
Alcohol Consumption and Hepatitis C Virus (HCV) RNA Levels in HIV/HCV Coinfected Patients

 ,
,
Abstract
1. Introduction
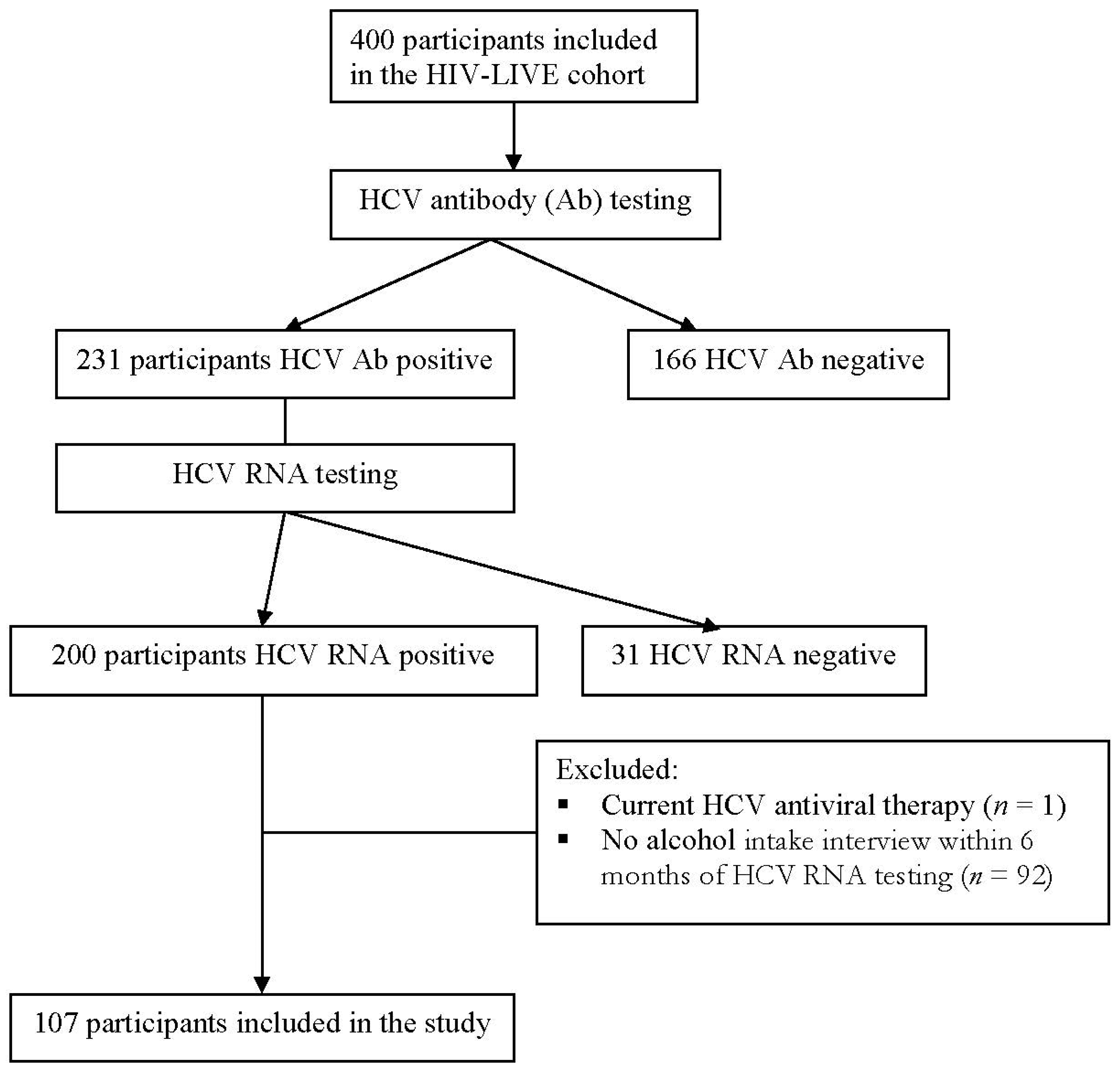
2. Subjects and Methods
2.1. Study Design
2.2. Independent Variables:
2.3. Primary Outcome
2.4. Covariates
2.5. Statistical Analyses
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Joshi, D.; O’Grady, J.; Dieterich, D.; Gazzard, B.; Agarwal, K. Increasing burden of liver disease in patients with HIV infection. Lancet 2011, 377, 1198–1209. [Google Scholar] [CrossRef]
- Alter, M.J. Epidemiology of hepatitis C virus infection. World J. Gastroenterol. 2007, 13, 2436–2441. [Google Scholar] [CrossRef] [PubMed]
- Dore, G.J.; Freeman, A.J.; Law, M.; Kaldor, J.M. Natural history models for hepatitis C-related liver disease: Different disease progression parameters for different settings. Antivir. Ther. 2003, 8, 365–372. [Google Scholar]
- Thomas, D.L.; Thio, C.L.; Martin, M.P.; Qi, Y.; Ge, D.; O’Huigin, C.; Kidd, J.; Kidd, K.; Khakoo, S.I.; Alexander, G.; et al. Genetic variation in IL28B and spontaneous clearance of hepatitis C virus. Nature 2009, 461, 798–801. [Google Scholar] [CrossRef] [PubMed]
- Hisada, M.; Chatterjee, N.; Kalaylioglu, Z.; Battjes, R.J.; Goedert, J.J. Hepatitis C virus load and survival among injection drug users in the United States. Hepatology 2005, 42, 1446–1452. [Google Scholar] [CrossRef]
- Fanning, L.; Kenny, E.; Sheehan, M.; Cannon, B.; Whelton, M.; O’Connell, J.; Collins, J.K.; Shanahan, F. Viral load and clinicopathological features of chronic hepatitis C (1b) in a homogeneous patient population. Hepatology 1999, 29, 904–907. [Google Scholar] [CrossRef] [PubMed]
- Adinolfi, L.E.; Utili, R.; Andreana, A.; Tripodi, M.F.; Marracino, M.; Gambardella, M.; Giordano, M.; Ruggiero, G. Serum HCV RNA levels correlate with histological liver damage and concur with steatosis in progression of chronic hepatitis C. Dig. Dis. Sci. 2001, 46, 1677–1683. [Google Scholar] [CrossRef] [PubMed]
- Afdhal, N.H. The natural history of hepatitis C. Semin. Liver Dis. 2004, 24 (Suppl. 2), 3–8. [Google Scholar] [CrossRef]
- Ghany, M.G.; Strader, D.B.; Thomas, D.L.; Seeff, L.B.; Diseases, A.A. For the S. of L. Diagnosis, management, and treatment of hepatitis C: An update. Hepatology 2009, 49, 1335–1374. [Google Scholar] [CrossRef]
- Poynard, T.; Ratziu, V.; Charlotte, F.; Goodman, Z.; McHutchison, J.; Albrecht, J. Rates and risk factors of liver fibrosis progression in patients with chronic hepatitis c. J. Hepatol. 2001, 34, 730–739. [Google Scholar] [CrossRef]
- Hutchinson, S.J.; Bird, S.M.; Goldberg, D.J. Influence of alcohol on the progression of hepatitis C virus infection: A meta-analysis. Clin. Gastroenterol. Hepatol. 2005, 3, 1150–1159. [Google Scholar] [CrossRef]
- Siu, L.; Foont, J.; Wands, J.R. Hepatitis C virus and alcohol. Semin. Liver Dis. 2009, 29, 188–199. [Google Scholar] [CrossRef]
- Mehta, S.H.; Genberg, B.L.; Astemborski, J.; Kavasery, R.; Kirk, G.D.; Vlahov, D.; Strathdee, S.A.; Thomas, D.L. Limited uptake of hepatitis C treatment among injection drug users. J. Community Health 2008, 33, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Le Lan, C.; Guillygomarc’h, A.; Danielou, H.; Le Dréau, G.; Lainé, F.; Védeilhié, C.; Deugnier, Y.; Brissot, P.; Guyader, D.; Moirand, R. A multi-disciplinary approach to treating hepatitis C with interferon and ribavirin in alcohol-dependent patients with ongoing abuse. J. Hepatol. 2012, 56, 334–340. [Google Scholar] [CrossRef]
- Pessione, F.; Degos, F.; Marcellin, P.; Duchatelle, V.; Njapoum, C.; Martinot-Peignoux, M.; Degott, C.; Valla, D.; Erlinger, S.; Rueff, B. Effect of alcohol consumption on serum hepatitis C virus RNA and histological lesions in chronic hepatitis C. Hepatology 1998, 27, 1717–1722. [Google Scholar] [CrossRef]
- Loguercio, C.; Di Pierro, M.; Di Marino, M.P.; Federico, A.; Disalvo, D.; Crafa, E.; Tuccillo, C.; Baldi, F.; del Vecchio Blanco, C. Drinking habits of subjects with hepatitis C virus-related chronic liver disease: Prevalence and effect on clinical, virological and pathological aspects. Alcohol Alcohol. 2000, 35, 296–301. [Google Scholar] [CrossRef]
- Anand, B.S.; Thornby, J. Alcohol has no effect on hepatitis C virus replication: A meta-analysis. Gut 2005, 54, 1468–1472. [Google Scholar] [CrossRef]
- Seronello, S.; Montanez, J.; Presleigh, K.; Barlow, M.; Park, S.B.; Choi, J. Ethanol and reactive species increase basal sequence heterogeneity of hepatitis C virus and produce variants with reduced susceptibility to antivirals. PLoS ONE 2011, 6, e27436. [Google Scholar] [CrossRef] [PubMed]
- Hahn, J.A.; Samet, J.H. Alcohol and HIV disease progression: Weighing the evidence. Curr. HIV/AIDS Rep. 2010, 7, 226–233. [Google Scholar] [CrossRef]
- Chander, G.; Josephs, J.; Fleishman, J.A.; Korthuis, P.T.; Gaist, P.; Hellinger, J.; Gebo, K.; Network, H.I.V.R. Alcohol use among HIV-infected persons in care: Results of a multi-site survey. HIV Med. 2008, 9, 196–202. [Google Scholar] [CrossRef]
- Westergaard, R.P.; Hess, T.; Astemborski, J.; Mehta, S.H.; Kirk, G.D. Longitudinal changes in engagement in care and viral suppression for HIV-infected injection drug users. AIDS 2013, 27, 2559–2566. [Google Scholar] [CrossRef]
- Korthuis, P.T.; Fiellin, D.A.; McGinnis, K.A.; Skanderson, M.; Justice, A.C.; Gordon, A.J.; Doebler, D.A.; Asch, S.M.; Fiellin, L.E.; Bryant, K.; et al. Unhealthy alcohol and illicit drug use are associated with decreased quality of HIV care. J. Acquir. Immune Defic. Syndr. 2012, 61, 171–178. [Google Scholar] [CrossRef]
- Hendershot, C.S.; Stoner, S.A.; Pantalone, D.W.; Simoni, J.M. Alcohol use and antiretroviral adherence: Review and meta-analysis. J. Acquir. Immune Defic. Syndr. 2009, 52, 180–202. [Google Scholar] [CrossRef]
- Chander, G.; Lau, B.; Moore, R.D. Hazardous alcohol use: A risk factor for non-adherence and lack of suppression in HIV infection. J. Acquir. Immune Defic. Syndr. 2006, 43, 411–417. [Google Scholar] [CrossRef]
- Samet, J.H.; Cheng, D.M.; Libman, H.; Nunes, D.P.; Alperen, J.K.; Saitz, R. Alcohol consumption and HIV disease progression. J. Acquir. Immune Defic. Syndr. 2007, 46, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Cribier, B.; Schmitt, C.; Rey, D.; Uhl, G.; Lang, J.M.; Vetter, D.; Kirn, A.; Stoll-Keller, F. HIV increases hepatitis C viraemia irrespective of the hepatitis C virus genotype. Res. Virol. 1997, 148, 267–271. [Google Scholar] [CrossRef]
- Perez-Olmeda, M.; Garcia-Samaniego, J.; Soriano, V. Hepatitis C viraemia in HIV-HCV co-infected patients having immune restoration with highly active antiretroviral therapy. AIDS 2000, 14, 212. [Google Scholar] [CrossRef] [PubMed]
- Peters, L.; Grint, D.; Lundgren, J.D.; Rockstroh, J.K.; Soriano, V.; Reiss, P.; Grzeszczuk, A.; Sambatakou, H.; Mocroft, A.; Kirk, O.; et al. HCV viremia increases the incidence of chronic kidney disease in HIV-infected patients. AIDS 2012. [Google Scholar] [CrossRef]
- Clausen, L.N.; Astvad, K.; Ladelund, S.; Larsen, M.V.; Schonning, K.; Benfield, T. Hepatitis C viral load, genotype 3 and interleukin-28B CC genotype predict mortality in HIV and hepatitis C-coinfected individuals. AIDS 2012, 26, 1509–1516. [Google Scholar] [CrossRef]
- Cooper, C.L.; Cameron, D.W. Effect of alcohol use and highly active antiretroviral therapy on plasma levels of hepatitis C virus (HCV) in patients coinfected with HIV and HCV. Clin. Infect. Dis. 2005, 41 (Suppl. 1), S105–S109. [Google Scholar] [CrossRef][Green Version]
- Fishbein, D.A.; Lo, Y.; Netski, D.; Thomas, D.L.; Klein, R.S. Predictors of hepatitis C virus RNA levels in a prospective cohort study of drug users. J. Acquir. Immune Defic. Syndr. 2006, 41, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Sulkowski, M.S.; Eron, J.J.; Wyles, D.; Trinh, R.; Lalezari, J.; Wang, C.; Slim, J.; Bhatti, L.; Gathe, J.; Ruane, P.J.; et al. Ombitasvir, Paritaprevir Co-dosed With Ritonavir, Dasabuvir, and Ribavirin for Hepatitis C in Patients Co-infected with HIV-1. JAMA 2015, 313, 1223–1231. [Google Scholar] [CrossRef]
- Tsui, J.I.; Williams, E.C.; Green, P.K.; Berry, K.; Su, F.; Ioannou, G.N. Alcohol use and hepatitis C virus treatment outcomes among patients receiving direct antiviral agents. Drug Alcohol Depend. 2016, 169, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Nunes, D.; Saitz, R.; Libman, H.; Cheng, D.M.; Vidaver, J.; Samet, J.H. Barriers to treatment of hepatitis C in HIV/HCV-coinfected adults with alcohol problems. Alcohol. Clin. Exp. Res. 2006, 30, 1520–1526. [Google Scholar] [CrossRef] [PubMed]
- AASLD-IDSA. Recommendations for Testing, Managing, and Treating Hepatitis C; AASLD-IDSA: Arlington, VA, USA, 2014. [Google Scholar]
- Samet, J.H.; Horton, N.J.; Meli, S.; Freedberg, K.A.; Palepu, A. Alcohol consumption and antiretroviral adherence among HIV-infected persons with alcohol problems. Alcohol. Clin. Exp. Res. 2004, 28, 572–577. [Google Scholar] [CrossRef]
- Smith, K.L.; Horton, N.J.; Saitz, R.; Samet, J.H. The use of the mini-mental state examination in recruitment for substance abuse research studies. Drug Alcohol Depend. 2006, 82, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Sobell, L.C.; Brown, J.; Leo, G.I.; Sobell, M.B. The reliability of the Alcohol Timeline Followback when administered by telephone and by computer. Drug Alcohol Depend. 1996, 42, 49–54. [Google Scholar] [CrossRef]
- Russell, M.; Marshall, J.R.; Trevisan, M.; Freudenheim, J.L.; Chan, A.W.; Markovic, N.; Vana, J.E.; Priore, R.L. Test-retest reliability of the cognitive lifetime drinking history. Am. J. Epidemiol. 1997, 146, 975–981. [Google Scholar] [CrossRef][Green Version]
- Kertesz, S.G.; Larson, M.J.; Horton, N.J.; Winter, M.; Saitz, R.; Samet, J.H. Homeless chronicity and health-related quality of life trajectories among adults with addictions. Med. Care 2005, 43, 574–585. [Google Scholar] [CrossRef]
- Chesney, M.A.; Ickovics, J.R.; Chambers, D.B.; Gifford, A.L.; Neidig, J.; Zwickl, B.; Wu, A.W. Self-reported adherence to antiretroviral medications among participants in HIV clinical trials: The AACTG adherence instruments. Patient Care Committee & Adherence Working Group of the Outcomes Committee of the Adult AIDS Clinical Trials Group (AACTG). AIDS Care 2000, 12, 255–266. [Google Scholar] [CrossRef]
- Kim, T.W.; Palepu, A.; Cheng, D.M.; Libman, H.; Saitz, R.; Samet, J.H. Factors associated with discontinuation of antiretroviral therapy in HIV-infected patients with alcohol problems. AIDS Care 2007, 19, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Walley, A.Y.; Cheng, D.M.; Libman, H.; Nunes, D.; Horsburgh, C.R., Jr.; Saitz, R.; Samet, J.H. Recent drug use, homelessness and increased short-term mortality in HIV-infected persons with alcohol problems. AIDS 2008, 22, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Szabo, G.; Aloman, C.; Polyak, S.J.; Weinman, S.A.; Wands, J.; Zakhari, S. Hepatitis C infection and alcohol use: A dangerous mix for the liver and antiviral immunity. Alcohol. Clin. Exp. Res. 2006, 30, 709–719. [Google Scholar] [CrossRef]
- Fuster, D.; Tor, J.; Rey-Joly, C.; Muga, R. Pathogenic interactions between alcohol and hepatitis C. Med. Clin. 2012, 138, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Fuster, D.; Samet, J.H. Alcohol Use in Patients with Chronic Liver Disease. N. Engl. J. Med. 2018, 379, 1251–1261. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Total (n = 107) | Abstinent (n = 64) | Any Use (n = 43) | p-Value |
|---|---|---|---|---|
| Age [Mean (SD)] | 43.1 (7.5) | 42.9 (7.5) | 43.5 (7.3) | 0.68 |
| Sex, male [n (%)] | 80 (75.0%) | 47 (73.4%) | 33 (76.7%) | 0.70 |
| Race [n (%)] | 0.14 | |||
| Black | 40 (37.4%) | 24 (37.5%) | 16 (37.2%) | |
| White | 40 (37.4%) | 20 (31.2%) | 20 (46.5%) | |
| Other | 27 (25.2%) | 20 (31.2%) | 7 (16.3%) | |
| Homeless [n (%)] | 32 (29.9%) | 16 (25.0%) | 16 (37.2%) | 0.18 |
| ART | <0.05 | |||
| Adherent | 52 (48.6%) | 37 (57.8%) | 15 (34.9%) | |
| Not adherent | 15 (14.0%) | 6 (9.4%) | 9 (20.9%) | |
| No ART | 40 (37.4%) | 21 (32.8%) | 19 (44.2%) | |
| Drinks per month | <0.01 | |||
| Mean (SD) | 58.3 (177.3) | 0 | 145.1 (257.7) | |
| Median (IQR) | 0 (0, 30) | 0 | 38 (12, 120) | |
| Mean log HCV RNA (SD) | 6.1 (0.8) | 6.1 (0.9) | 6.1 (0.6) | 0.73 |
| Mean log HIV RNA (SD) | 3.1 (1.4) | 2.8 (1.3) | 3.2 (1.9) | 0.03 |
| Mean CD4 (SD) [cells/mm3] | 404.9 (274.2) | 421.7 (290.3) | 381.1 (251.2) | 0.46 |
| Mean ALT (SD) [IU/L] | 65.5 (51.0) | 60.9 (50.3) | 71.2 (52.8) | 0.38 |
| Mean AST (SD) [IU/L] | 69.2 (48.4) | 64.2 (48.1) | 74.7(49.4) | 0.28 |
| Model I | Model II | Model III | ||||
|---|---|---|---|---|---|---|
| β (95% CI) | p-Value | β (95% CI) | p-Value | β (95% CI) | p-Value | |
| Alcohol measure | ||||||
| Any use vs. abstinent | −0.04 (−0.34, 0.26) | 0.79 | ||||
| Any heavy drinking day | 0.05 (−0.28, 0.38) | 0.78 | ||||
| Drinks/month * | 0.00 (−0.02, 0.03) | 0.91 | ||||
| Covariates | ||||||
| Age | 0.01 (−0.02, 0.03) | 0.62 | 0.00 (−0.02, 0.03) | 0.65 | 0.01 (−0.02, 0.03) | 0.64 |
| Female | −0.10 (−0.43, 0.24) | 0.58 | −0.09 (−0.43, 0.25) | 0.60 | −0.10 (−0.44, 0.24) | 0.58 |
| Black race | 0.16 (−0.19, 0.50) | 0.37 | 0.17 (−0.18, 0.51) | 0.35 | 0.16 (−0.18, 0.51) | 0.36 |
| Homeless | 0.15 (−0.17, 0.46) | 0.36 | 0.14 (−0.17, 0.45) | 0.37 | 0.14 (−0.17, 0.46) | 0.37 |
| CD4 | 0.00 (0.00, 0.00) | 0.49 | 0.00 (0.00, 0.00) | 0.50 | 0.00 (0.00, 0.00) | 0.49 |
| ART Adherent | 0.09 (−0.25, 0.43) | 0.61 | 0.11 (−0.24, 0.47) | 0.53 | 0.10 (−0.24, 0.43) | 0.57 |
| ART Not adherent | 0.19 (−0.26, 0.63) | 0.41 | 0.18 (−0.27, 0.63) | 0.43 | 0.18 (−0.26; 0.63) | 0.42 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fuster, D.; Nunes, D.; Cheng, D.M.; Saitz, R.; Samet, J.H. Alcohol Consumption and Hepatitis C Virus (HCV) RNA Levels in HIV/HCV Coinfected Patients. Viruses 2021, 13, 716. https://doi.org/10.3390/v13050716
Fuster D, Nunes D, Cheng DM, Saitz R, Samet JH. Alcohol Consumption and Hepatitis C Virus (HCV) RNA Levels in HIV/HCV Coinfected Patients. Viruses. 2021; 13(5):716. https://doi.org/10.3390/v13050716
Chicago/Turabian StyleFuster, Daniel, David Nunes, Debbie M. Cheng, Richard Saitz, and Jeffrey H. Samet. 2021. "Alcohol Consumption and Hepatitis C Virus (HCV) RNA Levels in HIV/HCV Coinfected Patients" Viruses 13, no. 5: 716. https://doi.org/10.3390/v13050716
APA StyleFuster, D., Nunes, D., Cheng, D. M., Saitz, R., & Samet, J. H. (2021). Alcohol Consumption and Hepatitis C Virus (HCV) RNA Levels in HIV/HCV Coinfected Patients. Viruses, 13(5), 716. https://doi.org/10.3390/v13050716