
Identification of High-Risk Human Papillomavirus DNA, p16, and E6/E7 Oncoproteins in Laryngeal and Hypopharyngeal Squamous Cell Carcinomas

 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients’ Characteristics
2.2. DNA Extraction
2.3. HPV DNA Detection Using MY09/11 and GP5+/6+ Consensus Primers
2.4. HPV Genotyping
2.5. Immunohistochemistry
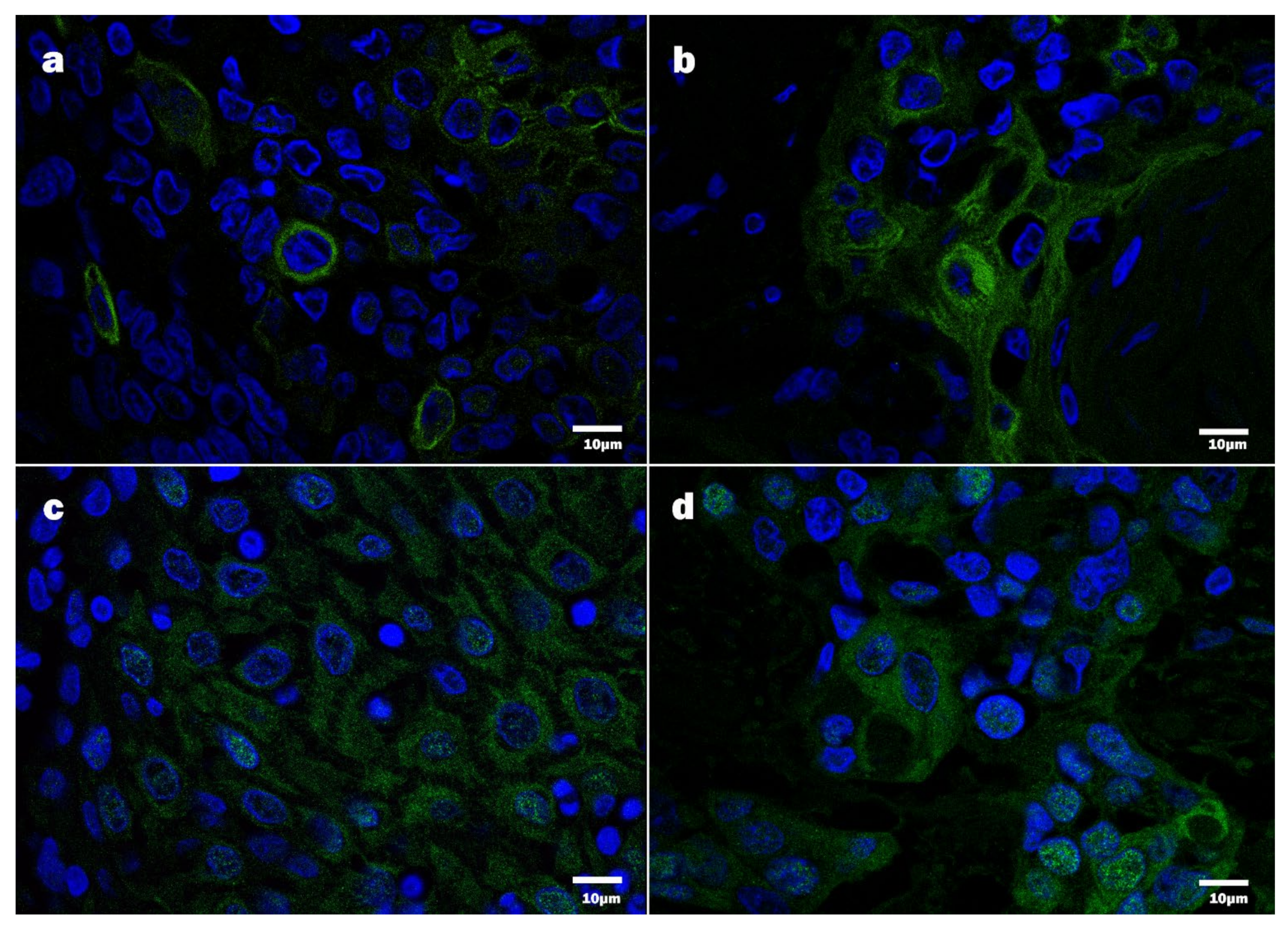
2.6. Immunofluorescence
2.7. Statistical Data Analysis
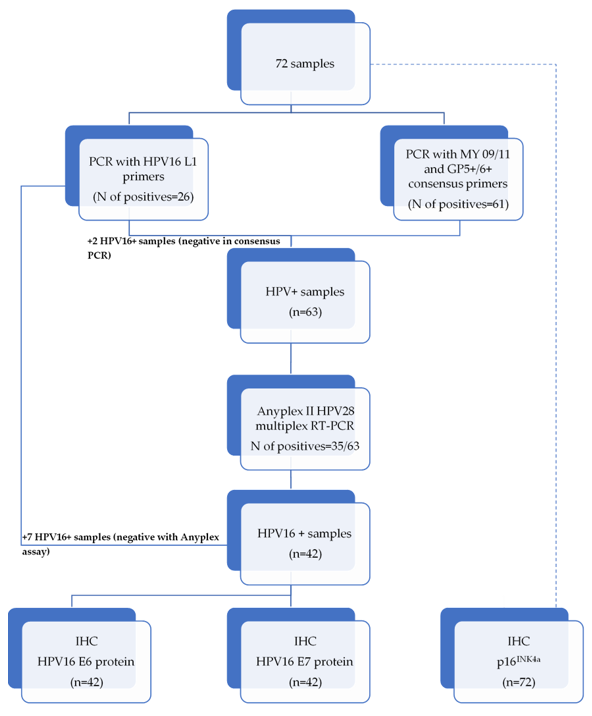
3. Results
3.1. HPV DNA Detection Using MY09/11 and GP5+/6+ Consensus Primers
3.2. HPV Genotyping Using HPV16 and HPV18 L1 Primers
3.3. Detection of HPV Using Anyplex II HPV28 RT-PCR
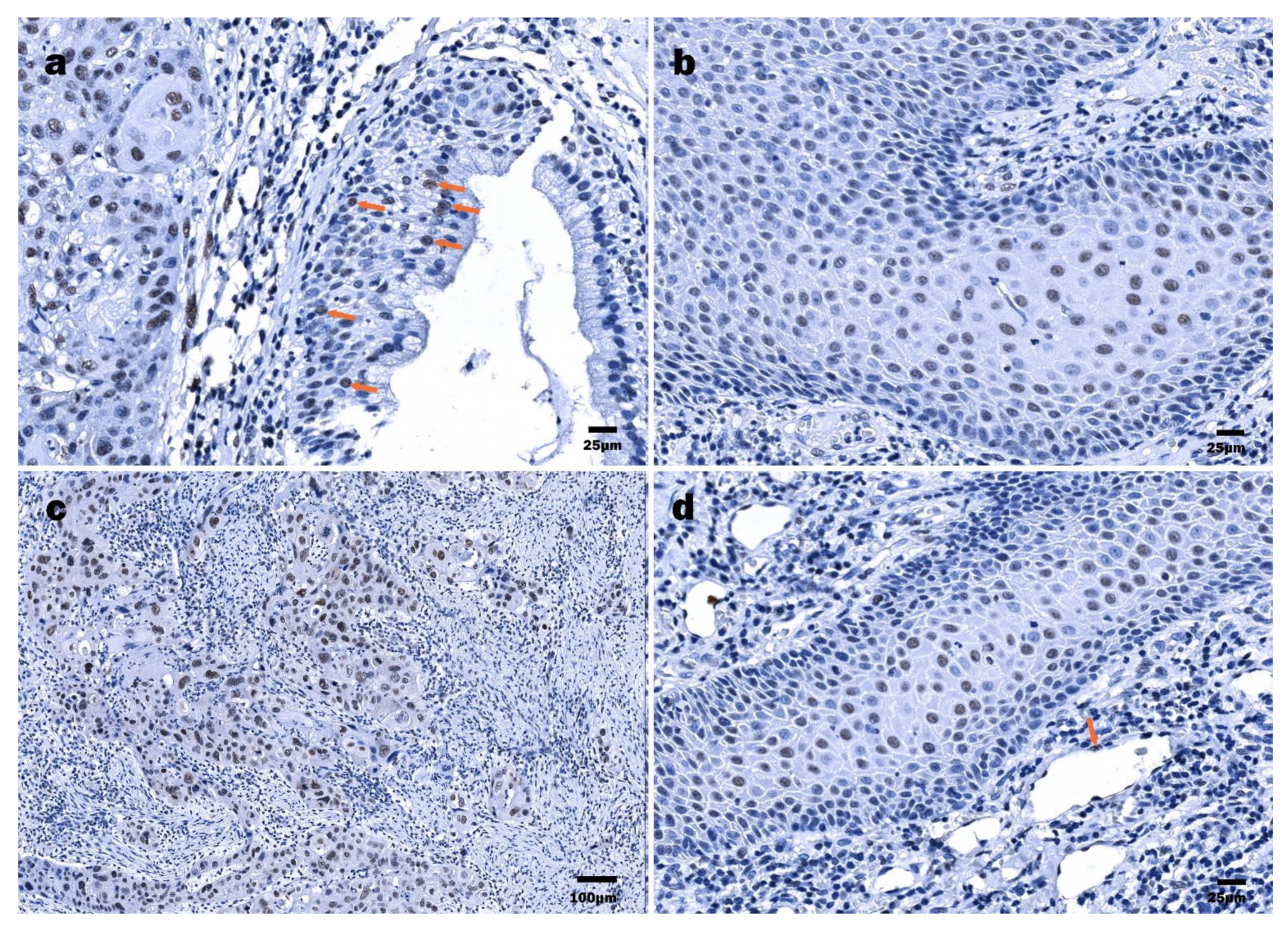
3.4. Immunohistochemical Detection of p16INK4a
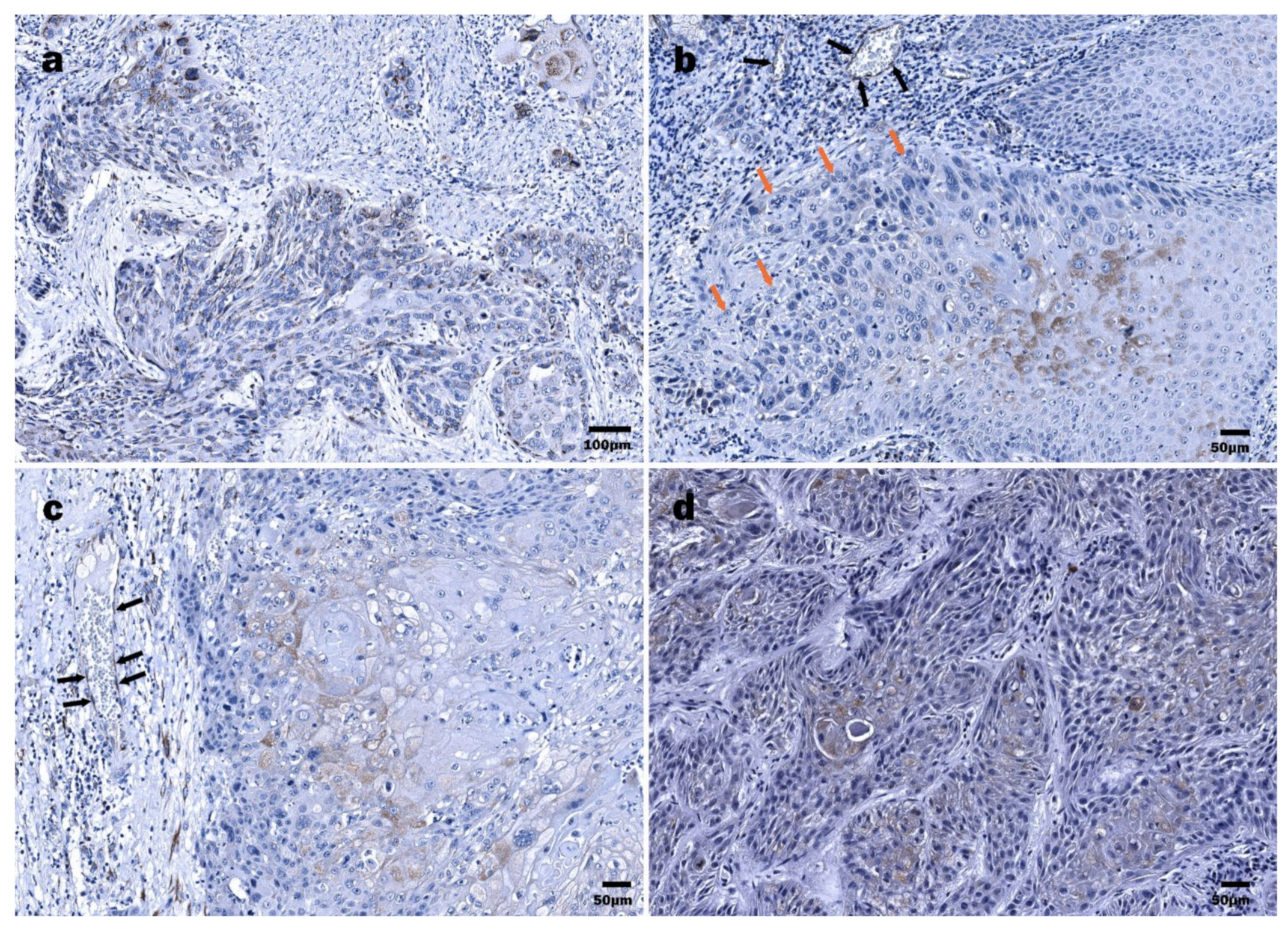
3.5. Immunohistochemical Detection of HPV16 E6 and E7 Oncoproteins in LSCC and HPSCC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Cancer Today. Available online: http://gco.iarc.fr/today/home (accessed on 24 April 2021).
- Liu, J.; Zhu, W.; Li, Z.; Cai, G.; Wang, J.; Tang, Q.; Maroun, C.A.; Zhu, G. Proteomic Analysis of Hypopharyngeal and Laryngeal Squamous Cell Carcinoma Sheds Light on Differences in Survival. Sci. Rep. 2020, 10, 19459. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, A.K.; Engels, E.A.; Pfeiffer, R.M.; Hernandez, B.Y.; Xiao, W.; Kim, E.; Jiang, B.; Goodman, M.T.; Sibug-Saber, M.; Cozen, W.; et al. Human Papillomavirus and Rising Oropharyngeal Cancer Incidence in the United States. J. Clin. Oncol. 2011, 29, 4294–4301. [Google Scholar] [CrossRef] [PubMed]
- Mac, M.; Moody, C.A. Epigenetic Regulation of the Human Papillomavirus Life Cycle. Pathogens 2020, 9, 483. [Google Scholar] [CrossRef] [PubMed]
- Chi, J.; Preeshagul, I.R.; Sheikh-Fayyaz, S.; Teckie, S.; Kohn, N.; Ziemba, Y.; Laser, A.; Frank, D.; Ghaly, M.; Kamdar, D.; et al. Evaluating of HPV–DNA ISH as an Adjunct to P16 Testing in Oropharyngeal Cancer. Future Sci. OA 2020, 6. [Google Scholar] [CrossRef]
- Elrefaey, S.; Massaro, M.A.; Chiocca, S.; Chiesa, F.; Ansarin, M. HPV in Oropharyngeal Cancer: The Basics to Know in Clinical Practice. Acta Otorhinolaryngol. Ital. 2014, 34, 299–309. [Google Scholar]
- Mirghani, H.; Lang Kuhs, K.A.; Waterboer, T. Biomarkers for Early Identification of Recurrences in HPV-Driven Oropharyngeal Cancer. Oral Oncol. 2018, 82, 108–114. [Google Scholar] [CrossRef]
- Craig, S.G.; Anderson, L.A.; Schache, A.G.; Moran, M.; Graham, L.; Currie, K.; Rooney, K.; Robinson, M.; Upile, N.S.; Brooker, R.; et al. Recommendations for Determining HPV Status in Patients with Oropharyngeal Cancers under TNM8 Guidelines: A Two-Tier Approach. Br. J. Cancer 2019, 120, 827–833. [Google Scholar] [CrossRef]
- Huang, S.H.; Perez-Ordonez, B.; Weinreb, I.; Hope, A.; Massey, C.; Waldron, J.N.; Kim, J.; Bayley, A.J.; Cummings, B.; Cho, B.C.J.; et al. Natural Course of Distant Metastases Following Radiotherapy or Chemoradiotherapy in HPV-Related Oropharyngeal Cancer. Oral Oncol. 2013, 49, 79–85. [Google Scholar] [CrossRef]
- Dahm, V.; Haitel, A.; Kaider, A.; Stanisz, I.; Beer, A.; Lill, C. Cancer Stage and Pack-Years, but Not P16 or HPV, Are Relevant for Survival in Hypopharyngeal and Laryngeal Squamous Cell Carcinomas. Eur. Arch. Otorhinolaryngol. 2018, 275, 1837–1843. [Google Scholar] [CrossRef]
- Gallo, A.; Degener, A.M.; Pagliuca, G.; Pierangeli, A.; Bizzoni, F.; Greco, A.; de Vincentiis, M. Detection of Human Papillomavirus and Adenovirus in Benign and Malignant Lesions of the Larynx. Otolaryngol. Head Neck Surg. 2009, 141, 276–281. [Google Scholar] [CrossRef]
- Ferreira, A.R.; Ramalho, A.C.; Marques, M.; Ribeiro, D. The Interplay between Antiviral Signalling and Carcinogenesis in Human Papillomavirus Infections. Cancers 2020, 12, 646. [Google Scholar] [CrossRef]
- Graham, S.V.; Faizo, A.A.A. Control of Human Papillomavirus Gene Expression by Alternative Splicing. Virus Res. 2017, 231, 83–95. [Google Scholar] [CrossRef]
- Moody, C. Mechanisms by Which HPV Induces a Replication Competent Environment in Differentiating Keratinocytes. Viruses 2017, 9, 261. [Google Scholar] [CrossRef]
- Bodily, J.; Laimins, L.A. Persistence of Human Papillomavirus Infections: Keys to Malignant Progression. Trends Microbiol. 2011, 19, 33–39. [Google Scholar] [CrossRef]
- Münger, K.; Baldwin, A.; Edwards, K.M.; Hayakawa, H.; Nguyen, C.L.; Owens, M.; Grace, M.; Huh, K. Mechanisms of Human Papillomavirus-Induced Oncogenesis. J. Virol. 2004, 78, 11451–11460. [Google Scholar] [CrossRef]
- Yeo-Teh, N.S.L.; Ito, Y.; Jha, S. High-Risk Human Papillomaviral Oncogenes E6 and E7 Target Key Cellular Pathways to Achieve Oncogenesis. Int. J. Mol. Sci. 2018, 19, 1706. [Google Scholar] [CrossRef]
- Smeets, S.J.; van der Plas, M.; Schaaij-Visser, T.B.M.; van Veen, E.A.M.; van Meerloo, J.; Braakhuis, B.J.M.; Steenbergen, R.D.M.; Brakenhoff, R.H. Immortalization of Oral Keratinocytes by Functional Inactivation of the P53 and PRb Pathways. Int. J. Cancer 2011, 128, 1596–1605. [Google Scholar] [CrossRef]
- McLaughlin-Drubin, M.E.; Park, D.; Munger, K. Tumor Suppressor P16INK4A Is Necessary for Survival of Cervical Carcinoma Cell Lines. Proc. Natl. Acad. Sci. USA 2013, 110, 16175–16180. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to Build a Bridge from a Population-Based to a More “Personalized” Approach to Cancer Staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Zanoni, D.K.; Patel, S.G.; Shah, J.P. Changes in the 8th Edition of the American Joint Committee on Cancer (AJCC) Staging of Head and Neck Cancer: Rationale and Implications. Curr. Oncol. Rep. 2019, 21, 52. [Google Scholar] [CrossRef]
- Kato, M.G.; Baek, C.-H.; Chaturvedi, P.; Gallagher, R.; Kowalski, L.P.; Leemans, C.R.; Warnakulasuriya, S.; Nguyen, S.A.; Day, T.A. Update on Oral and Oropharyngeal Cancer Staging—International Perspectives. World J. Otorhinolaryngol. Head Neck Surg. 2020, 6, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Augustin, J.; Mandavit, M.; Outh-Gauer, S.; Grard, O.; Gasne, C.; Lépine, C.; Mirghani, H.; Hans, S.; Bonfils, P.; Denize, T.; et al. HPV RNA CISH Score Identifies Two Prognostic Groups in a P16 Positive Oropharyngeal Squamous Cell Carcinoma Population. Modern Pathology 2018, 31, 1645–1652. [Google Scholar] [CrossRef] [PubMed]
- Bishop, J.A.; Lewis, J.S.; Rocco, J.W.; Faquin, W.C. HPV-Related Squamous Cell Carcinoma of the Head and Neck: An Update on Testing in Routine Pathology Practice. Semin. Diagn. Pathol. 2015, 32, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Rietbergen, M.M.; Snijders, P.J.F.; Beekzada, D.; Braakhuis, B.J.M.; Brink, A.; Heideman, D.A.M.; Hesselink, A.T.; Witte, B.I.; Bloemena, E.; Baatenburg-De Jong, R.J.; et al. Molecular Characterization of P16-Immunopositive but HPV DNA-Negative Oropharyngeal Carcinomas. Int. J. Cancer 2014, 134, 2366–2372. [Google Scholar] [CrossRef] [PubMed]
- Schache, A.G.; Liloglou, T.; Risk, J.M.; Filia, A.; Jones, T.M.; Sheard, J.; Woolgar, J.A.; Helliwell, T.R.; Triantafyllou, A.; Robinson, M.; et al. Evaluation of Human Papilloma Virus Diagnostic Testing in Oropharyngeal Squamous Cell Carcinoma: Sensitivity, Specificity, and Prognostic Discrimination. Clin. Cancer Res. 2011, 17, 6262–6271. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Tribius, S.; Quabius, E.S.; Henry, H.; Pfannenschmidt, S.; Burkhardt, C.; Görögh, T.; Halec, G.; Hoffmann, A.S.; Kahn, T.; et al. HPV DNA, E6*I-MRNA Expression and P16INK4A Immunohistochemistry in Head and Neck Cancer—How Valid Is P16INK4A as Surrogate Marker? Cancer Lett. 2012, 323, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.; Sloan, P.; Shaw, R. Refining the Diagnosis of Oropharyngeal Squamous Cell Carcinoma Using Human Papillomavirus Testing. Oral Oncol. 2010, 46, 492–496. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, G.; Westra, W.H.; Wang, S.J.; van Zante, A.; Wentz, A.; Kluz, N.; Rettig, E.; Ryan, W.R.; Ha, P.K.; Kang, H.; et al. Differences in the Prevalence of Human Papillomavirus (HPV) in Head and Neck Squamous Cell Cancers by Sex, Race, Anatomic Tumor Site, and HPV Detection Method. JAMA Oncol. 2017, 3, 169–177. [Google Scholar] [CrossRef]
- Augustin, J.G.; Lepine, C.; Morini, A.; Brunet, A.; Veyer, D.; Brochard, C.; Mirghani, H.; Péré, H.; Badoual, C. HPV Detection in Head and Neck Squamous Cell Carcinomas: What Is the Issue? Front. Oncol. 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.S., Jr.; Beadle, B.; Bishop, J.A.; Chernock, R.D.; Colasacco, C.; Lacchetti, C.; Moncur, J.T.; Rocco, J.W.; Schwartz, M.R.; Seethala, R.R.; et al. Human Papillomavirus Testing in Head and Neck Carcinomas: Guideline From the College of American Pathologists. Arch. Pathol. Lab. Med. 2017, 142, 559–597. [Google Scholar] [CrossRef] [PubMed]
- de Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide Burden of Cancer Attributable to HPV by Site, Country and HPV Type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Ndiaye, C.; Mena, M.; Alemany, L.; Arbyn, M.; Castellsagué, X.; Laporte, L.; Bosch, F.X.; de Sanjosé, S.; Trottier, H. HPV DNA, E6/E7 MRNA, and P16INK4a Detection in Head and Neck Cancers: A Systematic Review and Meta-Analysis. Lancet Oncol. 2014, 15, 1319–1331. [Google Scholar] [CrossRef]
- Plummer, M.; de Martel, C.; Vignat, J.; Ferlay, J.; Bray, F.; Franceschi, S. Global Burden of Cancers Attributable to Infections in 2012: A Synthetic Analysis. Lancet Glob. Health 2016, 4, e609–e616. [Google Scholar] [CrossRef]
- Combes, J.-D.; Franceschi, S. Role of Human Papillomavirus in Non-Oropharyngeal Head and Neck Cancers. Oral Oncol. 2014, 50, 370–379. [Google Scholar] [CrossRef]
- Mills, A.M.; Dirks, D.C.; Poulter, M.D.; Mills, S.E.; Stoler, M.H. HR-HPV E6/E7 MRNA In Situ Hybridization: Validation Against PCR, DNA In Situ Hybridization, and P16 Immunohistochemistry in 102 Samples of Cervical, Vulvar, Anal, and Head and Neck Neoplasia. Am. J. Surg. Pathol. 2017, 41, 607–615. [Google Scholar] [CrossRef]
- Bagnardi, V.; Rota, M.; Botteri, E.; Tramacere, I.; Islami, F.; Fedirko, V.; Scotti, L.; Jenab, M.; Turati, F.; Pasquali, E.; et al. Alcohol Consumption and Site-Specific Cancer Risk: A Comprehensive Dose-Response Meta-Analysis. Br. J. Cancer 2015, 112, 580–593. [Google Scholar] [CrossRef]
- Vandamme, A.-M.; Fransen, K.; Debaisieux, L.; Marissens, D.; Sprecher, S.; Vaira, D.; Vandenbroucke, A.T.; Verhofstede, C.; Van Dooren, S.; Goubau, P.; et al. Standardisation of Primers and an Algorithm for HIV-1 Diagnostic PCR Evaluated in Patients Harbouring Strains of Diverse Geographical Origin. J. Virol. Methods 1995, 51, 305–316. [Google Scholar] [CrossRef]
- Şahiner, F.; Kubar, A.; Gümral, R.; Ardıç, M.; Yiğit, N.; Şener, K.; Dede, M.; Yapar, M. Efficiency of MY09/11 Consensus PCR in the Detection of Multiple HPV Infections. Diagn. Microbiol. Infect. Dis. 2014, 80, 43–49. [Google Scholar] [CrossRef]
- Shikova, E.; Todorova, I.; Ganchev, G.; Kouseva-Dragneva, V. Detection and Typing of Human Papillomaviruses by PCR. Biotechnol. Biotechnol. Equip. 2009, 23, 877–880. [Google Scholar] [CrossRef]
- Zake, T.; Skuja, S.; Kalere, I.; Konrade, I.; Groma, V. Upregulated Tissue Expression of T Helper (Th) 17 Pathogenic Interleukin (IL)-23 and IL-1β in Hashimoto’s Thyroiditis but Not in Graves’ Disease. Endocr. J. 2019, 66, 423–430. [Google Scholar] [CrossRef]
- Skuja, S.; Vilmane, A.; Svirskis, S.; Groma, V.; Murovska, M. Evidence of Human Parvovirus B19 Infection in the Post-Mortem Brain Tissue of the Elderly. Viruses 2018, 10, 582. [Google Scholar] [CrossRef]
- Yang, J.; Dai, L.-X.; Chen, M.; Li, B.; Ding, N.; Li, G.; Liu, Y.-Q.; Li, M.-Y.; Wang, B.-N.; Shi, X.-L.; et al. Inhibition of Antiviral Drug Cidofovir on Proliferation of Human Papillomavirus-Infected Cervical Cancer Cells. Exp. Ther. Med. 2016, 12, 2965–2973. [Google Scholar] [CrossRef]
- Meng, Y.; Liang, H.; Hu, J.; Liu, S.; Hao, X.; Wong, M.S.K.; Li, X.; Hu, L. PD-L1 Expression Correlates With Tumor Infiltrating Lymphocytes And Response To Neoadjuvant Chemotherapy In Cervical Cancer. J. Cancer 2018, 9, 2938–2945. [Google Scholar] [CrossRef]
- Stiasny, A.; Kuhn, C.; Mayr, D.; Alexiou, C.; Janko, C.; Wiest, I.; Jeschke, U.; Kost, B. Immunohistochemical Evaluation of E6/E7 HPV Oncoproteins Staining in Cervical Cancer. Anticancer Res. 2016, 36, 3195–3198. [Google Scholar]
- Hong, A.; Jones, D.; Chatfield, M.; Soon Lee, C.; Zhang, M.; Clark, J.; Elliott, M.; Harnett, G.; Milross, C.; Rose, B. HPV Status of Oropharyngeal Cancer by Combination HPV DNA/P16 Testing: Biological Relevance of Discordant Results. Ann. Surg. Oncol. 2013, 20, 450–458. [Google Scholar] [CrossRef]
- Akoglu, H. User’s Guide to Correlation Coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Saraiya, M.; Unger, E.R.; Thompson, T.D.; Lynch, C.F.; Hernandez, B.Y.; Lyu, C.W.; Steinau, M.; Watson, M.; Wilkinson, E.J.; Hopenhayn, C.; et al. US Assessment of HPV Types in Cancers: Implications for Current and 9-Valent HPV Vaccines. J. Natl. Cancer Inst. 2015, 107. [Google Scholar] [CrossRef]
- Chaturvedi, A.K.; Anderson, W.F.; Lortet-Tieulent, J.; Curado, M.P.; Ferlay, J.; Franceschi, S.; Rosenberg, P.S.; Bray, F.; Gillison, M.L. Worldwide Trends in Incidence Rates for Oral Cavity and Oropharyngeal Cancers. J. Clin. Oncol. 2013, 31, 4550–4559. [Google Scholar] [CrossRef]
- Reuschenbach, M.; Tinhofer, I.; Wittekindt, C.; Wagner, S.; Klussmann, J.P. A Systematic Review of the HPV-Attributable Fraction of Oropharyngeal Squamous Cell Carcinomas in Germany. Cancer Med. 2019, 8, 1908–1918. [Google Scholar] [CrossRef]
- Wittekindt, C.; Wagner, S.; Bushnak, A.; Prigge, E.-S.; von Knebel Doeberitz, M.; Würdemann, N.; Bernhardt, K.; Pons-Kühnemann, J.; Maulbecker-Armstrong, C.; Klussmann, J.P. Increasing Incidence Rates of Oropharyngeal Squamous Cell Carcinoma in Germany and Significance of Disease Burden Attributed to Human Papillomavirus. Cancer Prev. Res. 2019, 12, 375–382. [Google Scholar] [CrossRef]
- Lifsics, A.; Rate, E.; Ivanova, A.; Tars, J.; Murovska, M.; Groma, V. Survival Analysis of Oropharyngeal Squamous Cell Carcinoma Patients Linked to Histopathology, Disease Stage, Tumor Stage, Risk Factors, and Received Therapy. Exp. Oncol. 2020, 42, 51–59. [Google Scholar] [CrossRef]
- Kreimer, A.R.; Clifford, G.M.; Boyle, P.; Franceschi, S. Human Papillomavirus Types in Head and Neck Squamous Cell Carcinomas Worldwide: A Systematic Review. Cancer Epidemiol. Biomark. Prev. 2005, 14, 467–475. [Google Scholar] [CrossRef]
- Janecka-Widła, A.; Mucha-Małecka, A.; Majchrzyk, K.; Halaszka, K.; Przewoźnik, M.; Słonina, D.; Biesaga, B. Active HPV Infection and Its Influence on Survival in Head and Neck Squamous-Cell Cancer. J. Cancer Res. Clin. Oncol. 2020, 146, 1677–1692. [Google Scholar] [CrossRef] [PubMed]
- Jung, A.C.; Briolat, J.; Millon, R.; de Reyniès, A.; Rickman, D.; Thomas, E.; Abecassis, J.; Clavel, C.; Wasylyk, B. Biological and Clinical Relevance of Transcriptionally Active Human Papillomavirus (HPV) Infection in Oropharynx Squamous Cell Carcinoma. Int. J. Cancer 2010, 126, 1882–1894. [Google Scholar] [CrossRef] [PubMed]
- Wittekindt, C.; Wagner, S.; Sharma, S.J.; Würdemann, N.; Knuth, J.; Reder, H.; Klußmann, J.P. HPV—A Different View on Head and Neck Cancer. Laryngorhinootologie 2018, 97, S48–S113. [Google Scholar] [CrossRef]
- Ernoux-Neufcoeur, P.; Arafa, M.; Decaestecker, C.; Duray, A.; Remmelink, M.; Leroy, X.; Herfs, M.; Somja, J.; Depuydt, C.E.; Delvenne, P.; et al. Combined Analysis of HPV DNA, P16, P21 and P53 to Predict Prognosis in Patients with Stage IV Hypopharyngeal Carcinoma. J. Cancer Res. Clin. Oncol. 2011, 137, 173–181. [Google Scholar] [CrossRef]
- Brand, T.M.; Hartmann, S.; Bhola, N.E.; Li, H.; Zeng, Y.; O’Keefe, R.A.; Ranall, M.V.; Bandyopadhyay, S.; Soucheray, M.; Krogan, N.J.; et al. Cross-Talk Signaling between HER3 and HPV16 E6 and E7 Mediates Resistance to PI3K Inhibitors in Head and Neck Cancer. Cancer Res. 2018, 78, 2383–2395. [Google Scholar] [CrossRef]
- Rodrigues, L.C.; de Gois Speck, N.M.; de Azevedo Focchi, G.R.; Schimidt, M.A.; Marques, R.M.; Ribalta, J.C.L. Immunoexpression of HPV 16/18 E6 and E7 Oncoproteins in High-Grade Cervical Squamous Intraepithelial Lesions in HIV-Positive Women. Genet. Mol. Res. 2016, 15. [Google Scholar] [CrossRef]
- Phaëton, R.; Gutierrez, J.; Jiang, Z.; Karabakhtsian, R.G.; Albanese, J.; Sunkara, J.; Fisher, D.R.; Goldberg, G.L.; Dadachova, E. Naive and Radiolabeled Antibodies to E6 and E7 HPV-16 Oncoproteins Show Pronounced Antitumor Activity in Experimental Cervical Cancer. Immunotherapy 2015, 7, 631–640. [Google Scholar] [CrossRef]
- Kiyuna, A.; Ikegami, T.; Uehara, T.; Hirakawa, H.; Agena, S.; Uezato, J.; Kondo, S.; Yamashita, Y.; Deng, Z.; Maeda, H.; et al. High-Risk Type Human Papillomavirus Infection and P16 Expression in Laryngeal Cancer. Infect. Agent Cancer 2019, 14. [Google Scholar] [CrossRef]
- Jeon, S.; Lambert, P.F. Integration of Human Papillomavirus Type 16 DNA into the Human Genome Leads to Increased Stability of E6 and E7 MRNAs: Implications for Cervical Carcinogenesis. Proc. Natl. Acad. Sci. USA 1995, 92, 1654–1658. [Google Scholar] [CrossRef]
- Vojtechova, Z.; Sabol, I.; Salakova, M.; Turek, L.; Grega, M.; Smahelova, J.; Vencalek, O.; Lukesova, E.; Klozar, J.; Tachezy, R. Analysis of the Integration of Human Papillomaviruses in Head and Neck Tumours in Relation to Patients’ Prognosis. Int. J. Cancer 2016, 138, 386–395. [Google Scholar] [CrossRef]
- Reuschenbach, M.; Huebbers, C.U.; Prigge, E.-S.; Bermejo, J.L.; Kalteis, M.S.; Preuss, S.F.; Seuthe, I.M.C.; Kolligs, J.; Speel, E.-J.M.; Olthof, N.; et al. Methylation Status of HPV16 E2-Binding Sites Classifies Subtypes of HPV-Associated Oropharyngeal Cancers. Cancer 2015, 121, 1966–1976. [Google Scholar] [CrossRef]
- McBride, A.A.; Warburton, A. The Role of Integration in Oncogenic Progression of HPV-Associated Cancers. PLoS Pathog. 2017, 13. [Google Scholar] [CrossRef]
- Torrente, M.C.; Rodrigo, J.P.; Haigentz, M.; Dikkers, F.G.; Rinaldo, A.; Takes, R.P.; Olofsson, J.; Ferlito, A. Human Papillomavirus Infections in Laryngeal Cancer. Head Neck 2011, 33, 581–586. [Google Scholar] [CrossRef]
- Rosenthal, D.I.; Harari, P.M.; Giralt, J.; Bell, D.; Raben, D.; Liu, J.; Schulten, J.; Ang, K.K.; Bonner, J.A. Association of Human Papillomavirus and P16 Status With Outcomes in the IMCL-9815 Phase III Registration Trial for Patients With Locoregionally Advanced Oropharyngeal Squamous Cell Carcinoma of the Head and Neck Treated With Radiotherapy With or Without Cetuximab. J. Clin. Oncol. 2016, 34, 1300–1308. [Google Scholar] [CrossRef]
- Chung, C.H.; Zhang, Q.; Kong, C.S.; Harris, J.; Fertig, E.J.; Harari, P.M.; Wang, D.; Redmond, K.P.; Shenouda, G.; Trotti, A.; et al. P16 Protein Expression and Human Papillomavirus Status As Prognostic Biomarkers of Nonoropharyngeal Head and Neck Squamous Cell Carcinoma. J. Clin. Oncol. 2014, 32, 3930–3938. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cases (n = 72) | ||
|---|---|---|
| LSCC (n = 41) | HPSCC (n = 31) | |
| Sex: | ||
| Male | 39 | 29 |
| Female | 2 | 2 |
| Hazardous habits | ||
| Smoking | 37 | 27 |
| Excessive drinking | 8 | 7 |
| Age (median) | 64.3 | 65.9 |
| T grade: | ||
| T1 | 4 | 0 |
| T2 | 8 | 4 |
| T3 | 24 | 16 |
| T4 | 5 | 11 |
| N grade | ||
| N0 | 35 | 6 |
| N1 | 4 | 16 |
| N2 | 2 | 8 |
| N3 | 0 | 1 |
| M grade | ||
| M0 | 40 | 27 |
| M1 | 1 | 4 |
| Stage: | ||
| I | 4 | 0 |
| II | 7 | 0 |
| III | 22 | 10 |
| IV | 8 | 21 |
| Primers | Sequence (5′-3′) | Amplicon (bp) |
|---|---|---|
| β-globin primers | ||
| GS 268 | ACACAACTGTGTTCACTAGC | 200 |
| GS 269 | TGGTCTCCTTAAACCTGTCTTG | |
| Consensus primers | ||
| MY09 | CGTCC(AC)A(AG)(AG)GGA(T)ACTGATC | 450 |
| MY11 | GC(AC)CAGGG(AT)CATAA(CT)AATGG | |
| GP5+ | TTTGTTACTGTGGTAGATACTAC | 150 |
| GP6+ | GAAAAATAAACTGTAAATCATATTC | |
| Type-specific primers | ||
| 16.L1-1 | TGCTAGTGCTTATGCAGCAA | 152 |
| 16.L1-2 | ATTTACTGCAACATTGGTAC | |
| 18.1 | AAGGATGCTGCACCGGCTGA | 216 |
| 18.2 | CACGCACACGCTTGGCAGGT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lifsics, A.; Groma, V.; Cistjakovs, M.; Skuja, S.; Deksnis, R.; Murovska, M. Identification of High-Risk Human Papillomavirus DNA, p16, and E6/E7 Oncoproteins in Laryngeal and Hypopharyngeal Squamous Cell Carcinomas. Viruses 2021, 13, 1008. https://doi.org/10.3390/v13061008
Lifsics A, Groma V, Cistjakovs M, Skuja S, Deksnis R, Murovska M. Identification of High-Risk Human Papillomavirus DNA, p16, and E6/E7 Oncoproteins in Laryngeal and Hypopharyngeal Squamous Cell Carcinomas. Viruses. 2021; 13(6):1008. https://doi.org/10.3390/v13061008
Chicago/Turabian StyleLifsics, Andrejs, Valerija Groma, Maksims Cistjakovs, Sandra Skuja, Renars Deksnis, and Modra Murovska. 2021. "Identification of High-Risk Human Papillomavirus DNA, p16, and E6/E7 Oncoproteins in Laryngeal and Hypopharyngeal Squamous Cell Carcinomas" Viruses 13, no. 6: 1008. https://doi.org/10.3390/v13061008
APA StyleLifsics, A., Groma, V., Cistjakovs, M., Skuja, S., Deksnis, R., & Murovska, M. (2021). Identification of High-Risk Human Papillomavirus DNA, p16, and E6/E7 Oncoproteins in Laryngeal and Hypopharyngeal Squamous Cell Carcinomas. Viruses, 13(6), 1008. https://doi.org/10.3390/v13061008