


Cytomegalovirus-Specific T Cells in Pediatric Liver Transplant Recipients
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Monitoring of CMV Infection
2.2. Analysis of CMV-Specific T Cells
2.3. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Peripheral Immune Cells in Enrolled Patients
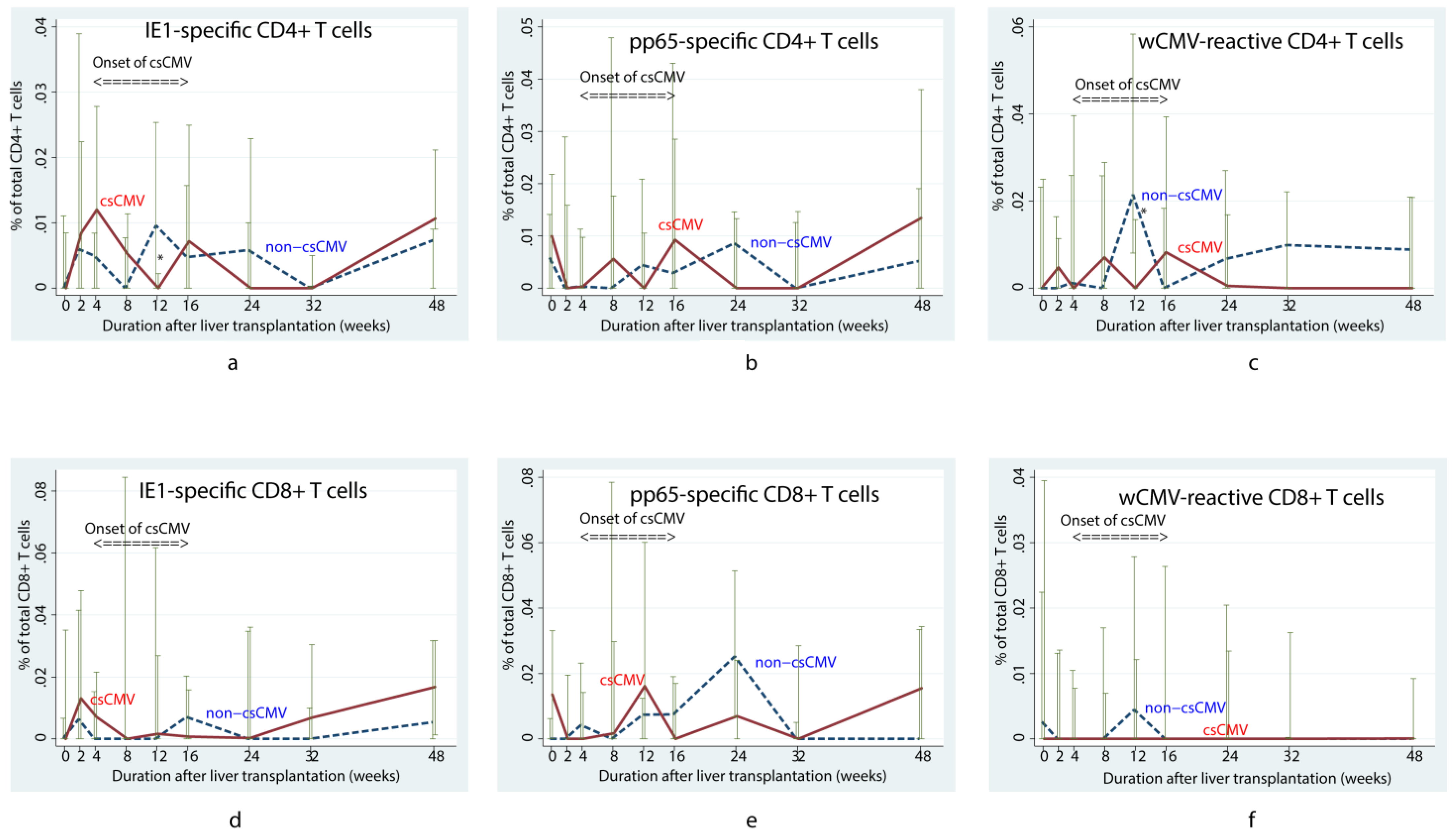
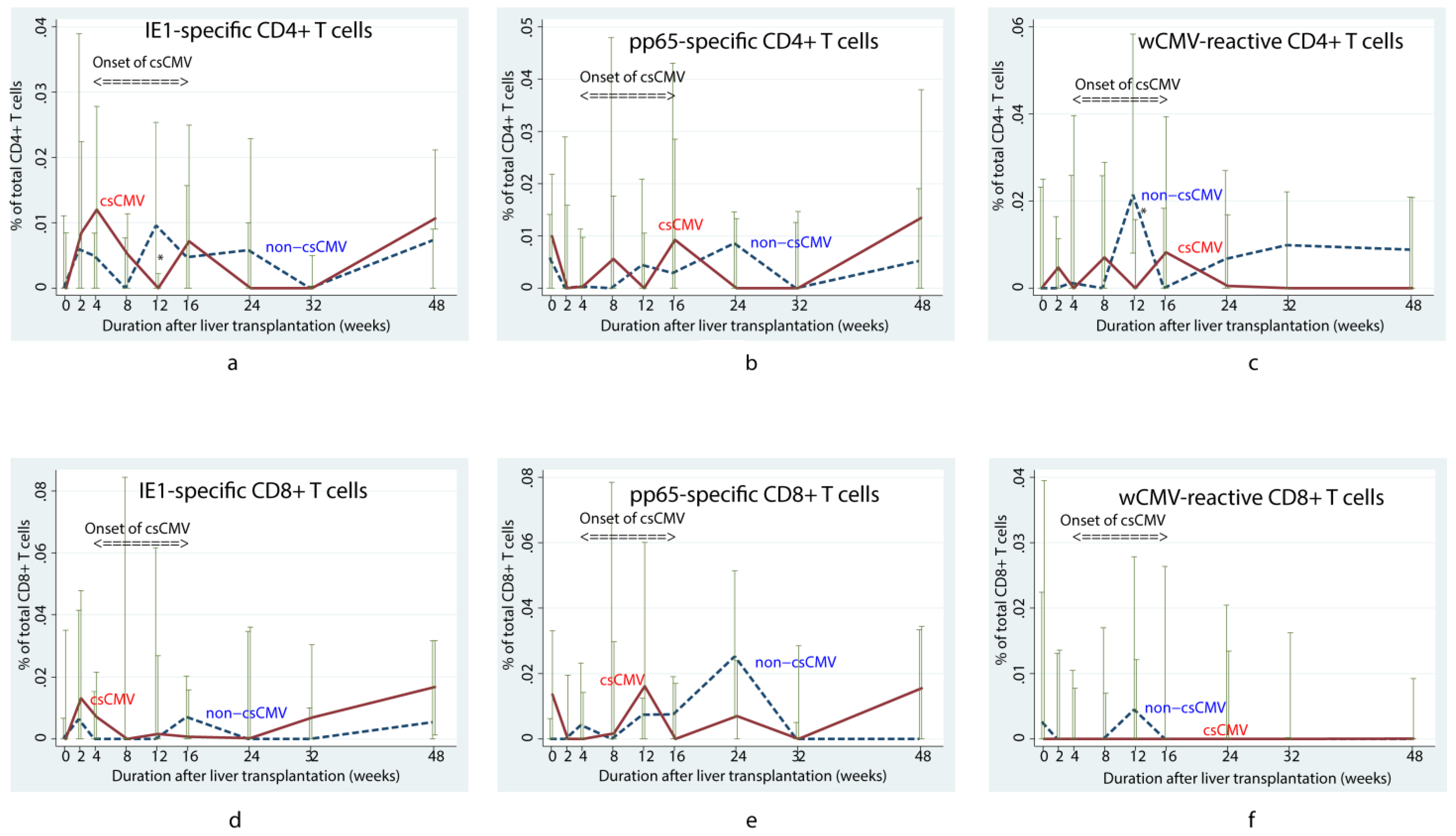
3.3. CMV-Specific T Cells Responding to pp65, IE1 and Whole Viral Lysate Ag in Patients Who Had Undergone LT
3.4. Correlation between CMV Load at csCMV Diagnosis and Virus-Specific Peripheral Immune Cells before Diagnosis
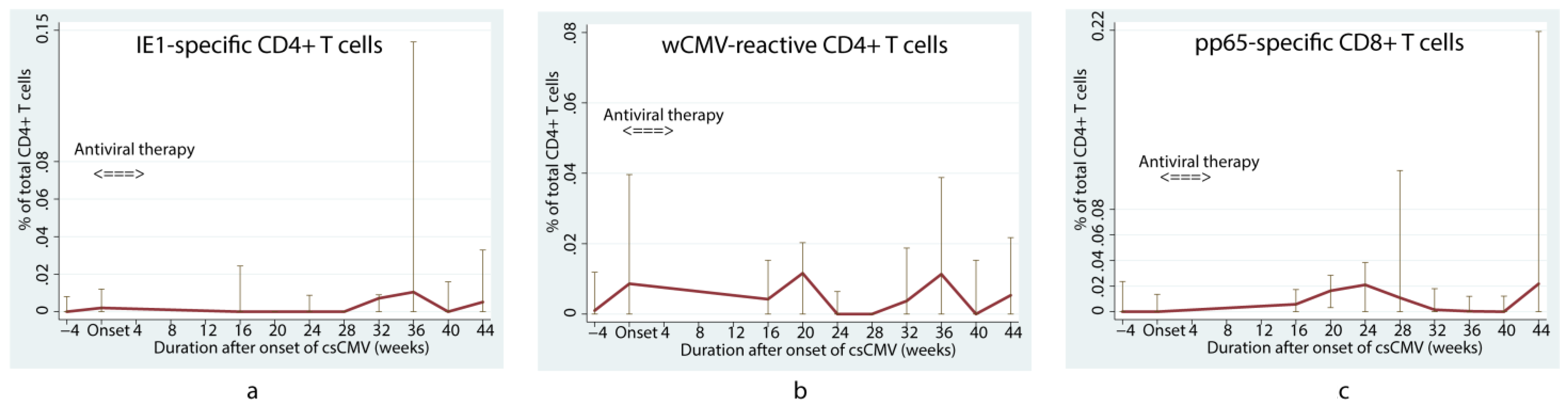
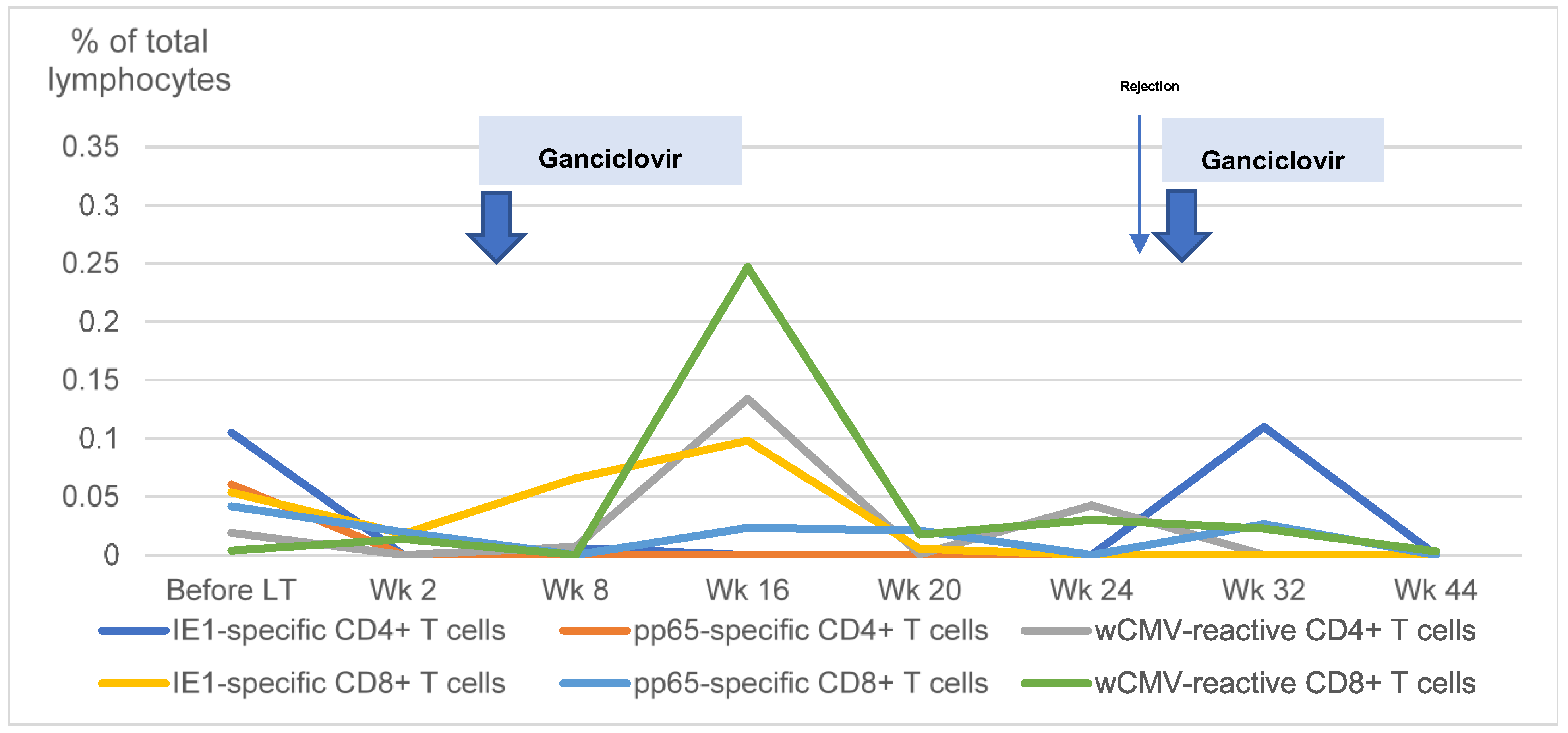
3.5. CMV-Specific T Cells in Patients with Recurrent csCMV
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A
References
- Lizaola-Mayo, B.C.; Rodriguez, E.A. Cytomegalovirus infection after liver transplantation. World J. Transplant. 2020, 10, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, P.; Reeves, M. Pathogenesis of human cytomegalovirus in the immunocompromised host. Nat. Rev. Microbiol. 2021, 19, 759–773. [Google Scholar] [CrossRef]
- Razonable, R.R.; Humar, A. Cytomegalovirus in solid organ transplant recipients-Guidelines of the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13512. [Google Scholar] [CrossRef]
- Rogers, R.; Saharia, K.; Chandorkar, A.; Weiss, Z.F.; Vieira, K.; Koo, S.; Farmakiotis, D. Clinical experience with a novel assay measuring cytomegalovirus (CMV)-specific CD4+ and CD8+ T-cell immunity by flow cytometry and intracellular cytokine staining to predict clinically significant CMV events. BMC Infect. Dis. 2020, 20, 58. [Google Scholar] [CrossRef]
- Chanburanavah, N.; Boonsathorn, S.; Apiwattanakul, N.; Lertudomphonwanit, C.; Getsuwan, S.; Tanpowpong, P.; Treepongkaruna, S. Risk factors of cytomegalovirus infection after pediatric liver transplantation and effectiveness of preemptive therapy. Transpl. Infect. Dis. 2023, 25, e14057. [Google Scholar] [CrossRef] [PubMed]
- Apiwattanakul, N.; Hongeng, S.; Anurathapan, U.; Pakakasama, S.; Srisala, S.; Klinmalai, C.; Andersson, B.S. CMV-Reactive NK Cells in Pediatric Post-Hematopoietic Stem Cell Transplant. Transplant. Proc. 2020, 52, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Benz, C.; Utermohlen, O.; Wulf, A.; Villmow, B.; Dries, V.; Goeser, T.; Koszinowski, U.; Busch, D.H. Activated virus-specific T cells are early indicators of anti-CMV immune reactions in liver transplant patients. Gastroenterology 2002, 122, 1201–1215. [Google Scholar] [CrossRef] [PubMed]
- Nebbia, G.; Mattes, F.M.; Smith, C.; Hainsworth, E.; Kopycinski, J.; Burroughs, A.; Griffiths, P.D.; Klenerman, P.; Emery, V.C. Polyfunctional cytomegalovirus-specific CD4+ and pp65 CD8+ T cells protect against high-level replication after liver transplantation. Am. J. Transplant. 2008, 8, 2590–2599. [Google Scholar] [CrossRef] [PubMed]
- Gabanti, E.; Bruno, F.; Lilleri, D.; Fornara, C.; Zelini, P.; Cane, I.; Migotto, C.; Sarchi, E.; Furione, M.; Gerna, G. Human cytomegalovirus (HCMV)-specific CD4+ and CD8+ T cells are both required for prevention of HCMV disease in seropositive solid-organ transplant recipients. PLoS ONE 2014, 9, e106044. [Google Scholar] [CrossRef] [PubMed]
- Cummins, N.W.; Deziel, P.J.; Abraham, R.S.; Razonable, R.R. Deficiency of cytomegalovirus (CMV)-specific CD8+ T cells in patients presenting with late-onset CMV disease several years after transplantation. Transpl. Infect. Dis. 2009, 11, 20–27. [Google Scholar] [CrossRef] [PubMed]
- La Rosa, C.; Limaye, A.P.; Krishnan, A.; Longmate, J.; Diamond, D.J. Longitudinal assessment of cytomegalovirus (CMV)-specific immune responses in liver transplant recipients at high risk for late CMV disease. J. Infect. Dis. 2007, 195, 633–644. [Google Scholar] [CrossRef]
- Shin, K.H.; Lee, H.J.; Chang, C.L.; Kim, E.J.; Lim, S.; Lee, S.J.; Ryu, J.H.; Yang, K.; Choi, B.H.; Lee, T.B.; et al. CMV specific T cell immunity predicts early viremia after liver transplantation. Transpl. Immunol. 2018, 51, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Carvalho-Gomes, A.; Cubells, A.; Pallares, C.; Corpas-Burgos, F.; Berenguer, M.; Aguilera, V.; López-Labrador, F.X. Cytomegalovirus specific polyfunctional T-cell responses expressing CD107a predict control of CMV infection after liver transplantation. Cell. Immunol. 2022, 371, 104455. [Google Scholar] [CrossRef] [PubMed]
- Burton, C.E.; Sester, M.; Robinson, J.L.; Eurich, D.T.; Preiksaitis, J.K.; Urschel, S. Assigning Cytomegalovirus Status in Children Awaiting Organ Transplant: Viral Shedding, CMV-Specific T Cells, and CD27-CD28-CD4+ T Cells. J. Infect. Dis. 2018, 218, 1205–1209. [Google Scholar] [CrossRef] [PubMed]
- Mena-Romo, J.D.; Perez Romero, P.; Martin-Gandul, C.; Gentil, M.A.; Suarez-Artacho, G.; Lage, E.; Sánchez, M.; Cordero, E. CMV-specific T-cell immunity in solid organ transplant recipients at low risk of CMV infection. Chronology and applicability in preemptive therapy. J. Infect. 2017, 75, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Sood, S.; Haifer, C.; Yu, L.; Pavlovic, J.; Gow, P.J.; Jones, R.M.; Visvanathan, K.; Angus, P.W.; Testro, A.G. Targeted individual prophylaxis offers superior risk stratification for cytomegalovirus reactivation after liver transplantation. Liver Transpl. 2015, 21, 1478–1485. [Google Scholar] [CrossRef] [PubMed]
- Sood, S.; Haifer, C.; Yu, L.; Pavlovic, J.; Gow, P.J.; Jones, R.M.; Visvanathan, K.; Angus, P.; Testro, A. Early viral-specific T-cell testing predicts late cytomegalovirus reactivation following liver transplantation. Transpl. Infect. Dis. 2018, 20, e12934. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Results |
|---|---|
| Age (years), median (IQR) | 1.9 (1.2–5.0) |
| Male, N (%) | 21 (51.2%) |
| Diagnosis of primary liver disease, N (%) | |
| - Biliary atresia | 33 (80.5%) |
| - Other chronic liver diseases * | 6 (14.6%) |
| - Acute liver failure | 2 (4.9%) |
| Types of liver transplantation, N (%) | |
| - Living donor liver transplantation | 34 (82.9%) |
| - Deceased donor liver transplantation | 7 (17.1%) |
| Acute cellular rejection, N (%) | 11 (26.8%) |
| Anti-CMV IgG before transplant, N (%) | |
| - D+/R+ | 38 (92.7%) |
| - D+/R− | 1 (2.4%) |
| - D−/R+ | 2 (4.9%) |
| Clinically significant CMV viremia after transplant, N (%) | 20 (48.8%) |
| - CMV reactivation | 17 |
| Onset of CMV infection after transplant (weeks), median (IQR) | 7 (4–12.9) |
| Duration of CMV infection treatment (weeks), median (IQR) | 4 (3–4.1) |
| Cells | Spearman’s Rho | p |
|---|---|---|
| Total lymphocyte count | 0.406 | 0.10 |
| Percentage of cells per total CD4+ T cells | ||
| - IE1-specific CD4+ | −0.097 | 0.70 |
| - pp65-specific CD4+ | 0.039 | 0.88 |
| - wCMV-reactive CD4+ | 0.125 | 0.62 |
| Percentage of cells per total CD8+ T cells | ||
| - IE1-specific CD8+ | −0.298 | 0.23 |
| - pp65-specific CD8+ | −0.553 | 0.02 |
| - wCMV-reactive CD8+ | −0.273 | 0.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Getsuwan, S.; Apiwattanakul, N.; Lertudomphonwanit, C.; Hongeng, S.; Boonsathorn, S.; Manuyakorn, W.; Tanpowpong, P.; Anurathapan, U.; Tangnararatchakit, K.; Treepongkaruna, S. Cytomegalovirus-Specific T Cells in Pediatric Liver Transplant Recipients. Viruses 2023, 15, 2213. https://doi.org/10.3390/v15112213
Getsuwan S, Apiwattanakul N, Lertudomphonwanit C, Hongeng S, Boonsathorn S, Manuyakorn W, Tanpowpong P, Anurathapan U, Tangnararatchakit K, Treepongkaruna S. Cytomegalovirus-Specific T Cells in Pediatric Liver Transplant Recipients. Viruses. 2023; 15(11):2213. https://doi.org/10.3390/v15112213
Chicago/Turabian StyleGetsuwan, Songpon, Nopporn Apiwattanakul, Chatmanee Lertudomphonwanit, Suradej Hongeng, Sophida Boonsathorn, Wiparat Manuyakorn, Pornthep Tanpowpong, Usanarat Anurathapan, Kanchana Tangnararatchakit, and Suporn Treepongkaruna. 2023. "Cytomegalovirus-Specific T Cells in Pediatric Liver Transplant Recipients" Viruses 15, no. 11: 2213. https://doi.org/10.3390/v15112213
APA StyleGetsuwan, S., Apiwattanakul, N., Lertudomphonwanit, C., Hongeng, S., Boonsathorn, S., Manuyakorn, W., Tanpowpong, P., Anurathapan, U., Tangnararatchakit, K., & Treepongkaruna, S. (2023). Cytomegalovirus-Specific T Cells in Pediatric Liver Transplant Recipients. Viruses, 15(11), 2213. https://doi.org/10.3390/v15112213