
Creating an Optimal In Vivo Environment to Enhance Outcomes Using Cell Therapy to Repair/Regenerate Injured Tissues of the Musculoskeletal System



Abstract
1. Introduction
1.1. Purpose of the Review
1.2. Characteristics of Musculoskeletal (MSK) Tissues
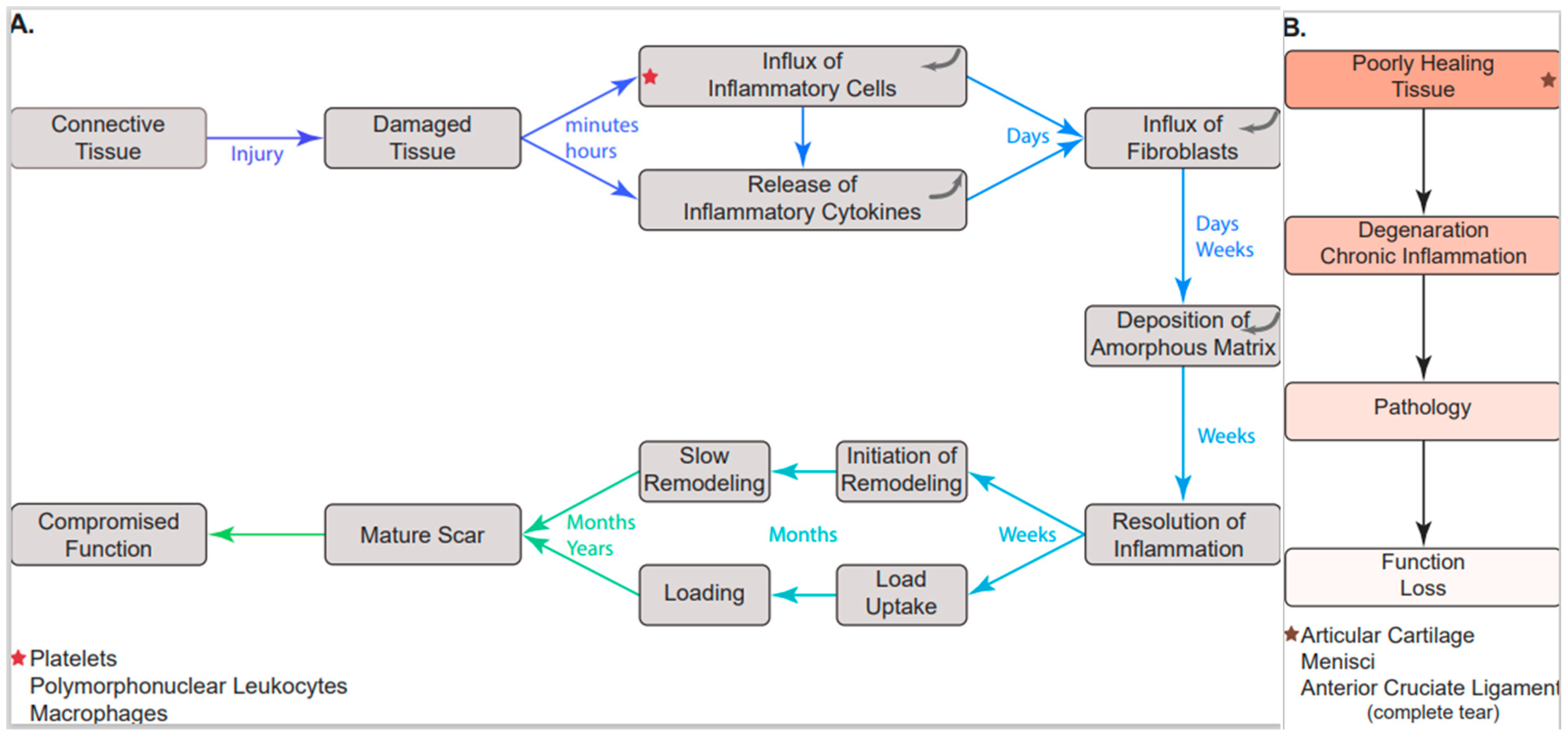
1.3. The Inflammatory Response
2. Interactions between Inflammation and Injured Connective Tissues of the MSK System-Loss of Function
3. Factors That Can Complicate Post-Injury Processes and Inflammation
4. The Role of Mechanics in Connective Tissue Repair and Regeneration: The Interface with Biology Is Critical
5. Enhancing Repair/Regeneration of Injured Connective Tissues of the MSK System
6. Use of Single Cell Preparations of Mesenchymal Stem/Signaling Cells (MSC) to Enhance the Repair/Regeneration of Damaged Mechanically Active Connective Tissues
7. Use of MSC in Tissue Engineered Constructs to Enhance Repair of Injured or Diseased Tissues
8. The Way Forward
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lo, I.K.Y.; Marchuk, L.L.; Leatherbarrow, K.E.; Frank, C.B.; Hart, D.A. Collagen fibrillogenesis and mRNA levels in the maturing rabbit medial collateral ligament and patellar tendon. Connect. Tis. Res. 2004, 45, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Frank, C.B.; Matyas, J.; Hart, D. Aging of the medial collateral ligament. Interdisciplinary studies. In Musculoskeletal Soft-Tissue Aging: Impact on Mobility; Buckwalter, J.A., Goldberg, V.M., Woo, S.L.Y., Eds.; AAOS: Rosemont, IL, USA, 1993; pp. 305–326. [Google Scholar]
- Eng, K.; Rangayyan, R.M.; Bray, R.C.; Frank, C.B.; Anscomb, J.; Veale, P. Quantitative analysis of the fine vascular anatomy of articular ligaments. IEEE Trans. Biomed. Eng. 1992, 39, 296–306. [Google Scholar] [CrossRef] [PubMed]
- Bray, R.C.; Salo, P.T.; Lo, I.K.; Ackermann, P.; Rattner, J.B.; Hart, D.A. Normal ligament structure, physiology, and function. Sports Med. Arthrosc. Rev. 2005, 13, 127–135. [Google Scholar] [CrossRef]
- Georgiev, G.P.; LLiev, A.; Kotov, G.; Kinov, P.; Slavcher, S.; Landzhov, B. Light and electron microscopic study of the medial collateral epiligament tissue in human knees. World J. Orthop. 2017, 8, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Hart, D.A.; Frank, C.B.; Bray, R. Inflammatory processes in repetitive motion and over-use syndromes: Potential role of neurogenic mechanisms in tendon and ligaments. In Repetitive Motion Disorders of the Upper Extremity; Gordon, S.L., Blair, S.J., Fine, L.J., Eds.; AAOS: Park Ridge, IL, USA, 1995; pp. 247–262. [Google Scholar]
- Scott, A.; Lian, O.; Bahr, R.; Hart, D.A.; Duronio, V.; Khan, K.M. Increased mast cell numbers in human patellar tendinosis: Correlation with symptom duration and vascular hyperplasia. Br. J. Sports Med. 2008, 42, 753–757. [Google Scholar] [CrossRef]
- Benjamin, M.; McGonagle, D. Entheses: Tendon and ligament attachment sites. Scand. J. Med. Sci. Sports 2009, 19, 520–527. [Google Scholar] [CrossRef]
- Benjamin, M.; McGonagle, D. The enthesis organ concept and its relevance to the spondyloarthropathies. Adv. Exp. Med. Biol. 2009, 649, 57–70. [Google Scholar] [CrossRef]
- Sevick, J.L.; Abusara, Z.; Andrews, S.H.; Xu, M.; Shurshid, S.; Chatta, J.; Hart, D.A.; Shrive, N.G. Fibril deformation underload of the rabbit Achilles tendon and medial collateral ligament femoral entheses. J. Orthop. Res. 2018, 36, 2506–2515. [Google Scholar] [CrossRef]
- Sarmiento, P.; Little, D. Tendon and multiomics: Advantages, advances, and opportunities. NPJ Regen. Med. 2021, 6, 61. [Google Scholar] [CrossRef]
- Huisman, E.S.; Andersson, G.; Scott, A.; Reno, C.R.; Hart, D.A.; Thornton, G.M. Regional molecular and cellular differences in the female rabbit Achilles tendon complex: Potential implications for understanding responses to loading. J. Anat. 2014, 224, 538. [Google Scholar] [CrossRef]
- Arnoczky, S.P.; Cook, J.L.; Carter, T.; Turner, A.S. Translational models for studying meniscal repair and replacement: What they can and cannot tell us. Tissue Eng. Part B Rev. 2010, 16, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Andrews, S.H.; Rattner, J.B.; Abusara, Z.; Adesida, A.; Shrive, N.G.; Ronsky, J.L. Tie-fibre structure and organization in the knee menisci. J. Anat. 2012, 224, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Andrews, S.H.; Rattner, J.B.; Jamniczky, H.A.; Shrive, N.G.; Adesida, A. The structural and composition transition of the menisci roots into the fibrocartilage of the menisci. J. Anat. 2015, 226, 169–174. [Google Scholar] [CrossRef]
- Andrews, S.H.J.; Adesida, A.; Abusara, Z.; Shrive, N.G. Current concepts on structure-function relationships in the menisci. Connect. Tissue Res. 2017, 58, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Frost, H.M. The mechanostat: A proposed pathogenic mechanism of osteoporosis and bone mass effects of mechanical and nonmechanical agents. Bone Miner. 1987, 2, 73–85. [Google Scholar]
- Frost, H.M. Perspectives: A proposed general model of the “mechanostat” (suggestions from a new skeletal-biologic paradigm). Anat. Rec. 1996, 244, 139–147. [Google Scholar] [CrossRef]
- Frost, H.M. Bone’s mechanostat: A 2003 update. Anat. Rec. A Discov. Mol. Cell. Evol. Biol. 2003, 275, 1081–1101. [Google Scholar] [CrossRef]
- Hart, D.A. Learning from human responses to deconditioning environments: Improved understanding of the “use it or lose it” principle. Front. Sports Act. Living 2021, 3, 685845. [Google Scholar] [CrossRef]
- Hart, D.A.; Natsu-ume, T.; Sciore, P.; Tasevski, V.; Frank, C.B.; Shrive, N.G. Mechanobiology: Similarities and differences between in vivo and in vitro analysis at the functional and molecular levels. Recent Res. Devel. Biophys. Biochem. 2002, 2, 153–177. [Google Scholar]
- Natsu-Ume, T.; Majima, T.; Reno, C.; Shrive, N.G.; Frank, C.B.; Hart, D.A. Menisci of the rabbit knee require mechanical loading to maintain homeostasis: Cyclic hydrostatic compression in vitro prevents derepression of catabolic genes. J. Orthop. Sci. 2005, 10, 396–405. [Google Scholar] [CrossRef]
- Moretti, L.; Stalfort, J.; Barker, T.H.; Abebayehu, D. The interplay of fibroblasts, the extracellular matrix, and inflammation in scar formation. J. Biol. Chem. 2022, 298, 101530. [Google Scholar] [CrossRef] [PubMed]
- Thornton, J.M.; Yin, K. Role of specialized pro-resolving mediators in modifying host defense and decreasing bacterial virulence. Molecules 2021, 26, 6970. [Google Scholar] [CrossRef] [PubMed]
- Leuti, A.; Fava, M.; Pellegini, N.; Maccarrone, M. Role of specialized pro-resolving mediators in neuropathic pain. Front. Pharmacol. 2021, 12, 717993. [Google Scholar] [CrossRef]
- Han, Y.H.; Lee, K.; Saha, A.; Han, J.; Choi, H.; Noh, M.; Lee, Y.H.; Lee, M.C. Specialized proresolving mediators for therapeutic interventions targeting metabolic and inflammatory disorders. Biomol. Ther. 2021, 29, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Blaudez, F.; Ivanovski, S.; Fournier, B.; Vaquette, C. The utilization of resolvins in medicine and tissue engineering. Acta Biomater. 2021, 140, 116–135. [Google Scholar] [CrossRef]
- Bartczak, K.; Bialas, A.J.; Kotecki, M.J.; Gorski, P.; Piotrowski, W.J. More than a genetic code: Epigenetics of lung fibrosis. Mol. Diagn. Ther. 2020, 24, 665–681. [Google Scholar] [CrossRef]
- Cai, Q.; Gan, C.; Tang, C.; Wu, H.; Gao, J. Mechanism and therapeutic opportunities of histone modifications in chronic liver disease. Front. Pharmacol. 2021, 12, 78491. [Google Scholar] [CrossRef]
- Doody, K.M.; Bottini, N.; Firestein, G.S. Epigenetic alterations in rheumatoid arthritis fibroblast-like synoviocytes. Epigenomics 2017, 9, 479–492. [Google Scholar] [CrossRef]
- Lin, Z.; Ding, Q.; Li, X.; Feng, Y.; He, H.; Huang, C.; Zhu, Y.Z. Targeting epigenetic mechanisms in vascular aging. Front. Cardiovasc. Med. 2022, 8, 806988. [Google Scholar] [CrossRef]
- Guttzeit, S.; Backs, J. Post-translational modifications talk and crosstalk to class IIa histone deacetylases. J. Mol. Cell Cardiol. 2022, 162, 53–61. [Google Scholar] [CrossRef]
- Kishi, K.; Okabe, K.; Shimizu, R.; Kubota, Y. Fetal skin possesses the ability to regenerate completely: Complete regeneration of skin. Keio J. Med. 2012, 61, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Pratsinis, H.; Mavrogonatou, E.; Kietsas, D. Scarless wound healing: From development to senescence. Adv. Drug Deliv. Rev. 2019, 146, 325–343. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.L.; Wu, Y.; Yuan, Z.W.; Gao, X.H.; Chen, H.D. Advances in scarless foetal wound healing and prospects for scar reduction in adults. Cell Prolif. 2020, 53, e12916. [Google Scholar] [CrossRef] [PubMed]
- Gilliver, S.C. Sex steroids as inflammatory regulators. J. Steroid Biochem. Mol. Biol. 2010, 120, 105–115. [Google Scholar] [CrossRef]
- Gilliver, S.C.; Ashworth, J.J.; Ashcroft, G.S. The hormonal regulation of cutaneous wound healing. Clin. Dermatol. 2007, 25, 56–62. [Google Scholar] [CrossRef]
- Ashcroft, G.S.; Ashworth, J.J. Potential role of estrogens in wound healing. Am. J. Clin. Dermatol. 2003, 4, 737–743. [Google Scholar] [CrossRef]
- Handman, M.J.; Ashcroft, G.S. Estrogen, not intrinsic aging, is the major regulator of delayed human wound healing in the elderly. Genome Biol. 2008, 9, R80. [Google Scholar] [CrossRef]
- Arida, C.; Mastrokalos, D.S.; Panagopoulos, A.; Vlamis, J.; Triantafyllopoulos, I.K. A systematic approach for stronger documentation of anterior cruciate ligament graft choice. Cureus 2021, 13, e19017. [Google Scholar] [CrossRef]
- Hayback, G.; Raas, C.; Rosenberger, R. Failure rates of common grafts used in ACL reconstructions: A systematic review of studies published in the last decade. Arch. Orthop. Trauma Surg. 2021. [Google Scholar] [CrossRef]
- Hart, D.A.; Werle, J.; Robert, J.; Kania-Richmond, A. Long wait times for knee and hip total joint replacement in Canada: An isolated health system problem, or a symptom of a larger problem? Osteoarthr. Cartil. Open. 2021, 3, 100141. [Google Scholar] [CrossRef]
- Frank, C.; MacFarlane, B.; Edwards, P.; Rangayyan, R.; Liu, Z.Q.; Walsh, S.; Bray, R. A quantitative analysis of matrix alignment in ligament scars: A comparison of movement versus immobilization in an immature rabbit model. J. Orthop. Res. 1991, 9, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Achari, Y.; Chin, J.W.S.; Heard, B.J.; Rattner, J.B.; Shrive, N.G.; Frank, C.B.; Hart, D.A. Molecular events surrounding collagen fibril assembly in the early healing rabbit medial collateral ligament—Failure to recapitulate normal ligament development. Connect. Tissue Res. 2011, 52, 301–312. [Google Scholar] [CrossRef]
- Marieswaran, M.; Jain, I.; Garg, B.; Sharma, V.; Kalyanasundaram, D. A review of biomechanics of anterior cruciate ligament and material for reconstruction. Appl. Bionics Biomech. 2018, 2018, 4657824. [Google Scholar] [CrossRef] [PubMed]
- Blythe, A.; Tasker, T.; Zioupos, P. ACL fraft constructs: In-vitro fatigue testing highlights the occurrence of irrecoverable lengthening and the need for adequate (pre) conditioning to avert the reoccurance of knee instability. Technol. Health Care. 2006, 14, 335–347. [Google Scholar] [CrossRef]
- Miller, R.M.; Rahnemai-Azar, A.A.; Suer, L.; Arilla, F.V.; Fu, F.H.; Debski, R.E.; Musahl, V. Tensile properties of a split quadriceps graft for ACL reconstruction. Knee Surg. Sports Traumatol. 2017, 25, 1249–1254. [Google Scholar] [CrossRef] [PubMed]
- Bedi, A. Editorial Commentary: Buckle Up Surgeons: “Safety Belt” Reinforcement of Knee Anterior Cruciate Ligament Reconstruction Grafts. Arthroscopy 2018, 34, 500–501. [Google Scholar] [CrossRef]
- Heard, B.J.; Barton, K.I.; Chung, M.; Achari, Y.; Shrive, N.G.; Frank, C.B.; Hart, D.A. Single intra-articular dexamethasone injection immediately post-surgery in a rabbit model mitigates early inflammatory response and post-traumatic osteoarthritis-like alterations. J. Orthop. Res. 2015, 33, 1826–1834. [Google Scholar] [CrossRef]
- Sieker, J.T.; Ayturk, U.M.; Proffen, B.L.; Weissenberger, M.H.; Kiapour, A.M.; Murray, M.M. Immediate administration of intraarticular triamcinolone acetonide after joint injury modulates molecular outcomes associated with early synovitis. Arthritis Rheum. 2016, 68, 1637–1647. [Google Scholar] [CrossRef]
- Bedrin, M.D.; Kartalias, K.; Yow, B.G.; Dickens, J.F. Degenerative joint disease after meniscectomy. Sports Med. Arthrosc. Rev. 2021, 29, e44–e50. [Google Scholar] [CrossRef]
- Vinagre, G.; Cruz, F.; Alkhelaifi, K.; D’Hooghe, P. Isolated meniscus injuries in skeletally immature children and adolescents: State of the art. J. ISAKOS 2022, 7, 19–26. [Google Scholar] [CrossRef]
- Kaul, G.; Cucchiarini, M.; Remberger, K.; Kohn, D.; Madry, H. Failed cartilage repair for early osteoarthritis defects: A biochemical, histological and immunohistochemical analysis of the repair tissue after treatment with marrow-stimulation techniques. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 2315–2324. [Google Scholar] [CrossRef] [PubMed]
- Erggelet, C.; Vavken, P. Microfracture for the treatment of cartilage defects in the knee joint—A golden standard? J. Clin. Orthop. Trauma. 2016, 7, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Gudeman, A.S.; Hinckel, B.B.; Oladeji, L.; Ray, T.E.; Gersoff, W.; Farr, J.; Sherman, S.L. Evaluation of commercially available knee cartilage restoration techniques stratified by FDA approval pathway. Am. J. Sports Med. 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Armoiry, X.; Cummins, E.; Connock, M.; Metcalfe, A.; Royle, P.; Johnston, R.; Rodrigues, J.; Waugh, N.; Mistry, H. Autologous chondrocyte implantation with chondrosphere for treating articular cartilage defects in the knee: An evidence review group perspective of a NICE single technology appraisal. Pharmocoeconomics 2019, 37, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Sharma, U.R.; Rathnakaran, A.N.; Raj, B.P.P.; Padinjakkara, G.; Das, A.; Vada, S.; Mudagal, M. The positive effect of pregnancy in rheumatoid arthritis and the use of medications for the management of rheumatoid arthritis during pregnancy. Inflammopharmacology 2021, 29, 987–1000. [Google Scholar] [CrossRef]
- Gomez-Chavez, F.; Correa, D.; Navarrete-Meneses, P.; Cancino-Diaz, J.C.; Cancino-Diaz, M.E.; Rodriguez-Matinez, S. NF-kB and its regulators during pregnancy. Front. Immunol. 2021, 12, 679106. [Google Scholar] [CrossRef]
- Hart, D.A.; Kydd, A.S.; Frank, C.B.; Hildebrand, K.A. Tissue repair in rheumatoid arthritis: Challenges and opportunities in the face of a systemic inflammatory disease. Best Pract. Res. Clin. Rheumatol. 2004, 18, 187–202. [Google Scholar] [CrossRef]
- Ackermann, P.; Hart, D.A. Influence of comorbidities: Neuropathy, vasculopathy, and diabetes in healing response quality. Adv. Wound Care 2013, 2, 410–421. [Google Scholar] [CrossRef]
- Ahmed, A.S.; Schizas, N.; Li, J.; Ahmed, M.; Ostenson, C.-G.; Salo, P.; Hewitt, C.; Hart, D.A.; Ackermann, P.W. Type 2 diabetes impairs tendon repair after injury in a rat model. J. Appl. Physiol. 2012, 113, 1784–1791. [Google Scholar] [CrossRef]
- Ahmed, A.S.; Li, J.; Schizas, N.; Ahmed, M.; Ostenson, C.-G.; Salo, P.; Hewitt, C.; Hart, D.A.; Ackermann, P.W. Expressional changes in growth and inflammatory mediators during Achille’s tendon repair in diabetic rats: New insights into a possible basis for compromised healing. Cell Tissue Res. 2014, 357, 109–117. [Google Scholar] [CrossRef]
- Ahmed, A.S.; Li, J.; Abdul, A.M.D.; Ahmed, M.; Ostenson, C.-G.; Salo, P.T.; Hewitt, C.; Hart, D.A.; Ackermann, P.W. Compromised neurotrophic and angiogenic regenerative capability during tendon healing in a rat model of type-II diabetes. PLoS ONE 2017, 12, e0170748. [Google Scholar] [CrossRef] [PubMed]
- Collins, K.H.; Herzog, W.; MacDonald, G.Z.; Reimer, R.A.; Rios, J.L.; Smith, I.C.; Zernicke, R.F.; Hart, D.A. Obesity, metabolic syndrome, and musculoskeletal disease: Common inflammatory pathways suggest a central role for loss of muscle integrity. Front. Physiol. 2018, 9, 112. [Google Scholar] [CrossRef] [PubMed]
- Scott, A.; Zwerver, J.; Grewal, N.; de Sa, A.; Alktebi, T.; Granville, D.J.; Hart, D.A. Lipids, adiposity and tendinopathy: Is there a mechanistic link? Critical review. Br. J. Sports Med. 2015, 49, 984–988. [Google Scholar] [CrossRef] [PubMed]
- De Sa, A.; Hart, D.A.; Khan, K.; Scott, A. Achilles tendon structure is negatively correlated with body mass index, but not influenced by statin use: A cross-sectional study using ultrasound tissue characterization. PLoS ONE 2018, 13, e0199645. [Google Scholar] [CrossRef]
- Ghosh, N.; Kolade, O.O.; Shontz, E.; Rosenthal, Y.; Zuckerman, J.D.; Bosco, J.A., 3rd; Virk, M.S. Nonsteroidal anti-inflammatory drugs (NSAIDS) and their effect on musculoskeletal soft-tissue healing: A scoping review. JBJS Rev. 2019, 7, e4. [Google Scholar] [CrossRef]
- White, A.E.; Henry, J.K.; Dziadosz, D. The effect of nonsteroidal anti-inflammatory drugs and selective COX-2 inhibitors on bone healing. HSS J. 2021, 17, 231–234. [Google Scholar] [CrossRef]
- Kigera, J.W.M.; Gichangi, P.B.; Abdelmalek, A.K.M.; Ogeng’o, J.A. Age related effects of selective and non-selective COX-2 inhibitors on bone healing. J. Clin. Orthop. Trauma 2022, 25, 101763. [Google Scholar] [CrossRef]
- Yasui, Y.; Hart, D.A.; Sugita, N.; Chiijimatsu, R.; Koizumi, K.; Ando, W.; Moriguchi, Y.; Shimomura, K.; Myoui, A.; Yoshikawa, H.; et al. Time-dependent recovery of human synovial membrane mesenchymal stem cell function after high-dose steroid therapy: Case report and laboratory study. Am. J. Sports Med. 2018, 46, 695–701. [Google Scholar] [CrossRef]
- Lee, S.; Kruger, B.T.; Ignatius, A.; Tuckerman, J. Distinct glucocorticoid receptor actions in bone homeostasis and bone diseases. Front. Endocrinol. 2022, 12, 815386. [Google Scholar] [CrossRef]
- Roughley, P.J. Structural changes in the proteoglycans of human articular cartilage during aging. J. Rheumatol. 1987, 14, 14–15. [Google Scholar]
- Chen, M.; Zhou, S.; Shi, H.; Gu, H.; Wen, Y.; Chen, L. Identification and validation of pivotal genes related to age-related meniscus degeneration based on gene exporession profiling analysis and in vivo and in vitro models detection. BMC Med. Genom. 2021, 14, 237. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Wojtkiewicz, M.; Patwardhan, C.; Greer, S.; Kong, Y.; ZKuss, M.; Huang, X.; Liao, J.; Lu, Y.; Dudley, A.; et al. The effects of maturation and aging on the rotator cuff tendon-to-bone interface. FASEB J. 2021, 35, e22066. [Google Scholar] [CrossRef] [PubMed]
- Hart, D.A.; Nakamura, N.; Shrive, N.G. Perspective: Challenges presented for regeneration of heterogeneous musculoskeletal tissues that normally develop in unique biomechanical environments. Front. Bioeng. Biotechnol. 2021, 9, 760273. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Li, D.L.; Chuang, A.D.C.; Dash, B.S.; Chen, J.P. Tension stimulation of tenocytes in aligned hyaluronic acid/platelet -rich plasma-polycaprolactone core-sheath nanofiber membrane scaffold for tendon tissue engineering. Int. J. Mol. Sci. 2021, 22, 11215. [Google Scholar] [CrossRef] [PubMed]
- Szojka, A.R.; Li, D.X.; Sopcak, M.E.J.; Ma, Z.; Kunze, M.; Mulet-Sierra, A.; Adeeb, S.M.; Westover, L.; Jomha, N.M.; Adesida, A.B. Mechano-hypoxia conditioning of engineered human meniscus. Front. Bioeng. Biotechnol. 2021, 9, 739438. [Google Scholar] [CrossRef] [PubMed]
- Hart, D.A.; Shrive, N.G.; Goulet, F. Tissue engineering of ACL replacements. Sports Med. Arthrosc. Rev. 2005, 13, 170–176. [Google Scholar] [CrossRef]
- Kobayashi, M.; Spector, M. In vitro response of bone marrow-derived mesenchymal stem cells seeded in a type-1 collagen-glycosaminoglycan scaffold for skin wound repair under mechanical loading condition. Mol. Cell Biomech. 2009, 6, 217–227. [Google Scholar]
- Yong, K.W.; Choi, J.R.; Choi, J.W.; Cowie, A.C. Recent advances in mechanically loaded human mesenchymal stem cells for bone tissue engineering. Int. J. Mol. Sci. 2020, 21, 5816. [Google Scholar] [CrossRef]
- Pattappa, G.; Zellner, J.; Johnstone, B.; Docheva, D.; Angele, P. Cells under pressure- the relationship between hydrostatic pressure and mesenchymal stem cell chondrogenesis. Eur. Cell Mater. 2019, 37, 360–381. [Google Scholar] [CrossRef]
- Zhang, S.; Yao, Y. The role of mechanical regulation in cartilage tissue engineering. Curr. Stem Cell Res. Ther. 2021, 16, 939–948. [Google Scholar] [CrossRef]
- Shimomura, K.; Ando, W.; Tateishi, K.; Nansai, R.; Fujie, H.; Hart, D.A.; Kohda, H.; Kita, K.; Kanamoto, T.; Mae, T.; et al. The influence of skeletal maturity on allogenic synovial mesenchymal stem cell-based repair of cartilage in a large animal model. Biomaterials 2010, 31, 8004–8011. [Google Scholar] [CrossRef] [PubMed]
- Fujie, H.; Nansai, R.; Ando, W.; Shimomura, K.; Moriguchi, Y.; Hart, D.A.; Nakamura, N. Zone-specific integrated cartilage repair using a scaffold-free tissue engineered construct derived from allogenic synovial mesenchymal stem cells: Biomechanical and histological assessments. J. Biomech. 2015, 48, 4101–4108. [Google Scholar] [CrossRef] [PubMed]
- Andia, I.; Atilano, L.; Maffulli, N. Moving towards targeting the right phenotype with the right platelet-rich plasma (PRP) formulation for knee osteoarthritis. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X211004336. [Google Scholar] [CrossRef] [PubMed]
- Kydd, A.S.R.; Hart, D.A. Efficacy and safety of platelet-rich plasma injections of osteoarthritis. Curr. Treat. Options Rheum. 2020, 6, 87–98. [Google Scholar] [CrossRef]
- Burnham, R.; Smith, A.; Hart, D. The safety and efficacy of bone marrow concentrate injection for knee and hip osteoarthritis: A Canadian cohort. Regen. Med. 2021, 16, 619–628. [Google Scholar] [CrossRef]
- Rodriguez-Merchan, E.C. Anterior cruciate ligament reconstruction: Is biological augmentation beneficial? Int. J. Mol. Sci. 2021, 22, 12566. [Google Scholar] [CrossRef]
- Evans, C.H.; Huard, J. Gene therapy approaches to regenerating the musculoskeletal system. Nat. Rev. Rheumatol. 2015, 11, 234–242. [Google Scholar] [CrossRef]
- Clutterbuck, A.L.; Asplin, K.E.; Harris, P.; Allaway, D.; Mobsdheri, A. Targeting matrix metalloproteinases in inflammatory conditions. Curr. Drug Targets 2009, 10, 1245–1254. [Google Scholar] [CrossRef]
- Hildebrand, K.A.; Frank, C.B.; Hart, D.A. Gene intervention in ligament and tendon: Current status, challenges, future directions. Gene Ther. 2004, 11, 368–378. [Google Scholar] [CrossRef]
- Hart, D.A.; Nakamura, N.; Marchuk, L.; Hiraoka, H.Y.; Boorman, R.; Kaneda, Y.; Shrive, N.G.; Frank, C.B. Complexity of determining cause and effect in vivo after antisense gene therapy. Clin. Orthop. Relat. Res. 2000, 379, S242–S251. [Google Scholar] [CrossRef]
- Frank, C.; Shrive, N.; Hiraoka, H.; Nakamura, N.; Kaneda, Y.; Hart, D. Optimization of the biology of soft tissue repair. J. Sci. Med. Sport. 1999, 2, 190–210. [Google Scholar] [CrossRef]
- Li, Z.J.; Yang, Q.Q.; Zhou, Y.L. Basic research on tendon repair: Strategies, evaluation, and development. Front. Med. 2021, 8, 664909. [Google Scholar] [CrossRef] [PubMed]
- Padilla, S.; Sanchez, M.; Vaquerizo, V.; Malanga, G.A.; Fiz, N.; Azofra, J.; Rogers, C.J.; Samitier, G.; Sampson, S.; Seijas, R.; et al. Platelet-rich plasma applications for Achille’s tendon repair: A bridge between biology and surgery. Int. J. Mol. Sci. 2021, 22, 824. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, I.D.; Rodeo, S.A.; Perrone, G.S.; Murray, M.M. Can platelet-rich plasma enhance anterior cruciate ligament and meniscal repair? J. Knee Surg. 2015, 28, 19–28. [Google Scholar] [CrossRef]
- Kunze, K.N.; Pakanati, J.J.; Vadhera, A.S.; Polce, E.M.; Williams, B.T.; Panvaresh, K.C.; Chahla, J. The efficacy of platelet-rich plasma for ligament injuries: A systematic review of basic science literature with protocol quality assessment. Orthop. J. Sports Med. 2022, 10, 23259671211066504. [Google Scholar] [CrossRef]
- Collins, T.; Alexander, D.; Barkatali, B. Platelet-rich plasma: A narrative review. EFORT Open Rev. 2021, 6, 225–235. [Google Scholar] [CrossRef]
- Belk, J.W.; Kraeulter, M.J.; Thon, S.G.; Littlefield, C.P.; Smith, J.H.; McCarty, E.C. Augmentation of meniscal repair with platelet-rich plasma: A systematic review of comparative studies. Orthop. J. Sports Med. 2020, 8, 2325967120926145. [Google Scholar] [CrossRef]
- Herdea, A.; Struta, A.; Derihaci, R.P.; Ulici, A.; Costache, A.; Furtunescu, F.; Toma, A.; Charkaoui, A. Efficiency of platelet-rich plasma therapy for healing sports injuries in young athletes. Exp. Ther. Med. 2022, 23, 215. [Google Scholar] [CrossRef]
- Sanchez, M.; Anitua, E.; Orive, G.; Mukika, I.; Andia, I. Platelet-rich therapies in the treatment of orthopaedic sport injuries. ASports Med. 2009, 39, 345–354. [Google Scholar] [CrossRef]
- Sharun, K.; Jambagi, K.; Dhama, K.; Kumar, R.; Pawde, A.M. Amarpal, Therapeutic potential of platelet-rich plasma in canine medicine. Arch. Razi Inst. 2021, 76, 721–730. [Google Scholar] [CrossRef]
- Cash, C.; Scott, L.; Walden, R.L.; Kuhn, A.; Bowman, E. Bibliometric analysis of the top 50 highly cited articles on platelet-rich plasma in osteoarthritis and tendinopathy. Regen. Med. 2022, 17, 491–506. [Google Scholar] [CrossRef] [PubMed]
- Sax, O.C.; Chen, Z.; Mont, M.A.; Delanois, R.E. The efficacy of platelet-rich plasma for the treatment of knee osteoarthritis symptoms and structural changes: A systematic review and meta-analysis. J. Arthroplast. 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- Trams, E.; Malesa, K.; Pomianowski, S.; Kaminski, R. Role of platelets in osteoarthritis-updated systematic review and meta-analysis on the role of platelet-rich plasma in osteoarthritis. Cells 2022, 11, 1080. [Google Scholar] [CrossRef] [PubMed]
- Venosa, M.; Calafiore, F.; Mazzoleni, M.; Romanini, E.; Cerciello, S.; Calvisi, V. Platelet-rich plasma and adipose-derived mesenchymal stem cells in association with arthroscopic microfracture of knee articular cartilage defects: A pilot randomized controlled trial. Adv. Orthop. 2022, 2022, 6048477. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Yang, G.; Zhang, H.; Li, X.; Lu, Y. A systematic review on the efficacy of different types of platelet-rich plasma in the management of lateral epicondylitis. J. Shoulder Elb. Surg. 2022, 13, 1533–1544. [Google Scholar] [CrossRef]
- Barman, A.; Sinha, M.K.; Sahoo, J.; Jena, D.; Patel, V.; Patel, S.; Bhattacharjee, S.; Baral, D. Platelet-rich plasma injection in the treatment of patellar tendinopathy: A systematic review and meta-analysis. Knee Surg. Relat. Res. 2022, 34, 22. [Google Scholar] [CrossRef]
- Mishra, A.; Pavelko, T. Treatment of chronic elbow tendinosis with buffered platelet-rich plasma. Am. J. Sports Med. 2006, 34, 1774–1778. [Google Scholar] [CrossRef]
- Murray, M.M.; Spindler, K.P.; Abreu, E.; Muller, J.A.; Nedder, A.; Kelly, M.; Frino, J.; Zurakowski, D.; Valenza, M.; Snyder, B.D.; et al. Collen-platelet ricj plasma hydrogel enhances primary repair of the porcine anterior cruciate ligament. J. Orthop. Res. 2007, 25, 81–91. [Google Scholar] [CrossRef]
- Braun, H.J.; Wasterlain, A.S.; Dragoo, J.L. The use of PRP in ligament and meniscal healing. Sports Med. Arthrosc. Rev. 2013, 21, 206–212. [Google Scholar] [CrossRef]
- Chang, Y.; Yang, M.; Ke, S.; Zhang, Y.; Xu, G.; Li, Z. Effect of platelet-rich plasma on intervertebral disc degeneration in vivo and in vitro: A critical review. Oxid. Med. Cell Longev. 2020, 2020, 8893819. [Google Scholar] [CrossRef]
- Li, P.; Zhang, R.; Zhou, Q. Efficacy of platelet-rich plasma in retarding intervertebral disc degeneration: A meta-analysis of animal studies. Biomed. Res. Int. 2017, 2017, 7919201. [Google Scholar] [CrossRef] [PubMed]
- Basso, M.; Cavagnaro, L.; Zanirato, A.; Divano, S.; Formica, C.; Formica, M.; Felli, L. What is the clinical evidence on regenerative medicine in intervertebral disc degeneration? Musculoskelet. Surg. 2017, 101, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Akeda, K.; Ohishi, K.; Takegami, N.; Sudo, T.; Yamada, J.; Fujiwara, T.; Niimi, R.; Matsumoto, T.; Nishimura, Y.; Ogura, T.; et al. Platelet-rich plasma releasate versu corticosteroid for the treatment of discogenic low back paIn A double-blind randomized controlled trial. J. Clin. Med. 2022, 11, 304. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.B.; Adesida, A.B. Angiogenic approaches to meniscal healing. Injury 2018, 49, 467–472. [Google Scholar] [CrossRef]
- Anz, A.W.; Hackel, J.G.; Nilsson, E.C.; Andrews, J.R. Application of biologics in the treatment of the rotator cuff, meniscus, cartilage, and osteoarthritis. J. Am. Acad. Orthop. Surg. 2014, 22, 68–79. [Google Scholar] [CrossRef]
- Halper, J. Advances in the use of growth factors for treatment of disorders of soft tissues. Adv. Exp. Med. Biol. 2014, 802, 59–76. [Google Scholar] [CrossRef]
- Liu, X.; Zhu, B.; Li, Y.; Liu, X.; Guo, S.; Wang, C.; Li, S.; Wang, D. The role of vascular endothelial growth factor in tendon healing. Front. Physiol. 2021, 12, 766080. [Google Scholar] [CrossRef]
- Molloy, T.; Wang, Y.; Murrell, G. The roles of growth factors in tendon and ligament healing. Sports Med. 2003, 33, 381–394. [Google Scholar] [CrossRef]
- Nakamura, N.; Timmermann, S.A.; Hart, D.A.; Kaneda, Y.; Shrive, N.G.; Shino, K.; Ochi, T.; Frank, C.B. A comparison of in vivo gene delivery methods for antisense therapy in ligament healing. Gene Ther. 1998, 5, 1455–1561. [Google Scholar] [CrossRef][Green Version]
- Pittenger, M.F.; Dischert, D.E.; Peault, B.M.; Phinney, D.G.; Hare, J.M.; Caplan, A.I. Mesenchymal stem cell perspective: Cell biology to clinical progress. npj Regen. Med. 2019, 4, 22. [Google Scholar] [CrossRef]
- Hart, D.A. What molecular recognition systems do mesenchymal stem cells/medicinal signaling cells (MSC) use to facilitate cell-cell and cell-matrix interactions? A review of evidence and options. Int. J. Mol. Sci. 2021, 22, 8637. [Google Scholar] [CrossRef] [PubMed]
- Ando, W.; Kutcher, J.J.; Krawetz, R.; Sen, A.; Nakamura, N.; Frank, C.B.; Hart, D.A. Clonal analysis of synovial fluid stem cells to characterize and identify stable mesenchymal stromal cell/mesenchymal progenitor cell phenotypes in a porcine model: A cell source with enhancec commitment of the chondrogenic lineage. Cytotherapy 2014, 16, 776–788. [Google Scholar] [CrossRef] [PubMed]
- Hart, D.A. Perspective: Is it time to rename MSC (mesenchymal stem cells/medicinal signaling cells) with a name that reflects their combined in vivo functions and their in vitro abilities?—Possibly “pluripotent mesenchymal regulatory cells (PMRC)”. J. Biomed. Sci. Eng. 2021, 14, 317–324. [Google Scholar] [CrossRef]
- Motejunas, M.W.; Bonneval, L.; Carter, C.; Reed, D.; Ehrhardt, K. Biologic therapy in chronic pain management: A review of the clinical data and future investigations. Curr. Pain Headache Rep. 2021, 25, 30. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, P.A.; de la Mata Lloyd, J. Expanded mesenchymal stromal cells in knee osteoarthritis: A systematic literature review. Rheumatol. Clin. 2022, 18, 49–55. [Google Scholar] [CrossRef]
- Hernigou, J.; Vertongen, P.; Rasschaert, J.; Hernigou, P. Role of scaffolds, subchondral, intra-articular injections of fresh autologous bone marrow concentrate regenerative cells in treating human knee cartilage lesion: Different approaches and different results. Int. J. Mol. Sci. 2021, 22, 3844. [Google Scholar] [CrossRef]
- El-Kadiry, A.E.; Lumbao, C.; Salame, N.; Rafei, M.; Shammaa, R. Bone marrow aspirate concentrate versus platelet-rich plasma for treating knee osteoarthritis: A one-year non-randomized retrospective comparative study. BMC Musculoskelet. Disord. 2022, 23, 23. [Google Scholar] [CrossRef]
- Caplan, A.I. Mesenchymal stem cells: Time to change the name! Stem Cells Transl. Med. 2017, 6, 1445–1451. [Google Scholar] [CrossRef]
- Harris, Q.; Seto, J.; O’Brien, K.; Lee, P.S.; Kondo, C.; Heard, B.J.; Hart, D.A.; Krawetz, R.J. Monocyte chemotactic protein-1 inhibits chondrogenesis of synovial mesenchymal progenitor cells: An in vitro study. Stem Cells 2013, 31, 2253–2265. [Google Scholar] [CrossRef]
- Krawetz, R.J.; Wu, Y.E.; Martin, L.; Rattner, J.B.; Matyas, J.R.; Hart, D.A. Synovial fluid progenitors expressing CD90+ from normal but not osteoarthritic joints undergo chondrogenic differentiation without micro-mass culture. PLoS ONE 2012, 7, e43616. [Google Scholar] [CrossRef]
- Cabral, J.; Ryan, A.E.; Griffin, M.D.; Ritter, T. Extracellular vesicles as modulators of wound healing. Adv. Drug Deliv. Rev. 2018, 129, 394–406. [Google Scholar] [CrossRef] [PubMed]
- Harrell, C.R.; Jovicic, N.; Djonov, V.; Arsenijevic, N.; Volarevic, V. Mesenchymal stem cell-derived exosomes and other extracellular vesicles as new remedies in the therapy of inflammatory diseases. Cells 2019, 8, 1605. [Google Scholar] [CrossRef] [PubMed]
- Casado-Diaz, A.; Quesada-Gomez, J.M.; Dorada, G. Extracellular vesicles derived from mesenchymal stem cells (MSC) in regenerative medicine: Applications in skin wound healing. Front. Bioeng. Biotechnol. 2020, 8, 146. [Google Scholar] [CrossRef] [PubMed]
- Roefs, M.T.; Sluijter, J.P.G.; Vader, P. Extracellular vesicle-associated proteins in tissue repair. Trends Cell Biol. 2020, 30, 990–1013. [Google Scholar] [CrossRef]
- Shimomura, K.; Uasui, Y.; Koisumi, K.; Chijimatsu, R.; Hart, D.A.; Yonetani, Y.; Ando, W.; Nishi, T.; Kanamoto, T.; Horibe, S.; et al. First-in-human pilot study of implantation of a scaffold-free tissue-engineered construct generated from autologous synovial mesenchymal stem cells for the repair of knee chondral lesions. Am. J. Sports Med. 2018, 46, 2384–2393. [Google Scholar] [CrossRef]
- Malekpour, K.; Hazrati, A.; Zahar, M.; Markov, A.; Zekiy, A.O.; Navashenaq, J.G.; Roshangar, L.; Ahmadi, M. The potential use of mesenchymal stem cells and their derived exosomes for orthopedic diseases treatment. Stem Cell Rev. Rep. 2022, 18, 933–951. [Google Scholar] [CrossRef]
- Ren, S.; Wang, C.; Guo, S. Review of the role of mesenchymal stem cells and exosomes derived from mesenchymal stem cells in the treatment of orthopedic disease. Med. Sci. Monit. 2022, 28, e935937. [Google Scholar] [CrossRef]
- Longhini, A.L.; Salazar, T.E.; Vieira, C.; Trinh, T.; Duan, Y.; Pay, L.M.; Calzi, S.L.; Losh, M.; Johnston, N.A.; Xie, H. Peripheral blood-derived mesenchymal stem cells demonstrate immunomodulatory potential for therapeutic use in horses. PLoS ONE 2019, 14, e0212642. [Google Scholar] [CrossRef]
- Zha, K.; Li, X.; Yang, Z.; Tian, G.; Sun, Z.; Sui, X.; Dai, Y.; Liu, S.; Guo, Q. Heterogeneity of mesenchymal stem cells in cartilage regeneration: From characterization to application. NPJ Regen. Med. 2021, 6, 14. [Google Scholar] [CrossRef]
- Vahedi, P.; Moghaddamshahabi, R.; Webster, T.J.; Koyuncu, A.C.C.; Ahmadian, E.; Khan, W.S.; Mohamed, A.J.; Eftekhari, A. The use of infrapatellar fat pad-derived mesenchymal stem cells in articular cartilage regeneration: A review. Int. J. Mol. Sci. 2021, 22, 9215. [Google Scholar] [CrossRef]
- Meng, H.Y.H.; Lu, V.; Khan, W. Adipose tissue-derived mesenchymal stem cells as a potential restorative treatment for cartilage defects: A PRISMA review and meta-analysis. Pharmaceuticals 2021, 14, 1280. [Google Scholar] [CrossRef] [PubMed]
- Leong, D.J.; Sun, H.B. Mesenchymal stem cells in tendon repair and regeneration: Basic understanding and translational challenges. Ann. N. Y. Acad. Sci. 2016, 1383, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.P.Y. Mesenchymal stem cell-derived extracellular vesicles for the promotion of tendon repair-an update of literature. Stem Cell Rev. Rep. 2021, 17, 379–389. [Google Scholar] [CrossRef]
- Meeremans, M.; Van de Walle, G.R.; Van Vlierberghe, S.; De Schauwer, C. The lack of a representative tendinopathy model hampers fundamental mesenchymal stem cell research. Front Cell Dev. Biol. 2021, 9, 651164. [Google Scholar] [CrossRef] [PubMed]
- Jang, K.M.; Lim, H.C.; Bae, J.H. Mesenchymal stem cells for enhancing biologic healing after anterior cruciate ligament injuries. Curr. Stem Cell Res. 2015, 10, 535. [Google Scholar] [CrossRef]
- Yu, H.; Adesida, A.; Jomha, N.M. Meniscus repair using mesenchymal stem cells—A comprehensive review. Stem Cell Res. Ther. 2015, 6, 86. [Google Scholar] [CrossRef]
- Chew, E.; Prakash, R.; Khan, W. Mesenchymal stem cells in human meniscal regeneration: A systematic review. Ann. Med. Surg. 2017, 24, 3–7. [Google Scholar] [CrossRef]
- Rhim, H.C.; Jeon, O.H.; Han, S.B.; Bae, J.H.; Suh, D.W.; Jang, K.M. Mesenchymal stem cells for enhancing biological healing after meniscal injuries. World J. Stem Cells 2021, 13, 1005–1029. [Google Scholar] [CrossRef]
- Zhou, Y.F.; Zhang, D.; Yan, W.T.; Lian, K.; Zhang, Z.Z. Meniscus regeneration with multipotent stromal cell therapies. Front. Bioeng. Biotechnol. 2022, 10, 796408. [Google Scholar] [CrossRef]
- Croft, A.S.W.; Illien-Junger, S.; Grad, S.; Guerrero, J.; Wangler, S.; Gantenbein, B. The application of mesenchymal stromal cells and their homing capabilities to regenerate intervertebral disc. Int. J. Mol. Sci. 2021, 22, 3519. [Google Scholar] [CrossRef]
- Laing, W.; Han, B.; Hai, Y.; Sun, D.; Yin, P. Mechanism of action of mesenchymal stem cell-derived exosomes in the intervertebral disc degeneration treatment and bone repair and regeneration. Front. Cell Dev. Biol. 2022, 9, 833840. [Google Scholar] [CrossRef] [PubMed]
- DiStefano, T.J.; Vaso, K.; Danias, G.; Chionuma, H.N.; Weiser, J.R.; Iatridis, J.C. Extracellular vesicles as an emerging treatment option for intervertebral disc degeneration: Therapeutic potential, translational pathways, and regulatory considerations. Adv. Healthc. Mater. 2022, 11, e100596. [Google Scholar] [CrossRef] [PubMed]
- Barbon, S.; Rajendran, S.; Bertalot, T.; Piccione, M.; Gasparella, M.; Parnigotto, P.P.; Di Liddo, R.; Concorni, M.T. Growth and differentiation of circulating stem cells after extensive ex vivo expansion. Tissue Eng. Regen. Med. 2021, 18, 411–427. [Google Scholar] [CrossRef] [PubMed]
- Shimomura, K.; Hamada, H.; Hart, D.a.; Ando, W.; Nishi, T.; Trattnig, S.; Nehrer, S.; Nakamura, N. Histological analysis of cartilage defects repaired with an autologous human stem cell construct 48 weeks postimplantation reveals structural details not detected by T2-mapping MRI. Cartilage 2021, 13 (Suppl. S1), 694S–706S. [Google Scholar] [CrossRef]
- Sart, S.; Jeske, R.; Chen, X.; Ma, T.; Li, Y. Engineering stem cell-derived extracellular matrices: Decellularization, characterization, and biological function. Tissue Eng. Part B Rev. 2020, 26, 402–422. [Google Scholar] [CrossRef]
- Venkataiah, V.S.; Yahata, Y.; Kitagawa, A.; Inagaki, M.; Kakiuchi, Y.; Nakano, M.; Suzuki, S.; Handa, K.; Saito, M. Clinical applications of cell-scaffold constructs for bone regeneration therapy. Cells 2021, 10, 2687. [Google Scholar] [CrossRef]
- Ahmed, E.; Saleh, T.; Xu, M. Recellularization of native tissue derived acellular scaffold with mesenchymal stem cells. Cells 2021, 10, 1787. [Google Scholar] [CrossRef]
- Luo, T.; Tan, B.; Zhu, L.; Wang, Y.; Liao, J. A review on the design of hydrogels with different stiffness and their effects on tissue repair. Front. Bioeng. Biotechnol. 2022, 10, 817391. [Google Scholar] [CrossRef]
- Messaoudi, O.; Henrionnet, C.; Bourge, K.; Loeuille, D.; Gillet, P.; Pinzano, A. Stem cells and extrusion 3D printing for hyaline cartilage engineering. Cells 2020, 10, 2. [Google Scholar] [CrossRef]
- Tharakan, S.; Khondkar, S.; Ilyas, A. Bioprinting of stem cells in multimaterial scaffolds and their applications in bone tissue engineering. Sensors 2021, 21, 7477. [Google Scholar] [CrossRef]
- Ando, W.; Tateishi, K.; Hart, D.A.; Katakai, D.; Tanaka, Y.; Nakata, K.; Hashimoto, J.; Fujie, H.; Shino, K.; Yoshikawa, H.; et al. Cartilage repair using an in vitro generated scaffold-free tissue-engineered construct derived from porcine synovial mesenchymal stem cells. Biomaterials 2007, 28, 5462–5470. [Google Scholar] [CrossRef] [PubMed]
- Moriguchi, Y.; Tateishi, K.; Ando, W.; Shimomura, K.; Yonetani, Y.; Kita, K.; Hart, D.A.; Gobbi, A.; Shino, K.; Yoshikawa, H.; et al. Repair of meniscal lesions using a scaffold-free tissue-engineered construct derived from allogenic synovial MSCs in a miniature swine model. Biomaterials 2013, 34, 2185–2193. [Google Scholar] [CrossRef] [PubMed]
- Shimomura, K.; Ando, W.; Fujie, H.; Hart, D.A.; Yoshikawa, H.; Nakamura, N. Scaffold-free tissue engineering for injured joint surface restoration. J. Exp. Orthop. 2018, 5, 2. [Google Scholar] [CrossRef] [PubMed]
- Shimomura, K.; Rothrauff, S.; Hart, D.A.; Hamamoto, S.; Kobayashi, M.; Yoshikawa, H.; Tuan, R.S.; Nakamura, N. Enhanced repair of meniscal hoop structure injuries using an aligned electrospun nanofibrous scaffold combined with a mesenchymal stem cell-derived tissue engineered construct. Biomaterials 2019, 192, 346–354. [Google Scholar] [CrossRef]
- Ishiguro, H.; Kaito, T.; Yarimitsu, S.; Hashimoto, K.; Okada, R.; Kushioka, J.; Chijimatsu, R.; Takenka, S.; Makino, T.; Saka, Y.; et al. Interbertebral disc regeneration with an adipose mesenchymal stem cell-derived tissue-engineered construct in a rat nucleotomy model. Acta Biomater. 2019, 87, 118–129. [Google Scholar] [CrossRef]
- Ando, W.; Fujie, H.; Moriguchi, Y.; Nansai, R.; Shimomura, K.; Hart, D.A.; Yoshikawa, H.; Nakamura, N. Detection of abnormalities in the superficial zone of cartilage repaired using a tissue engineered construct derived from synovial stem cells. Eur. Cell Mater. 2012, 24, 292. [Google Scholar] [CrossRef]
- MacConaill, M.A. The movements of bones and joints. IV. The mechanical structure of articulating cartilage. J. Bone Jt. Surg. 1951, B33, 251–257. [Google Scholar] [CrossRef]
- Takada, N.; Wada, I.; Sugimura, I.; Maruyama, H.; Matsui, N. A possible barrier function of the articular surface. Kaibogaku Zasshi. 1999, 74, 631–637. [Google Scholar]
- Kumar, P.; Oka, M.; Toguchida, J.; Kobayashi, M.; Uchida, E.; Nakamura, T.; Tanaka, K. Role of uppermost superficial layer of articular cartilage in the lubrication mechanism of joints. J. Anat. 2001, 1999, 241–250. [Google Scholar] [CrossRef]
- Hollander, A.P.; Dickinson, S.C.; Kafienah, W. Stem cells and cartilage development: Complexities of a simple tissue. Stem Cells 2010, 28, 1992–1996. [Google Scholar] [CrossRef]
- Wu, J.P.; Kirk, T.B.; Zheng, M.H. Study of the collagen structure in the superficial zone and physiological state of articular cartilage using a 3D confocal imaging technique. J. Orthop. Surg. Res. 2008, 3, 29. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, R.; Christian, R.G.; Nakano, T.; Aherne, F.X.; Thompson, J.R. Age related changes and osteochondrosis in swine articular and epiphyseal cartilage: Light and electron microscopy. Can. J. Comp. Med. 1981, 45, 188–195. [Google Scholar] [PubMed]
- Wan, H.; Ren, K.; Kaoer, H.J.; Sharma, P.K. Cartilage lamina splendens inspired nanostructured coating for biomaterial lubrication. J. Colloid Interface Sci. 2021, 594, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Choudhery, M.S. Strategies to improve regenerative potential of mesenchymal stem cells. World J. Stem Cells 2021, 13, 1845. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Wang, Y.; Zhu, L.; Liu, Y.; Li, W. Epigenetic regulation in mesenchymal stem cell aging and differentiation and osteoporosis. Stem Cells Int. 2020, 2020, 8836258. [Google Scholar] [CrossRef] [PubMed]
- Sadlik, B.; Jaroslawski, G.; Gladusz, D.; Puszkarz, M.; Markowska, M.; Paweler, K.; Bonuczkowski, D.; Oldak, T. Knee cartilage regeneration with umbilical cord mesenchymal stem cells embedded in collagen scaffold using dry arthroscopy technique. Adv. Exp. Med. Biol. 2017, 1020, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.H.; Na, S.M.; Ahn, H.W.; Kang, J.K.; Seon, J.K.; Song, E.K. Allogenic human umbilical cord blood-derived mesenchymal stem cells are more effective than bone marrow aspiration concentrate for cartilage regeneration after high tibial osteotomy in medial unicompartment osteoarthritis of the knee. Arthroscopy 2021, 37, 2521–2530. [Google Scholar] [CrossRef]
- Felson, D.T. Osteoarthritis as a disease of mechanics. Osteoarthr. Cartil. 2013, 21, 10–15. [Google Scholar] [CrossRef]
- Berenbaum, F.; Walker, C. Osteoarthritis and inflammation: A serious disease with overlapping phenotypic patterns. Postgrad. Med. 2020, 132, 377–384. [Google Scholar] [CrossRef]
- Radin, E.L.; Burr, D.B.; Caterson, B.; Fyhrie, D.; Brown, T.D.; Boyd, R.D. Mechanical determinants of osteoarthrosis. Semin. Arthritis Rheum. 1991, 21 (Suppl. S2), 12–21. [Google Scholar] [CrossRef]
- Frank, C.B.; Shrive, N.G.; Boorman, R.S.; Lo, I.K.Y.; Hart, D.A. New perspectives on bioengineering of joint tissues: Joint adaptation creates a moving target for engineering replacement tissues. Ann. Biomed. Eng. 2004, 32, 458. [Google Scholar] [CrossRef] [PubMed]
- Courties, A.; Berenbaum, F.; Sellam, J. The phenotypic approach to osteoarthritis: A look at metabolic syndrome-associated osteoarthritis. Jt. Bone Spine 2019, 86, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Thornton, G.M.; Shao, X.; Chung, M.; Sciore, P.; Boorman, R.S.; Hart, D.A.; Lo, I.K.Y. Changes in mechanical loading lead to tendon-specific alterations in MMP and TIMP expression: Influence of stress deprivation and intermittent cyclic hydrostatic compression on rat supraspinatus and Achilles tendon. Br. J. Sports Med. 2010, 44, 698–703. [Google Scholar] [CrossRef] [PubMed]
- Sarbacher, C.A.; Halger, J.T. Connective tissue and age-related diseases. Subcell. Biochem. 2019, 91, 281–310. [Google Scholar] [CrossRef]
- Siadat, S.M.; Zamboulis, D.E.; Thorpe, C.T.; Ruberti, J.W.; Connizzo, B.K. Tendon extracellular matrix assembly, maintenance and dysregulation throughout life. Adv. Exp. Med. Biol. 2021, 1348, 45–103. [Google Scholar] [CrossRef]
- Gumina, S.; Villani, C.; Arcen, V.; Fagnani, C.; Nistico, L.; Venditto, T.; Castagna, A.; Candela, V. Rotator cuff degeneration: The role of genetics. J. Bone Jt. Surg. Am. 2019, 101, 600–605. [Google Scholar] [CrossRef]
- Keener, J.D.; Patterson, B.M.; Orvets, N.; Chamberlain, A.M. Degenerative rotator cuff tears: Refining surgical indications based on natural history data. J. Am. Acad. Orthop. Surg. 2019, 27, 156. [Google Scholar] [CrossRef]
- Long, Z.; Nakagawa, K.; Wang, Z.; Amadio, P.C.; Zhao, C.; Gingery, A. Age-related cellular and microstructural changes to the rotator cuff enthesis. J. Orthop. Res. 2021; in press. [Google Scholar] [CrossRef]
- Klett, C.C. Hereditary disorders of connective tissue: A review. Wound Repair Regen. 1997, 5, 3–11. [Google Scholar] [CrossRef]
- Trudgian, J.; Trotman, S. Ehlers-Danlos syndrome and wound healing: Injury in a collagen disorder. Br. J. Nurs. 2011, 20, S10. [Google Scholar] [CrossRef]
- Handa, K.; Abe, S.; Suresh, V.V.; Fujieda, Y.; Oshikawa, M.; Orimoto, A.; Kobayashi, Y.; Yamada, S.; Yamaba, S.; Murakami, S.; et al. Fibrillin-1 insufficiency alters periodontal wound healing failure in a mouse model of Marfan syndrome. Arch. Oral Biol. 2018, 90, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Malfait, F.; Castori, M.; Francomano, C.A.; Giunta, C.; Kosho, T.; Byers, P.H. The Ehlers-Danlos syndromes. Nat. Rev. Dis. Primers 2020, 6, 64. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.; Chang, C.; Gershwin, M.E. Ehlers-Danlos syndrome: Immunologic contrasts and connective tissue comparisons. J. Transl. Autoimmun. 2020, 4, 100077. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Yan, L.; Stoddard, C.; Wang, X.; Yue, Z.; Crandall, L.; Robinson, T.; Chang, Y.; Denton, K.; Li, E.; et al. Recapitulating and correcting Marfan syndrome in a cellular model. Int. J. Biol. Sci. 2017, 13, 588. [Google Scholar] [CrossRef]
- Prentice, D.A.; Pearson, W.A.; Fogarty, J. Vascular Ehlers-Danlos syndrome: Treatment of a complex abdominal wound with vitamin C and mesenchymal stromal cells. Adv. Skin Wound Care 2021, 34, 1–6. [Google Scholar] [CrossRef]
- Shimomura, K.; Hamamoto, S.; Hart, D.A.; Yoshikawa, H.; Nakamura, N. Meniscal repair and regeneration: Current strategies and future perspectives. J. Clin. Orthop. Trauma 2018, 9, 247–253. [Google Scholar] [CrossRef]
- Murray, I.R.; Chahla, J.; Frank, R.M.; Piuzzi, N.S.; Mandelbaum, B.R.; Dragoo, J.L.; Members of the Biologics Association. Rogue stem cell clinics. Bone Jt. J. 2020, 102-B, 148–154. [Google Scholar] [CrossRef]
- Liska, M.G.; Crowley, M.G.; Borlongan, C.V. Regulated and unregulated clinical trials of stem cell therapies for stroke. Transl. Stroke Res. 2017, 8, 93–103. [Google Scholar] [CrossRef]
- Yeo-The, N.S.L.; Tang, B.L. Moral obligations in conducting stem cell-based therapy trials for autism spectrum disorder. J. Med. Ethics 2022, 48, 343–348. [Google Scholar] [CrossRef]
- Eliasberg, C.L.; Rodeo, S.A. Editorial Commentary: Cell-based therapies for articular cartilage repair require precise progenitor cell characterization and determination of mechanism of action. Arthroscopy 2021, 37, 3357–3359. [Google Scholar] [CrossRef]
- Knapik, D.M.; Evuarherhe, A., Jr.; Frank, R.M.; Steinwaches, M.; Rodeo, S.; Mumme, M.; Cole, B.J. Nonoperative and operative soft-tissue and cartilage regeneration and orthopaedic biologics of the knee: An orthoregeneration network (ON) foundation review. Arthroscopy 2021, 37, 2704–2721. [Google Scholar] [CrossRef] [PubMed]
- Rodeo, S. Cell therapy in orthopaedics: Where are we in 2019? Bone Jt. J. 2019, 101-B, 361–364. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Tissue | Species | Condition | Article Type | Year | Citation |
|---|---|---|---|---|---|
| Sports Injuries | Humans | Several | Review | 2022 | Herdea et al. [100] |
| Humans | Several | Review | 2009 | Sanchez et al. [101] | |
| MSK | Canine | Several | Review | 2021 | Sharun et al. [102] |
| Cartilage | Human | OA | Review | 2022 | Cash et al. [103] |
| Human | Knee OA | Review | 2022 | Sax et al. [104] | |
| Human | OA | Review | 2022 | Trams et al. [105] | |
| Human | OA | Review | 2020 | Kydd & Hart [86] | |
| Human | Defects | Trial | 2022 | Venosa et al. [106] | |
| Tendons | Human | Epicondylitis | Review | 2022 | Li et al. [107] |
| Human | Tendinopathy | Review | 2022 | Barman et al. [108] | |
| Human | Tendinopathy | Review | 2022 | Cash et al. [103] | |
| Human | Tendinosis | Trial | 2006 | Mishra & Pavelko [109] | |
| Ligaments | Porcine | ACL | Trial | 2007 | Murray et al. [110] |
| Human | ACL | Review | 2013 | Braun et al. [111] | |
| Human | ACL/MCL | Review | 2022 | Kunze et al. [97] | |
| IVD | Human | Degeneration | Review | 2020 | Chang et al. [112] |
| Animal | Degeneration | Review | 2017 | Li et al. [113] | |
| Human | Degeneration | Review | 2017 | Basso et al. [114] | |
| Human | Low Back Pain | Trial | 2022 | Akeda et al. [115] | |
| Menisci | Human | Sports | Review | 2022 | Herdea et al. [100] |
| Tissue | Species | Condition | Article Type | Year | Citation |
|---|---|---|---|---|---|
| Orthopedic Disease | Humans | Several | Review | 2022 | Malekpour et al. [138] |
| Humans | Several | Review | 2022 | Ren et al. [139] | |
| Horses | Lameness | Original | 2019 | Longhini et al. [140] | |
| Cartilage/OA | Human | General | Review | 2021 | Zha et al. [141] |
| Human | General | Review | 2021 | Vahedi et al. [142] | |
| Human | Defects | Review | 2021 | Meng et al. [143] | |
| Human | Defects | Trial | 2018 | Shimomura et al. [137] | |
| Tendons | Preclinical | General | Review | 2016 | Leong & Sun [144] |
| General | Injury | Review | 2021 | Liu et al. [145] | |
| Human | Tendinopathy | Review | 2021 | Meeremans et al. [146] | |
| Ligaments | Preclinical | ACL | Review | 2015 | Jang et al. [147] |
| Human | ACL | Review | 2015 | Jang et al. [147] | |
| Menisci | Preclinical | Injury | Review | 2015 | Yu et al. [148] |
| Human | Injury | Review | 2017 | Chew et al. [149] | |
| All | Injury | Review | 2021 | Rhim et al. [150] | |
| All | Injury | Review | 2022 | Zhou et al. [151] | |
| IVD | All | Degenerated | Review | 2021 | Croft et al. [152] |
| All | Degenerated | Review | 2022 | Liang et al. [153] | |
| All | Degeneration | Review | 2022 | DiStefano et al. [154] | |
| Muscle | Rat | Injury | Original | 2021 | Barbon et al. [155] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hart, D.A.; Nakamura, N. Creating an Optimal In Vivo Environment to Enhance Outcomes Using Cell Therapy to Repair/Regenerate Injured Tissues of the Musculoskeletal System. Biomedicines 2022, 10, 1570. https://doi.org/10.3390/biomedicines10071570
Hart DA, Nakamura N. Creating an Optimal In Vivo Environment to Enhance Outcomes Using Cell Therapy to Repair/Regenerate Injured Tissues of the Musculoskeletal System. Biomedicines. 2022; 10(7):1570. https://doi.org/10.3390/biomedicines10071570
Chicago/Turabian StyleHart, David A., and Norimasa Nakamura. 2022. "Creating an Optimal In Vivo Environment to Enhance Outcomes Using Cell Therapy to Repair/Regenerate Injured Tissues of the Musculoskeletal System" Biomedicines 10, no. 7: 1570. https://doi.org/10.3390/biomedicines10071570
APA StyleHart, D. A., & Nakamura, N. (2022). Creating an Optimal In Vivo Environment to Enhance Outcomes Using Cell Therapy to Repair/Regenerate Injured Tissues of the Musculoskeletal System. Biomedicines, 10(7), 1570. https://doi.org/10.3390/biomedicines10071570