
Preclinical Evaluation of the Safety and Immunological Action of Allogeneic ADSC-Collagen Scaffolds in the Treatment of Chronic Ischemic Cardiomyopathy

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Characterization of ADSCs and Production of Cellularized Collagen Scaffolds
2.2. Rat and Minipig MI Models
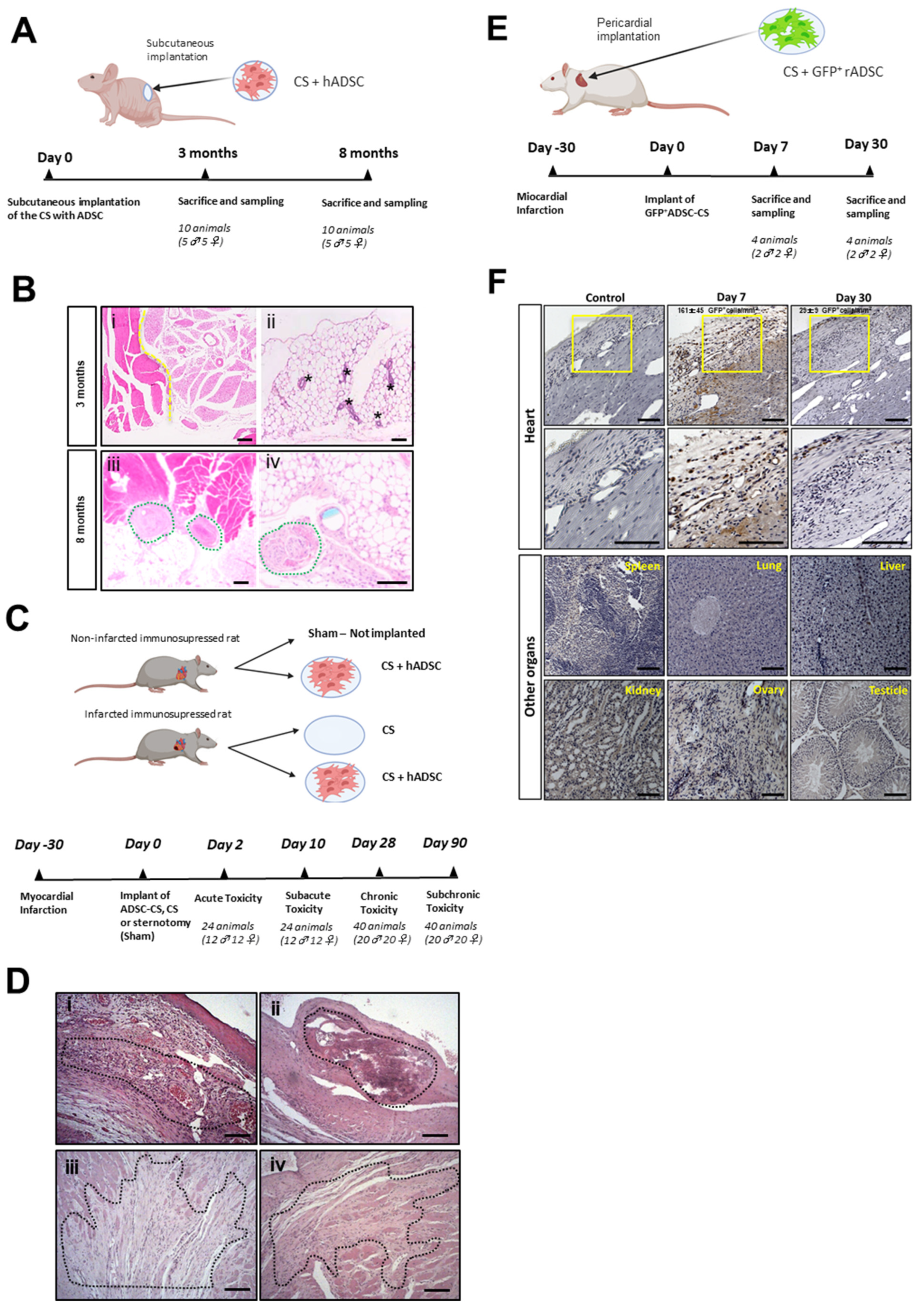
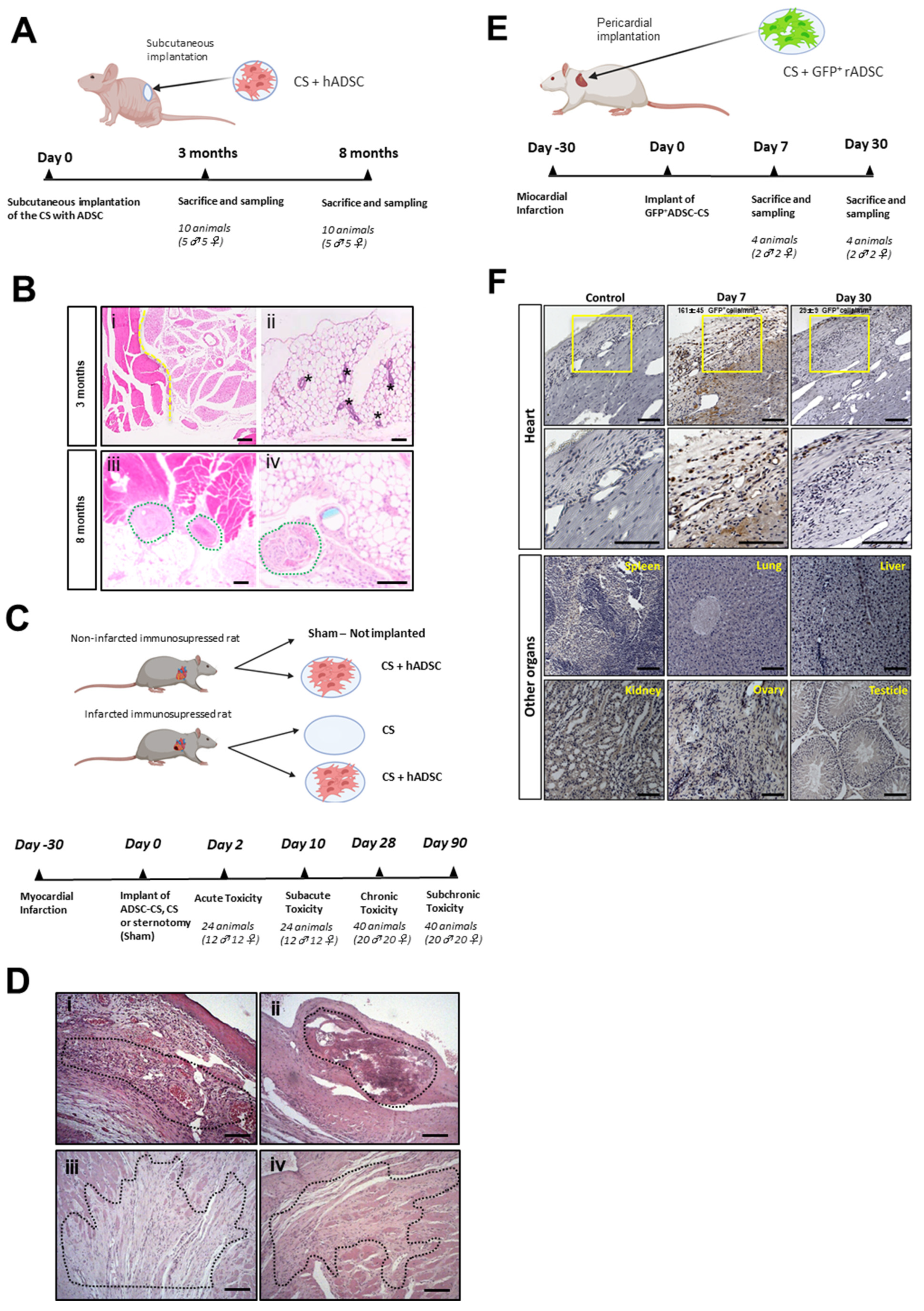
2.3. ADSC-CS Safety Assessment in Rodent Models
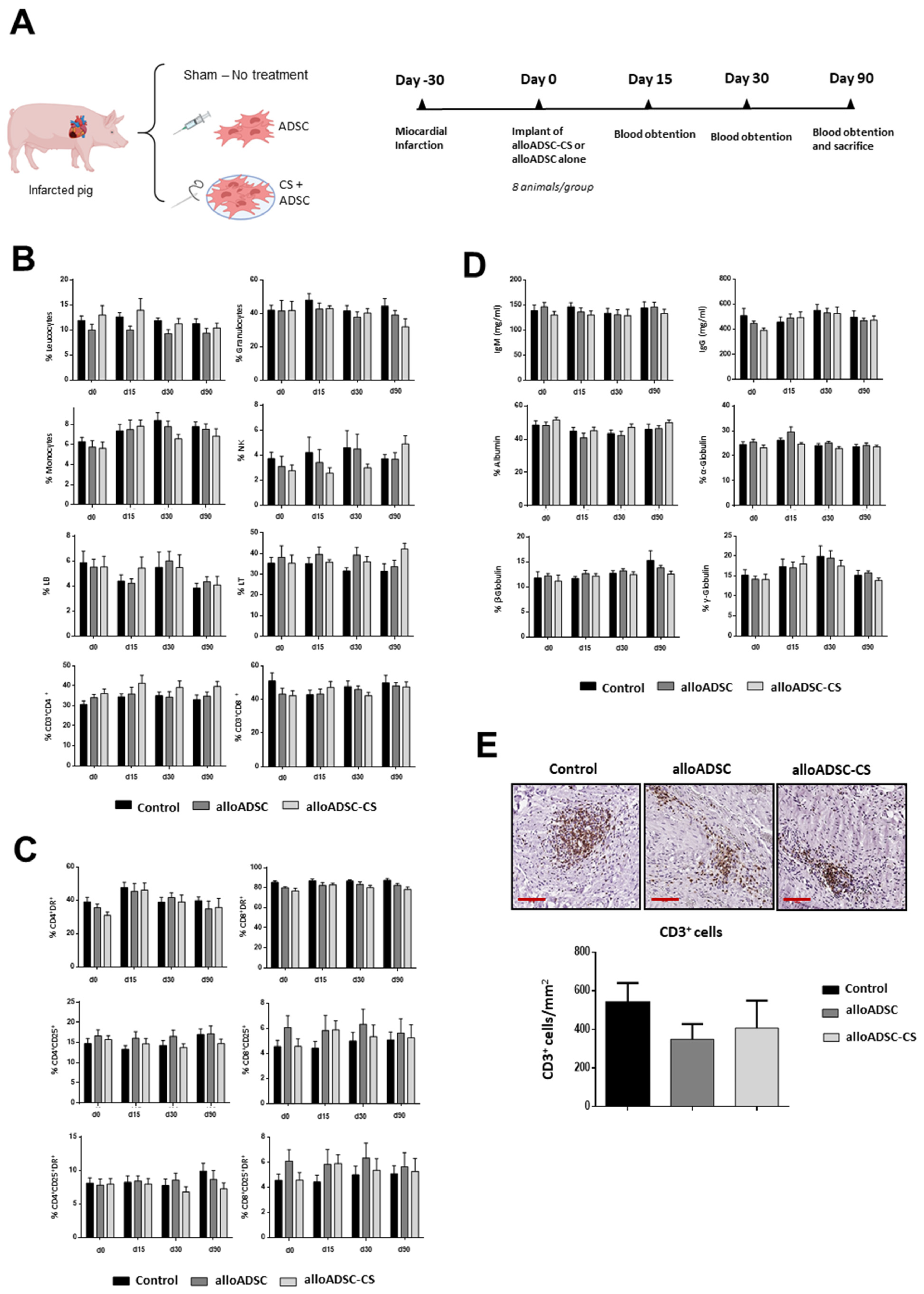
2.4. Implantation of alloADSC-CS in a Preclinical Porcine Model of MI
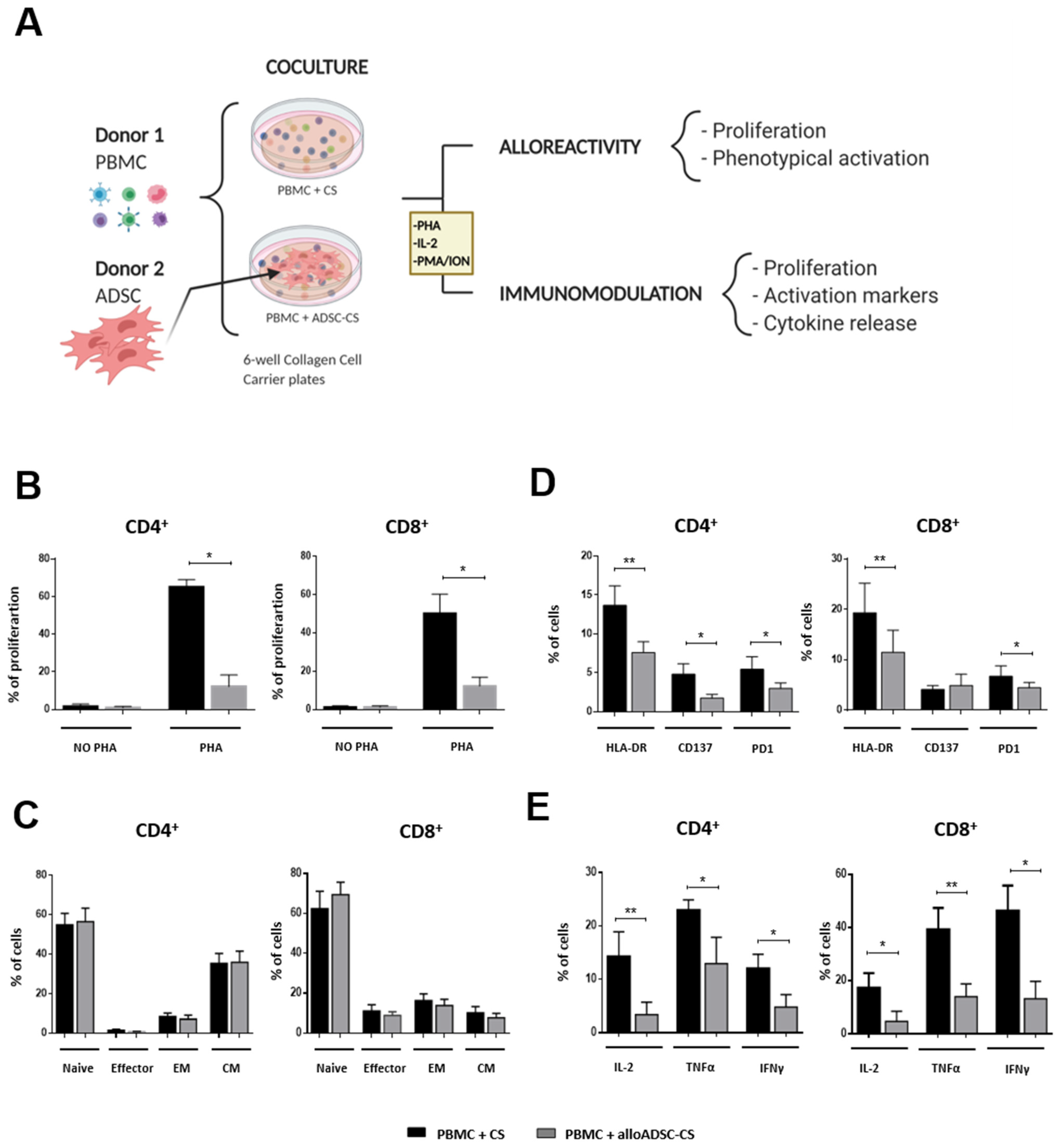
2.5. In Vitro Coculture of alloADSC-CS and PBMCs
3. Results
3.1. Safety Assessment of ADSC-CS
3.2. Inflammatory and Immunomodulatory Action of Allogeneic Pig ADSC-CS
3.3. In Vitro Assessment of Human ADSC-CS Immunomodulatory Action
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Timmis, A.; Townsend, N.; Gale, C.P.; Torbica, A.; Lettino, M.; Petersen, S.E.; Mossialos, E.A.; Maggioni, A.P.; Kazakiewicz, D.; May, H.T.; et al. European society of cardiology: Cardiovascular disease statistics. Eur. Heart J. 2020, 41, 12–85. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Yu, Y.; Hu, S.; Chen, Y.; Shen, Z. The therapeutic potential of mesenchymal stem cells for cardiovascular diseases. Cell Death Dis. 2020, 11, 349. [Google Scholar] [CrossRef]
- Mathiasen, A.B.; Qayyum, A.A.; Jørgensen, E.; Helqvist, S.; Kofoed, K.F.; Haack-Sørensen, M.; Ekblond, A.; Kastrup, J. Bone marrow-derived mesenchymal stromal cell treatment in patients with ischaemic heart failure: Final 4-year follow-up of the MSC-HF trial. Eur. J. Heart Fail. 2020, 22, 884–892. [Google Scholar] [CrossRef] [PubMed]
- Guijarro, D.; Lebrin, M.; Lairez, O.; Bourin, P.; Piriou, N.; Pozzo, J.; Lande, G.; Berry, M.; Le Tourneau, T.; Cussac, D.; et al. Intramyocardial transplantation of mesenchymal stromal cells for chronic myocardial ischemia and impaired left ventricular function: Results of the MESAMI 1 pilot trial. Int. J. Cardiol. 2016, 209, 258–265. [Google Scholar] [CrossRef] [Green Version]
- Henry, T.D.; Pepine, C.; Lambert, C.R.; Traverse, J.H.; Schatz, R.; Costa, M.; Povsic, T.J.; Anderson, R.D.; Willerson, J.T.; Kesten, S.; et al. The Athena trials: Autologous adipose-derived regenerative cells for refractory chronic myocardial ischemia with left ventricular dysfunction. Catheter. Cardiovasc. Interv. 2017, 89, 169–177. [Google Scholar] [CrossRef]
- Razeghian-Jahromi, I.; Matta, A.G.; Canitrot, R.; Zibaeenezhad, M.J.; Razmkhah, M.; Safari, A.; Nader, V.; Roncalli, J. Surfing the clinical trials of mesenchymal stem cell therapy in ischemic cardiomyopathy. Stem Cell Res. Ther. 2021, 12, 361. [Google Scholar] [CrossRef]
- Perez-Estenaga, I.; Prosper, F.; Pelacho, B. Allogeneic Mesenchymal Stem Cells and Biomaterials: The Perfect Match for Cardiac Repair? Int. J. Mol. Sci. 2018, 19, 3236. [Google Scholar] [CrossRef] [Green Version]
- Wu, W.Q.; Peng, S.; Song, Z.Y.; Lin, S. Collagen biomaterial for the treatment of myocardial infarction: An update on cardiac tissue engineering and myocardial regeneration. Drug Deliv. Transl. Res. 2019, 9, 920–934. [Google Scholar] [CrossRef]
- Wang, Q.; He, X.; Wang, B.; Pan, J.; Shi, C.; Li, J.; Wang, L.; Zhao, Y.; Dai, J.; Wang, D. Injectable collagen scaffold promotes swine myocardial infarction recovery by long-term local retention of transplanted human umbilical cord mesenchymal stem cells. Sci. China Life Sci. 2021, 64, 269–281. [Google Scholar] [CrossRef]
- Araña, M.; Gavira, J.J.; Peña, E.; Gonzalez, A.; Abizanda, G.; Cilla, M.; Pérez, M.M.; Albiasu, E.; Aguado, N.; Casado, M.; et al. Epicardial delivery of collagen patches with adipose-derived stem cells in rat and minipig models of chronic myocardial infarction. Biomaterials 2014, 35, 143–151. [Google Scholar] [CrossRef]
- Muñoz, M.F.; Argüelles, S.; Marotta, F.; Barbagallo, M.; Cano, M.; Ayala, A. Effect of Age and Lipoperoxidation in Rat and Human Adipose Tissue-Derived Stem Cells. Oxidative Med. Cell. Longev. 2020, 2020, 1–20. [Google Scholar] [CrossRef]
- Kot, M.; Baj-Krzyworzeka, M.; Szatanek, R.; Musiał-Wysocka, A.; Suda-Szczurek, M.; Majka, M. The Importance of HLA Assessment in “Off-the-Shelf” Allogeneic Mesenchymal Stem Cells Based-Therapies. Int. J. Mol. Sci. 2019, 20, 5680. [Google Scholar] [CrossRef] [Green Version]
- Yau, T.M.; Pagani, F.D.; Mancini, D.M.; Chang, H.L.; Lala, A.; Woo, Y.J.; Acker, M.A.; Selzman, C.H.; Soltesz, E.G.; Kern, J.A.; et al. Intramyocardial Injection of Mesenchymal Precursor Cells and Successful Temporary Weaning From Left Ventricular Assist Device Support in Patients With Advanced Heart Failure: A Randomized Clinical Trial. JAMA 2019, 321, 1176–1186. [Google Scholar] [CrossRef] [Green Version]
- Araña, M.; Mazo, M.; Aranda, P.; Pelacho, B.; Prosper, F. Adipose Tissue-Derived Mesenchymal Stem Cells: Isolation, Expansion, and Characterization. Cardiovasc. Dev. 2013, 1036, 47–61. [Google Scholar] [CrossRef]
- Araña, M.; Peña, E.; Abizanda, G.; Cilla, M.; Ochoa, I.; Gavira, J.J.; Espinosa, G.; Doblaré, M.; Pelacho, B.; Prosper, F.; et al. Preparation and characterization of collagen-based ADSC-carrier sheets for cardiovascular application. Acta Biomater. 2013, 9, 6075–6083. [Google Scholar] [CrossRef]
- Mazo, M.M.; Gavira, J.J.; Abizanda, G.; Moreno, C.; Ecay, M.; Soriano, M.; Aranda, P.; Collantes, M.; Alegría, E.; Merino, J.; et al. Transplantation of Mesenchymal Stem Cells Exerts a Greater Long-Term Effect than Bone Marrow Mononuclear Cells in a Chronic Myocardial Infarction Model in Rat. Cell Transplant. 2010, 19, 313–328. [Google Scholar] [CrossRef] [Green Version]
- Gavira, J.J.; Nasarre, E.; Abizanda, G.; Pérez-Ilzarbe, M.; De Martino-Rodriguez, A.; De Jalón, J.A.G.; Mazo, M.M.; Macias, A.; García-Bolao, I.; Pelacho, B.; et al. Repeated implantation of skeletal myoblast in a swine model of chronic myocardial infarction. Eur. Hear. J. 2009, 31, 1013–1021. [Google Scholar] [CrossRef] [Green Version]
- Daum, L.; Maurer, S.; Vaegler, M.; Sievert, K.D. In Vivo Biocompatibility Testing of a Collagen Cell Carrier Seeded with Human Urothelial Cells in Rats. J. Cell. Sci. Ther. 2015, 6, 215. [Google Scholar]
- Sievert, K.-D.; Daum, L.; Maurer, S.; Toomey, P.; Vaegler, M.; Aufderklamm, S.; Amend, B. Urethroplasty performed with an autologous urothelium-vegetated collagen fleece to treat urethral stricture in the minipig model. World J. Urol. 2019, 38, 2123–2131. [Google Scholar] [CrossRef]
- Isakova, I.A.; Lanclos, C.; Bruhn, J.; Kuroda, M.J.; Baker, K.C.; Krishnappa, V.; Phinney, N.G. Allo-Reactivity of Mesenchymal Stem Cells in Rhesus Macaques Is Dose and Haplotype Dependent and Limits Durable Cell Engraftment In Vivo. PLoS ONE 2014, 9, e87238. [Google Scholar] [CrossRef]
- Tano, N.; Kaneko, M.; Ichihara, Y.; Ikebe, C.; Coppen, S.R.; Shiraishi, M.; Shintani, Y.; Yashiro, K.; Warrens, A.; Suzuki, K. Allogeneic Mesenchymal Stromal Cells Transplanted Onto the Heart Surface Achieve Therapeutic Myocardial Repair Despite Immunologic Responses in Rats. J. Am. Heart Assoc. 2016, 5, e002815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berglund, A.K.; Schnabel, L.V. Allogeneic major histocompatibility complex-mismatched equine bone marrow-derived mesenchymal stem cells are targeted for death by cytotoxic anti-major histocompatibility complex antibodies. Equine Vet. J. 2017, 49, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Castellano, D.; Blanes, M.; Marco, B.; Cerrada, I.; Ruiz-Saurí, A.; Pelacho, B.; Araña, M.; Montero, J.A.; Cambra, V.; Prosper, F.; et al. A Comparison of Electrospun Polymers Reveals Poly(3-Hydroxybutyrate) Fiber as a Superior Scaffold for Cardiac Repair. Stem Cells Dev. 2014, 23, 1479–1490. [Google Scholar] [CrossRef] [Green Version]
- Hare, J.M.; Traverse, J.H.; Henry, T.D.; Dib, N.; Strumpf, R.K.; Schulman, S.P.; Gerstenblith, G.; DeMaria, A.N.; Denktas, A.E.; Gammon, R.S.; et al. A Randomized, Double-Blind, Placebo-Controlled, Dose-Escalation Study of Intravenous Adult Human Mesenchymal Stem Cells (Prochymal) After Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2009, 54, 2277–2286. [Google Scholar] [CrossRef] [Green Version]
- Hare, J.M.; Fishman, J.E.; Gerstenblith, G.; Velazquez, D.L.D.; Zambrano, J.P.; Suncion, V.Y.; Tracy, M.; Ghersin, E.; Johnston, P.V.; Brinker, J.A.; et al. Comparison of allogeneic vs autologous bone marrow-derived mesenchymal stem cells delivered by transendocardial injection in patients with ischemic cardiomyopathy: The POSEIDON randomized trial. JAMA 2012, 308, 2369–2379. [Google Scholar] [CrossRef]
- Florea, V.; Rieger, A.C.; DiFede, D.L.; El-Khorazaty, J.; Natsumeda, M.; Banerjee, M.N.; Tompkins, B.A.; Khan, A.; Schulman, I.H.; Landin, A.M.; et al. Dose Comparison Study of Allogeneic Mesenchymal Stem Cells in Patients With Ischemic Cardiomyopathy (The TRIDENT Study). Circ. Res. 2017, 121, 1279–1290. [Google Scholar] [CrossRef]
- Bolli, R.; Perin, E.C.; Willerson, J.T.; Yang, P.C.; Traverse, J.H.; Henry, T.D.; Pepine, C.J.; Mitrani, R.D.; Hare, J.M.; Murphy, M.P.; et al. Allogeneic Mesenchymal Cell Therapy in Anthracycline-Induced Cardiomyopathy Heart Failure Patients: The CCTRN SENECA Trial. JACC. Cardio Oncol. 2020, 2, 581–595. [Google Scholar]
- Ochando, J.; Ordikhani, F.; Boros, P.; Jordan, S. The innate immune response to allotransplants: Mechanisms and therapeutic potentials. Cell. Mol. Immunol. 2019, 16, 350–356. [Google Scholar] [CrossRef]
- Lin, C.M.; Gill, R.G. Direct and indirect allograft recognition: Pathways dictating graft rejection mechanisms. Curr. Opin. Organ. Transplant. 2016, 21, 40. [Google Scholar] [CrossRef] [Green Version]
- van Megen, K.M.; van’t Wout, E.J.T.; Lages Motta, J.; Dekker, B.; Nikolic, T.; Roep, B.O. Activated mesenchymal stromal cells process and present antigens regulating adaptive immunity. Front. Immunol. 2019, 10, 694. [Google Scholar] [CrossRef]
- Davies, L.C.; Heldring, N.; Kadri, N.; Le Blanc, K. Mesenchymal Stromal Cell Secretion of Programmed Death-1 Ligands Regulates T Cell Mediated Immunosuppression. Stem Cells 2017, 35, 766–776. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Time-Point | Findings | MI-ADSC-CS | MI-CS | Sham-ADSC-CS | Sham | ||||
|---|---|---|---|---|---|---|---|---|---|
| Day 2 | Sex (N° of animals) | Males (3) | Females (3) | Males (3) | Females (3) | Males (3) | Females (3) | Males (3) | Females (3) |
| Remains of matrix | 3 | 3 | 3 | 3 | 3 | 2 | - | - | |
| Inflammation, acute, pericardium | 3 (2.3) | 3 (1.3) | 3 (1.3) | 3 (1.3) | 3 (1.3) | 1 (2.0) | - | - | |
| Myocardial necrosis | 3 (3.0) | 3 (3.0) | 3 (3.0) | 3 (2.7) | - | - | - | - | |
| Macrophage aggregates | 3 (3.0) | 3 (1.7) | 3 (2.3) | 3 (2.0) | 3 (2.0) | 3 (1.3) | - | - | |
| Pigmented macrophages | - | 1 (1.0) | 3 (1.0) | 3 (1.3) | - | - | - | - | |
| Epicardial fibrosis | 3 (1.3) | 3 (1.7) | 3 (1.7) | 3 (1.0) | 2 (1.5) | 2 (2.0) | - | - | |
| Multinucleated giant cells | - | - | - | - | - | - | - | - | |
| Day 10 | Sex (N° of animals) | Males (3) | Females (3) | Males (3) | Females (3) | Males (3) | Females (3) | Males (3) | Females (3) |
| Remains of matrix | 3 | 3 | 3 | 3 | 3 | 2 | - | - | |
| Inflammation, acute, pericardium | - | - | - | - | - | - | - | - | |
| Myocardial necrosis | 3 (3.0) | 3 (3.0) | 3 (3.0) | 3 (2.7) | - | - | - | - | |
| Macrophage aggregates | 3 (3.0) | 3 (1.7) | 3 (2.3) | 3 (2.0) | 3 (2.0) | 3 (1.3) | - | - | |
| Pigmented macrophages | - | 1 (1.0) | 3 (1.0) | 3 (1.3) | - | - | - | - | |
| Epicardial fibrosis | 3 (1.3) | 3 (1.7) | 3 (1.7) | 3 (1.0) | 2 (1.5) | 2 (2.0) | - | - | |
| Multinucleated giant cells | - | - | - | - | - | - | - | - | |
| Day 90 | Sex (N° of animals) | Males (5) | Females (5) | Males (5) | Females (5) | Males (5) | Females (5) | Males (5) | Females (5) |
| Remains of matrix | 0 | 0 | 1 | 0 | 0 | 1 | - | - | |
| Inflammation, acute, pericardium | - | - | - | - | - | - | - | - | |
| Myocardial necrosis | - | - | - | - | - | 1 (2.0) | - | - | |
| Macrophage aggregates | - | - | - | - | - | - | - | - | |
| Pigmented macrophages | 4 (1.5) | 4 (1.0) | 2 (1.0) | 1 (1.0) | - | 3 (1.0) | -- | - | |
| Epicardial fibrosis | 5 (2.4) | 4 (1.8) | - | - | 2 (2.5) | 5 (2.2) | - | - | |
| Multinucleated giant cells | 1 (1.0) | - | - | - | - | - | - | - | |
| Myocardial mineralization | 5 (2.8) | 1 (3.0) | 1 (2.0) | - | - | - | - | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Díaz de Cerio, A.; Perez-Estenaga, I.; Inoges, S.; Abizanda, G.; Gavira, J.J.; Larequi, E.; Andreu, E.; Rodriguez, S.; Gil, A.G.; Crisostomo, V.; et al. Preclinical Evaluation of the Safety and Immunological Action of Allogeneic ADSC-Collagen Scaffolds in the Treatment of Chronic Ischemic Cardiomyopathy. Pharmaceutics 2021, 13, 1269. https://doi.org/10.3390/pharmaceutics13081269
López-Díaz de Cerio A, Perez-Estenaga I, Inoges S, Abizanda G, Gavira JJ, Larequi E, Andreu E, Rodriguez S, Gil AG, Crisostomo V, et al. Preclinical Evaluation of the Safety and Immunological Action of Allogeneic ADSC-Collagen Scaffolds in the Treatment of Chronic Ischemic Cardiomyopathy. Pharmaceutics. 2021; 13(8):1269. https://doi.org/10.3390/pharmaceutics13081269
Chicago/Turabian StyleLópez-Díaz de Cerio, Ascensión, Iñigo Perez-Estenaga, Susana Inoges, Gloria Abizanda, Juan José Gavira, Eduardo Larequi, Enrique Andreu, Saray Rodriguez, Ana Gloria Gil, Verónica Crisostomo, and et al. 2021. "Preclinical Evaluation of the Safety and Immunological Action of Allogeneic ADSC-Collagen Scaffolds in the Treatment of Chronic Ischemic Cardiomyopathy" Pharmaceutics 13, no. 8: 1269. https://doi.org/10.3390/pharmaceutics13081269
APA StyleLópez-Díaz de Cerio, A., Perez-Estenaga, I., Inoges, S., Abizanda, G., Gavira, J. J., Larequi, E., Andreu, E., Rodriguez, S., Gil, A. G., Crisostomo, V., Sanchez-Margallo, F. M., Bermejo, J., Jauregui, B., Quintana, L., Fernández-Avilés, F., Pelacho, B., & Prósper, F. (2021). Preclinical Evaluation of the Safety and Immunological Action of Allogeneic ADSC-Collagen Scaffolds in the Treatment of Chronic Ischemic Cardiomyopathy. Pharmaceutics, 13(8), 1269. https://doi.org/10.3390/pharmaceutics13081269