In Vitro Evaluation of a Vibrating-Mesh Nebulizer Repeatedly Use over 28 Days

 ,
, 
 ,
,
Abstract

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
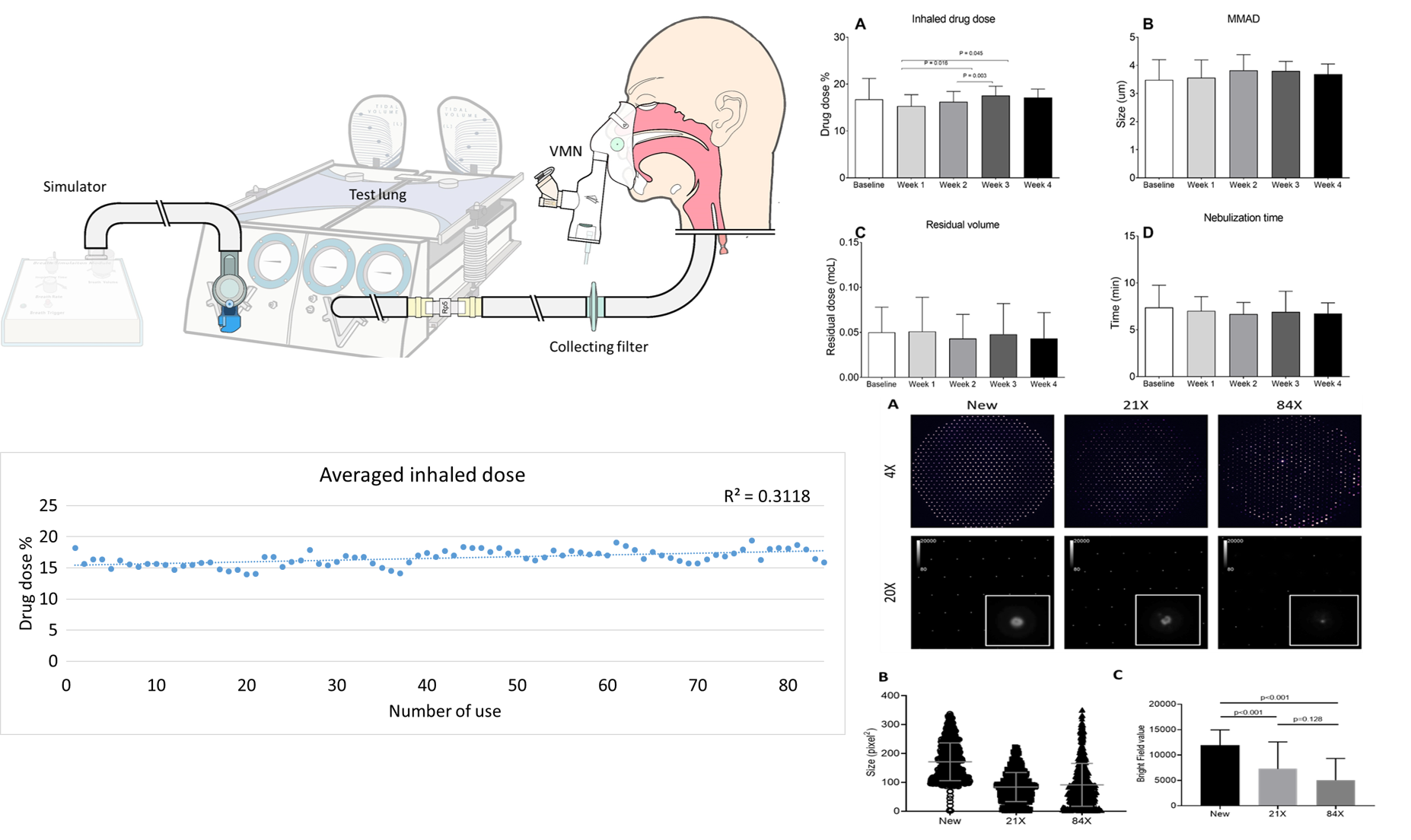
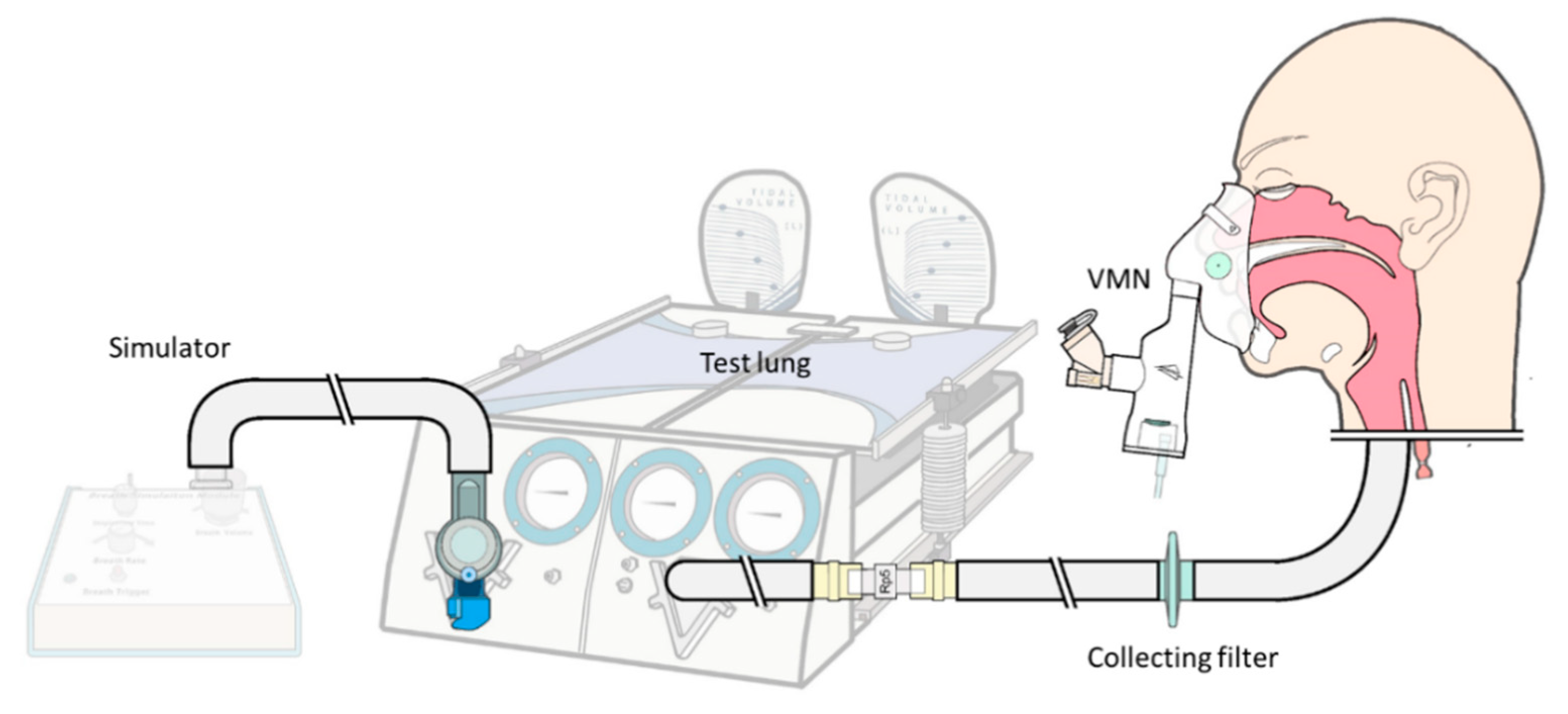
2.1. Lung Model
2.2. Experiment Protocol
2.3. Drug Assay
2.4. Aperture Plate Imaging
2.5. Statistical Analysis
3. Results
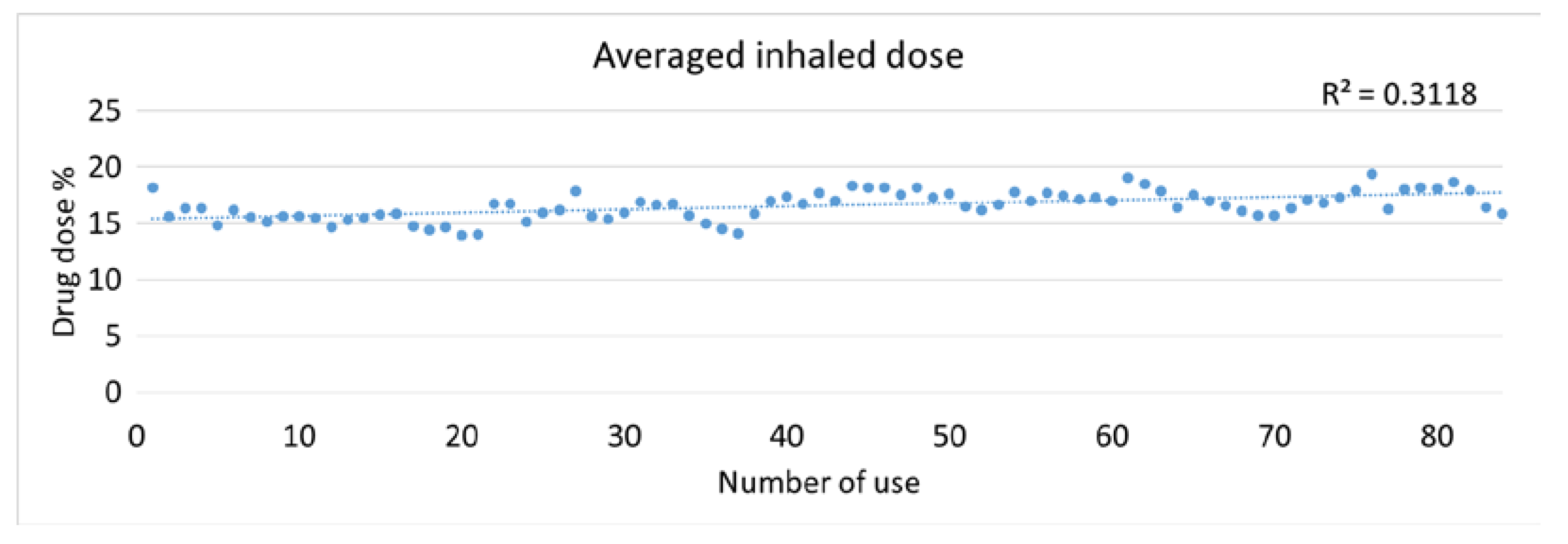
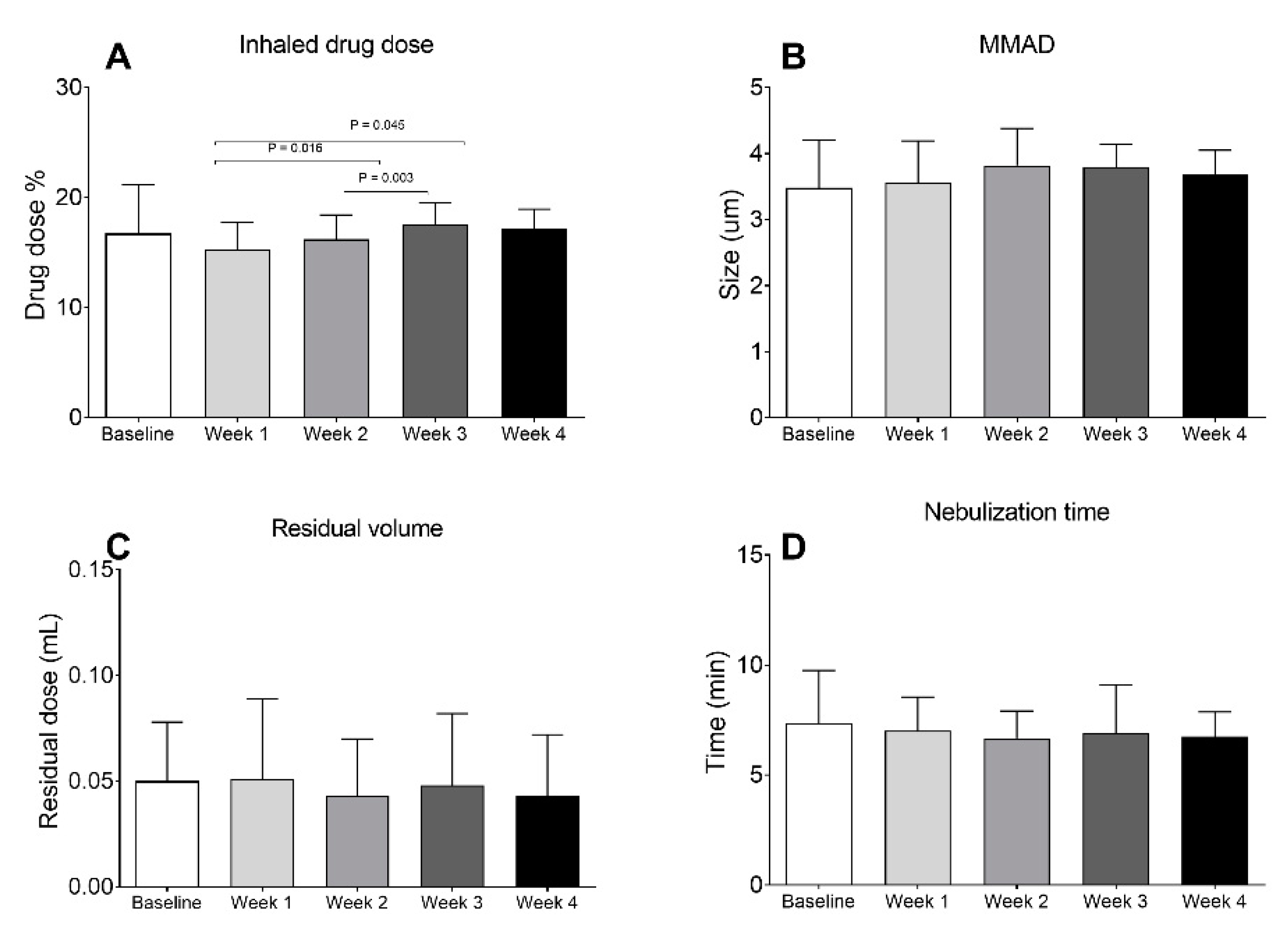
3.1. Inhaled Drug Dose
3.2. Nebulizer Performance
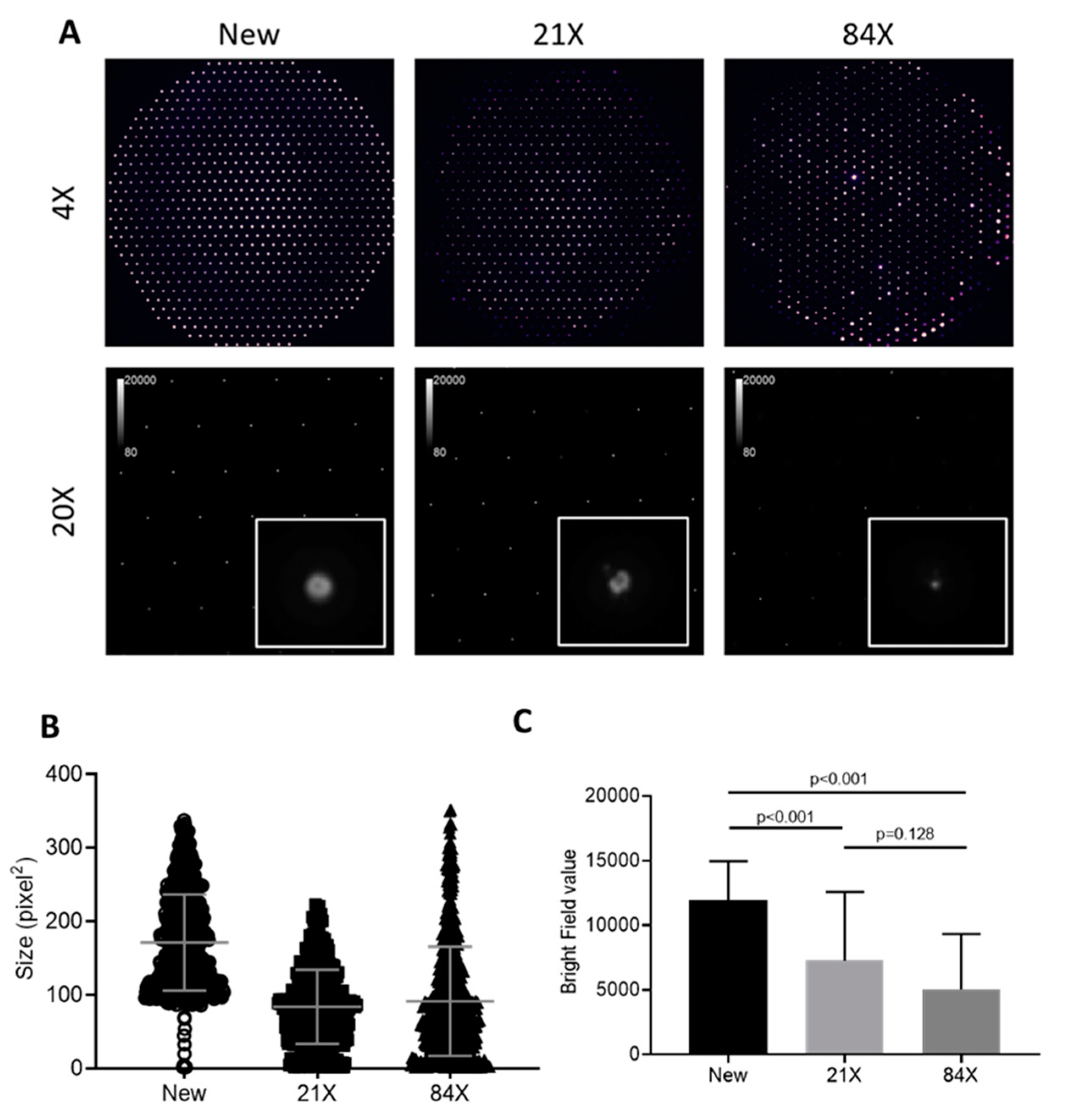
3.3. Images of Aperture Plates
4. Discussion
4.1. Nebulizer Performance
4.2. Aperture Image
4.3. Clinical Implication
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ari, A. Aerosol Therapy in Pulmonary Critical Care. Respir. Care 2015, 60, 858. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, S.D.; González, H.E.; Higgins, B.D. Future trends in nebulized therapies for pulmonary disease. J. Pers. Med. 2020, 10, 37. [Google Scholar] [CrossRef] [PubMed]
- Bohr, A.; Beck-Broichsitter, M. Generation of tailored aerosols for inhalative drug delivery employing recent vibrating-mesh nebulizer systems. Ther. Deliv. 2015, 6, 621–636. [Google Scholar] [CrossRef] [PubMed]
- Dhand, R. How should aerosols be delivered during invasive mechanical ventilation? Respir. Care 2017, 62, 1343–1367. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.H.; Moon, S.H.; Yoo, S.K.; Park, B.J.; Nam, K.C. Aerosol delivery of dornase alfa generated by jet and mesh nebulizers. Pharmaceutics 2020, 12, 721. [Google Scholar] [CrossRef] [PubMed]
- Esmaeilizand, R.; Rocha, T.; Harrison, A.; Gray, S.; Fusch, G.; Dolovich, M.; Mukerji, A. Efficiency of budesonide delivery via a mesh nebulizer in an in-vitro neonatal ventilator model. Pediatr. Pulmonol. 2020, 55, 2283–2288. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.Q.; Denault, A.Y.; Théoret, Y.; Perrault, L.P.; Varin, F. Inhaled milrinone in cardiac surgical patients: A pilot randomized controlled trial of jet vs. mesh nebulization. Sci. Rep. 2020, 10, 2069. [Google Scholar] [CrossRef] [PubMed]
- Pourheidar, E.; Haghighi, M.; Kouchek, M.; Miri, M.M.; Shojaei, S.; Salarian, S.; Hassanpour, R.; Sistanizad, M. Comparison of intravenous ampicillin-sulbactam plus nebulized colistin with intravenous colistin plus nebulized colistin in treatment of ventilator associated pneumonia caused by multi drug resistant acinetobacter baumannii: Randomized open label trial. Iran. J. Pharm. Res. 2019, 18 (Suppl. 1), 269–281. [Google Scholar] [PubMed]
- Rottier, B.L.; van Erp, C.J.; Sluyter, T.S.; Heijerman, H.G.; Frijlink, H.W.; Boer, A.H. Changes in performance of the Pari eFlow rapid and Pari LC Plus during 6 months use by CF patients. J. Aerosol Med. Pulm. Drug Deliv. 2009, 22, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Beck-Broichsitter, M. Aerosol production by vibrating membrane technology: Analysis of the electrolyte effect on generated droplet size and nebulizer output rate. J. Pharm. Sci. 2017, 10, 2168–2172. [Google Scholar] [CrossRef] [PubMed]
- Beck-Broichsitter, M.; Oesterheld, N. Electrolyte type and nozzle composition affect the process of vibrating-membrane nebulization. Eur. J. Pharm. Biopharm. 2017, 119, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Beck-Broichsitter, M.; Knuedeler, M.C.; Seeger, W.; Schmehl, T. Controlling the droplet size of formulations nebulized by vibrating-membrane technology. Eur. J. Pharm. Biopharm. 2014, 87, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Ghazanfari, T.; Elhissi, A.M.; Ding, Z.; Taylor, K.M. The influence of fluid physicochemical properties on vibrating-mesh nebulization. Int. J. Pharm. 2007, 339, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Najlah, M.; Vali, A.; Taylor, M.; Arafat, B.T.; Ahmed, W.; Phoenix, D.A.; Taylor, K.M.; Elhissi, A. A study of the effects of sodium halides on the performance of air-jet and vibrating-mesh nebulizers. Int. J. Pharm. 2013, 456, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Gowda, A.A.; Cuccia, A.D.; Smaldone, G.C. Reliability of vibrating mesh technology. Respir. Care 2017, 62, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, T.C.; McConville, J.T. The function and performance of aqueous aerosol devices for inhalation therapy. J. Pharm. Pharmacol. 2016, 68, 556–578. [Google Scholar] [CrossRef] [PubMed]
- Fink, J.B.; Ehrmann, S.; Li, J.; Dailey, P.; McKiernan, P.; Darquenne, C.; Martin, A.R.; Rothen-Rutishauser, B.; Kuehl, P.J.; Häussermann, S.; et al. Reducing Aerosol-Related Risk of Transmission in the Era of COVID-19: An Interim Guidance Endorsed by the International Society of Aerosols in Medicine. J. Aerosol Med. Pulm. Drug Deliv. 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- McCallion, O.N.M.; Patel, M.J. Viscosity effects on nebulisation of aqueous solutions. Int. J. Pharm. 1996, 130, 245–249. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, H.-L.; Chen, C.-S.; Fink, J.B.; Lee, G.-H.; Huang, C.-W.; Chen, J.-C.; Chiang, Z.Y. In Vitro Evaluation of a Vibrating-Mesh Nebulizer Repeatedly Use over 28 Days. Pharmaceutics 2020, 12, 971. https://doi.org/10.3390/pharmaceutics12100971
Lin H-L, Chen C-S, Fink JB, Lee G-H, Huang C-W, Chen J-C, Chiang ZY. In Vitro Evaluation of a Vibrating-Mesh Nebulizer Repeatedly Use over 28 Days. Pharmaceutics. 2020; 12(10):971. https://doi.org/10.3390/pharmaceutics12100971
Chicago/Turabian StyleLin, Hui-Ling, Chi-Shuo Chen, James B. Fink, Guo-Hao Lee, Chun-Wei Huang, Jui-Chi Chen, and Zi Yi Chiang. 2020. "In Vitro Evaluation of a Vibrating-Mesh Nebulizer Repeatedly Use over 28 Days" Pharmaceutics 12, no. 10: 971. https://doi.org/10.3390/pharmaceutics12100971
APA StyleLin, H.-L., Chen, C.-S., Fink, J. B., Lee, G.-H., Huang, C.-W., Chen, J.-C., & Chiang, Z. Y. (2020). In Vitro Evaluation of a Vibrating-Mesh Nebulizer Repeatedly Use over 28 Days. Pharmaceutics, 12(10), 971. https://doi.org/10.3390/pharmaceutics12100971