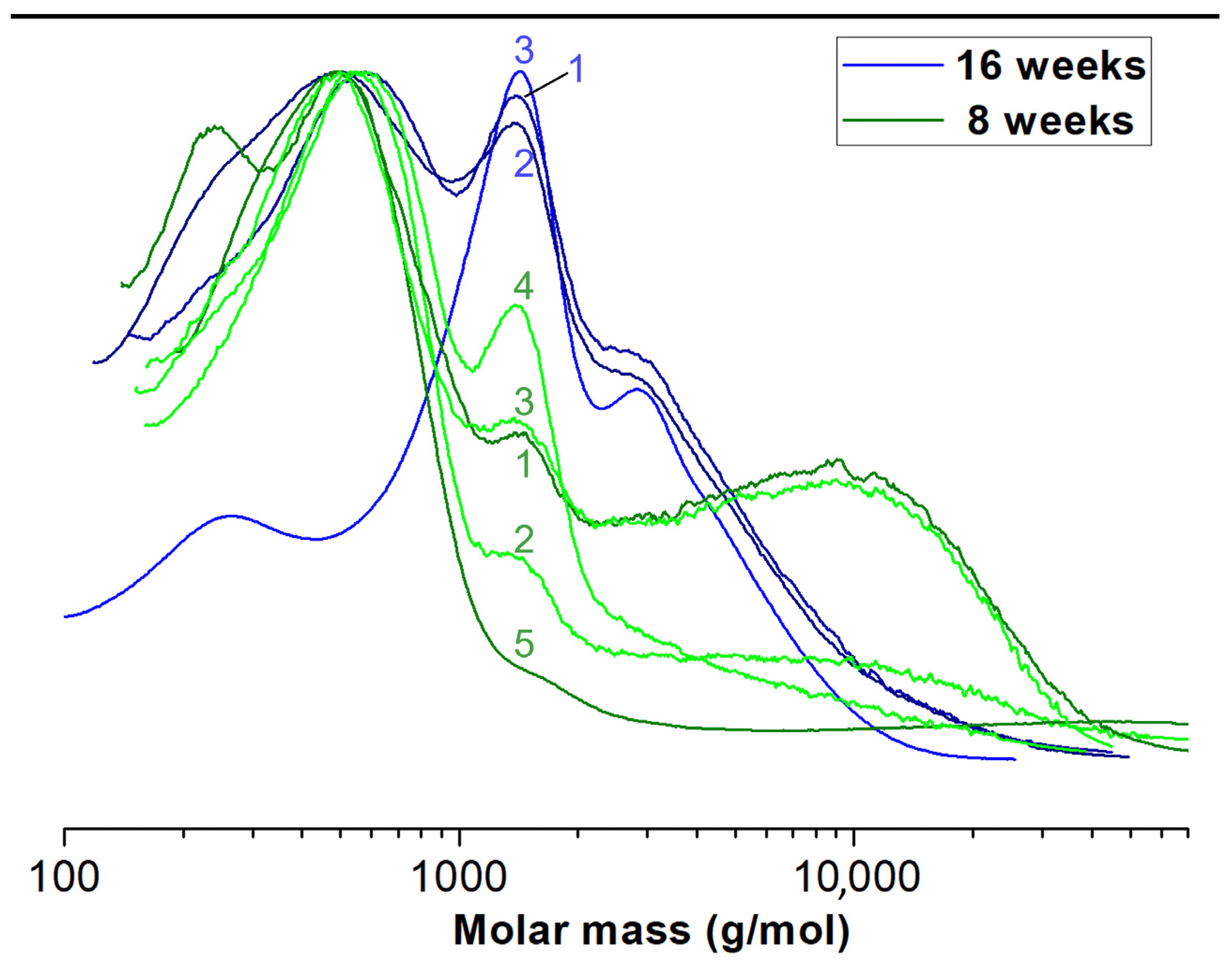
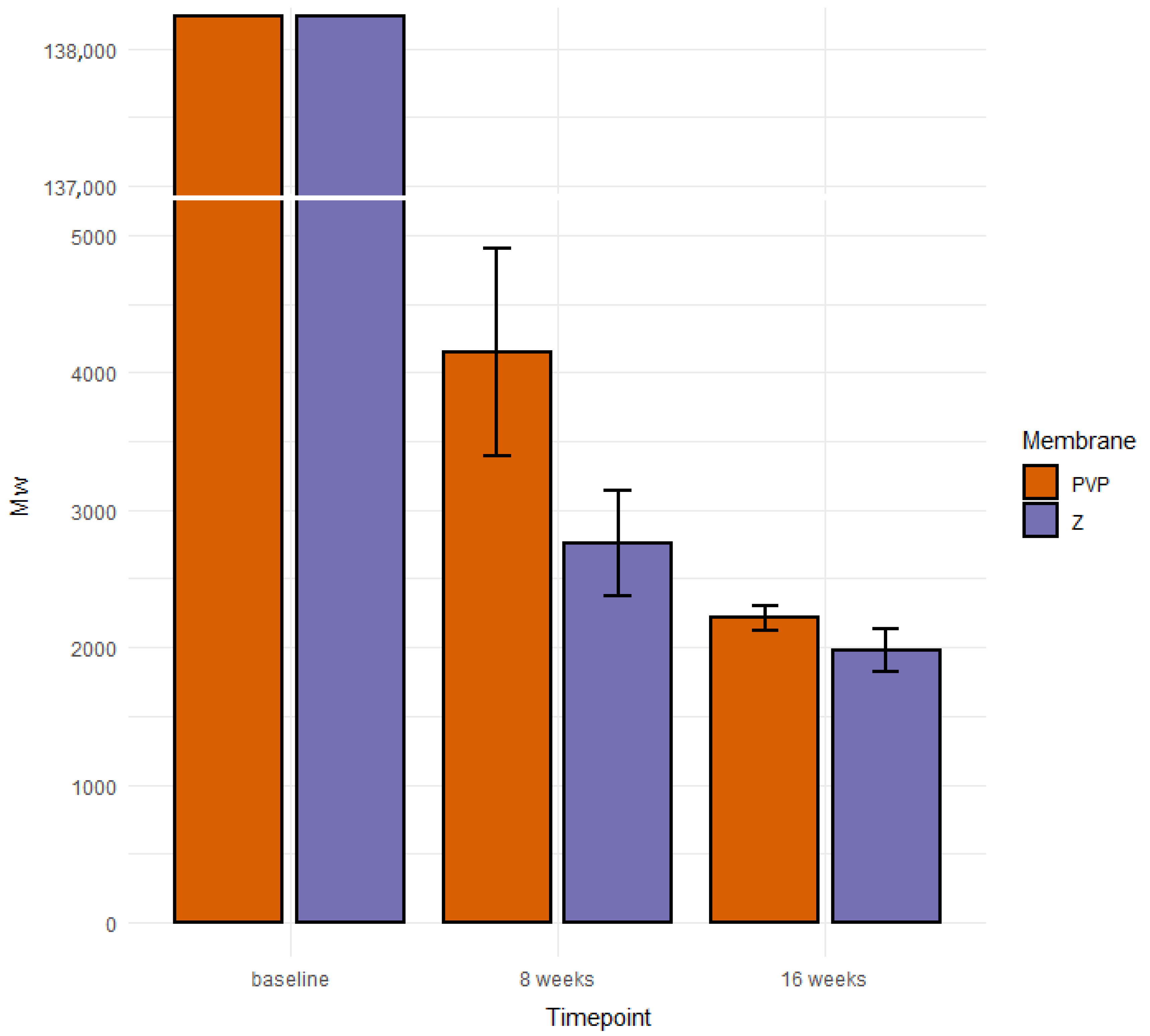
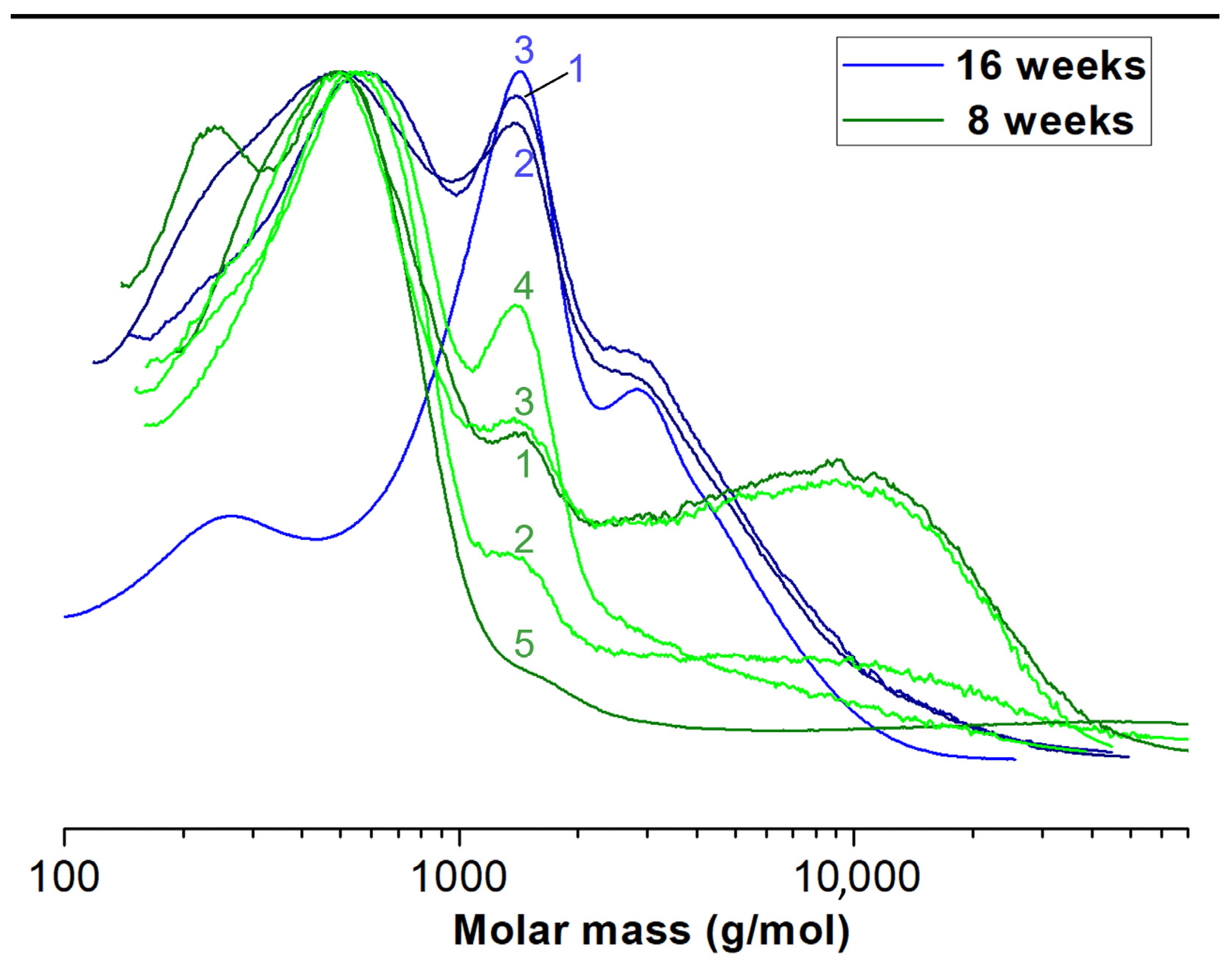
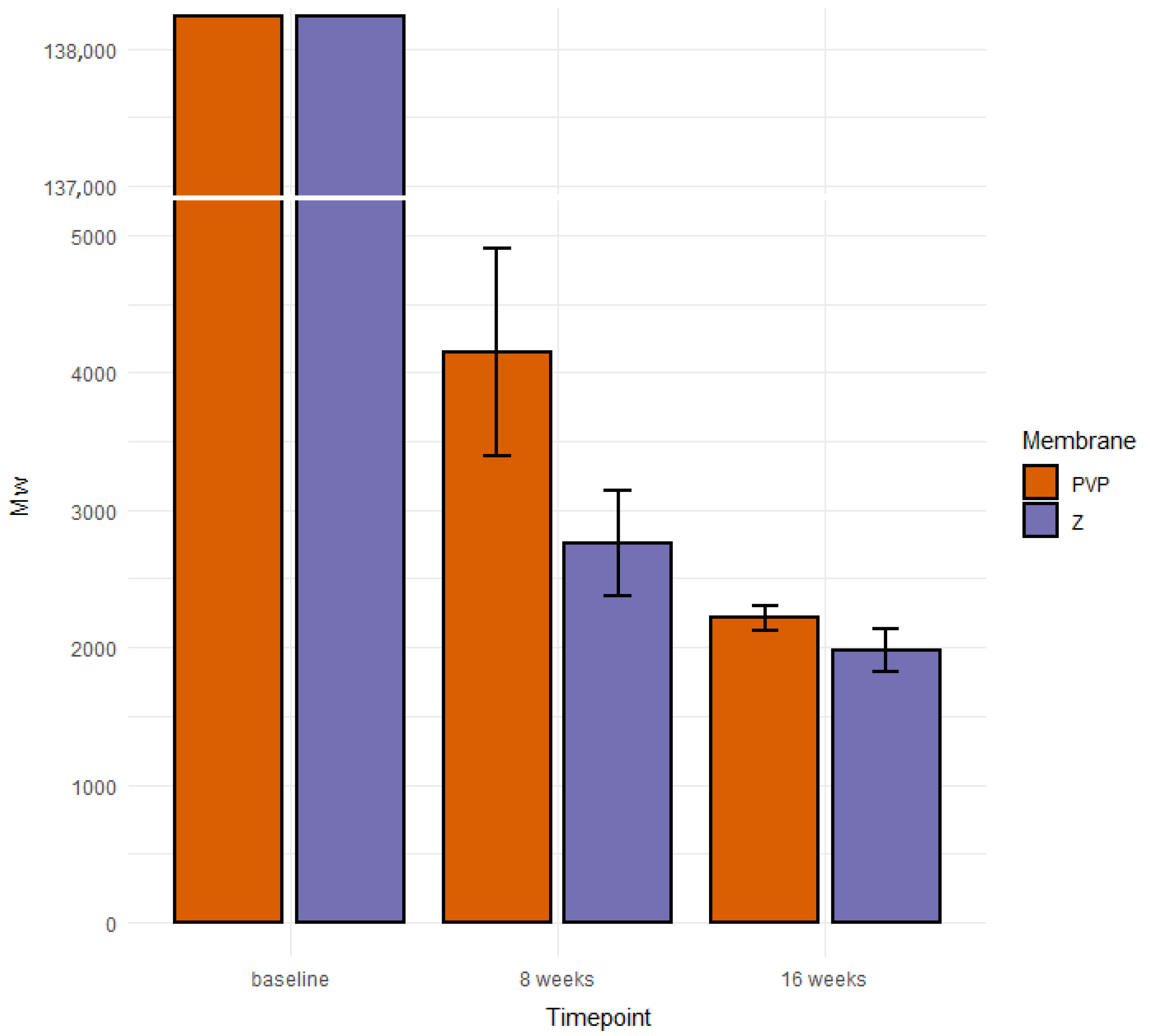
3.1. Destruction of PLCA Materials in Membranes Analyzed by Means of GPC
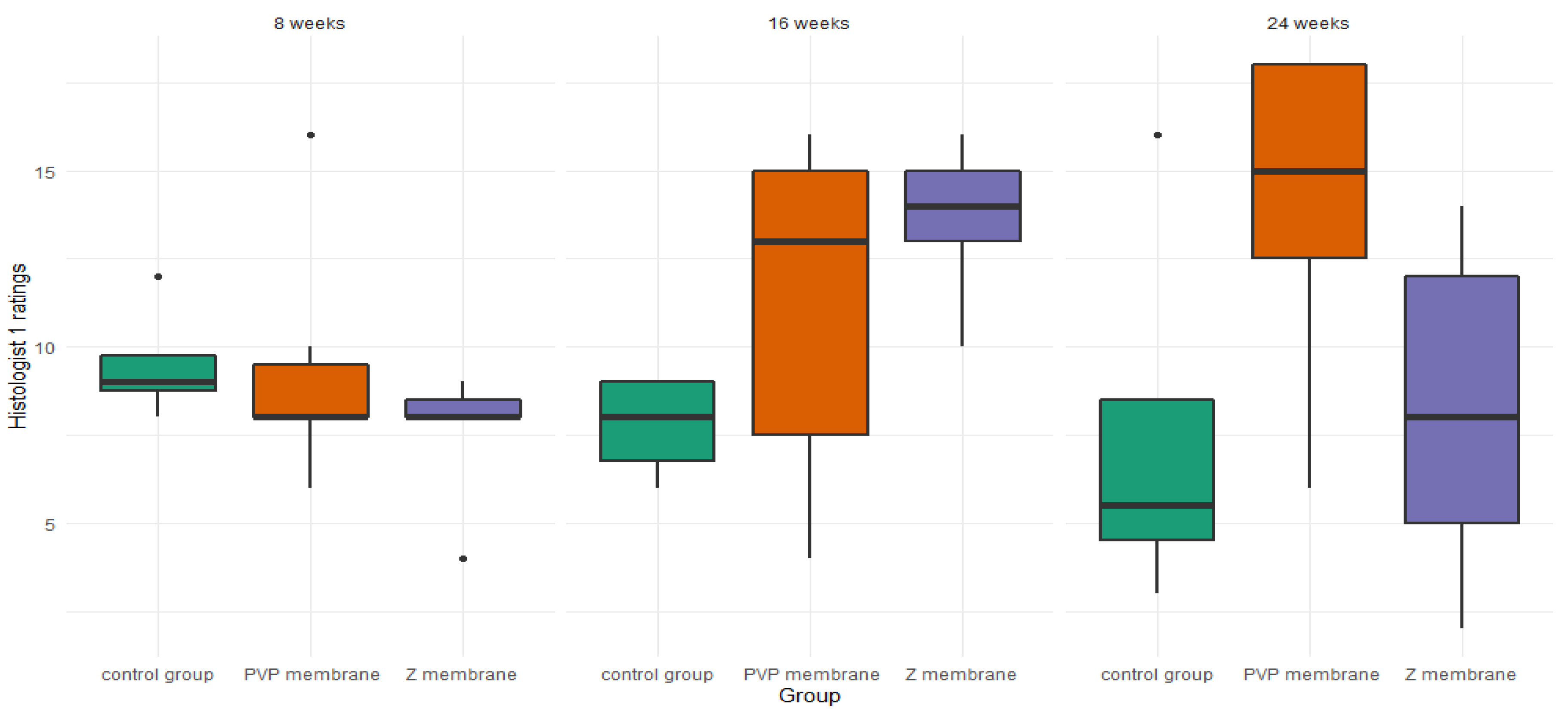
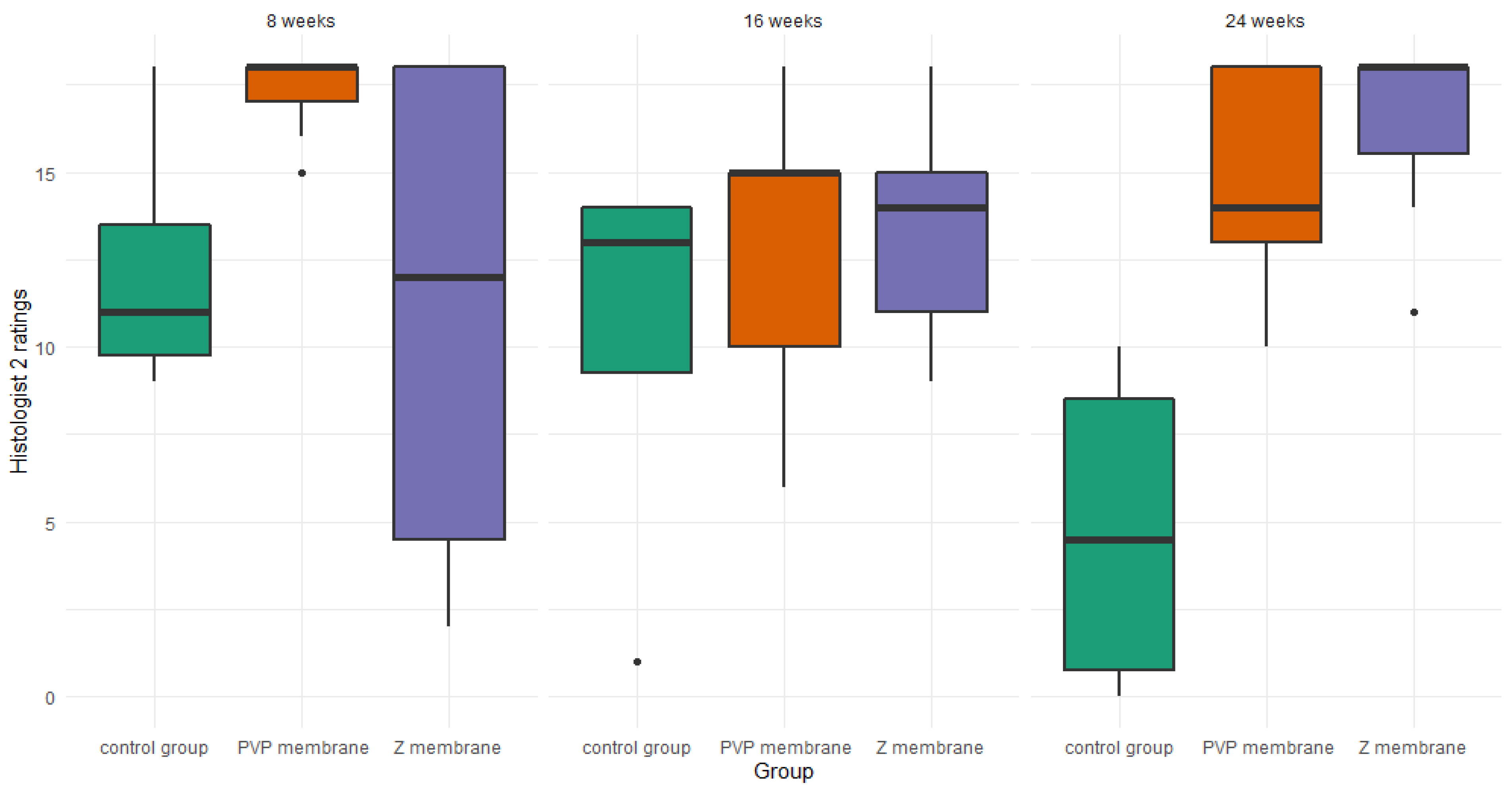
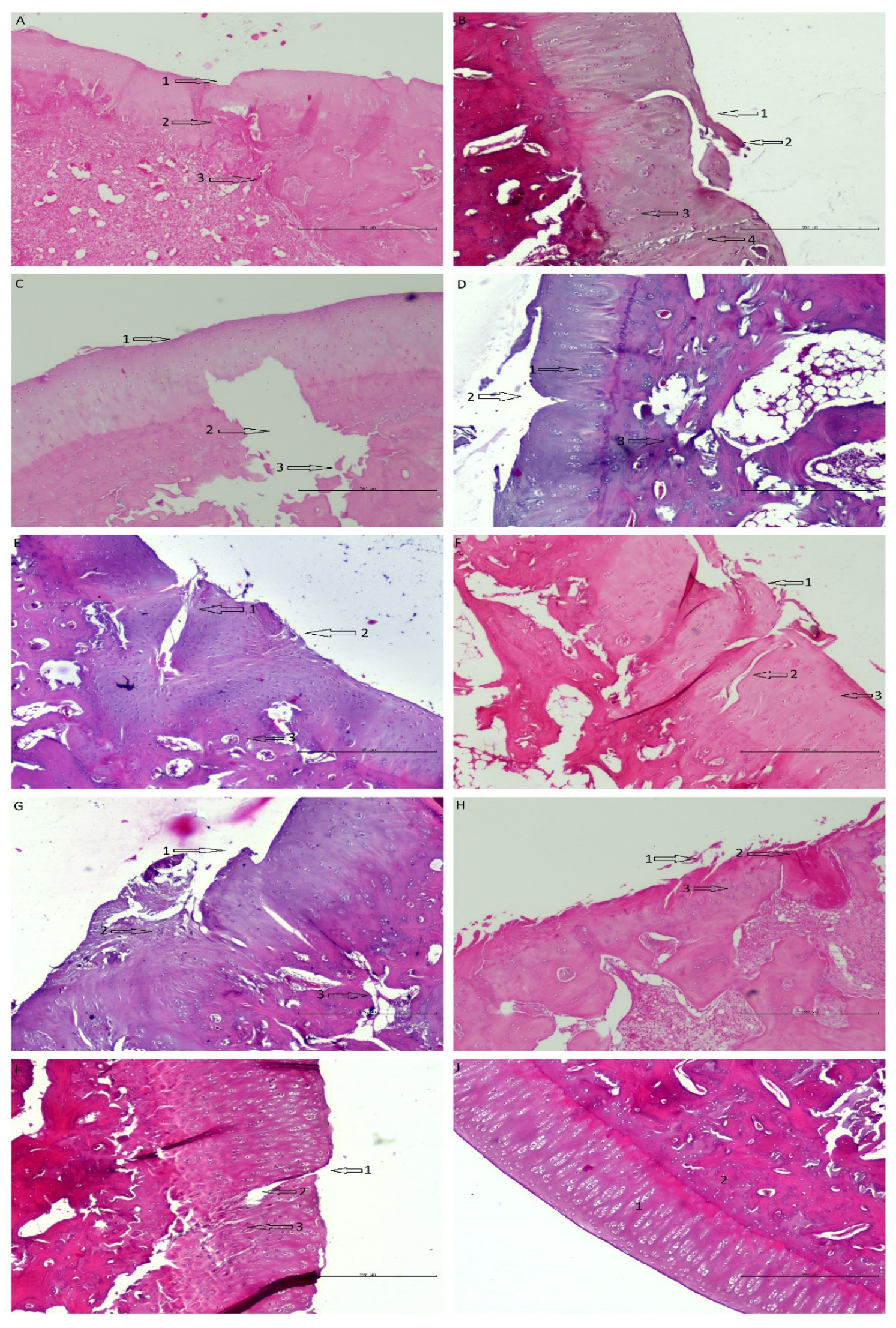
3.2. Histopathology
3.2.1. Differences in Membranes Performance
3.2.2. Histologist 1
3.2.3. Histologist 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chung, C.; Burdick, J.A. Engineering cartilage tissue. Adv. Drug Deliv. Rev. 2008, 60, 243–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sophia Fox, A.J.; Bedi, A.; Rodeo, S.A. The basic science of articular cartilage: Structure, composition, and function. Sports Health 2009, 1, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, Y.; Grodzinsky, A.J. Cartilage diseases. Matrix Biol. 2018, 71–72, 51–69. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Shen, J.; Zhao, W.; Wang, T.; Han, L.; Hamilton, J.L.; Im, H.J. Osteoarthritis: Toward a comprehensive understanding of pathological mechanism. Bone Res. 2017, 5, 16044. [Google Scholar] [CrossRef]
- Nauth, A.; McKee, M.D.; Einhorn, T.A.; Watson, J.T.; Li, R.; Schemitsch, E.H. Managing bone defects. J. Orthop. Trauma 2011, 25, 462–466. [Google Scholar] [CrossRef] [PubMed]
- Yeung, P.; Zhang, W.; Wang, X.N.; Yan, C.H.; Chan, B.P. A human osteoarthritis osteochondral organ culture model for cartilage tissue engineering. Biomaterials 2018, 162, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Merkely, G.; Ackermann, J.; Lattermann, C. Articular Cartilage Defects: Incidence, Diagnosis, and Natural History. Oper. Tech. Sports Med. 2018, 26, 156–161. [Google Scholar] [CrossRef]
- Silverwood, V.; Blagojevic-Bucknall, M.; Jinks, C.; Jordan, J.L.; Protheroe, J.; Jordan, K.P. Current evidence on risk factors for knee osteoarthritis in older adults: A systematic review and meta-analysis. Osteoarthr. Cartil. 2015, 23, 507–515. [Google Scholar] [CrossRef] [Green Version]
- Collins, A.T.; Kulvaranon, M.L.; Cutcliffe, H.C.; Utturkar, G.M.; Smith, W.A.R.; Spritzer, C.E.; Guilak, F.; Defrate, L.E. Obesity alters the in vivo mechanical response and biochemical properties of cartilage as measured by MRI. Arthritis Res. Ther. 2018, 20, 232. [Google Scholar] [CrossRef] [Green Version]
- Walter, S.G.; Ossendorff, R.; Schildberg, F.A. Articular cartilage regeneration and tissue engineering models: A systematic review. Arch. Orthop. Trauma Surg. 2019, 139, 305–316. [Google Scholar] [CrossRef]
- Dewan, A.K.; Gibson, M.A.; Elisseeff, J.H.; Trice, M.E. Evolution of autologous chondrocyte repair and comparison to other cartilage repair techniques. BioMed Res. Int. 2014, 2014, 272481. [Google Scholar] [CrossRef] [PubMed]
- Dzobo, K.; Thomford, N.E.; Senthebane, D.A.; Shipanga, H.; Rowe, A.; Dandara, C.; Pillay, M.; Motaung, K.S.C.M. Advances in regenerative medicine and tissue engineering: Innovation and transformation of medicine. Stem Cells Int. 2018, 2018, 2495848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medvedeva, E.V.; Grebenik, E.A.; Gornostaeva, S.N.; Telpuhov, V.I.; Lychagin, A.V.; Timashev, P.S.; Chagin, A.S. Repair of damaged articular cartilage: Current approaches and future directions. Int. J. Mol. Sci. 2018, 19, 2366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armiento, A.R.; Alini, M.; Stoddart, M.J. Articular fibrocartilage—Why does hyaline cartilage fail to repair? Adv. Drug Deliv. Rev. 2019, 146, 289–305. [Google Scholar] [CrossRef] [PubMed]
- Mirza, U.; Shubeena, S.; Shah, M.S.; Zaffer, B. Microfracture: A technique for repair of chondral defects. J. Entomol. Zool. Stud. 2018, 6, 1092–1097. [Google Scholar]
- Zhao, Z.; Fan, C.; Chen, F.; Sun, Y.; Xia, Y.; Ji, A.; Wang, D. Progress in Articular Cartilage Tissue Engineering: A Review on Therapeutic Cells and Macromolecular Scaffolds. Macromol. Biosci. 2019, 20, 1900278. [Google Scholar] [CrossRef]
- Płończak, M.; Czubak, J. Culture of Human Autologous Chondrocytes on Polysulphonic Membrane—Preliminary Studies. Biocybern. Biomed. Eng. 2012, 32, 63–67. [Google Scholar] [CrossRef]
- Kim, Y.S.; Mikos, A.G. Emerging strategies in reprogramming and enhancing the fate of mesenchymal stem cells for bone and cartilage tissue engineering. J. Control. Release 2021, 330, 565–574. [Google Scholar] [CrossRef]
- Knutsen, G.; Isaksen, V.; Johansen, O.; Engebretsen, L.; Ludvigsen, T.C.; Drogset, J.O.; Grøntvedt, T.; Solheim, E.; Strand, T.; Roberts, S. Autologous Chondrocyte Implantation Compared with Microfracture in the Knee: A Randomized Trial. J. Bone Jt. Surg.—Ser. A 2004, 86, 455–464. [Google Scholar] [CrossRef]
- Mastrolia, I.; Foppiani, E.M.; Murgia, A.; Candini, O.; Samarelli, A.V.; Grisendi, G.; Veronesi, E.; Horwitz, E.M.; Dominici, M. Challenges in Clinical Development of Mesenchymal Stromal/Stem Cells: Concise Review. Stem Cells Transl. Med. 2019, 8, 1135–1148. [Google Scholar] [CrossRef] [Green Version]
- Fahy, N.; Alini, M.; Stoddart, M.J. Mechanical stimulation of mesenchymal stem cells: Implications for cartilage tissue engineering. J. Orthop. Res. 2018, 36, 52–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grässel, S.; Lorenz, J. Tissue-Engineering Strategies to Repair Chondral and Osteochondral Tissue in Osteoarthritis: Use of Mesenchymal Stem Cells. Curr. Rheumatol. Rep. 2014, 16, 452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Zhou, G.; Cao, Y. Recent Progress in Cartilage Tissue Engineering—Our Experience and Future Directions. Engineering 2017, 3, 28–35. [Google Scholar] [CrossRef]
- Wasyłeczko, M.; Sikorska, W.; Chwojnowski, A. Review of synthetic and hybrid scaffolds in cartilage tissue engineering. Membranes 2020, 10, 348. [Google Scholar] [CrossRef] [PubMed]
- Wasyłeczko, M.; Sikorska, W.; Przytulska, M.; Dulnik, J.; Chwojnowski, A. Polyester membranes as 3D scaffolds for cell culture. Desalination Water Treat. 2021, 214, 181–193. [Google Scholar] [CrossRef]
- Kalkan, R.; Nwekwo, C.W.; Adali, T. The Use of Scaffolds in Cartilage Regeneration. Eukaryot. Gene Expr. 2018, 28, 343–348. [Google Scholar] [CrossRef]
- Eltom, A.; Zhong, G.; Muhammad, A. Scaffold Techniques and Designs in Tissue Engineering Functions and Purposes: A Review. Adv. Mater. Sci. Eng. 2019, 2019, 3429527. [Google Scholar] [CrossRef] [Green Version]
- Bironait, D. Scaffolds and cells for tissue regeneration: Different scaffold pore sizes—different cell effects. Cytotechnology 2015, 68, 355–369. [Google Scholar] [CrossRef] [Green Version]
- Pina, S.; Ribeiro, V.P.; Marques, C.F.; Maia, F.R.; Silva, T.H.; Reis, R.L.; Oliveira, J.M. Scaffolding Strategies for Tissue Engineering and Regenerative Medicine Applications. Materials 2019, 12, 1824. [Google Scholar] [CrossRef] [Green Version]
- Loh, Q.L.; Choong, C. Three-dimensional scaffolds for tissue engineering applications: Role of porosity and pore size. Tissue Eng.—Part B Rev. 2013, 19, 485–502. [Google Scholar] [CrossRef] [Green Version]
- Pompe, W.; Worch, H.; Epple, M.; Friess, W.; Gelinsky, M.; Greil, P.; Hempel, U.; Scharnweber, D.; Schulte, K. Functionally graded materials for biomedical applications. Mater. Sci. Eng. A 2003, 362, 40–60. [Google Scholar] [CrossRef]
- Smidsrød, O. Molecular basis for some physical properties of alginates in the gel state. Faraday Discuss. Chem. Soc. 1974, 57, 263. [Google Scholar] [CrossRef]
- Bretcanu, O.; Samaille, C.; Boccaccini, A.R. Simple methods to fabricate Bioglass®-derived glass-ceramic scaffolds exhibiting porosity gradient. J. Mater. Sci. 2008, 43, 4127–4134. [Google Scholar] [CrossRef]
- Van Tienen, T.G.; Heijkants, R.G.J.C.; Buma, P.; De Groot, J.H.; Pennings, A.J.; Veth, R.P.H. Tissue ingrowth and degradation of two biodegradable porous polymers with different porosities and pore sizes. Biomaterials 2002, 23, 1731–1738. [Google Scholar] [CrossRef]
- Harley, B.A.; Hastings, A.Z.; Yannas, I.V.; Sannino, A. Fabricating tubular scaffolds with a radial pore size gradient by a spinning technique. Biomaterials 2006, 27, 866–874. [Google Scholar] [CrossRef]
- Okubo, R.; Asawa, Y.; Watanabe, M.; Nagata, S.; Nio, M. Proliferation medium in three-dimensional culture of auricular chondrocytes promotes effective cartilage regeneration in vivo. Regen. Ther. 2019, 11, 306–315. [Google Scholar] [CrossRef]
- Armiento, A.R.; Stoddart, M.J.; Alini, M.; Eglin, D. Biomaterials for articular cartilage tissue engineering: Learning from biology. Acta Biomater. 2018, 65, 1–20. [Google Scholar] [CrossRef]
- Zhao, P.; Gu, H.; Mi, H.; Rao, C.; Fu, J.; Turng, L. sheng Fabrication of scaffolds in tissue engineering: A review. Front. Mech. Eng. 2018, 13, 107–119. [Google Scholar] [CrossRef]
- Koh, Y.G.; Lee, J.A.; Kim, Y.S.; Lee, H.Y.; Kim, H.J.; Kang, K.T. Optimal mechanical properties of a scaffold for cartilage regeneration using finite element analysis. J. Tissue Eng. 2019, 10, 2041731419832133. [Google Scholar] [CrossRef] [Green Version]
- Bistolfi, A.; Ferracini, R.; Galletta, C.; Tosto, F.; Sgarminato, V.; Digo, E.; Vernè, E.; Massè, A. Regeneration of articular cartilage: Scaffold used in orthopedic surgery. A short handbook of available products for regenerative joints surgery. Clin. Sci. Res. Rep. 2017, 1, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Ye, H.; Zhang, K.; Kai, D.; Li, Z.; Loh, X.J. Polyester elastomers for soft tissue engineering. Chem. Soc. Rev. 2018, 47, 4545–4580. [Google Scholar] [CrossRef] [PubMed]
- Urbánek, T.; Jäger, E.; Jäger, A.; Hrubý, M. Selectively biodegradable polyesters: Nature-inspired construction materials for future biomedical applications. Polymers 2019, 11, 1061. [Google Scholar] [CrossRef] [Green Version]
- Jiang, L.; Xu, L.; Ma, B.; Ding, H.; Tang, C. Effect of component and surface structure on poly (L -lactide-co- ε—caprolactone) (PLCA) -based composite membrane. Compos. Part B 2019, 174, 107031. [Google Scholar] [CrossRef]
- Nikolova, M.P.; Chavali, M.S. Recent advances in biomaterials for 3D scaffolds: A review. Bioact. Mater. 2019, 4, 271–292. [Google Scholar] [CrossRef] [PubMed]
- Janmohammadi, M.; Nourbakhsh, M.S. International Journal of Polymeric Materials and Electrospun polycaprolactone scaffolds for tissue engineering: A review. Int. J. Polym. Mater. Polym. Biomater. 2018, 68, 527–539. [Google Scholar] [CrossRef]
- Laurent, P. Suitability of a PLCL fibrous scaffold for soft tissue engineering applications: A combined biological and mechanical characterisation. J. Biomater. Appl. 2018, 32, 1276–1288. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.; Kaduri, M.; Poley, M.; Adir, O.; Krinsky, N.; Shainsky-roitman, J.; Schroeder, A. Mini Review Biocompatibility, biodegradation and excretion of polylactic acid (PLA) in medical implants and theranostic systems. Chem. Eng. J. 2018, 340, 9–14. [Google Scholar] [CrossRef]
- Garkhal, K.; Verma, S.; Jonnalagadda, S.; Kumar, N. Fast degradable poly(L-lactide-co-ε-caprolactone) microspheres for tissue engineering: Synthesis, characterization, and degradation behavior. J. Polym. Sci. Part A Polym. Chem. 2007, 45, 2755–2764. [Google Scholar] [CrossRef]
- Herrera-Kao, W.A.; Loría-Bastarrachea, M.I.; Pérez-Padilla, Y.; Cauich-Rodríguez, J.V.; Vázquez-Torres, H.; Cervantes-Uc, J.M. Thermal degradation of poly(caprolactone), poly(lactic acid), and poly(hydroxybutyrate) studied by TGA/FTIR and other analytical techniques. Polym. Bull. 2018, 75, 4191–4205. [Google Scholar] [CrossRef]
- Tomihata, K.; Suzuki, M.; Tomita, N. Handling characteristics of poly(L-lactide-co-ε-caprolactone) monofilament suture. Bio-Med. Mater. Eng. 2005, 15, 381–391. [Google Scholar]
- Jung, Y.; Park, M.S.; Lee, J.W.; Kim, Y.H.; Kim, S.H.; Kim, S.H. Cartilage regeneration with highly-elastic three-dimensional scaffolds prepared from biodegradable poly(l-lactide-co-ε-caprolactone). Biomaterials 2008, 29, 4630–4636. [Google Scholar] [CrossRef] [PubMed]
- Morokov, E.S.; Demina, V.A.; Sedush, N.G.; Kalinin, K.T.; Khramtsova, E.A.; Dmitryakov, P.V.; Bakirov, A.V.; Grigoriev, T.E.; Levin, V.M.; Chvalun, S.N. Noninvasive high-frequency acoustic microscopy for 3D visualization of microstructure and estimation of elastic properties during hydrolytic degradation of lactide and ε-caprolactone polymers. Acta Biomater. 2020, 109, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Sikorska, W.; Wasyłeczko, M.; Przytulska, M.; Wojciechowski, C.; Rokicki, G.; Chwojnowski, A. Chemical degradation of PSF-PUR blend hollow fiber membranes-assessment of changes in properties and morphology after hydrolysis. Membranes 2021, 11, 51. [Google Scholar] [CrossRef] [PubMed]
- Chwojnowski, A.; Kruk, A.; Wojciechowski, C. The dependence of the membrane structure on the non-woven forming the macropores in the 3D scaffolds preparation. Desalination Water Treat. 2017, 64, 11394. [Google Scholar] [CrossRef]
- Dutta, R.C.; Dey, M.; Dutta, A.K.; Basu, B. Competent processing techniques for scaffolds in tissue engineering. Biotechnol. Adv. 2017, 35, 240–250. [Google Scholar] [CrossRef]
- Prasad, A.; Sankar, M.R.; Katiyar, V. State of Art on Solvent Casting Particulate Leaching Method for Orthopedic ScaffoldsFabrication. Mater. Today Proc. 2017, 4, 898–907. [Google Scholar] [CrossRef]
- Plisko, T.V.; Penkova, A.V.; Burts, K.S.; Bildyukevich, A.V.; Dmitrenko, M.E.; Melnikova, G.B.; Atta, R.R.; Mazur, A.S.; Zolotarev, A.A.; Missyul, A.B. Effect of Pluronic F127 on porous and dense membrane structure formation via non-solvent induced and evaporation induced phase separation. J. Membr. Sci. 2019, 580, 336–349. [Google Scholar] [CrossRef]
- Caplan, N.; Kader, D.F. The Etiology of Chondromalacia Patellae; Classic Papers in Orthopaedics; Springer: London, UK, 2014; pp. 185–187. [Google Scholar] [CrossRef]
- Hurtig, M.B.; Buschmann, M.D.; Fortier, L.A.; Hoemann, C.D.; Hunziker, E.B.; Jurvelin, J.S.; Mainil-Varlet, P.; McIlwraith, C.W.; Sah, R.L.; Whiteside, R.A. Preclinical studies for cartilage repair: Recommendations from the international cartilage repair society. Cartilage 2011, 2, 137–152. [Google Scholar] [CrossRef] [Green Version]
- Rutgers, M.; van Pelt, M.J.P.; Dhert, W.J.A.; Creemers, L.B.; Saris, D.B.F. Evaluation of histological scoring systems for tissue-engineered, repaired and osteoarthritic cartilage. Osteoarthr. Cartil. 2010, 18, 12–23. [Google Scholar] [CrossRef] [Green Version]
- Oksanen, A.J.; Blanchet, F.G.; Friendly, M.; Kindt, R.; Legendre, P.; Mcglinn, D.; Minchin, P.R.; Hara, R.B.O.; Simpson, G.L.; Solymos, P.; et al. Vegan. In Encyclopedia of Food and Agricultural Ethics; Springer: Dordrecht, Germany, 2019; pp. 2395–2396. [Google Scholar] [CrossRef]
- Hothorn, T.; Van De Wiel, M.A.; Hornik, K.; Zeileis, A. Implementing a class of permutation tests: The coin package. J. Stat. Softw. 2008, 28, 1–23. [Google Scholar] [CrossRef]
- Ogle, D.H.; Doll, J.C.; Wheeler, P.; Dinno, A. FSA: Fisheries Stock Analysis. R Package Version 0.9.1. Available online: https://github.com/fishR-Core-Team/FSA (accessed on 1 July 2021).
- Kemp, A.W.; Manly, B.F.J. Randomization, Bootstrap and Monte Carlo Methods in Biology. Biometrics 1997, 53, 1560. [Google Scholar] [CrossRef]
- Legendre, P. Species associations: The Kendall coefficient of concordance revisited. J. Agric. Biol. Environ. Stat. 2005, 10, 226–245. [Google Scholar] [CrossRef]
- Panadero, J.A.; Lanceros-Mendez, S.; Ribelles, J.L.G. Differentiation of mesenchymal stem cells for cartilage tissue engineering: Individual and synergetic effects of three-dimensional environment and mechanical loading. Acta Biomater. 2016, 33, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Tan, K.; Zhou, Y.; Ye, Z.; Tan, W.S. A combinatorial variation in surface chemistry and pore size of three-dimensional porous poly(ε-caprolactone) scaffolds modulates the behaviors of mesenchymal stem cells. Mater. Sci. Eng. C 2016, 59, 193–202. [Google Scholar] [CrossRef]
- Matsiko, A.; Gleeson, J.P.; O’Brien, F.J. Scaffold mean pore size influences mesenchymal stem cell chondrogenic differentiation and matrix deposition. Tissue Eng.—Part A 2015, 21, 486–497. [Google Scholar] [CrossRef]
- Jeong, S.I.; Kim, B.; Lee, Y.M.; Ihn, K.J.; Kim, S.H. Morphology of Elastic Poly (L -lactide-co- E -caprolactone) Copolymers and in Vitro and in Vivo Degradation Behavior of Their Scaffolds. Biomacromolecules 2004, 5, 1303–1309. [Google Scholar] [CrossRef]
- In, S.; Kim, B.; Woong, S.; Hyun, J.; Moo, Y.; Hyun, S.; Ha, Y. In vivo biocompatibilty and degradation behavior of elastic poly (l -lactide- co—e -caprolactone) scaffolds. Biomaterials 2004, 25, 5939–5946. [Google Scholar] [CrossRef]
- Ota, Y.; Kamei, N.; Tamaura, T.; Adachi, N.; Ochi, M. Magnetic resonance imaging evaluation of cartilage repair and iron particle kinetics after magnetic delivery of stem cells. Tissue Eng.—Part C Methods 2018, 24, 679–687. [Google Scholar] [CrossRef]
- Koller, U.; Apprich, S.; Schmitt, B.; Windhager, R.; Trattnig, S. Evaluating the cartilage adjacent to the site of repair surgery with glycosaminoglycan-specific magnetic resonance imaging. Int. Orthop. 2017, 41, 969–974. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Kind of Membrane | Time of Implantation (Weeks) | Sample Nr | Mean Mw |
|---|---|---|---|
| PVP | 8 | 1 | 5155 |
| PVP | 8 | 2 | 4816 |
| PVP | 8 | 3 | 4737 |
| PVP | 8 | 4 | 1896 |
| PVP 1 | 8 | 5 | 24,238 |
| PVP | 16 | 1 | 2387 |
| PVP | 16 | 2 | 2176 |
| PVP | 16 | 3 | 2088 |
| Z | 8 | 1 | 3678 |
| Z | 8 | 2 | 3167 |
| Z | 8 | 3 | 3022 |
| Z | 8 | 4 | 2490 |
| Z | 8 | 5 | 1432 |
| Z | 16 | 1 | 2139 |
| Z | 16 | 2 | 2127 |
| Z | 16 | 3 | 1663 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baranowski, M.; Wasyłeczko, M.; Kosowska, A.; Plichta, A.; Kowalczyk, S.; Chwojnowski, A.; Bielecki, W.; Czubak, J. Regeneration of Articular Cartilage Using Membranes of Polyester Scaffolds in a Rabbit Model. Pharmaceutics 2022, 14, 1016. https://doi.org/10.3390/pharmaceutics14051016
Baranowski M, Wasyłeczko M, Kosowska A, Plichta A, Kowalczyk S, Chwojnowski A, Bielecki W, Czubak J. Regeneration of Articular Cartilage Using Membranes of Polyester Scaffolds in a Rabbit Model. Pharmaceutics. 2022; 14(5):1016. https://doi.org/10.3390/pharmaceutics14051016
Chicago/Turabian StyleBaranowski, Maciej, Monika Wasyłeczko, Anna Kosowska, Andrzej Plichta, Sebastian Kowalczyk, Andrzej Chwojnowski, Wojciech Bielecki, and Jarosław Czubak. 2022. "Regeneration of Articular Cartilage Using Membranes of Polyester Scaffolds in a Rabbit Model" Pharmaceutics 14, no. 5: 1016. https://doi.org/10.3390/pharmaceutics14051016
APA StyleBaranowski, M., Wasyłeczko, M., Kosowska, A., Plichta, A., Kowalczyk, S., Chwojnowski, A., Bielecki, W., & Czubak, J. (2022). Regeneration of Articular Cartilage Using Membranes of Polyester Scaffolds in a Rabbit Model. Pharmaceutics, 14(5), 1016. https://doi.org/10.3390/pharmaceutics14051016