
County-Level Life Expectancy Change: A Novel Metric for Monitoring Public Health

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview
2.2. Data Sources
2.3. Life Expectancy
2.4. Statistical Analysis
3. Results
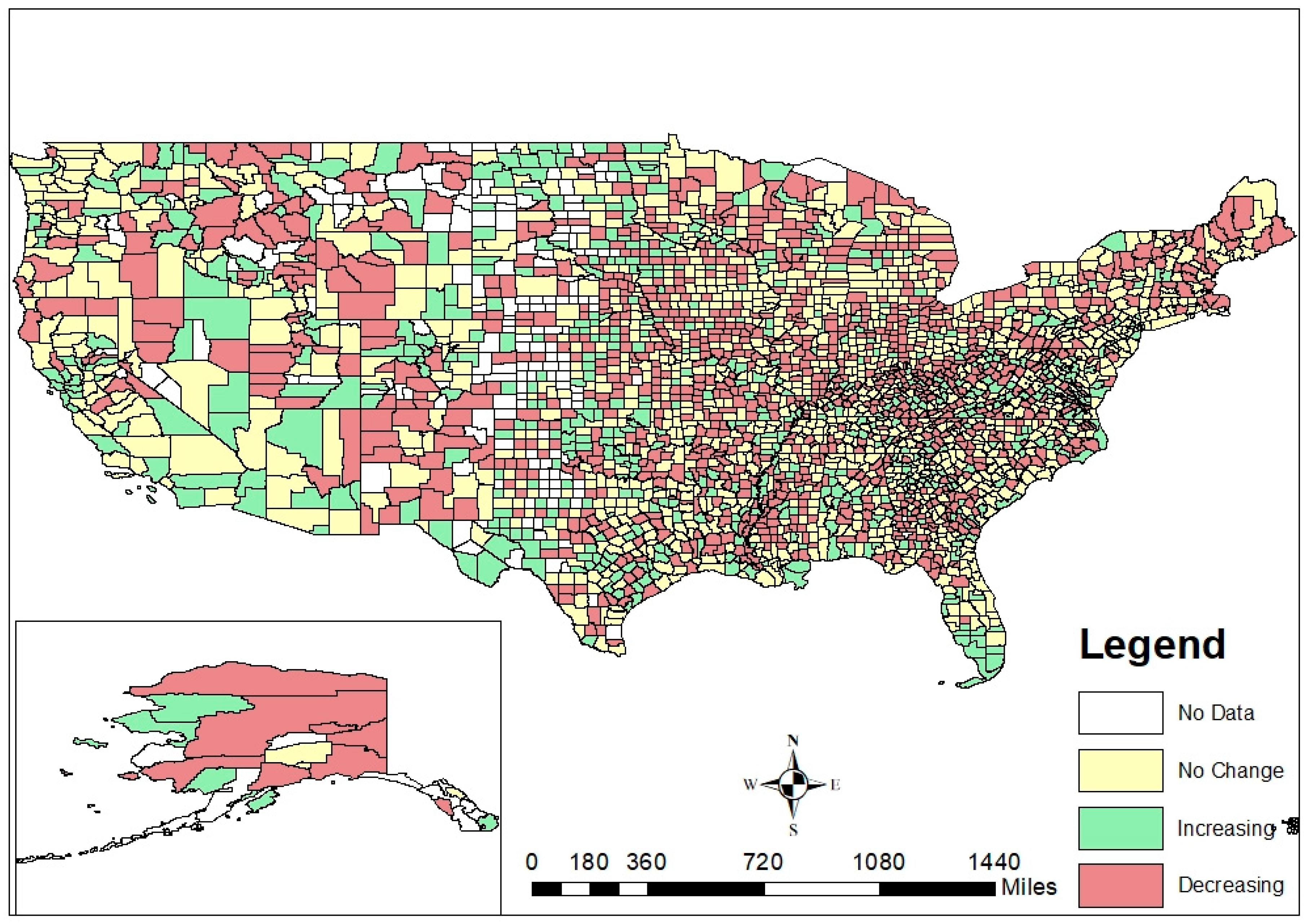
3.1. Description of LE Change
3.2. LE Change and Modifiable Determinants of Health Indicators
3.3. LE Change and COVID-19 Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roser, M.; Ortiz-Ospina, E.; Ritchie, H. Life expectancy. In Our World in Data; University of Oxford: Oxford, UK, 2013. [Google Scholar]
- Ortaliza, J.; Ramirez, G.; Satheeskumar, V.; Amin, K. How does US LIfe Expectancy Compare to Other Countries? Available online: https://www.healthsystemtracker.org/chart-collection/u-s-life-expectancy-compare-countries/#Life%20expectancy%20and%20healthcare%20spending%20per%20capita,%201980-2019%C2%A0 (accessed on 31 March 2022).
- National Research Council (US) Panel. Explaining Divergent Levels of Longevity in High-Income Countries; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Dwyer-Lindgren, L.; Bertozzi-Villa, A.; Stubbs, R. Inequalities in Life Expectancy among US Counties, 1980 to 2014: Temporal Trends and Key Drivers. JAMA Intern. Med. 2017, 177, 1003–1011. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P.; Valverde, J.R.; Bopp, M.; Bronnum-Hansen, H.; Deboosere, P.; Kalediene, R.; Kovacs, K.; Leinsalu, M.; Martikainen, P.; Menvielle, G.; et al. Determinants of inequalities in life expectancy: An international comparative study of eight risk factors. Lancet Public Health 2019, 4, e529–e537. [Google Scholar] [CrossRef]
- GBD US Health Disparities Collaborators. Life expectancy by county, race, and ethnicity in the USA, 2000–2019: A systematic analysis of health disparities. Lancet 2022, 400, 25–38. [Google Scholar] [CrossRef]
- Chetty, R.; Stepner, M.; Abraham, S.; Lin, S.; Scuderi, B.; Turner, N.; Bergeron, A.; Cutler, D. The Association Between Income and Life Expectancy in the United States, 2001–2014. JAMA 2016, 315, 1750–1766. [Google Scholar] [CrossRef] [PubMed]
- Vaupel, J.W.; Zhang, Z.; van Raalte, A.A. Life expectancy and disparity: An international comparison of life table data. BMJ Open 2011, 1, e000128. [Google Scholar] [CrossRef] [PubMed]
- Montez, J.K.; Beckfield, J.; Cooney, J.K.; Grumbach, J.M.; Hayward, M.D.; Koytak, H.Z.; Woolf, S.H.; Zajacova, A. US State Policies, Politics, and Life Expectancy. Milbank Q. 2020, 98, 668–699. [Google Scholar] [CrossRef] [PubMed]
- Case, A.; Deaton, A. Rising morbidity and mortality in midlife among white non-Hispanic Americans in the 21st century. Proc. Natl. Acad. Sci. USA 2015, 112, 15078–15083. [Google Scholar] [CrossRef] [PubMed]
- University of Wisconsin Population Health Institute. County Health Rankings & Roadmaps. Available online: https://www.countyhealthrankings.org (accessed on 15 February 2022).
- Hood, C.M.; Gennuso, K.P.; Swain, G.R.; Catlin, B.B. County Health Rankings: Relationships Between Determinant Factors and Health Outcomes. Am. J. Prev. Med. 2016, 50, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Andrasfay, T.; Goldman, N. Reductions in 2020 US life expectancy due to COVID-19 and the disproportionate impact on the Black and Latino populations. medRxiv 2020, 118, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Arias, E.; Escobedo, L.A.; Kennedy, J.; Fu, C.; Cisewki, J.U.S. Small-area Life Expectancy Estimates Project: Methodology and Results Summary. Vital Health Stat. 2018, 181, 1–40. [Google Scholar]
- National Center for Health Statistics. Restricted-Use Vital Statistics Data. Available online: https://www.cdc.gov/nchs/nvss/nvss-restricted-data.htm (accessed on 15 September 2018).
- National Center for Health Statistics. Provisional COVID-19 Death Counts in the United States by County. Available online: https://data.cdc.gov/NCHS/Provisional-COVID-19-Death-Counts-in-the-United-St/kn79-hsxy (accessed on 8 September 2021).
- US Census Bureau. Geographic Levels. Available online: https://www2.census.gov/geo/pdfs/maps-data/maps/reference/us_regdiv.pdf (accessed on 15 June 2021).
- Chiang, C.L. Lifetable and Its Application; Robert, E., Ed.; Krieger: New York, NY, USA, 1984. [Google Scholar]
- Karmakar, M.; Lantz, P.M.; Tipirneni, R. Association of Social and Demographic Factors With COVID-19 Incidence and Death Rates in the US. JAMA Netw. Open 2021, 4, e2036462. [Google Scholar] [CrossRef] [PubMed]
- Thakur, B.; Dubey, P.; Benitez, J.; Torres, J.P.; Reddy, S.; Shokar, N.; Aung, K.; Mukherjee, D.; Dwivedi, A.K. A systematic review and meta-analysis of geographic differences in comorbidities and associated severity and mortality among individuals with COVID-19. Sci. Rep. 2021, 11, 8562. [Google Scholar] [CrossRef] [PubMed]
- Bray, I.; Gibson, A.; White, J. Coronavirus disease 2019 mortality: A multivariate ecological analysis in relation to ethnicity, population density, obesity, deprivation and pollution. Public Health 2020, 185, 261–263. [Google Scholar] [CrossRef] [PubMed]
- Woolf, S.H.; Schoomaker, H. Life Expectancy and Mortality Rates in the United States, 1959–2017. JAMA 2019, 322, 1996–2016. [Google Scholar] [CrossRef] [PubMed]
- Dobis, E.A.; Stephens, H.M.; Skidmore, M.; Goetz, S.J. Explaining the spatial variation in American life expectancy. Soc. Sci. Med. 2020, 246, 112759. [Google Scholar] [CrossRef] [PubMed]
- Dukhovnov, D.; Barbieri, M. County-level socio-economic disparities in COVID-19 mortality in the USA. Int. J. Epidemiol. 2022, 51, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Q.; Song, G.; Yang, Z.; Chen, R.J.; Zheng, Y.L.; Hu, H.Y.; Su, X.; Chen, P.J. Association between ageing population, median age, life expectancy and mortality in coronavirus disease (COVID-19). Aging 2020, 12, 24570–24578. [Google Scholar] [CrossRef] [PubMed]
- United States Government Accountability Office. COVID-19: Data Quality and Considerations for Modeling and Analysis; United States Government Accountability Office: Washington, DC, USA, 2020. [Google Scholar]
- Baltrus, P.; Malhotra, K.; Rust, G.; Levine, R.; Li, C.; Gaglioti, A.H. Identifying County-Level All-Cause Mortality Rate Trajectories and Their Spatial Distribution Across the United States. Prev. Chronic Dis. 2019, 16, E55. [Google Scholar] [CrossRef] [PubMed]
- Meshram, S.S. Comparative Analysis of LIfe Expectancy between Developed and Developing Countries using Machine Learning. In Proceedings of the IEEE Bombay Section Signature Conference (IBSSC), Mumbai, India, 4–6 December 2020; pp. 6–10. [Google Scholar]


{kind=link}
| County-Level LE Change (2011–2016) | Baseline 2010 Life Expectancy (LE) | ||
|---|---|---|---|
| Tertile 1 (LE = 51–62 Years) | Tertile 2 (LE = 63–74 Years) | Tertile 3 (LE = 75–86 Years ) | |
| No change | 253 (26%) | 436 (44%) | 550 (56%) |
| Increasing | 256 (26%) | 183 (19%) | 177 (18%) |
| Decreasing | 472 (48%) | 362 (37%) | 254 (26%) |
| No Change (n = 1239) | Increasing LE (n = 616) | Decreasing LE (n = 1088) | |
|---|---|---|---|
| Geographic Region (n, %) | |||
| Midwest | 403 (33%) | 162 (26%) | 410 (38%) |
| Northeast | 123 (10%) | 24 (4%) | 69 (6%) |
| South | 565 (46%) | 327 (53%) | 484 (44%) |
| West | 148 (12%) | 103 (17%) | 125 (11%) |
| Baseline LE in 2010 (mean, SD) | 76.6 (4.49) | 73.7 (7.12) | 73.5 (5.95) |
| Age * (mean, SD) | |||
| Proportion ≤19 years | 25.0 (3.17) | 25.2 (4.03) | 24.6 (3.57) |
| Proportion >55 years | 32.0 (5.68) | 31.9 (6.97) | 33.7 (5.77) |
| Proportion Female * (mean, SD) | 50.2 (1.85) | 49.8 (2.26) | 49.8 (2.64) |
| Proportion Hispanic Ethnicity * (mean, SD) | 9.41 (13.3) | 11.8 (15.6) | 7.75 (13.0) |
| Proportion Race Category * (mean, SD) | |||
| Non-Hispanic White | 76.3 (18.8) | 73.0 (21.2) | 77.8 (20.5) |
| Non-Hispanic Black | 9.26 (13.5) | 8.94 (13.9) | 9.59 (16.0) |
| Non-Hispanic Other | 3.02 (5.27) | 4.20 (9.06) | 3.03 (8.59) |
| Population Density ** in 2019 (mean, SD) | 101 (231) | 238 (1510) | 46 (155) |
| Poverty Rate *** (mean, SD) | 26.4 (8.09) | 26.3 (9.21) | 29.1 (8.87) |
| County Health Ranking Indicator | Odds of Being an Increasing LE County Compared to No Change | Odds of Being a Decreasing LE County Compared to No Change | ||
|---|---|---|---|---|
| Adjusted Odds Ratio * | 95% CI | Adjusted Odds Ratio * | 95% CI | |
| Poor or Fair Health | 0.966 | [0.947, 0.984] | 1.016 | [1.000, 1.032] |
| Poor Physical Health Days | 0.825 | [0.746, 0.913] | 1.102 | [1.018, 1.193] |
| Poor Mental Health Days | 0.854 | [0.768, 0.949] | 1.040 | [0.954, 1.133] |
| Adult Smoking | 0.956 | [0.937, 0.975] | 1.019 | [1.002, 1.037] |
| Adult Obesity | 0.923 | [0.898, 0.95] | 1.029 | [1.003, 1.056] |
| Binge Drinking | 1.014 | [0.993, 1.036] | 0.992 | [0.974, 1.01] |
| Motor Vehicle Crash Death Rate | 0.995 | [0.984, 1.005] | 1.010 | [1.001, 1.019] |
| Unemployment | 0.888 | [0.844, 0.934] | 1.073 | [0.939, 0.961] |
| Children in Poverty | 0.981 | [0.969, 0.993] | 1.018 | [1.008, 1.029] |
| Single-Parent Households | 0.925 | [0.887, 0.965] | 1.044 | [1.008, 1.081] |
| Preventable Hospital Stays | 0.998 | [0.995, 1.001] | 1.003 | [1.000, 1.005] |
| College Degrees | 1.038 | [1.025, 1.051] | 0.970 | [0.958, 0.983] |
| Access to Healthy Foods | 1.000 | [0.995, 1.005] | 0.992 | [0.988, 0.997] |
| Covariates | Regression Coefficient | 95% Confidence Interval |
|---|---|---|
| No change in LE | Ref | Ref |
| Increasing LE | 0.953 | [0.943, 0.963] |
| Decreasing LE | 0.995 | [0.986, 1.004] |
| Baseline 2010 LE | 0.928 | [0.927, 0.930] |
| Proportion ≤19 years old in 2019 | 1.041 | [1.039, 1.043] |
| Proportion >55 years old in 2019 | 1.021 | [1.019, 1.022] |
| Proportion unemployed | 0.985 | [0.983, 0.987] |
| Poor physical health days | 0.965 | [0.960, 0.971] |
| Reference: quintile 1 | ||
| Population density—quintile 2 | 1.140 | [1.108, 1.172] |
| Population density—quintile 3 | 1.307 | [1.273, 1.342] |
| Population density—quintile 4 | 1.577 | [1.538, 1.617] |
| Population density—quintile 5 | 1.867 | [1.819, 1.913] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandran, A.; Purbey, R.; Leifheit, K.M.; Evans, K.M.; Baez, J.V.; Althoff, K.N. County-Level Life Expectancy Change: A Novel Metric for Monitoring Public Health. Int. J. Environ. Res. Public Health 2022, 19, 10672. https://doi.org/10.3390/ijerph191710672
Chandran A, Purbey R, Leifheit KM, Evans KM, Baez JV, Althoff KN. County-Level Life Expectancy Change: A Novel Metric for Monitoring Public Health. International Journal of Environmental Research and Public Health. 2022; 19(17):10672. https://doi.org/10.3390/ijerph191710672
Chicago/Turabian StyleChandran, Aruna, Ritika Purbey, Kathryn M. Leifheit, Kirsten McGhie Evans, Jocelyn Velasquez Baez, and Keri N. Althoff. 2022. "County-Level Life Expectancy Change: A Novel Metric for Monitoring Public Health" International Journal of Environmental Research and Public Health 19, no. 17: 10672. https://doi.org/10.3390/ijerph191710672
APA StyleChandran, A., Purbey, R., Leifheit, K. M., Evans, K. M., Baez, J. V., & Althoff, K. N. (2022). County-Level Life Expectancy Change: A Novel Metric for Monitoring Public Health. International Journal of Environmental Research and Public Health, 19(17), 10672. https://doi.org/10.3390/ijerph191710672