
Impaired Humoral Response in Renal Transplant Recipients to SARS-CoV-2 Vaccination with BNT162b2 (Pfizer-BioNTech)

 , , ,
, , ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kates, O.S.; Haydel, B.M.; Florman, S.S.; Rana, M.M.; Chaudhry, Z.S.; Ramesh, M.S.; Safa, K.; Kotton, C.N.; Blumberg, E.A.; Besharatian, B.D.; et al. Coronavirus Disease 2019 in Solid Organ Transplant: A Multicenter Cohort Study. Clin. Infect. Dis. 2020, 1–14. [Google Scholar] [CrossRef]
- Hugo, C.; Stecher, M.; Dolff, S.; Nattermann, J.; Vehreschild, J.; Hippchen, T.; Westhoff, T.; Bertolo, M.; Hohenstein, B.; Hanses, F.; et al. Solid organ transplantation is not a risk factor for COVID-19 disease outcome. Transpl. Int. 2021, 34, 378–381. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.J.; Rouphael, N.G.; Widge, A.T.; Jackson, L.A.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Safety and Immunogenicity of SARS-CoV-2 mRNA-1273 Vaccine in Older Adults. N. Engl. J. Med. 2020, 383, 2427–2438. [Google Scholar] [CrossRef] [PubMed]
- Stufenplan der STIKO zur Priorisierung der COVID-19-Impfung Hinweise zum Stufenplan der STIKO zur Priorisierung der COVID-19-Impfung. Robert Koch Institute. 2021. Available online: https://www.rki.de/DE/Content/Infekt/Impfen/ImpfungenAZ/COVID-19/Stufenplan.pdf?__blob=publicationFile (accessed on 17 February 2021).
- The German Ethics Council. The National Academy of Sciences Leopoldina Position Paper of the Joint Working Group of Members of the Standing Committee on Vaccination. How should Access to a COVID-19 Vaccine be Regulated; The German Ethics Council: Berlin, Germany, 2020; pp. 1–6. [Google Scholar]
- Korth, J.; Wilde, B.; Dolff, S.; Anastasiou, O.E.; Krawczyk, A.; Jahn, M.; Cordes, S.; Ross, B.; Esser, S.; Lindemann, M.; et al. SARS-CoV-2-specific antibody detection in healthcare workers in Germany with direct contact to COVID-19 patients. J. Clin. Virol. 2020, 128, 104437. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Eckerle, I.; Rosenberger, K.D.; Zwahlen, M.; Junghanss, T. Serologic Vaccination Response after Solid Organ Transplantation: A Systematic Review. PLoS ONE 2013, 8, e56974. [Google Scholar] [CrossRef] [PubMed]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Immunogenicity of a Single Dose of SARS-CoV-2 Messenger RNA Vaccine in Solid Organ Transplant Recipients. JAMA. Available online: https://jamanetwork.com/journals/jama/article-abstract/2777685 (accessed on 15 March 2021).
- Chavarot, N.; Ouedrani, A.; Marion, O.; Leruez-Ville, M.; Villain, E.; Baaziz, M.; Del Bello, A.; Burger, C.; Sberro-Soussan, R.; Martinez, F.; et al. Poor Anti-SARS-CoV-2 Humoral and T-cell Responses After 2 Injections of mRNA Vaccine in Kidney Transplant Recipients Treated with Belatacept. Transplantation. Available online: https://journals.lww.com/transplantjournal/citation/9000/poor_anti_sars_cov_2_humoral_and_t_cell_responses.95281.aspx (accessed on 8 April 2021). [CrossRef]
- Duchini, A.; Goss, J.A.; Karpen, S.; Pockros, P.J. Vaccinations for adult solid-organ transplant recipients: Current recommendations and protocols. Clin. Microbiol. Rev. 2003, 16, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Oesterreich, S.; Lindemann, M.; Goldblatt, D.; Horn, P.A.; Wilde, B.; Witzke, O. Humoral response to a 13-valent pneumococcal conjugate vaccine in kidney transplant recipients. Vaccine 2020, 38, 3339–3350. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| rtx | HCW | ||
|---|---|---|---|
| n | 23 | 23 | p |
| female/male (n; %) | 12 (52%)/11 (48%) | 14 (61%)/9 (39%) | 0.76 |
| age (years) | 57.7 +/− 13.5 | 44.4 +/− 9.2 | 0.0003 |
| immunosuppression (n) | -- | ||
| mycophenolate n (%) | 18, (78%) | ||
| corticosteroids n (%) | 14 (60%) | ||
| tacrolimus n (%) | 14 (60%) | ||
| cyclosporine n (%) | 4 (17%) | ||
| sirolimus n (%) | 5 (22%) | ||
| everolimus n (%) | 1 (4%) | ||
| belatacept n (%) | 1 (4%) | ||
| azathioprine n (%) | 1 (4%) | ||
| years after rtx | 11.4 +/− 9.2 | -- | |
| days between first and second dose (days) | 22.0 +/− 4.6 | 22.0 +/− 0 | |
| SARS-CoV-2 Ab detection after second dose (days) | 15.8 +/− 3.0 | 13.7 +/− 1.8 | |
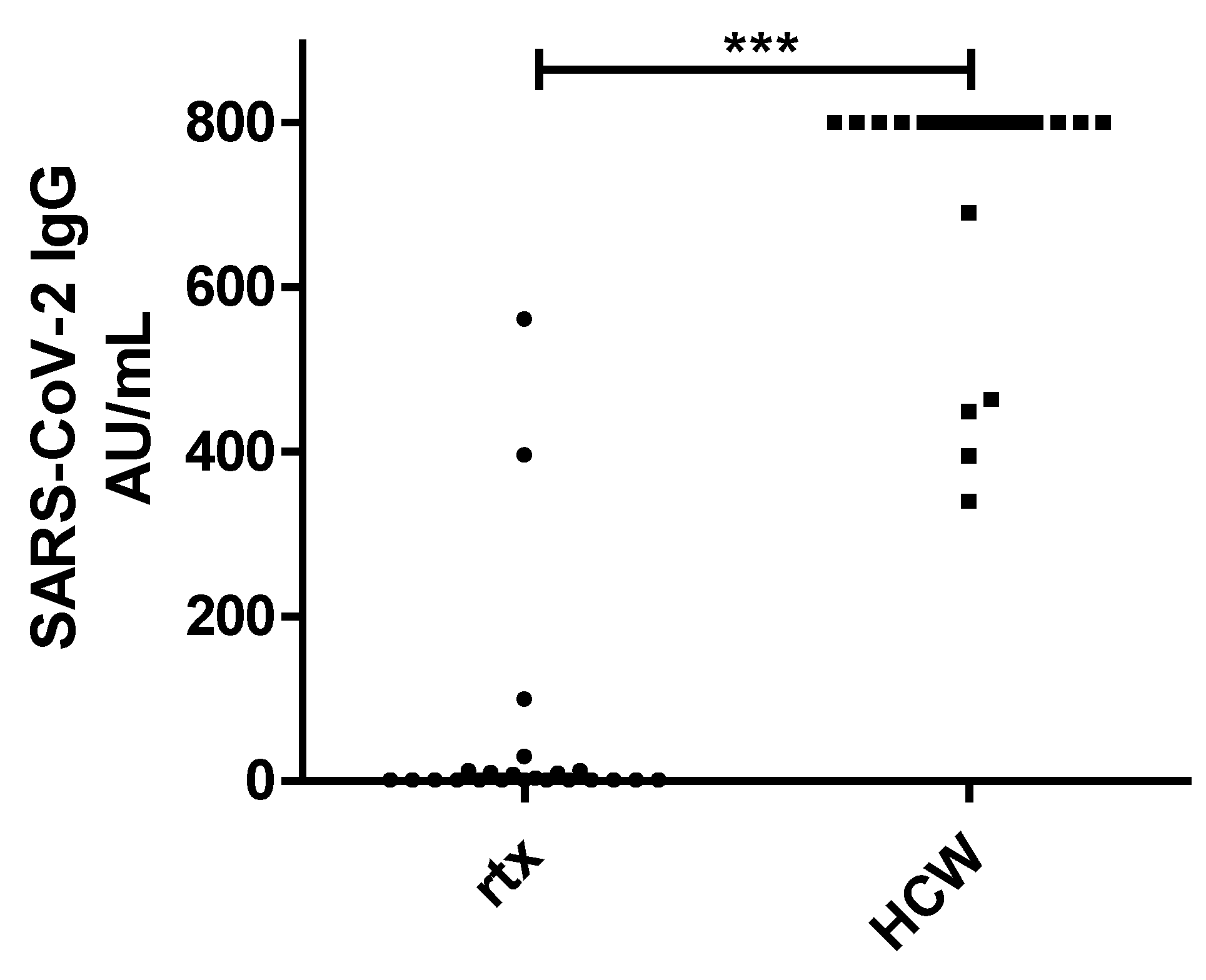
| SARS-CoV-2 Ab posCLIA (n; %) | 5 (22%) | 23 (100%) | 0.0001 |
| SARS-CoV-2 Ab negCLIA (n; %) | 18 (78%) | 0 (0%) | |
| Ab SARS-COV-2 CLIA (AU/mL) | 50.9 +/− 138.7 | 727.7 +/− 151.3 | 0.0001 |
| SARS-CoV-2 IgG Positive | SARS-CoV-2 IgG Negative | |
|---|---|---|
| n | 5 | 18 |
| female/male n (%) | 3 (60%)/2 (40%) | 9 (50%)/9 (50%) |
| age (years) | 57.0 +/− 8.1 | 57.9 +/− 14.9 |
| time after rtx (years) | 17.6 +/− 7.7 | 9.7 +/− 9.1 |
| mycophenolate n (%) | 3 (60%) | 15 (83%) |
| corticosteroids n (%) | 3 (60%) | 11 (61%) |
| tacrolimus n (%) | 2 (40%) | 12 (67%) |
| cyclosporine n (%) | 2 (40%) | 2 (11%) |
| sirolimus n (%) | 1 (20%) | 4 (22%) |
| everolimus n (%) | 1 (20%) | 0 |
| betalacept n (%) | 0 | 1 (6%) |
| azathioprine n (%) | 0 | 1 (6%) |
| number of immunosuppressive drugs n (%) | 2.4 +/− 0.5 | 2.6 +/− 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korth, J.; Jahn, M.; Dorsch, O.; Anastasiou, O.E.; Sorge-Hädicke, B.; Eisenberger, U.; Gäckler, A.; Dittmer, U.; Witzke, O.; Wilde, B.; et al. Impaired Humoral Response in Renal Transplant Recipients to SARS-CoV-2 Vaccination with BNT162b2 (Pfizer-BioNTech). Viruses 2021, 13, 756. https://doi.org/10.3390/v13050756
Korth J, Jahn M, Dorsch O, Anastasiou OE, Sorge-Hädicke B, Eisenberger U, Gäckler A, Dittmer U, Witzke O, Wilde B, et al. Impaired Humoral Response in Renal Transplant Recipients to SARS-CoV-2 Vaccination with BNT162b2 (Pfizer-BioNTech). Viruses. 2021; 13(5):756. https://doi.org/10.3390/v13050756
Chicago/Turabian StyleKorth, Johannes, Michael Jahn, Oliver Dorsch, Olympia Evdoxia Anastasiou, Burkhard Sorge-Hädicke, Ute Eisenberger, Anja Gäckler, Ulf Dittmer, Oliver Witzke, Benjamin Wilde, and et al. 2021. "Impaired Humoral Response in Renal Transplant Recipients to SARS-CoV-2 Vaccination with BNT162b2 (Pfizer-BioNTech)" Viruses 13, no. 5: 756. https://doi.org/10.3390/v13050756
APA StyleKorth, J., Jahn, M., Dorsch, O., Anastasiou, O. E., Sorge-Hädicke, B., Eisenberger, U., Gäckler, A., Dittmer, U., Witzke, O., Wilde, B., Dolff, S., & Kribben, A. (2021). Impaired Humoral Response in Renal Transplant Recipients to SARS-CoV-2 Vaccination with BNT162b2 (Pfizer-BioNTech). Viruses, 13(5), 756. https://doi.org/10.3390/v13050756