


Incidence Characteristics and Histological Types of Head and Neck Cancer among Adults in Central Sudan: A Retrospective Study


Abstract
1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Ethical Considerations
3. Statistical Analysis
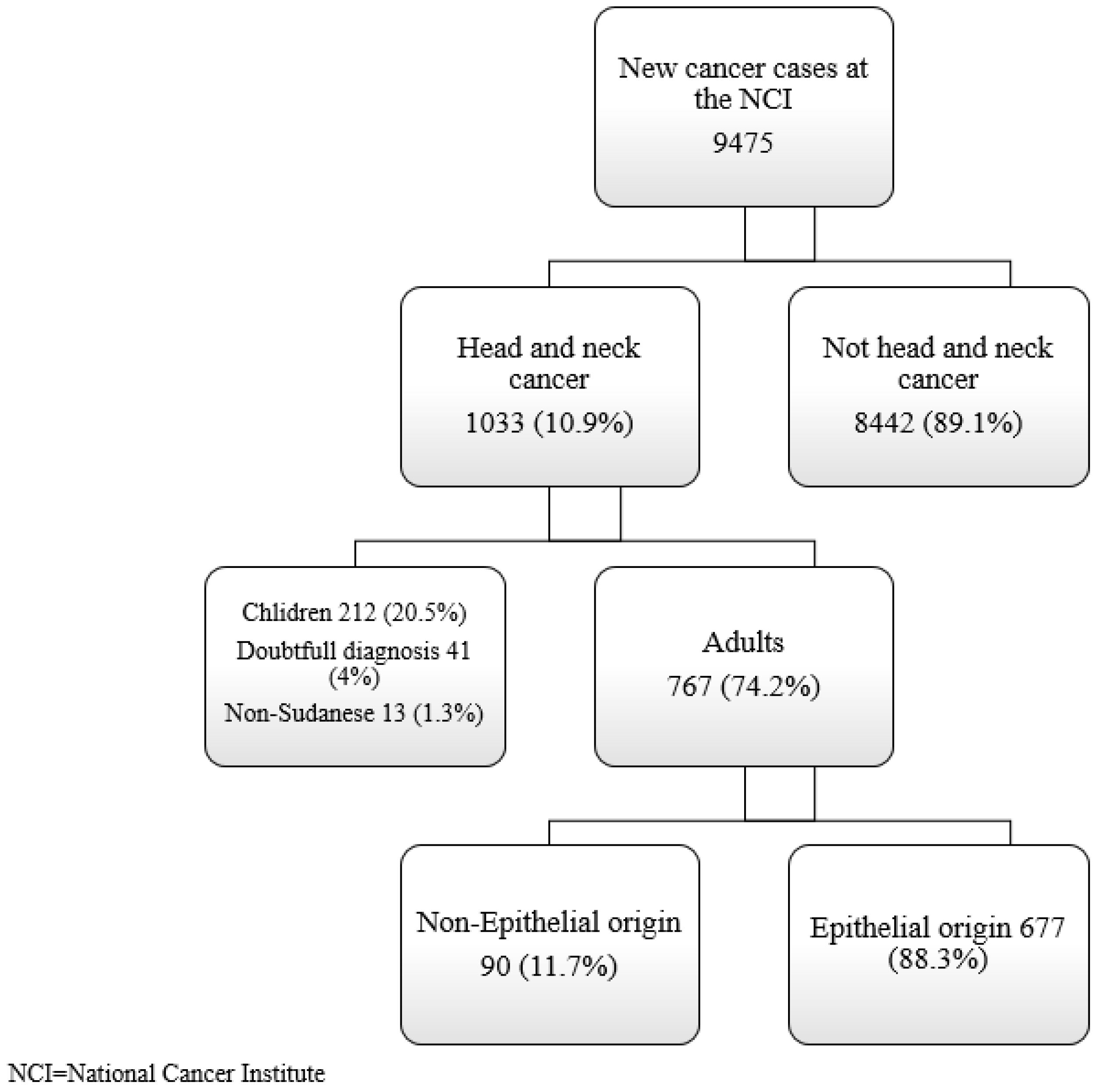
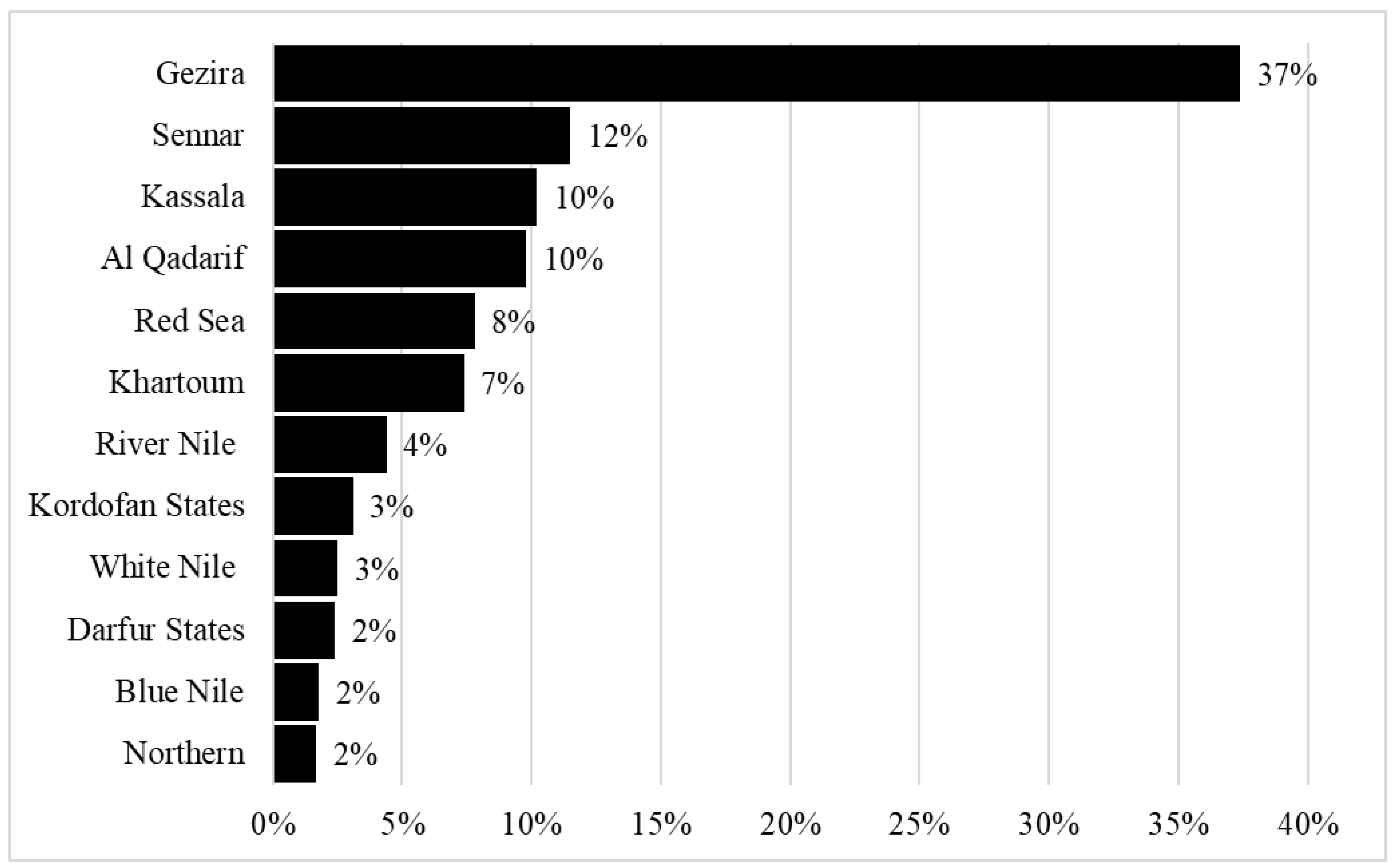
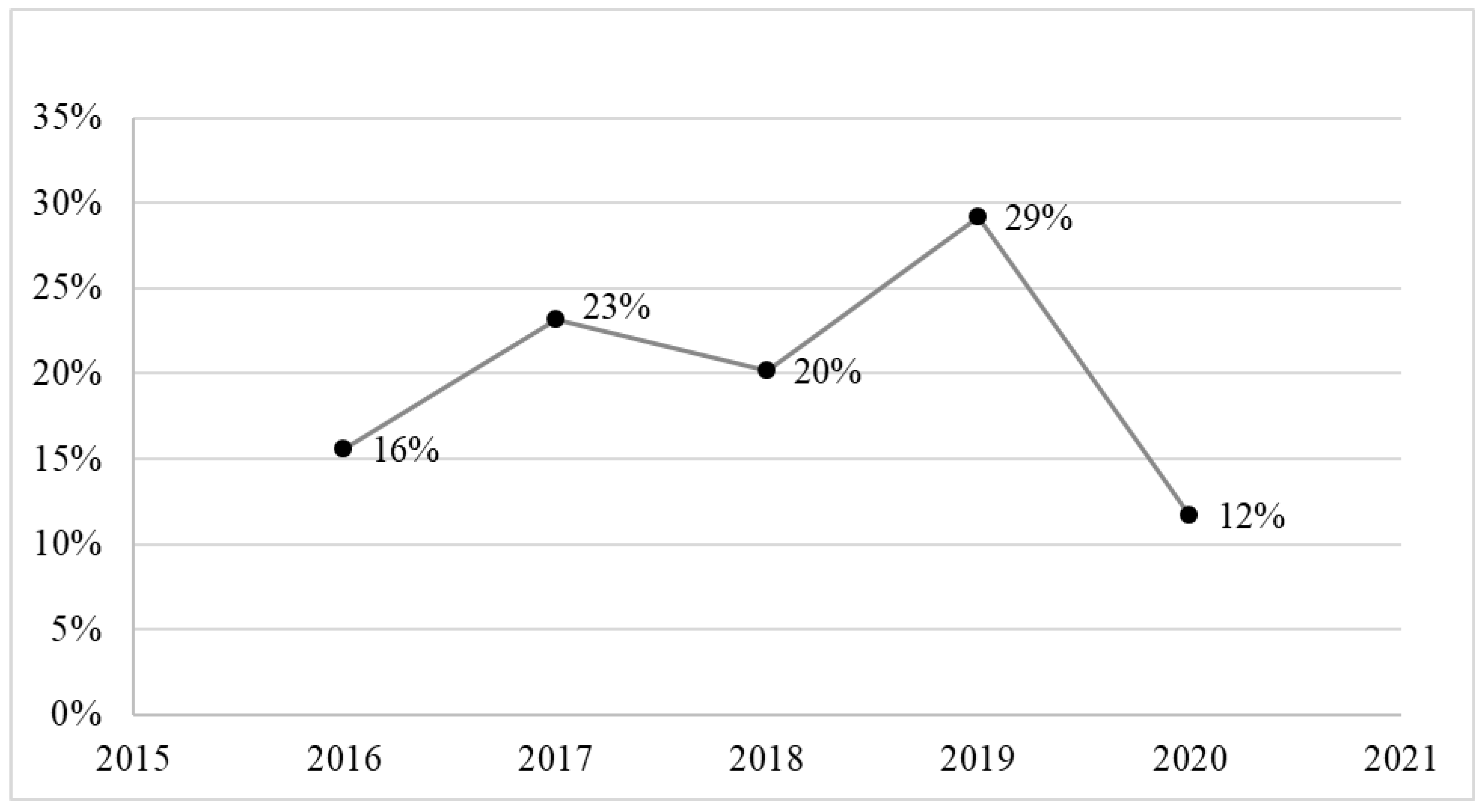
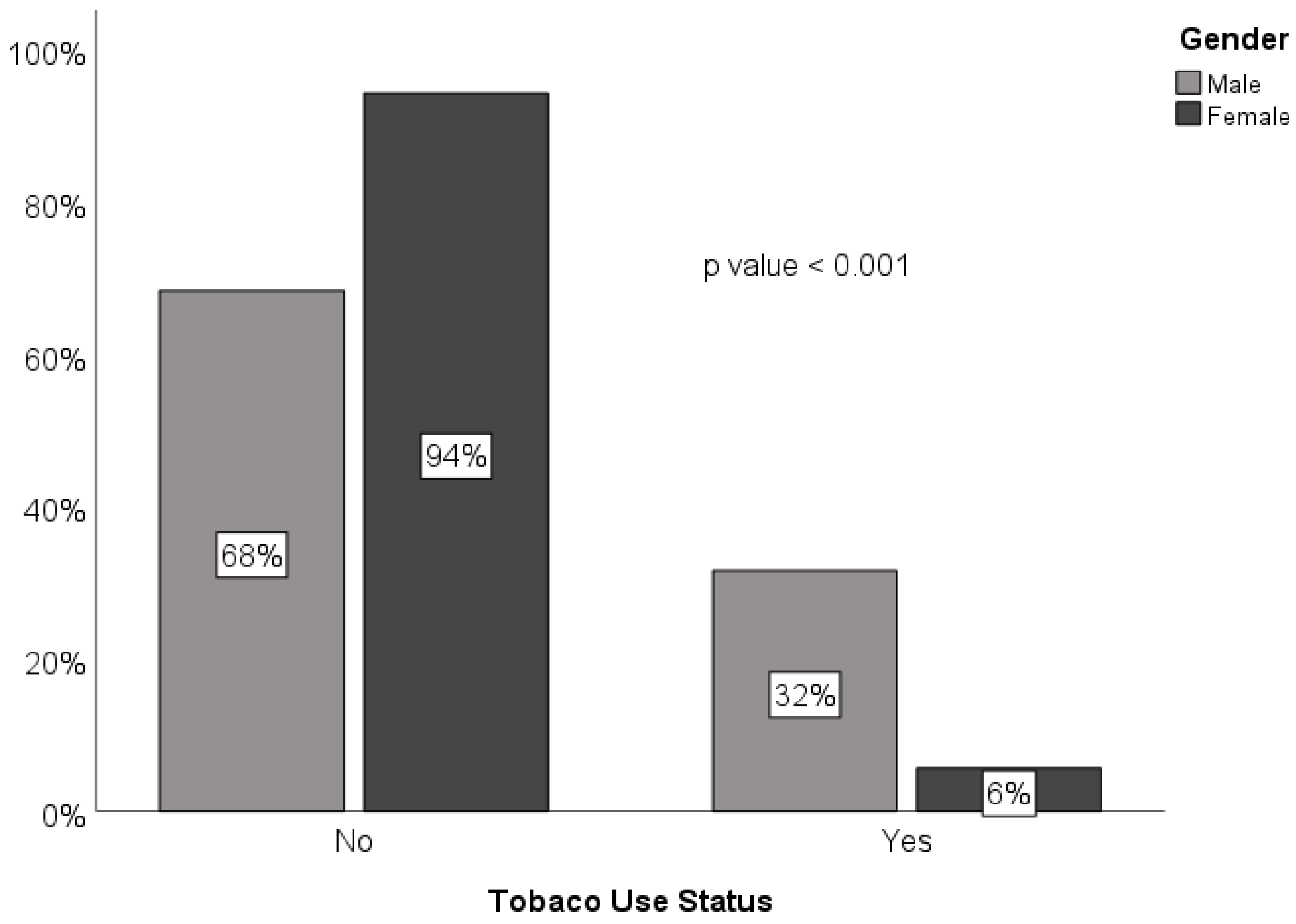
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chow, L.Q. Head and neck cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Vigneswaran, N.; Williams, M.D. Epidemiologic trends in head and neck cancer and aids in diagnosis. Oral Maxillofac. Surg. Clin. 2014, 26, 123–141. [Google Scholar] [CrossRef] [PubMed]
- Sarradin, V.; Siegfried, A.; Uro-Coste, E.; Delord, J.P. WHO classification of head and neck tumours 2017: Main novelties and update of diagnostic methods. Bull. Du Cancer 2018, 105, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Helliwell, T.R.; Giles, T.E. Pathological aspects of the assessment of head and neck cancers: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S59–S65. [Google Scholar] [CrossRef]
- Huang, S.H.; O’Sullivan, B. Overview of the 8th edition TNM classification for head and neck cancer. Curr. Treat. Options Oncol. 2017, 18, 40. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Adeola, H.A.; Afrogheh, A.H.; Hille, J.J. The burden of head and neck cancer in Africa: The status quo and research prospects. S. Afr. Dent. J. 2018, 73, 477–488. [Google Scholar] [CrossRef]
- Saeed, M.E.; Cao, J.; Fadul, B.; Kadioglu, O.; Khalid, H.E.; Yassin, Z.; Mustafa, S.M.; Saeed, E.; Efferth, T. A five-year survey of cancer prevalence in Sudan. Anticancer Res. 2016, 36, 279–286. [Google Scholar]
- Gupta, B.; Johnson, N.W.; Kumar, N. Global epidemiology of head and neck cancers: A continuing challenge. Oncology 2016, 91, 13–23. [Google Scholar] [CrossRef]
- Mourad, M.; Jetmore, T.; Jategaonkar, A.A.; Moubayed, S.; Moshier, E.; Urken, M.L. Epidemiological trends of head and neck cancer in the United States: A SEER population study. J. Oral Maxillofac. Surg. 2017, 75, 2562–2572. [Google Scholar] [CrossRef]
- Dittberner, A.; Friedl, B.; Wittig, A.; Buentzel, J.; Kaftan, H.; Boeger, D.; Mueller, A.H.; Schultze-Mosgau, S.; Schlattmann, P.; Ernst, T.; et al. Gender disparities in epidemiology, treatment, and outcome for head and neck cancer in germany: A population-based long-term analysis from 1996 to 2016 of the thuringian cancer registry. Cancers 2020, 12, 3418. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, H.G. Aetiology of oral cancer in the Sudan. J. Oral Maxillofac. Res. 2013, 4, e3. [Google Scholar] [CrossRef] [PubMed]
- Elgoni, H.E.; Mohammed, M. Tobacco Use in Sudan: Prevalence, Patterns, and Determinants—A Systematic Review. Saudi J. Health Syst. Res. 2021, 2, 1–8. [Google Scholar] [CrossRef]
- Aupérin, A. Epidemiology of head and neck cancers: An update. Curr. Opin. Oncol. 2020, 32, 178–186. [Google Scholar] [CrossRef]
- Faggons, C.E.; Mabedi, C.; Shores, C.G.; Gopal, S. Review: Head and neck squamous cell carcinoma in sub-Saharan Africa. Malawi Med. J. 2015, 27, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Rettig, E.M.; D’Souza, G. Epidemiology of head and neck cancer. Surg. Oncol. Clin. 2015, 24, 379–396. [Google Scholar] [CrossRef] [PubMed]
- Boscolo-Rizzo, P.; Zorzi, M.; Del Mistro, A.; Da Mosto, M.C.; Tirelli, G.; Buzzoni, C.; Rugge, M.; Polesel, J.; Guzzinati, S.; AIRTUM Working Group. The evolution of the epidemiological landscape of head and neck cancer in Italy: Is there evidence for an increase in the incidence of potentially HPV-related carcinomas? PLoS ONE 2018, 13, e0192621. [Google Scholar] [CrossRef]
- Tsentemeidou, A.; Fyrmpas, G.; Stavrakas, M.; Vlachtsis, K.; Sotiriou, E.; Poutoglidis, A.; Tsetsos, N. Human Papillomavirus Vaccine to End Oropharyngeal Cancer. A Systematic Review and Meta-Analysis. Sex Transm. Dis. 2021, 48, 700–707. [Google Scholar] [CrossRef]
- Blomberg, M.; Nielsen, A.; Munk, C.; Kjaer, S.K. Trends in head and neck cancer incidence in Denmark, 1978–2007: Focus on human papillomavirus associated sites. Int. J. Cancer 2011, 129, 733–741. [Google Scholar] [CrossRef]
- Kofi, B.; Mossoro-Kpinde, C.D.; Mboumba Bouassa, R.S.; Péré, H.; Robin, L.; Gresenguet, G.; Bélec, L. Infrequent detection of human papillomavirus infection in head and neck cancers in the Central African Republic: A retrospective study. Infect. Agents Cancer 2019, 14, 9. [Google Scholar] [CrossRef] [PubMed]
- Oga, E.A.; Schumaker, L.M.; Alabi, B.S.; Obaseki, D.; Umana, A.; Bassey, I.A.; Ebughe, G.; Oluwole, O.; Akeredolu, T.; Adebamowo, S.N.; et al. Paucity of HPV-related head and neck cancers (HNC) in Nigeria. PLoS ONE 2016, 11, e0152828. [Google Scholar] [CrossRef] [PubMed]
- Jalouli, J.; Ibrahim, S.O.; Sapkota, D.; Jalouli, M.M.; Vasstrand, E.N.; Hirsch, J.M.; Larsson, P.-A. Presence of human papilloma virus, herpes simplex virus and Epstein—Barr virus DNA in oral biopsies from Sudanese patients with regard to toombak use. J. Oral Pathol. Med. 2010, 39, 599–604. [Google Scholar] [CrossRef] [PubMed]
- Feng, B.J.; Khyatti, M.; Ben-Ayoub, W.; Dahmoul, S.; Ayad, M.; Maachi, F.; Bedadra, W.; Abdoun, M.; Mesli, S.; Bakkali, H.; et al. Cannabis, tobacco and domestic fumes intake are associated with nasopharyngeal carcinoma in North Africa. Br. J. Cancer 2009, 101, 1207–1212. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.T.; Ye, W.; Zeng, Y.X.; Adami, H.O. The evolving epidemiology of nasopharyngeal carcinoma. Cancer Epidemiol. Biomark. Prev. 2021, 30, 1035–1047. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, N.E.; Adam, A.A.; Khalifa, E.H.; Hassan, L.A.; Ibrahim, M.E.; Hamad, K.M.; Hassan, A.M.E. Nasopharyngeal cancer in Sudan: Epidemiology, clinical and histological characteristics. Clin. Med. Insights Ear Nose Throat 2011, 4, CMENT-S5825. [Google Scholar] [CrossRef] [PubMed]
- Adam, A.A.; Abdullah, N.E.; El Hassan, L.A.; Elamin, E.M.; Ibrahim, M.E.; El Hassan, A.M. Detection of Epstein-Barr virus in nasopharyngeal carcinoma in Sudanese by in situ hybridization. J. Cancer Ther. 2014, 2014, 45947. [Google Scholar]
- Edris, A.; Mohamed, M.A.; Mohamed, N.S.; Siddig, E.E. Molecular detection of Epstein-Barr virus in nasopharyngeal carcinoma among Sudanese population. Infect. Agents Cancer 2016, 11, 55. [Google Scholar] [CrossRef][Green Version]
- Marur, S.; Forastiere, A. Head and neck cancer: Changing epidemiology, diagnosis, and treatment. Mayo Clin. Proc. 2008, 83, 489–501. [Google Scholar] [CrossRef]
- Da Lilly-Tariah, O.B.; Somefun, A.O.; Adeyemo, W.L. Current evidence on the burden of head and neck cancers in Nigeria. Head Neck Oncol. 2009, 1, 14. [Google Scholar] [CrossRef][Green Version]
- Hounkpatin, S.H.; Brun, L.V.; Balle, M.C.; Bouraima, F.A.; Bossou, T.A.; Amegan, N.H.; Flatin, M.C.; Akélé-Akpo, M.-T. Histo-Epidemiological Profile of Head and Neck Cancers in Benin. Int. J. Otolaryngol. Head Neck Surg. 2020, 9, 19. [Google Scholar] [CrossRef]
- Joshi, P.; Dutta, S.; Chaturvedi, P.; Nair, S. Head and Neck Cancers in Developing Countries. Rambam Maimonides Med. J. 2014, 5, e0009. [Google Scholar] [CrossRef] [PubMed]
- Beaudoin, P.L.; Anchouche, S.; Gaffar, R.; Guadagno, E.; Ayad, T.; Poenaru, D. Barriers in access to Care for Patients with Head and Neck Cancer in resource-limited settings: A systematic review. JAMA Otolaryngol.-Head Neck Surg. 2020, 146, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Inverso, G.; Mahal, B.A.; Aizer, A.A.; Donoff, R.B.; Chuang, S.K. Health insurance affects head and neck cancer treatment patterns and outcomes. J. Oral Maxillofac. Surg. 2016, 74, 1241–1247. [Google Scholar] [CrossRef] [PubMed]
- Elamin, A.; Ibrahim, M.E.; Abuidris, D.; Mohamed, K.E.; Mohammed, S.I. Part I: Cancer in Sudan—Burden, distribution, and trends breast, gynecological, and prostate cancers. Cancer Med. 2015, 4, 447–456. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n (%)/Mean (± SD) |
|---|---|
| Gender | |
| Female | 318 (41.5) |
| Male | 449 (58.5) |
| Age, years | |
| Mean | 54.5 (15.8) |
| Age groups | |
| 20–29 | 62 (8.1) |
| 30–39 | 74 (9.6) |
| 40–49 | 125 (16.3) |
| 50–59 | 180 (23.5) |
| 60–69 | 167 (21.8) |
| ≥70 | 159 (20.7) |
| Residence | |
| Gezira state | 290 (37.8) |
| Outside Gezira state | 447 (62.2) |
| Occupation | |
| Professional | 50 (6.5) |
| Student | 14 (1.8) |
| Farmer | 165 (21.5) |
| Free workers | 254 (33.1) |
| Housewife | 281 (36.6) |
| Unemployed | 3 (0.4) |
| Educational level | |
| Illiterate | 427 (55.7) |
| Primary | 190 (24.8) |
| Secondary | 112 (14.6) |
| Tertiary | 38 (5) |
| Tobacco use | |
| No | 607 (79.1) |
| Yes | 160 (20.9) |
| Location (ICD-10 Codes) | n (%) | Age, Mean (SD) | Sex, M:F | Tobacco Use, n (%) * |
|---|---|---|---|---|
| Nasopharynx (C11) | 194 (25.3) | 48.5 (15.6) | 2.3:1 | 38 (19.6) |
| Hypopharynx (C13) | 175 (22.8) | 49.5 (16.1) | 1:1.7 | 13 (7.4) |
| Oral cavity (C14) | 170 (22.2) | 61 (14.3) | 1.5:1 | 53 (31.2) |
| Larynx (C32) | 124 (16.2) | 60.5 (11.7) | 4:1 | 38 (30.6) |
| Oropharynx (C10) | 66 (8.6) | 55.9 (15.5) | 1:1.5 | 11 (16.7) |
| Nasal cavity and paranasal sinus (C30, C31) | 21 (2.7) | 56.4 (16.8) | 1:1.1 | 4 (19) |
| Major Salivary Gland (C08) | 17 (2.2) | 55.6 (15.7) | 1.4:1 | 3 (17.6) |
| Total | 767 (100) | 54.5 (15.8) | 1.4:1 | 160 (20.9) |
| Clinical Characteristics | Histological Types, n (%) | ||||
|---|---|---|---|---|---|
| Carcinoma 672 (87.6) | Lymphoma 43 (5.6) | Neuroectodermal 39 (5.1) | Sarcoma 11 (1.4) | Blastoma 2 (0.3) | |
| Subtypes | |||||
| Adenocarcinoma | 6 (0.9) | – | – | – | – |
| Clear cell carcinoma | 2 (0.3) | – | – | – | – |
| Ameloblastic carcinoma | 0 (0) | – | – | – | – |
| Squamous cell carcinoma | 664 (98.8) | – | – | – | – |
| Hodgkin lymphoma | – | 1 (2.3) | – | – | – |
| Non-Hodgkin lymphoma | – | 42 (97.7) | – | – | – |
| Soft tissue sarcoma | – | – | – | 8 (72.7) | – |
| Bony sarcoma | – | – | – | 1 (9.1) | – |
| Undocumented | 0 (0) | 0 (0) | 39 (100) | 2 (18.2) | 2 (100) |
| Presenting stage | |||||
| Stage I | 41 (6.1) | 9 (20.9) | 31 (79.5) | 0 (0) | 0 (0) |
| Stage II | 73 (10.9) | 10 (23.3) | 8 (20.5) | 0 (0) | 0 (0) |
| Stage III | 160 (23.8) | 5 (11.6) | 0 (0) | 3 (27.3) | 0 (0) |
| Stage IV | 345 (51.3) | 11 (25.6) | 0 (0) | 3 (27.3) | 2 (100) |
| Undocumented | 53 (7.9) | 8 (18.6) | 0 (0) | 5 (45.4) | 0 (0) |
| Two-year survival after diagnosis | |||||
| Not survived 2 years after diagnosis | 49 (7.3) | 4 (9.3) | 0 (0) | 3 (27.3) | 0 (0) |
| Survived 2 years after diagnosis | 89 (13.2) | 7 (16.3) | 0 (0) | 1 (9.1) | 0 (0) |
| Undocumented | 534 (79.5) | 32 (74.4) | 39 (100) | 7 (63.6) | 2(100) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gebril, M.A.B.; Mukhtar, W.N.O.; Elhassan, M.M.A.; Mahmoud, I. Incidence Characteristics and Histological Types of Head and Neck Cancer among Adults in Central Sudan: A Retrospective Study. Int. J. Environ. Res. Public Health 2022, 19, 13814. https://doi.org/10.3390/ijerph192113814
Gebril MAB, Mukhtar WNO, Elhassan MMA, Mahmoud I. Incidence Characteristics and Histological Types of Head and Neck Cancer among Adults in Central Sudan: A Retrospective Study. International Journal of Environmental Research and Public Health. 2022; 19(21):13814. https://doi.org/10.3390/ijerph192113814
Chicago/Turabian StyleGebril, Marwa Ahmed Balila, Wail Nuri Osman Mukhtar, Moawia Mohammed Ali Elhassan, and Ibrahim Mahmoud. 2022. "Incidence Characteristics and Histological Types of Head and Neck Cancer among Adults in Central Sudan: A Retrospective Study" International Journal of Environmental Research and Public Health 19, no. 21: 13814. https://doi.org/10.3390/ijerph192113814
APA StyleGebril, M. A. B., Mukhtar, W. N. O., Elhassan, M. M. A., & Mahmoud, I. (2022). Incidence Characteristics and Histological Types of Head and Neck Cancer among Adults in Central Sudan: A Retrospective Study. International Journal of Environmental Research and Public Health, 19(21), 13814. https://doi.org/10.3390/ijerph192113814