
Multisystem Inflammatory Syndrome Following SARS-CoV-2 Infection in Children: One Year after the Onset of the Pandemic in a High-Incidence Area


 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
| MIS-C | KD | ||
|---|---|---|---|
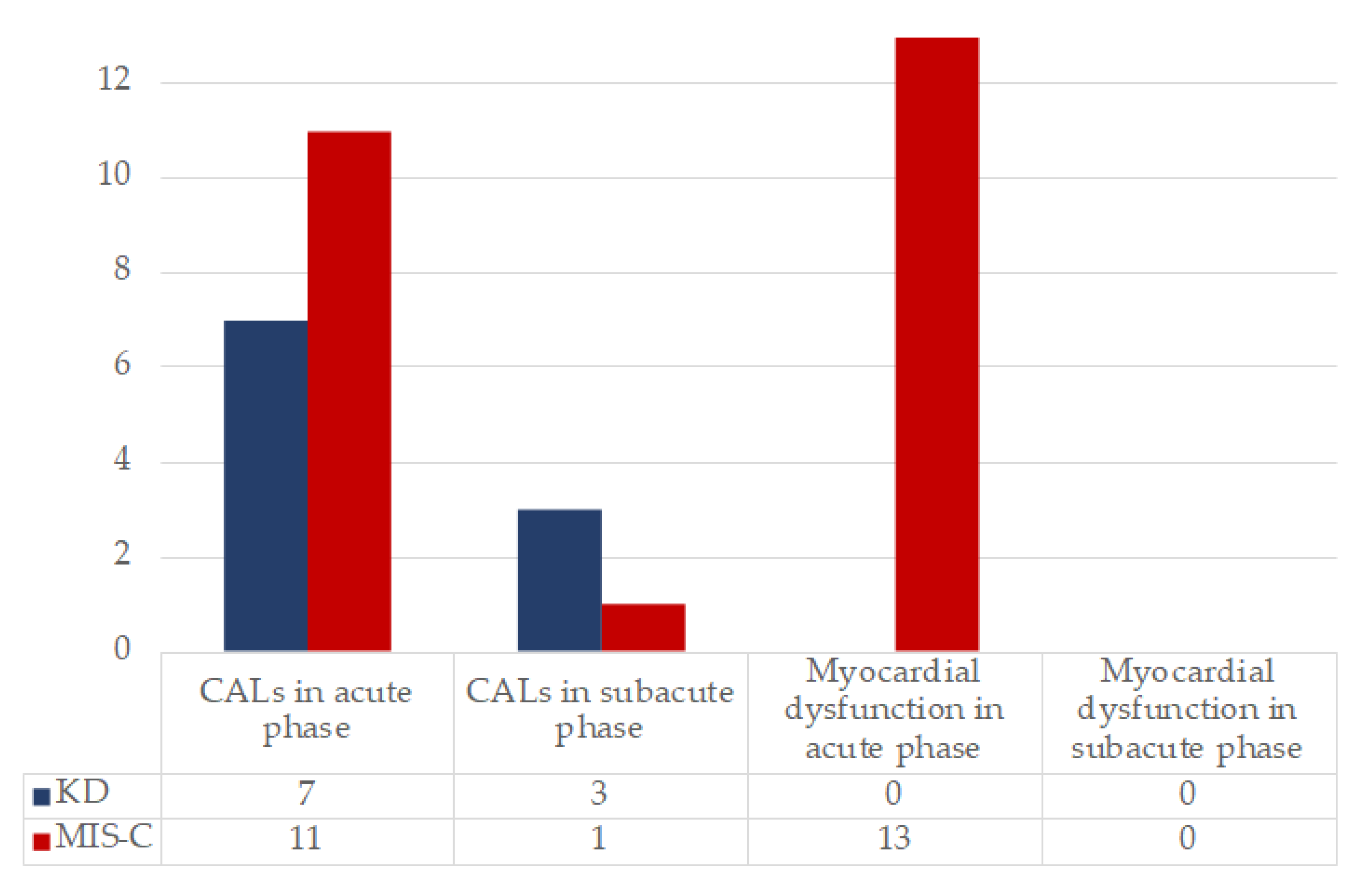
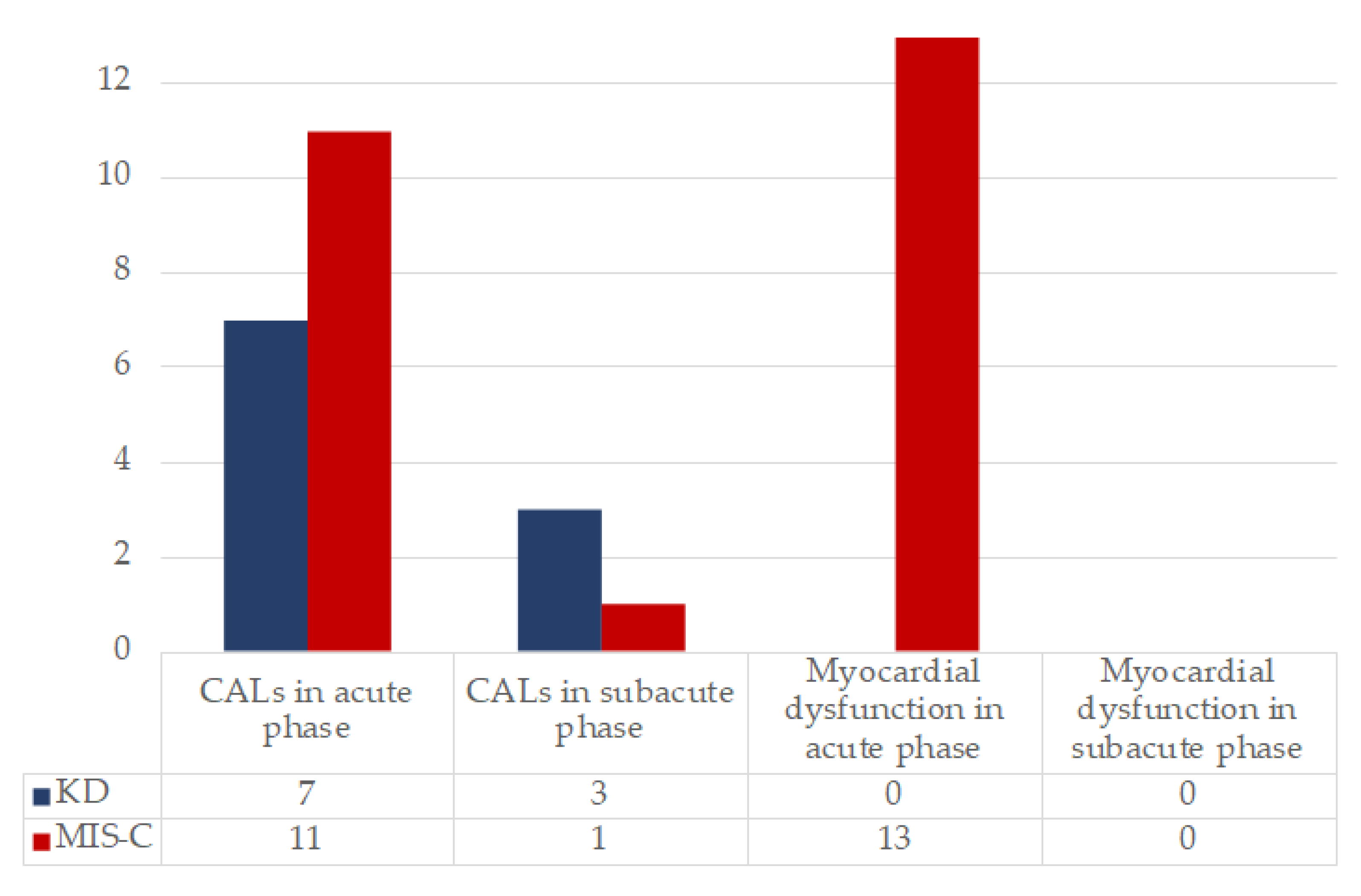
| CALs, n (%) | Dilation (2 < z-score < 2.5), n (%) | 7 (29.13%) | 3 (20%) |
| Aneurysm (z-score > 2.5), n (%) | 4 (16.66%) | 3 (20%) | |
| TTE findings | Pericardial Effusion, n (%) | 4 (16.66%) | 3 (20%) |
| Mitral/Aortic valve regurgitation, n (%) | 10 (41.66%) | 3 (20%) | |
| EF < 55%, n (%) | 11 (45.83%) | 0 | |
| Valvular regurgitation, n (%) | 10 (41.66%) | 3 (20%) | |
| Pericardial effusion | 4 (16.66%) | 3 (20%) | |
| Median EF (IQR1-IQR3) | 58 (48–64.5) | 65 (61.5–68.5) | |
| Arrhythmias, n (%) | Nonspecific ST-T repolarization abnormalities, n (%) | 3 (12.5%) | 1 (6.66%) |
| First-degree atrioventricular block, n (%) | 3 (12.5%) | 0 | |
| QT prolongation, n (%) | 1 (4.17%) | 0 | |
| Incomplete right bundle branch block, n (%) | 1 (4.17%) | 0 | |
References
- Wang, L.; Wang, Y.; Ye, D.; Liu, Q. Review of the 2019 novel coronavirus (SARS-CoV-2) based on current evidence. Int. J. Antimicrob. Agents 2020, 55, 105948. [Google Scholar] [CrossRef]
- Chen, L.; Li, X.; Chen, M.; Feng, Y.; Xiong, C. The ACE2 expression in human heart indicates new potential mechanism of heart injury among patients infected with SARS-CoV-2. Cardiovasc. Res. 2020, 116, 1097–1100. [Google Scholar] [CrossRef] [Green Version]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiological Characteristics of 2143 Pediatric Patients with 2019 Coronavirus Disease in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [Green Version]
- Shekerdemian, L.S.; Mahmood, N.R.; Wolfe, K.K.; Riggs, B.J.; Ross, C.E.; McKiernan, C.A.; Heidemann, S.M.; Kleinman, L.C.; Sen, A.I.; Hall, M.W.; et al. Characteristics and Outcomes of Children with Coronavirus Disease 2019 (COVID-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units. JAMA Pediatr. 2020, 174, 868. [Google Scholar] [CrossRef]
- Toubiana, J.; Poirault, C.; Corsia, A.; Bajolle, F.; Fourgeaud, J.; Angoulvant, F.; Debray, A.; Basmaci, R.; Salvador, E.; Biscardi, S.; et al. Outbreak of Kawasaki disease in children during COVID-19 pandemic: A prospective observational study in Paris, France. medRxiv 2020. [Google Scholar] [CrossRef]
- Verdoni, L.; Mazza, A.; Gervasoni, A.; Martelli, L.; Ruggeri, M.; Ciuffreda, M.; Bonanomi, E.; D’Antiga, L. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: An observational cohort study. Lancet 2020, 395, 1771–1778. [Google Scholar] [CrossRef]
- Viner, R.M.; Whittaker, E. Kawasaki-like disease: Emerging complication during the COVID-19 pandemic. Lancet 2020, 395, 1741–1743. [Google Scholar] [CrossRef]
- Ahmed, M.; Advani, S.; Moreira, A.; Zoretic, S.; Martinez, J.; Chorath, K.; Acosta, S.; Naqvi, R.; Burmeister-Morton, F.; Burmeister, F.; et al. Multisystem inflammatory syndrome in children: A systematic review. EClinicalMedicine 2020, 26, 100527. [Google Scholar] [CrossRef]
- HAN Archive - 00432 | Health Alert Network (HAN). Available online: https://emergency.cdc.gov/han/2020/han00432.asp (accessed on 16 May 2020).
- Multisystem Inflammatory Syndrome in Children and Adolescents with COVID-19. Available online: https://www.who.int/publications-detail/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19 (accessed on 26 May 2020).
- Rapid Risk Assessment: Paediatric Inflammatory Multisystem Syndrome and SARS -CoV-2 Infection in Children. Available online: https://www.ecdc.europa.eu/en/publications-data/paediatric-inflammatory-multisystem-syndrome-and-sars-cov-2-rapid-risk-assessment (accessed on 11 May 2021).
- Duarte-Neto, A.N.; Caldini, E.G.; Gomes-Gouvêa, M.S.; Kanamura, C.T.; de Almeida Monteiro, R.A.; Ferranti, J.F.; Ventura, A.M.C.; Regalio, F.A.; Fiorenzano, D.M.; Gibelli, M.A.B.C.; et al. An autopsy study of the spectrum of severe COVID-19 in children: From SARS to different phenotypes of MIS-C. E. Clin. Med. 2021, 35, 100850. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Sperotto, F.; Friedman, K.G.; Son, M.B.F.; VanderPluym, C.J.; Newburger, J.W.; Dionne, A. Cardiac manifestations in SARS-CoV-2-associated multisystem inflammatory syndrome in children: A comprehensive review and proposed clinical approach. Eur. J. Pediatr. 2021, 180, 307–322. [Google Scholar] [CrossRef]
- Feldstein, L.R.; Tenforde, M.W.; Friedman, K.G.; Newhams, M.; Rose, E.B.; Dapul, H.; Soma, V.L.; Maddux, A.B.; Mourani, P.M.; Bowens, C.; et al. Characteristics and Outcomes of US Children and Adolescents with Multisystem Inflammatory Syndrome in Children (MIS-C) Compared with Severe Acute COVID-19. JAMA-J. Am. Med. Assoc. 2021, 325, 1074–1087. [Google Scholar] [CrossRef]
- Sancho-Shimizu, V.; Brodin, P.; Cobat, A.; Biggs, C.M.; Toubiana, J.; Lucas, C.L.; Henrickson, S.E.; Belot, A.; Haddad, E.; Beland, K.; et al. SARS-CoV-2–related MIS-C: A key to the viral and genetic causes of Kawasaki disease? J. Exp. Med. 2021, 218. [Google Scholar] [CrossRef]
- Orenstein, J.M.; Shulman, S.T.; Fox, L.M.; Baker, S.C.; Takahashi, M.; Bhatti, T.R.; Russo, P.A.; Mierau, G.W.; Pierre De Chadaré Vian 10, J.; Perlman, E.J.; et al. Three Linked Vasculopathic Processes Characterize Kawasaki Disease: A Light and Transmission Electron Microscopic Study. PLoS ONE 2012, 7, e38998. [Google Scholar] [CrossRef] [Green Version]
- Ghelani, S.J.; Singh, S.; Manojkumar, R. Endothelial dysfunction in a cohort of North Indian children with Kawasaki disease without overt coronary artery involvement. J. Cardiol. 2009, 53, 226–231. [Google Scholar] [CrossRef] [Green Version]
- Noto, N.; Okada, T.; Karasawa, K.; Ayusawa, M.; Sumitomo, N.; Harada, K.; Mugishima, H. Age-related acceleration of endothelial dysfunction and subclinical atherosclerosis in subjects with coronary artery lesions after Kawasaki disease. Pediatr. Cardiol. 2009, 30, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Evans, P.C.; Rainger, G.E.; Mason, J.C.; Guzik, T.J.; Osto, E.; Stamataki, Z.; Neil, D.; Hoefer, I.E.; Fragiadaki, M.; Waltenberger, J.; et al. Endothelial dysfunction in COVID-19: A position paper of the ESC Working Group for Atherosclerosis and Vascular Biology, and the ESC Council of Basic Cardiovascular Science. Cardiovasc. Res. 2020, 116, 2177–2184. [Google Scholar] [CrossRef]
- Rowley, A.H. Understanding SARS-CoV-2-related multisystem inflammatory syndrome in children. Nat. Rev. Immunol. 2020, 20, 1. [Google Scholar] [CrossRef] [PubMed]
- Rowley, A.H.; Baker, S.C.; Arrollo, D.; Gruen, L.J.; Bodnar, T.; Innocentini, N.; Hackbart, M.; Cruz-Pulido, Y.E.; Wylie, K.M.; Kim, K.-Y.A.; et al. A Protein Epitope Targeted by the Antibody Response to Kawasaki Disease. J. Infect. Dis. 2020, 222, 158. [Google Scholar] [CrossRef] [PubMed]
- Esper, F.; Shapiro, E.D.; Weibel, C.; Ferguson, D.; Landry, M.L.; Kahn, J.S. Association between a Novel Human Coronavirus and Kawasaki Disease. J. Infect. Dis. 2005, 191, 499–502. [Google Scholar] [CrossRef]
- McMurray, J.C.; May, J.W.; Cunningham, M.W.; Jones, O.Y. Multisystem Inflammatory Syndrome in Children (MIS-C), a Post-viral Myocarditis and Systemic Vasculitis—A Critical Review of Its Pathogenesis and Treatment. Front. Pediatr. 2020, 8, 626182. [Google Scholar] [CrossRef]
- Consiglio, C.R.; Cotugno, N.; Sardh, F.; Pou, C.; Amodio, D.; Rodriguez, L.; Tan, Z.; Zicari, S.; Ruggiero, A.; Pascucci, G.R.; et al. The Immunology of Multisystem Inflammatory Syndrome in Children with COVID-19. Cell 2020, 183, 968–981.e7. [Google Scholar] [CrossRef]
- Cirks, B.T.; Geracht, J.C.; Jones, O.Y.; May, J.W.; Mikita, C.P.; Rajnik, M.; Helfrich, A.M. Multisystem Inflammatory Syndrome in Children during the COVID-19 Pandemic: A Case Report on Managing the Hyperinflammation. Mil. Med. 2021, 186, e270–e276. [Google Scholar] [CrossRef] [PubMed]
- Fouriki, A.; Fougère, Y.; De Camaret, C.; Blanchard Rohner, G.; Grazioli, S.; Wagner, N.; Relly, C.; Pachlopnik Schmid, J.; Trück, J.; Kottanatu, L.; et al. Case Report: Case Series of Children With Multisystem Inflammatory Syndrome following SARS-CoV-2 Infection in Switzerland. Front. Pediatr. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M.; Baker, A.L.; Jackson, M.A.; Takahashi, M.; Shah, P.B.; et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A scientific statement for health professionals from the American Heart Association. Circulation 2017, 135, e927–e999. [Google Scholar] [CrossRef]
- Dallaire, F.; Dahdah, N. New equations and a critical appraisal of coronary artery Z scores in healthy children. J. Am. Soc. Echocardiogr. 2011, 24, 60–74. [Google Scholar] [CrossRef]
- Henderson, L.A.; Canna, S.W.; Friedman, K.G.; Gorelik, M.; Lapidus, S.K.; Bassiri, H.; Behrens, E.M.; Ferris, A.; Kernan, K.F.; Schulert, G.S.; et al. American College of Rheumatology Clinical Guidance for Multisystem Inflammatory Syndrome in Children Associated With SARS-CoV-2 and Hyperinflammation in Pediatric COVID-19: Version 1. Arthritis Rheumatol. (Hoboken, N.J.) 2020, 72, 1791–1805. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, N.A.; Sochet, A.; Albisetti, M.; Biss, T.; Bonduel, M.; Jaffray, J.; MacLaren, G.; Monagle, P.; O’Brien, S.; Raffini, L.; et al. Consensus-based clinical recommendations and research priorities for anticoagulant thromboprophylaxis in children hospitalized for COVID-19–related illness. J. Thromb. Haemost. 2020, 18, 3099–3105. [Google Scholar] [CrossRef] [PubMed]
- Sirico, D.; Basso, A.; Reffo, E.; Cavaliere, A.; Castaldi, B.; Sabatino, J.; Meneghel, A.; Martini, G.; Da Dalt, L.; Zulian, F.; et al. Early Echocardiographic and Cardiac MRI Findings in Multisystem Inflammatory Syndrome in Children. J. Clin. Med. 2021, 10, 3360. [Google Scholar] [CrossRef]
- Ammirati, E.; Frigerio, M.; Adler, E.D.; Basso, C.; Birnie, D.H.; Brambatti, M.; Friedrich, M.G.; Klingel, K.; Lehtonen, J.; Moslehi, J.J.; et al. Management of Acute Myocarditis and Chronic Inflammatory Cardiomyopathy: An Expert Consensus Document. Circ. Heart Fail. 2020, 13, 663–687. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.R.; Kuo, H.C.; Lee, Y.J.; Chi, H.; Li, S.C.; Lee, H.C.; Yang, K.D. Phenotype, Susceptibility, Autoimmunity, and Immunotherapy Between Kawasaki Disease and Coronavirus Disease-19 Associated Multisystem Inflammatory Syndrome in Children. Front. Immunol. 2021, 12, 632890. [Google Scholar] [CrossRef]
- Carter, M.J.; Fish, M.; Jennings, A.; Doores, K.J.; Wellman, P.; Seow, J.; Acors, S.; Graham, C.; Timms, E.; Kenny, J.; et al. Peripheral immunophenotypes in children with multisystem inflammatory syndrome associated with SARS-CoV-2 infection. Nat. Med. 2020, 26, 1701–1707. [Google Scholar] [CrossRef]
- Azevedo, M.L.V.; Zanchettin, A.C.; Vaz de Paula, C.B.; Motta Júnior, J. da S.; Malaquias, M.A.S.; Raboni, S.M.; Neto, P.C.; Zeni, R.C.; Prokopenko, A.; Borges, N.H.; et al. Lung Neutrophilic Recruitment and IL-8/IL-17A Tissue Expression in COVID-19. Front. Immunol. 2021, 12. [Google Scholar] [CrossRef]
- Bontekoe, E.; Brailovsky, Y.; Hoppensteadt, D.; Bontekoe, J.; Siddiqui, F.; Newman, J.; Iqbal, O.; Reed, T.; Fareed, J.; Darki, A. Upregulation of Inflammatory Cytokines in Pulmonary Embolism Using Biochip-Array Profiling. Clin. Appl. Thromb. 2021, 27. [Google Scholar] [CrossRef]
- Ramaswamy, A.; Brodsky, N.N.; Sumida, T.S.; Comi, M.; Asashima, H.; Hoehn, K.B.; Li, N.; Liu, Y.; Shah, A.; Ravindra, N.G.; et al. Immune dysregulation and autoreactivity correlate with disease severity in SARS-CoV-2-associated multisystem inflammatory syndrome in children. Immunity 2021, 54, 1083–1095.e7. [Google Scholar] [CrossRef] [PubMed]
- Diorio, C.; Henrickson, S.E.; Vella, L.A.; McNerney, K.O.; Chase, J.; Burudpakdee, C.; Lee, J.H.; Jasen, C.; Balamuth, F.; Barrett, D.M.; et al. Multisystem inflammatory syndrome in children and COVID-19 are distinct presentations of SARS–CoV-2. J. Clin. Invest. 2020, 130, 5967–5975. [Google Scholar] [CrossRef] [PubMed]
- Kulcsar, K.A.; Baxter, V.K.; Greene, I.P.; Griffin, D.E. Interleukin 10 modulation of pathogenic Th17 cells during fatal alphavirus encephalomyelitis. Proc. Natl. Acad. Sci. USA 2014, 111, 16053–16058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Valle, D.M.; Kim-Schulze, S.; Huang, H.H.; Beckmann, N.D.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T.H.; Madduri, D.; Stock, A.; et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat. Med. 2020, 26, 1636–1643. [Google Scholar] [CrossRef]
- Ma, A.; Zhang, L.; Ye, X.; Chen, J.; Yu, J.; Zhuang, L.; Weng, C.; Petersen, F.; Wang, Z.; Yu, X. High Levels of Circulating IL-8 and Soluble IL-2R Are Associated With Prolonged Illness in Patients With Severe COVID-19. Front. Immunol. 2021, 12. [Google Scholar] [CrossRef]
- Anti-Interleukin-8 (Anti-IL-8) for Patients with COVID-19 —Full Text View—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04347226 (accessed on 15 May 2021).
- Reparixin in COVID-19 Pneumonia—Efficacy and Safety—Full Text View—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04794803 (accessed on 15 May 2021).
- Rojas, J.M.; Avia, M.; Martín, V.; Sevilla, N. IL-10: A multifunctional cytokine in viral infections. J. Immunol. Res. 2017, 2017, 6104054. [Google Scholar] [CrossRef] [Green Version]
- Shouval, D.S.; Biswas, A.; Goettel, J.A.; McCann, K.; Conaway, E.; Redhu, N.S.; Mascanfroni, I.D.; AlAdham, Z.; Lavoie, S.; Ibourk, M.; et al. Interleukin-10 receptor signaling in innate immune cells regulates mucosal immune tolerance and anti-inflammatory macrophage function. Immunity 2014, 40, 706–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cua, D.J.; Hutchins, B.; LaFace, D.M.; Stohlman, S.A.; Coffman, R.L. Central Nervous System Expression of IL-10 Inhibits Autoimmune Encephalomyelitis. J. Immunol. 2001, 166, 602–608. [Google Scholar] [CrossRef] [Green Version]
- Tilg, H.; Van Montfrans, C.; Van den Ende, A.; Kaser, A.; Van Deventer, S.J.H.; Schreiber, S.; Gregor, M.; Ludwiczek, O.; Rutgeerts, P.; Gasche, C.; et al. Treatment of Crohn’s disease with recombinant human interleukin 10 induces the proinflammatory cytokine interferon γ. Gut 2002, 50, 191–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puntambekar, S.S.; Bergmann, C.C.; Savarin, C.; Karp, C.L.; Phares, T.W.; Parra, G.I.; Hinton, D.R.; Stohlman, S.A. Shifting Hierarchies of Interleukin-10-Producing T Cell Populations in the Central Nervous System during Acute and Persistent Viral Encephalomyelitis. J. Virol. 2011, 85, 6702–6713. [Google Scholar] [CrossRef] [Green Version]
- Trandem, K.; Zhao, J.; Fleming, E.; Perlman, S. Highly Activated Cytotoxic CD8 T Cells Express Protective IL-10 at the Peak of Coronavirus-Induced Encephalitis. J. Immunol. 2011, 186, 3642–3652. [Google Scholar] [CrossRef]
- Loebbermann, J.; Schnoeller, C.; Thornton, H.; Durant, L.; Sweeney, N.P.; Schuijs, M.; O’Garra, A.; Johansson, C.; Openshaw, P.J. IL-10 regulates viral lung immunopathology during acute respiratory syncytial virus infection in mice. PLoS ONE 2012, 7, e32371. [Google Scholar] [CrossRef] [Green Version]
- Sikka, G.; Miller, K.L.; Steppan, J.; Pandey, D.; Jung, S.M.; Fraser, C.D.; Ellis, C.; Ross, D.; Vandegaer, K.; Bedja, D.; et al. Interleukin 10 knockout frail mice develop cardiac and vascular dysfunction with increased age. Exp. Gerontol. 2013, 48, 128–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinzenbaw, D.A.; Chu, Y.; Peña Silva, R.A.; Didion, S.P.; Faraci, F.M. Interleukin-10 protects against aging-induced endothelial dysfunction. Physiol. Rep. 2013, 1, 1–8. [Google Scholar] [CrossRef]
- Cubro, H.; Nath, K.A.; Suvakov, S.; Garcia-Valencia, O.; Parashuram, S.; White, W.M.; Weissgerber, T.L.; Nath, M.C.; Milic, N.M.; Sontag, F.; et al. Mechanisms of vascular dysfunction in the interleukin-10–deficient murine model of preeclampsia indicate nitric oxide dysregulation. Kidney Int. 2021, 99, 646–656. [Google Scholar] [CrossRef] [PubMed]
- Kakihana, Y.; Ito, T.; Nakahara, M.; Yamaguchi, K.; Yasuda, T. Sepsis-induced myocardial dysfunction: Pathophysiology and management. J. Intensive Care 2016, 4, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finkel, M.S.; Hoffman, R.A.; Shen, L.; Oddis, C.V.; Simmons, R.L.; Hattler, B.G. Interleukin-6 (IL-6) as a mediator of stunned myocardium. Am. J. Cardiol. 1993, 71, 1231–1232. [Google Scholar] [CrossRef]
- Haque, R.; Kan, H.; Finkel, M.S. Effects of cytokines and nitric oxide on myocardial E-C coupling. Basic Res. Cardiol. 1998, 93, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Rodó, X.; Curcoll, R.; Robinson, M.; Ballester, J.; Burns, J.C.; Cayan, D.R.; Lipkin, W.I.; Williams, B.L.; Couto-Rodriguez, M.; Nakamura, Y.; et al. Tropospheric winds from northeastern China carry the etiologic agent of Kawasaki disease from its source to Japan. Proc. Natl. Acad. Sci. USA 2014, 111, 7952–7957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowley, A.H.; Shulman, S.T. The Epidemiology and Pathogenesis of Kawasaki Disease. Front. Pediatr. 2018, 6, 374. [Google Scholar] [CrossRef] [Green Version]
- Burns, J.C.; Cayan, D.R.; Tong, G.; Bainto, E.V.; Turner, C.L.; Shike, H.; Kawasaki, T.; Nakamura, Y.; Yashiro, M.; Yanagawa, H. Seasonality and temporal clustering of Kawasaki syndrome. Epidemiology 2005, 16, 220–225. [Google Scholar] [CrossRef]
| Demographic Data | MIS-C | KD | p-Value | |
|---|---|---|---|---|
| Ethnicity, n (%) | Caucasian | 21 (87.50%) | 14 (93.3%) | n.s. |
| Asiatic | 1 (4.16%) | 0 (0%) | ||
| Hispanic | 0 (0%) | 0 (0%) | ||
| Others | 0 (0%) | 1 (6.6%) | ||
| African | 2 (8.33%) | 0 (0%) | ||
| Sex, n (%) | Male | 14 (58.33%) | 7 (46.66%) | n.s. |
| Female | 10 (41.67%) | 8 (53.33%) | ||
| Age in months, median (IQR1-IQR3) | 82 (59.5–108) | 27 (22.5–42.5) | 0.00 | |
| In-hospital stay, median (IQR1-IQR3) | 9 (7.25–11) | 8 (7–11) | n.s. | |
| ICU admission (%) | 11 (45.83%) | 0 (0%) | 0.003 | |
| Clinical features, n (%) | Bilateral bulbar conjunctival injection | 13 (54.17%) | 12 (80%) | n.s. |
| Erythema and edema of the hands and feet | 8 (33.3%) | 7 (46.66%) | n.s. | |
| Rash | 12 (50%) | 13 (86.66%) | 0.038 | |
| Erythema and cracking of lips/strawberry tongue/erythema of oral and pharyngeal mucosa | 10 (41.67%) | 13 (86.66%) | 0.008 | |
| Cervical lymphadenopathy | 3 (12.5%) | 12 (80%) | 0.000 | |
| Abdominal symptoms (abdominal pain, diarrhea) | 21 (87.5%) | 6 (40%) | 0.004 | |
| Respiratory symptoms (cough, respiratory failure) | 6 (25%) | 0 (0%) | n.s. | |
| Hypotension | 8 (33.33%) | 0 (0%) | 0.017 | |
| Laboratory Value | Normal Values | Group | Mean (± SD) | p-Value |
|---|---|---|---|---|
| WBC (/mmc) | 4800–12,000 | KD | 13,271.80 (±5831.09) | n.s. |
| MIS-C | 10,899.43 (±6356.01) | |||
| Lymphocytes (%) | 25.0–55.0 | KD | 20.33 (±12.03) | n.s. |
| MIS-C | 15.63 (±12.26) | |||
| Neutrophils (%) | 28.0–71.0 | KD | 71.19 (±12.94) | n.s. |
| MIS-C | 74.21 (±19.93) | |||
| Lymphocytes (/mmc) | 1800–7000 | KD | 1950.02 (±1406.84) | n.s. |
| MIS-C | 1373.32 (±1252.9) | |||
| Neutrophils (/mmc) | 1700–8500 | KD | 9452.43 (±5678.6) | n.s. |
| MIS-C | 7766.51 (±6317.94) | |||
| Platelets (/mmc) | 180,000–415,000 | KD | 326,016.93 (±144,952.74) | n.s. |
| MIS-C | 238,833.33 (±144,952.43) | |||
| ESR (mm/h) | <11 | KD | 59.45 (±22.89) | n.s. |
| MIS-C | 41.25 (±17.78) | |||
| CRP (mg/dL) | <0.5 | KD | 11.92 (±6.90) | n.s. |
| MIS-C | 18.07 (±9.53) | |||
| Procalcitonin (ng/mL) | <0.1 | KD | 7.86 (±14.16) | n.s. |
| MIS-C | 21.61 (±30.72) | |||
| IL-6 (pg/mL) | <5.9 | KD | 146.00 (±135.85) | n.s. |
| MIS-C | 140.84 (±161.43) | |||
| IL-10 (pg/mL) | <5.3 (adults) | KD | 4.78 (±3.67) | n.s. |
| MIS-C | 29.26 (±61.60) | |||
| IL-8 (pg/mL) | <70 (adults) | KD | 52.11 (±103.19) | 0.021 |
| MIS-C | 91.85 (±129.82) | |||
| TNF-alpha (pg/mL) | <8.1 (adults) | KD | 2.00 (±5.29) | n.s. |
| MIS-C | 1.11 (±1.54) | |||
| IL-1 beta (pg/mL) | <6.7 (adults) | KD | 4.57 (±10.36) | n.s. |
| MIS-C | 0.83 (±0.75) | |||
| IL-12p70 (pg/mL) | <4.7 (adults) | KD | 0.43 (±0.53) | n.s. |
| MIS-C | 0.50 (±0.58) | |||
| D-Dimer (mg/L) | <0.5 | KD | 2.18 (±1.48) | n.s. |
| MIS-C | 3.60 (±2.39) | |||
| Ferritin (ng/mL) | 25 –335 | KD | 163.60 (±58.79) | n.s. |
| MIS-C | 449.47 (±406.94) | |||
| BNP (pg/mL) | <100 | KD | 235.25 (±221.02) | n.s. |
| MIS-C | 878.38 (±1314.63) | |||
| TnI (ng/L) | <19.8 | KD | 2.67 (±2.87) | 0.026 |
| MIS-C | 684.02 (±2090.25) |
| MIS-C | KD | p-Value | |
|---|---|---|---|
| CD3+(PAN T)% | 54 (49–59.5) | 65 (54.25–67.5) | n.s. |
| CD3+/CD4+% | 32 (27.5–40.5) | 34.50 (32.25–39.75) | n.s. |
| CD3+/CD8+% | 20 (17.5–24) | 20 (14.5–21.75) | n.s. |
| CD4+/CD8+ | 1.50 (1.26–2.13) | 2.10 (1.71–2.54) | n.s. |
| CD56+/CD16+/CD3-(NK)% | 8 (5.5–13) | 6 (6–16) | n.s. |
| CD19 (PAN B) % | 33.56 (25.67–37.96) | 25.65 (20.03–27.45) | n.s. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fabi, M.; Filice, E.; Biagi, C.; Andreozzi, L.; Palleri, D.; Mattesini, B.E.; Rizzello, A.; Gabrielli, L.; Ghizzi, C.; Di Luca, D.; et al. Multisystem Inflammatory Syndrome Following SARS-CoV-2 Infection in Children: One Year after the Onset of the Pandemic in a High-Incidence Area. Viruses 2021, 13, 2022. https://doi.org/10.3390/v13102022
Fabi M, Filice E, Biagi C, Andreozzi L, Palleri D, Mattesini BE, Rizzello A, Gabrielli L, Ghizzi C, Di Luca D, et al. Multisystem Inflammatory Syndrome Following SARS-CoV-2 Infection in Children: One Year after the Onset of the Pandemic in a High-Incidence Area. Viruses. 2021; 13(10):2022. https://doi.org/10.3390/v13102022
Chicago/Turabian StyleFabi, Marianna, Emanuele Filice, Carlotta Biagi, Laura Andreozzi, Daniela Palleri, Bianca Elisa Mattesini, Alessia Rizzello, Liliana Gabrielli, Chiara Ghizzi, Daniela Di Luca, and et al. 2021. "Multisystem Inflammatory Syndrome Following SARS-CoV-2 Infection in Children: One Year after the Onset of the Pandemic in a High-Incidence Area" Viruses 13, no. 10: 2022. https://doi.org/10.3390/v13102022
APA StyleFabi, M., Filice, E., Biagi, C., Andreozzi, L., Palleri, D., Mattesini, B. E., Rizzello, A., Gabrielli, L., Ghizzi, C., Di Luca, D., Caramelli, F., De Fanti, A., & Lanari, M. (2021). Multisystem Inflammatory Syndrome Following SARS-CoV-2 Infection in Children: One Year after the Onset of the Pandemic in a High-Incidence Area. Viruses, 13(10), 2022. https://doi.org/10.3390/v13102022