
Effects of Augmented Reality Game-Based Cognitive–Motor Training on Restricted and Repetitive Behaviors and Executive Function in Patients with Autism Spectrum Disorder

 ,
, 


 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethics Statement and Trial Registration
2.3. Study Participants
2.4. Randomization and Blinding
2.5. Experiment Procedures
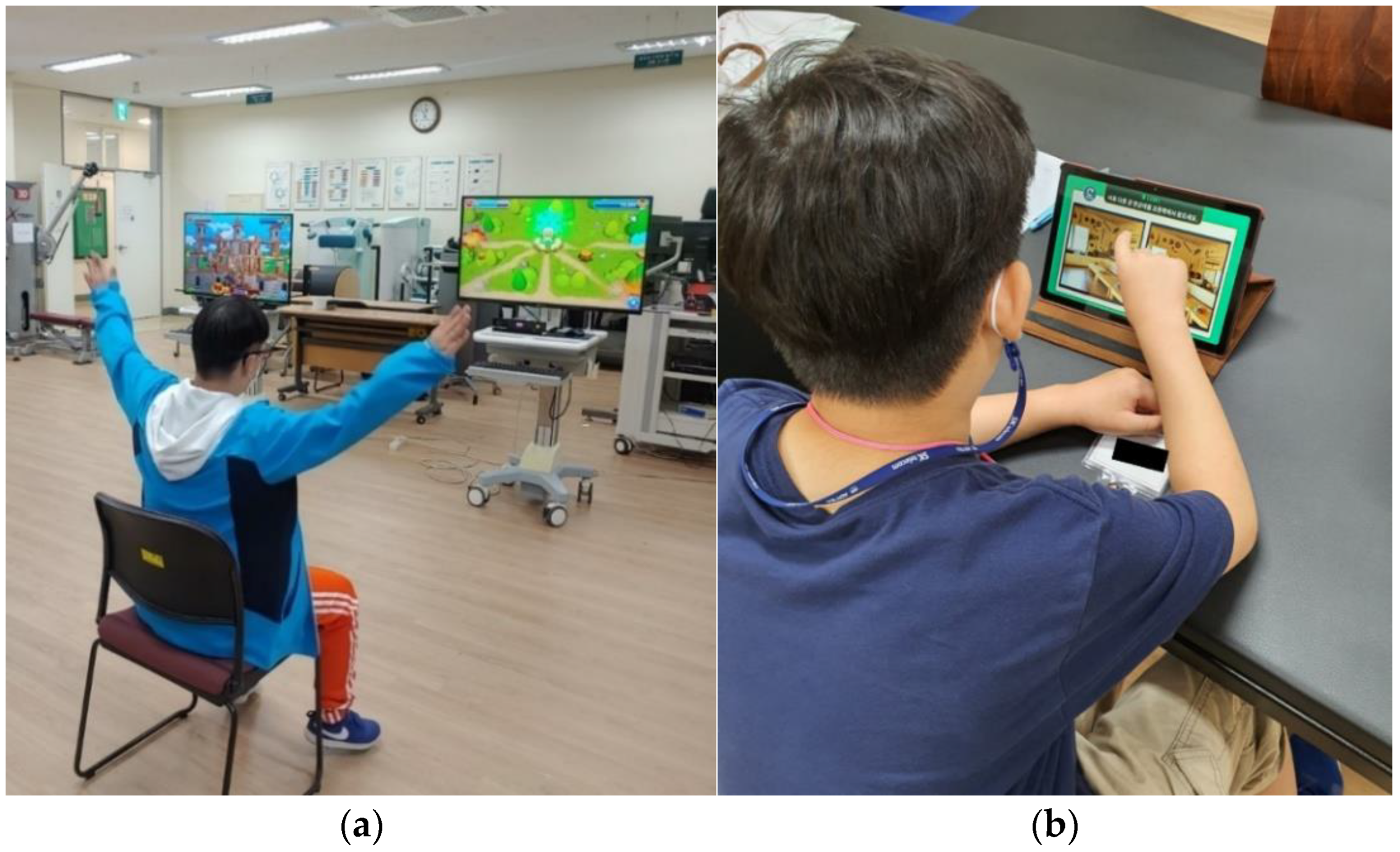
2.5.1. Study Group
2.5.2. Control Group
2.6. Outcome Measurements
2.6.1. RRBs
2.6.2. EF and Reaction Time
2.7. Data Analysis
3. Results
3.1. RRBs
3.2. EF and Reaction Time
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-V), 5th ed.; American Psychiatric Publishing: Arlington, TX, USA, 2013. [Google Scholar]
- Centers for Disease Control and Prevention. Prevalence of Autism Spectrum Disorders-Autism and Developmental Disabilities Monitoring Network, United States, 2006; Morbidity and mortality weekly report. Surveillance summaries; Centers for Disease Control and Prevention: Washington, DC, USA, 2009; Volume 58, pp. 1–20. [Google Scholar]
- Kim, Y.S.; Leventhal, B.L.; Koh, Y.J.; Fombonne, E.; Laska, E.; Lim, E.C.; Cheon, K.A.; Kim, S.J.; Kim, Y.K.; Lee, H.; et al. Prevalence of autism spectrum disorders in a total population sample. Am. J. Psychiatry 2011, 168, 904–912. [Google Scholar] [CrossRef] [PubMed]
- Courchesne, E.; Allen, G. Prediction and preparation, fundamental functions of the cerebellum. Learn. Mem. 1997, 4, 1–35. [Google Scholar] [CrossRef] [PubMed]
- Lopez, B.R.; Lincoln, A.J.; Ozonoff, S.; Lai, Z. Examining the relationship between executive functions and restricted, repetitive symptoms of autistic disorder. J. Autism Dev. Disord. 2005, 35, 445–460. [Google Scholar] [CrossRef] [PubMed]
- Turner, M. Annotation: Repetitive behaviour in autism: A review of psychological research. J. Child Psychol. Psychiatry Allied Discip. 1999, 40, 839–849. [Google Scholar] [CrossRef]
- Roselló, B.; Berenguer, C.; Navío, P.; Baixauli, I.; Miranda, A. Executive functioning, social cognition, pragmatics, and social interaction in attention deficit hyperactivity disorder and autism spectrum disorder. Curr. Dev. Disord. Rep. 2017, 4, 72–77. [Google Scholar] [CrossRef]
- Hill, E.L. Evaluating the theory of executive dysfunction in autism. Dev. Rev. 2004, 24, 189–233. [Google Scholar] [CrossRef]
- Petrus, C.; Adamson, S.R.; Block, L.; Einarson, S.J.; Sharifnejad, M.; Harris, S.R. Effects of exercise interventions on stereotypic behaviours in children with autism spectrum disorder. Physiother. Can. 2008, 60, 134–145. [Google Scholar] [CrossRef]
- Lang, R.; Koegel, L.K.; Ashbaugh, K.; Regester, A.; Ence, W.; Smith, W. Physical exercise and individuals with autism spectrum disorders: A systematic review. Res. Autism Spectr. Disord. 2010, 4, 565–576. [Google Scholar] [CrossRef]
- Ji, C.; Yang, J.; Lin, L.; Chen, S. Executive Function Improvement for Children with Autism Spectrum Disorder: A Comparative Study between Virtual Training and Physical Exercise Methods. Children 2022, 9, 507. [Google Scholar] [CrossRef]
- Tse, A.N.; Anderson, D.A.; Liu, V.E.; Tsui, S.H. Improving Executive Function of Children with Autism Spectrum Disorder through Cycling Skill Acquisition. Med. Sci. Sport Exer. 2021, 53, 1417–1424. [Google Scholar] [CrossRef]
- Park, J.H.; Park, J.H. A randomized controlled trial of the computer-based cognitive rehabilitation program for children (CoTras-C) to examine cognitive function and visual perception in children with developmental disabilities. J. Phys. Ther. Sci. 2015, 27, 3623–3626. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Choi, Y.I. Effects of a computerized cognitive training on cognitive, depression, life satisfaction and activity of daily living in older adults with mild dementia. J. Korea Acad.-Ind. Coop. Soc. 2019, 20, 311–319. [Google Scholar]
- Lee, J.S.; Kim, S.W. Effects of Korean Computer-Based Cognitive Rehabilitation Program on the Memory in Healthy Elderly. J. Int. Acad. Phys. Ther. Res. 2018, 9, 1591–1595. [Google Scholar] [CrossRef]
- Jang, C.; Bae, W.S. The Effect of Computerized Cognitive Program on Cognitive Function and Activities of Daily Living of Stroke Patients. J. Korean Soc. Integr. Med. 2021, 9, 49–58. [Google Scholar]
- Kim, M.; Park, J.; Lee, N. The effect of the computer-based cognitive rehabilitation program (CoTras) on the cognitive function and daily living activities of elderly stroke patients. J. Korean Soc. Integr. Med. 2020, 8, 121–130. [Google Scholar]
- Han, S.H.; Jo, E.J.; Noh, D.H.; Kam, K.Y. Effects of Korean Computer-Based Cognitive Rehabilitation Program (CoTras) on Frontal-Executive Functions in Patients with Traumatic Brain Injury. J. Korea Acad.-Ind. Coop. Soc. 2015, 16, 3344–3352. [Google Scholar]
- Wolff, J.J.; Boyd, B.A.; Elison, J.T. A quantitative measure of restricted and repetitive behaviors for early childhood. J. Neurodev. Disord. 2016, 8, 27. [Google Scholar] [CrossRef]
- Gualtieri, C.T.; Johnson, L.G. Reliability and validity of a computerized neurocognitive test battery, CNS Vital Signs. Arch. Clin. Neuropsychol. 2006, 21, 623–643. [Google Scholar] [CrossRef]
- Dong, Y.; Thompson, C.L.; Tan, S.H.; Lim, L.B.; Pang, W.; Chen, C.L. Test-retest reliability, convergent validity and practice effects of the RBANS in a memory clinic setting: A pilot study. Open J. Med. Psychol. 2013, 2, 11. [Google Scholar] [CrossRef]
- Kopp, B.; Lange, F.; Steinke, A. The reliability of the Wisconsin card sorting test in clinical practice. Assessment 2021, 28, 248–263. [Google Scholar] [CrossRef]
- Homack, S.; Riccio, C.A. A meta-analysis of the sensitivity and specificity of the Stroop Color and Word Test with children. Arch. Clin. Neuropsychol. 2004, 19, 725–743. [Google Scholar] [CrossRef] [PubMed]
- Bachman, J.E.; Fuqua, R.W. Management of inappropriate behaviors of trainable mentally impaired students using antecedent exercise. J. Appl. Behav. Anal. 1983, 16, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Rapp, J.T.; Vollmer, T.R.; St Peter, C.; Dozier, C.L.; Cotnoir, N.M. Analysis of response allocation in individuals with multiple forms of stereotyped behavior. J. Appl. Behav. Anal. 2004, 37, 481–501. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K.; Prinstein, M.J. Contextual features and behavioral functions of self-mutilation among adolescents. J. Abnorm. Psychol. 2005, 114, 140. [Google Scholar] [CrossRef]
- Nock, M.K.; Mendes, W.B. Physiological arousal, distress tolerance, and social problem-solving deficits among adolescent self-injurers. J. Consult. Clin. Psychol. 2008, 76, 28. [Google Scholar] [CrossRef]
- Selby, E.A.; Nock, M.K.; Kranzler, A. How does self-injury feel? Examining automatic positive reinforcement in adolescent self-injurers with experience sampling. Psychiatry Res. 2014, 215, 417–423. [Google Scholar] [CrossRef]
- Jacob, S.; Landeros-Weisenberger, A.; Leckman, J.F. Autism spectrum and obsessive–compulsive disorders: OC behaviors, phenotypes and genetics. Autism Res. 2009, 2, 293–311. [Google Scholar] [CrossRef]
- Minshew, N.J.; Williams, D.L. The new neurobiology of autism: Cortex, connectivity, and neuronal organization. Arch. Neurol. 2007, 64, 945–950. [Google Scholar] [CrossRef]
- Holschneider, D.P.; Yang, J.; Guo, Y.; Maarek, J.M. Reorganization of functional brain maps after exercise training: Importance of cerebellar–thalamic–cortical pathway. Brain Res. 2007, 1184, 96–107. [Google Scholar] [CrossRef]
- Rafiei Milajerdi, H.; Sheikh, M.; Najafabadi, M.G.; Saghaei, B.; Naghdi, N.; Dewey, D. The effects of physical activity and exergaming on motor skills and executive functions in children with autism spectrum disorder. Games Health J. 2021, 10, 33–42. [Google Scholar] [CrossRef]
- Anderson-Hanley, C.; Tureck, K.; Schneiderman, R.L. Autism and exergaming: Effects on repetitive behaviors and cognition. Psychol. Res. Behav. Manag. 2011, 4, 129. [Google Scholar] [CrossRef] [PubMed]
- Bremer, E.; Graham, J.D.; Heisz, J.J.; Cairney, J. Effect of acute exercise on prefrontal oxygenation and inhibitory control among male children with autism spectrum disorder: An exploratory study. Front. Behav. Neurosci. 2020, 14, 84. [Google Scholar] [CrossRef] [PubMed]
- Friedman, N.P.; Robbins, T.W. The role of prefrontal cortex in cognitive control and executive function. Neuropsychopharmacology 2022, 47, 72–89. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, J.; Vogel, E.K.; Lansner, A.; Bergström, F.; Nyberg, L. Neurocognitive architecture of working memory. Neuron 2015, 88, 33–46. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Study Group (n = 12) | Control Group (n = 12) | p |
|---|---|---|---|
| Male/Female (%) | 10/2 (83/17) | 12/0 (100/0) | - |
| Age (years) | 14.42 ± 5.14 | 14.17 ± 5.09 | 0.977 |
| Height (cm) | 155.42 ± 11.64 | 153.42 ± 11.75 | 0.525 |
| Weight (kg) | 53.42 ± 9.52 | 53.33 ± 11.33 | 0.840 |
| AMSE (points) | 3.33 ± 1.30 | 3.58 ± 1.31 | 0.651 |
| Variables | Study Group (n = 12) | Control Group (n = 12) | Mixed 2 × 2 ANOVA | ||||
|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | Pre-Test | Post-Test | p | Time F-Value | Time × Group F-Value | |
| Stereotypic behavior (points) | 5.50 ± 1.00 | 4.75 ± 1.05 * | 5.92 ± 1.24 | 5.50 ± 1.67 | 0.215 | 11.846 ** | 0.967 |
| Self-injury behavior (points) | 1.75 ± 0.75 | 1.25 ± 0.86 | 1.83 ± 0.83 | 1.33 ± 1.07 | 0.778 | 7.333 * | 0.000 *** |
| Compulsive behavior (points) | 3.50 ± 1.00 | 2.83 ± 1.33 * | 4.00 ± 1.34 | 3.42 ± 1.50 * | 0.749 | 15.184 ** | 0.067 |
| Ritualistic behavior (points) | 7.00 ± 1.12 | 6.33 ± 1.72 | 6.83 ± 1.11 | 6.25 ± 1.48 | 0.833 | 8.756 ** | 0.039 * |
| Sameness behavior (points) | 8.50 ± 0.90 | 7.67 ± 1.15 * | 8.92 ± 1.37 | 8.58 ± 1.73 | 0.289 | 8.045 * | 1.478 |
| Restricted behavior (points) | 3.50 ± 0.90 | 2.50 ± 1.44 * | 3.75 ± 1.21 | 3.08 ± 1.50 * | 0.426 | 13.750 ** | 0.550 |
| Variables | Study Group (n = 12) | Control Group (n = 12) | Mixed 2 × 2 ANOVA | |||||
|---|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | Pre-Test | Post-Test | p | Time F-Value | Time × Group F-Value | ||
| Working memory (points) | 13.92 ± 1.50 | 13.92 ± 1.50 * | 14.08 ± 1.83 | 15.17 ± 1.19* | 0.977 | 11.407 ** | 0.016 | |
| Cognitive Flexibility | RT (milliseconds) | 1102.08 ± 5.46 | 1092.25 ± 5.15 ** | 1102.00 ± 5.20 | 1098.58 ± 5.12* | 0.016 | 30.630 *** | 7.184 * |
| AR (points) | 79.08 ± 3.02 | 84.83 ± 2.40 ** | 79.25 ± 4.11 | 81.92 ± 2.42 * | 0.043 | 12.950 ** | 6.349 * | |
| Cognitive Inhibition | RT (milliseconds) | 1104.92 ± 8.17 | 1102.17 ± 7.34 * | 1104.83 ± 5.13 | 1104.25 ± 5.17 | 0.045 | 12.308 ** | 5.200 * |
| AR (points) | 76.08 ± 2.06 | 84.33 ± 2.10 ** | 76.33 ± 3.79 | 81.08 ± 2.42 * | 0.042 | 14.503 ** | 4.351 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nekar, D.M.; Lee, D.-Y.; Hong, J.-H.; Kim, J.-S.; Kim, S.-G.; Seo, Y.-G.; Yu, J.-H. Effects of Augmented Reality Game-Based Cognitive–Motor Training on Restricted and Repetitive Behaviors and Executive Function in Patients with Autism Spectrum Disorder. Healthcare 2022, 10, 1981. https://doi.org/10.3390/healthcare10101981
Nekar DM, Lee D-Y, Hong J-H, Kim J-S, Kim S-G, Seo Y-G, Yu J-H. Effects of Augmented Reality Game-Based Cognitive–Motor Training on Restricted and Repetitive Behaviors and Executive Function in Patients with Autism Spectrum Disorder. Healthcare. 2022; 10(10):1981. https://doi.org/10.3390/healthcare10101981
Chicago/Turabian StyleNekar, Daekook M., Dong-Yeop Lee, Ji-Heon Hong, Jin-Seop Kim, Seong-Gil Kim, Yong-Gon Seo, and Jae-Ho Yu. 2022. "Effects of Augmented Reality Game-Based Cognitive–Motor Training on Restricted and Repetitive Behaviors and Executive Function in Patients with Autism Spectrum Disorder" Healthcare 10, no. 10: 1981. https://doi.org/10.3390/healthcare10101981
APA StyleNekar, D. M., Lee, D.-Y., Hong, J.-H., Kim, J.-S., Kim, S.-G., Seo, Y.-G., & Yu, J.-H. (2022). Effects of Augmented Reality Game-Based Cognitive–Motor Training on Restricted and Repetitive Behaviors and Executive Function in Patients with Autism Spectrum Disorder. Healthcare, 10(10), 1981. https://doi.org/10.3390/healthcare10101981