1. Introduction
Euglena gracilis (EG) is a spindle-shaped unicellular microalga that lives in most freshwater habitats. EG can grow under both phototropic (autotropic) and heterotrophic conditions; when grown under phototropic conditions, it performs photosynthesis. EG is rich in storage granules called paramylon starch, a β-glucan known to engage Dectin-1 receptors on immune cells and contribute to immune-activating and immune-training events involving epigenetic and metabolic reprogramming [
1].
β-glucans are natural fibers found in the cell walls of cereal grains, bacteria, and fungi, with significantly different physical and chemical properties depending on the source. β-glucans have the ability to bind to several different Pattern Recognition Receptors (PRRs), including Toll-Like Receptors (TLRs) [
2] and Dectin receptors 1 and 2 [
3,
4]. Depending on the cell type and its epigenetic state, a cell may express different combinations of PRRs. The binding of β-glucans to different combinations of PRRs triggers selective downstream effects [
5].
While paramylon has received much attention as an immune modulator, we have previously documented complementary effects on immune activation by the non-paramylon aqueous fraction of whole EG algae [
6]. Both the aqueous fraction and paramylon triggered the activation of natural killer (NK) cells and NKT cells, as measured by increased expression of CD69. When cells were treated with whole EG algae, the increased CD69 expression was much more robust than for either fraction alone, suggesting synergistic effects between the paramylon and aqueous fractions. The regulation of additional cellular responses, such as reactive oxygen species production and resistance to oxidative stress, was strongly supported by both the whole EG algae and paramylon. The aqueous fraction contains antioxidants capable of entering into and protecting living cells from oxidative stress.
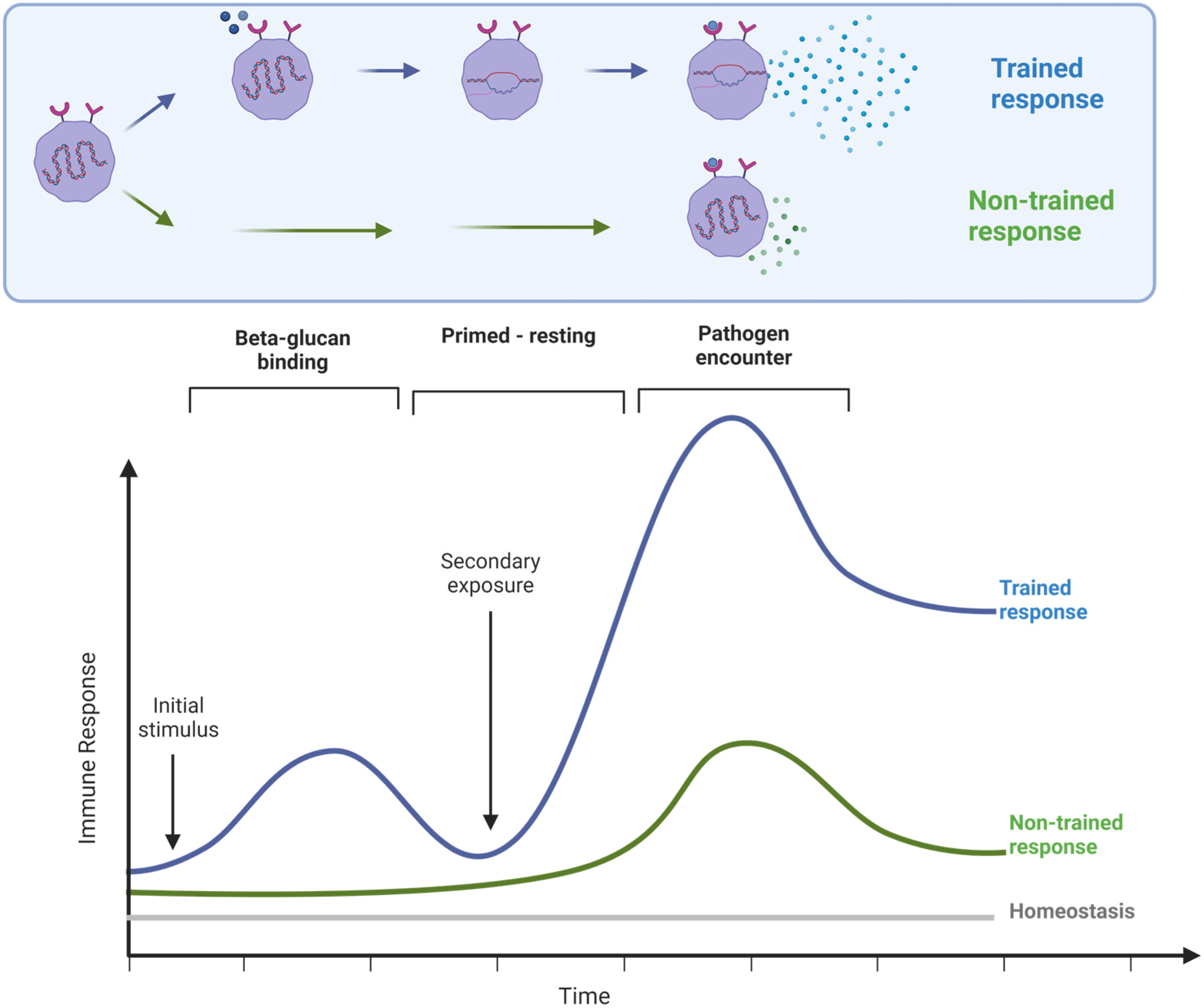
The classical understanding of long-term immune memory towards specific antigens involves the adaptive immune response, T and B lymphocyte activation, and hypermutation of genes for immunoglobulins, leading to long-term specific immunological memory toward highly-specific antigens, such as vaccine antigens. In addition, another type of immune memory involving the innate part of the immune system, responsible for immediate defense against invading pathogens, is becoming increasingly appreciated. This innate immune memory is also called trained immunity. β-glucans induce trained immunity, where immune cells that have been primed by binding of β-glucans to Dectin-1, and likely other cell surface receptors, respond more powerfully to a subsequent encounter with a pathogen [
7,
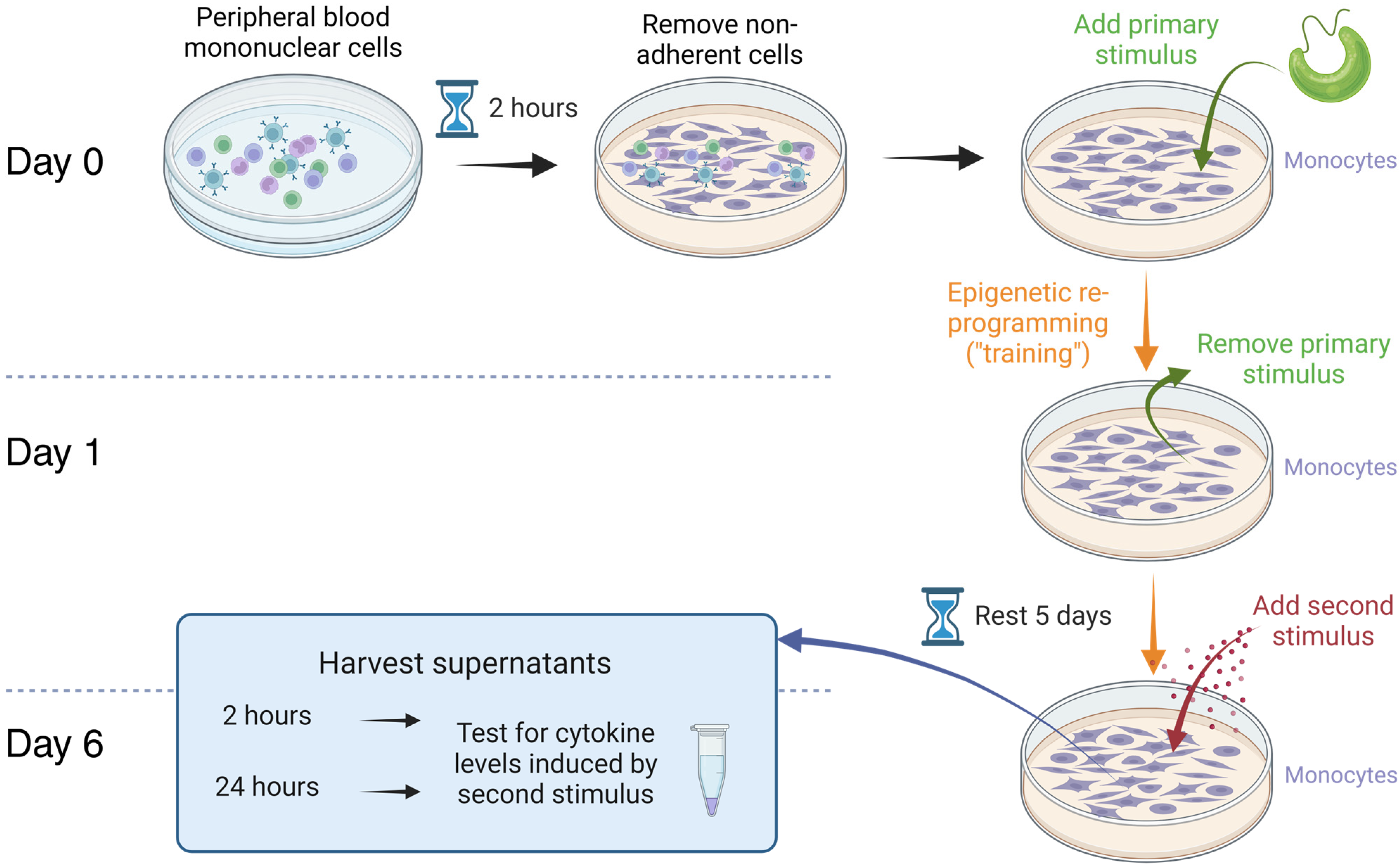
8]. To demonstrate ‘training’, it is necessary to document the magnitude of the second response to an immune trigger and compare it to the same stimulus on cells that were not previously stimulated (
Figure 1) [
9].
It has been demonstrated that EG and paramylon trigger cellular signaling in the intestinal tract and Peyer’s patches using intravital imaging; this is contrasted with the effects on intestinal sensory neurons, where only EG stimulated the cells while paramylon had no effect [
10]. A placebo-controlled parallel-arm 90-day study showed that healthy adults consuming EG experienced fewer sick days and symptoms compared to those consuming placebo [
11]. A placebo-controlled 8-week trial in severely stressed adults showed an increase in natural killer cell activity in participants consuming EG compared to participants consuming placebo [
12]. A 12-week study showed that consuming EG had positive effects on reducing tension and easing irritability associated with performing stressful mental tasks [
13]. A 4-week trial showed a significantly lower level of task-induced mental fatigue and a higher level of work efficiency when compared to the placebo group [
14].
The clinical trial reported here evaluated the effects of consuming
Euglena gracilis whole algae (EG) in 12 healthy subjects. Our overall approach was to document the effects of EG consumption using three distinct experimental models, based on the advantages that each methodological approach has to offer (
Figure 2). First, the in vivo model examined the effects of a single dose of EG on immune surveillance and immune cell trafficking within the body. From each blood sample, the numbers and activation status of innate immune cells were documented, following our previously published protocol [
15,
16,
17]. Secondly, as part of the clinical trial, an ex vivo model was applied to document the rapid re-programming of immune cells following EG consumption, where immune cells were cultured ex vivo, and the spontaneous versus inflammation-challenged cytokine production was evaluated. Lastly, the effects on isolated monocytes, as a model of the initiating events in the gut mucosa and Peyer’s patches, were studied in vitro and compared to the effects of pure EG-derived β-glucan. The results from this study are the first documentation of acute effects of EG consumption, evaluating the effectiveness of EG-induced trained immunity in humans using a combination of in vivo and ex vivo approaches.
2. Materials and Methods
2.1. Reagents
Blood collection tubes containing heparin (green-top, 6 mL vacutainer tubes, cat#367878), serum separator tubes (tiger-top, 8 mL vacutainer tubes, cat# 367988), and 21-gauge butterfly needles (cat# 367281) were purchased from Becton–Dickinson (Franklin Lakes, NJ, USA). Attune Focus fluid (cat# A24904), Performance tracking beads (cat# 4449754), wash and shut-down solutions (cat# A24974 and A24975), de-bubble buffer (cat# A10496), and High Yield Lysing buffer™ (cat# HYL250) were purchased from Thermo Fisher Scientific (Waltham, MA, USA). These monoclonal antibodies were obtained from Thermo Fisher Scientific (Waltham, MA, USA): Anti-CD3-Superbright™ 645 (clone OKT3, cat# 64-0037-42), anti-CD56-phycoerythrin (clone CMSSB, cat# 12-0567-42), and anti-CD69-fluorescein isothiocyanate (clone FN50, cat# 11-0699-42). The monoclonal anti-CD25-Brilliant Violet421 antibody (clone 2A3, cat# 564033) was obtained from BD Biosciences (Franklin Lakes, NJ, USA). Bio-Plex Pro™ human cytokine arrays were purchased from Bio-Rad Laboratories Inc. (Hercules, CA, USA).
Roswell Park Memorial Institute 1640 medium (cat# 11835030), penicillin–streptomycin 100× (cat# 15140-122), Fetal Bovine Serum (cat# A38401-01) phosphate-buffered saline (cat# 14190-235), lipopolysaccharide (LPS) from E. coli 026:B6 (cat# 50-112-9325), and lipopolysaccharide (LPS-EK) from E. coli K12 (cat# tlrl-eklps) were purchased from Thermo Fisher Scientific (Waltham, MA, USA). Interleukin-2 (IL-2) (cat# 17908-10KU) was purchased from Sigma-Aldrich Co. (St. Louis, MO, USA).
2.2. Study Design
A placebo-controlled cross-over study design was used for this clinical study (clinical trial registration NCT05431751), which was conducted in accordance with the Declaration of Helsinki, and approved by the Argus Independent Review Board, Tucson, AZ, USA. The sample size was determined based on previous studies on β-glucan-rich nutritional supplements and we aimed for a minimum of 10 participants to complete the study [
17]. People from the database at the study site, representing people who have previously indicated an interest in participating in clinical studies on natural products, were approached, and, if interested, were invited for screening. In the screening interview, we collected information on age, body mass index (BMI), medical/surgical history, diet and lifestyle, current health status, medication, and use of nutritional supplements. The following inclusion criteria were applied: healthy adult people of either gender, age 18–75 years (inclusive), body mass index (BMI) between 18.0 and 34.9 kg/m
2 (inclusive), veins easily accessible for multiple blood draws, and willing to comply with the study requirements—maintaining a consistent diet and lifestyle routine throughout the study, a consistent habit of bland breakfasts on days of clinic visits, abstaining from exercising and nutritional supplements on the morning of a study visit, abstaining from the use of coffee, tea, and soft drinks for at least one hour prior to a clinic visit, and abstaining from music, candy, gum, computer/cell phone use, during clinic visits.
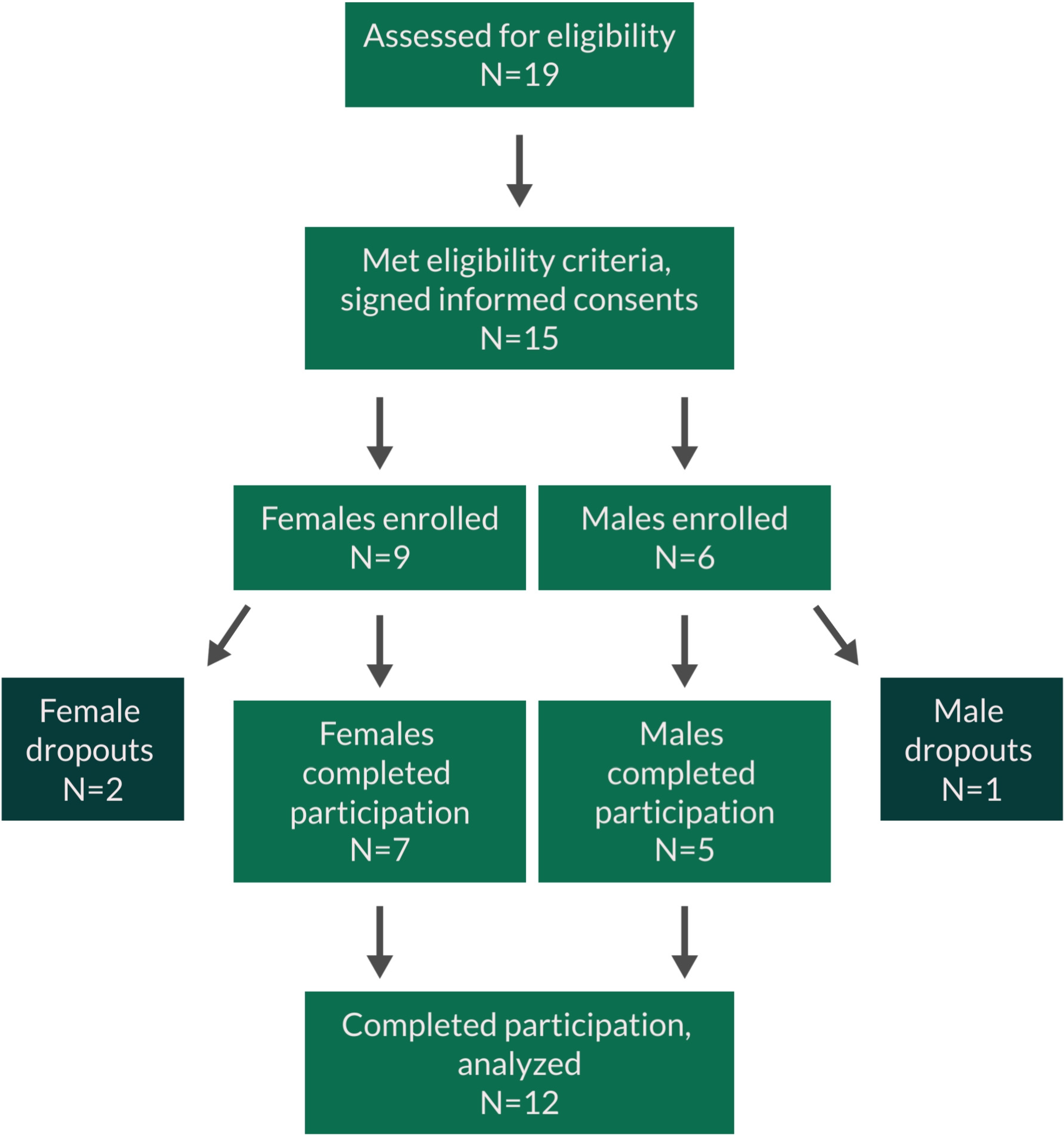
The following exclusion criteria were used: previous major gastrointestinal surgery (absorption of test product may be altered) (minor surgery not a problem, including previous removal of appendix and gall bladder); taking anti-inflammatory medications on a daily basis; currently in intensive athletic training (such as marathon runners); cancer during past 12 months; chemotherapy during past 12 months; currently treated with immune suppressant medication; diagnosed with autoimmune disorders, e.g., systemic lupus erythematosus, hemolytic anemia; donation of blood during the study or within the 4 weeks prior to the start of the study; received a cortisone shot within past 12 weeks; immunization during last month; currently taking antipsychotic, hypnotic, or anti-depressant prescription medication; ongoing acute infections (including teeth, sinus, ear, etc.); participation in another clinical trial study during this trial involving an investigational product or lifestyle change; an unusual sleep routine (examples: working graveyard shift, irregular routine with frequent late nights, studying, partying); unwilling to maintain a constant intake of supplements over the duration of the study; anxiety about having blood drawn; pregnant, nursing, or trying to become pregnant; known food allergies related to ingredients in active test product or placebo. If subjects met the inclusion criteria, they were informed that they qualified and were scheduled for clinic visits where they were enrolled into the study upon providing written informed consent. Fifteen people signed written informed consent, but one male and one female became unavailable due to a change in work schedule, and one female dropped out due to cold/flu onset. Twelve people finished the study participation (
Table 1), and their data were analyzed (
Figure 3).
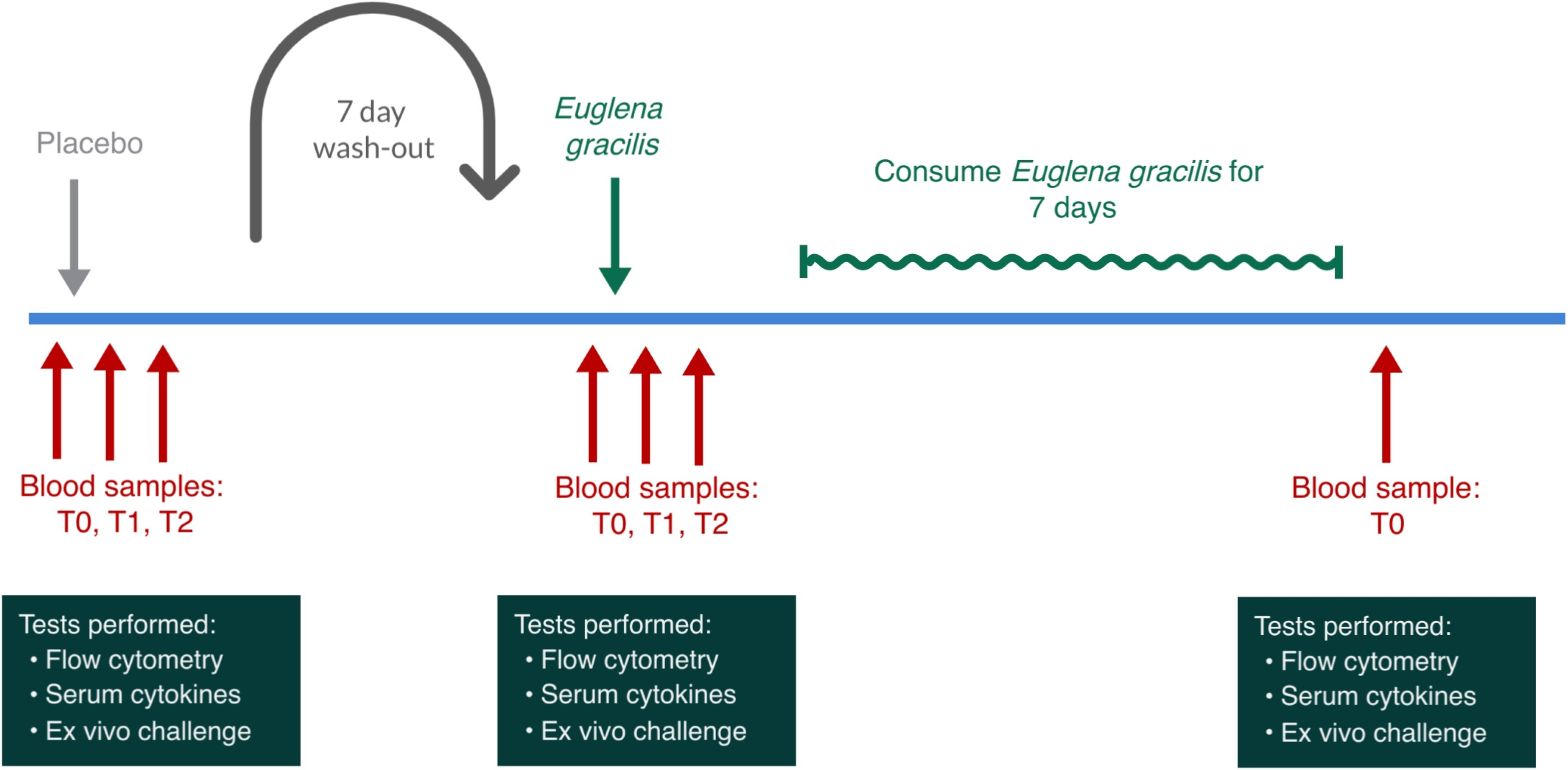
Study participants were scheduled for three clinic visits 1 week apart (
Figure 4). Due to the immune-training effects of β-glucans, the study was not randomized, and all participants received a placebo on the first clinic visit and EG on the second clinic visit. Through this non-randomized cross-over study design, we avoided biases that could result from EG-induced immune cell training affecting a subsequent visit where a placebo would be consumed. The participants received a single dose of placebo and the active product 1 week apart. After the second visit, participants consumed one daily dose of EG for 7 days and returned to the clinic for a blood draw to evaluate longer-term effects on the immune priming with daily consumption of EG. Below is a diagram illustrating the involvement of each participant.
For each participant, the visits were scheduled at the same time of the day during the morning hours of 7–11 am to minimize the effect of circadian fluctuations [
18,
19,
20,
21]. The first clinic visit involved consuming a placebo and served as a control for the circadian variations in cytokine levels and immune surveillance for each participant. Since there is a well-documented interference from exercise [
22] and stress [
23,
24,
25] with the release versus homing of lymphocytes, the study environment was managed so that any physical and mental stress was minimized during each visit. Upon arrival at a clinic visit, participants completed a questionnaire to help monitor exceptional circumstances that may influence the stress level of that person on that day. Predetermined criteria for rescheduling a visit included sleep deprivation and acute anxiety. After completing the questionnaire, volunteers were instructed to remain calm and inactive for 3 h, comfortably seated in a chair. After the first hour, the baseline blood sample was drawn. Immediately after the baseline sample was drawn, an encapsulated test product was provided with water and consumed in the presence of the clinic staff. Blood samples were drawn at 1 h and 2 h after consumption of the test product or placebo. For each blood draw, 14 mL of blood was drawn: eight milliliters of blood was drawn into a serum separator tube and allowed to coagulate for 30–60 min after which the tube was centrifuged for 15 min at 1500×
g at room temperature and the serum was harvested into a new tube, centrifuged for 10 min at 4 °C, aliquoted, and frozen at −80 °C for subsequent testing of cytokine profile. Six milliliters of blood were drawn into heparin vacutainer tubes for immunostaining, which was initiated within the hour of each blood draw. From each blood sample, the numbers and activation status of innate immune cells were documented [
15,
23,
24], and immune cells were cultured overnight to document the re-programming of the participants’ immune cells after consuming a single dose of EG compared to placebo.
2.3. Production of the Microalgae Material
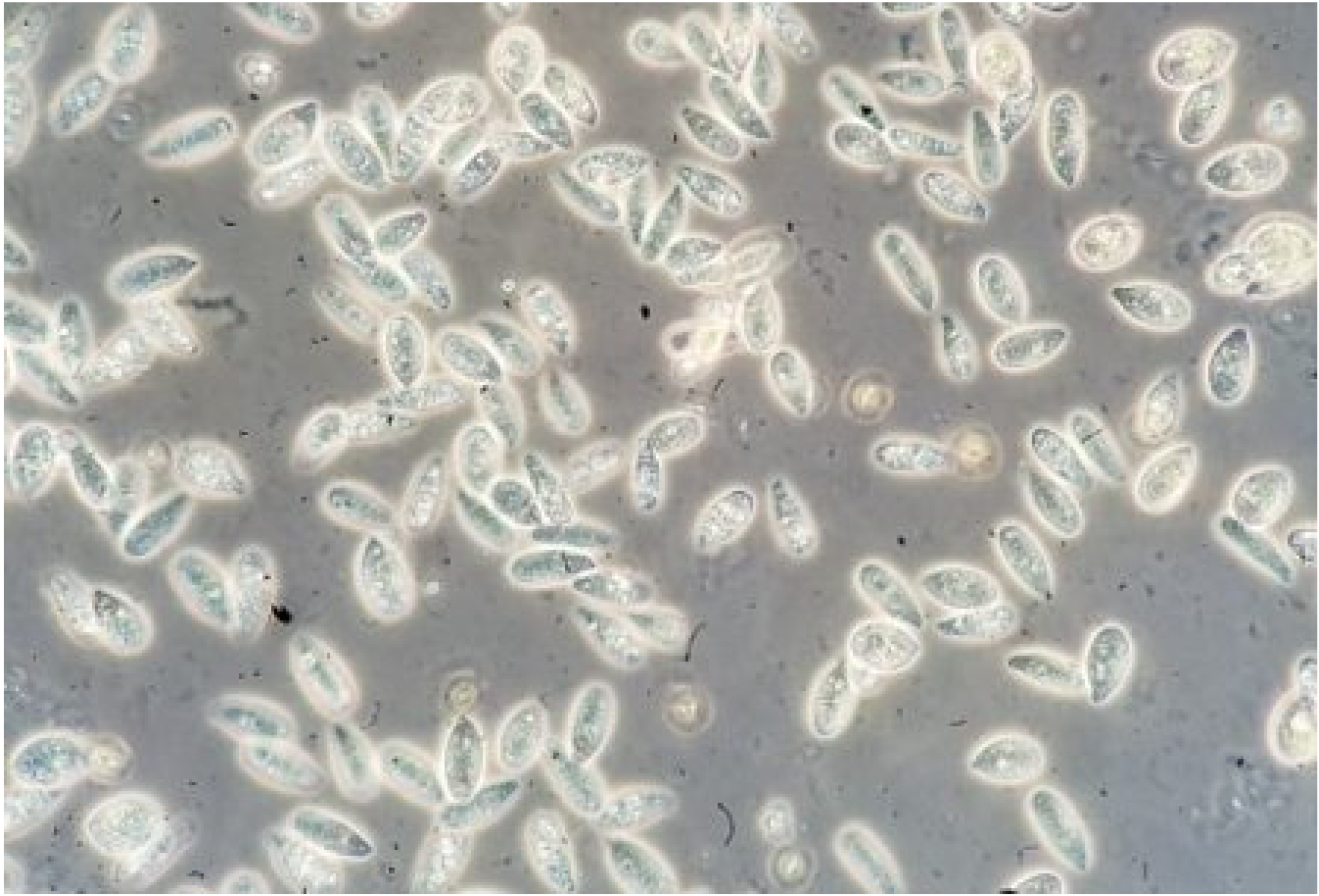
The whole unprocessed microalgae-based powder, BioGlena™, tested in this study was provided by Algatechnologies, Kibbutz Ketura, Israel. The single-celled alga
Euglena gracilis is grown by fermentation in closed bioreactors using a technology designed for obtaining a high content of β-glucan (
Figure 5). The powder contains a minimum of 50% linear β-glucan, complete protein, and essential vitamins and minerals (
Table 2).
2.4. Consumable Products for the Clinical Trial
Capsules of BioGlena™ powder of Euglena gracilis and matching placebo capsules containing plain rice flour were supplied by Algatechnologies Ltd., Kibbutz Ketura Hevel Eilot, Israel. On each clinic day, immediately after the baseline blood draw, study participants were given a single dose of either a placebo or the active test product in the presence of the clinic staff. The capsules with the active test product contained 375 mg EG. Participants consumed the capsules with water and a few bland soda crackers to stimulate digestive function.
2.5. Immune Cell Evaluation by Flow Cytometry
From each blood draw, triplicate samples of heparinized whole blood were stained with a panel of monoclonal antibodies focused on identifying NK cells, NKT cells, T cells, and monocytes, and documenting the expression levels of the CD25 and CD69 activation markers on those cell types.
To perform the staining, triplicate samples of 50 µL heparinized whole blood were stained with fluorochrome-conjugated monoclonal antibodies towards CD3, CD25, CD56, and CD69 and were incubated for at least 15 min at room temperature in the dark followed by the addition of 1 mL of High-Yield Lysing buffer, mixing, and incubation for at least 10 min at room temperature in the dark. Samples were transferred to 2 mL deep-well 96-well plates and acquired by flow cytometry within 1 h of staining.
All samples were acquired using an acoustic-focusing Attune™ Nxt flow cytometer (Thermo Fisher Scientific), using a microplate-based Autosampler. Data analysis utilized gating on forward/side scatter to identify lymphocyte and monocyte populations, followed by gating based on CD3 and CD56 markers, to allow enumeration of CD3+ CD56− T cells, CD3+ CD56+ NKT cells, CD3− CD56+ NK cells, and CD3− CD56− non-NK non-T cells. Each cell subset was then analyzed for expression levels of the activation markers CD25 and CD69.
2.6. Ex Vivo Immune Challenges
From each blood draw performed in the clinical trial, peripheral blood mononuclear cells (PBMCs) were purified and plated at 106/mL in 200 µL volumes in two different sets in U-bottom 96 well plates (Thermo Scientific, cat# 163320) in culture medium (Roswell Park Memorial Institute (RPMI) medium + 10% fetal calf serum + Penicillin-Streptomycin). No immune challenge was performed on the first set of cultures, and these cultures served as a way to monitor the spontaneous release of cytokines ex vivo after product consumption in vivo. To the second set of cultures, an immune challenge was performed: 0.01 mL of the inflammatory bacterial toxin LPS (cat# 50-112-9325) was added (5 µg/mL in cell culture). Culture supernatants were harvested at 24 h and banked frozen for cytokine testing.
2.7. Serum Levels of Cytokines, Chemokines, and Growth Factors
Serum samples from all blood draws were used for evaluation of changes to blood levels of 27 cytokines and chemokines, quantified using a Bio-Plex Pro Human Cytokine Grp I Panel protein array (cat# M500KCAF0Y) (Bio-Rad Laboratories Inc.) and utilizing xMAP technology (Luminex, Austin, TX, USA). The following markers were tested: Interleukin-1 beta (IL-1β), interleukin-1 receptor antagonist (IL-1ra), interleukin-2 (IL-2), interleukin-4 (IL-4), interleukin-5 (IL-5), interleukin-6 (IL-6), interleukin-7 (IL-7), interleukin-8 (IL-8), interleukin-9 (IL-9), interleukin-10 (IL-10), interleukin-12 (protein 70) (IL-12 (p70)), interleukin-13 (IL-13), interleukin-15 (IL-15), interleukin-17 (IL-17), eosinophil chemotactic protein (Eotaxin), basic fibroblast growth factor (Basic FGF), granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), interferon-gamma (IFN-γ), interferon gamma-induced protein 10 (IP-10), monocyte chemotactic protein 1 (MCP-1 (MCAF)), macrophage inflammatory protein 1 alpha (MIP-1α), macrophage Inflammatory protein 1 beta (MIP-1β), platelet-derived growth factor subunit beta (PDGF-BB), Regulated on Activation, Normal T cell Expressed and Secreted (RANTES), tumor necrosis factor-alpha (TNF-α), and vascular endothelial growth factor (VEGF).
2.8. Cytokines in Culture Supernatants from Ex Vivo and In Vitro PBMC Cultures
The culture supernatants from the 24 h ex vivo PBMC cultures from the clinical samples and the culture supernatants from the in vitro immune-training monocyte cultures were tested for the levels of seven cytokines and chemokines using Bio-Plex protein arrays (Bio-Rad Laboratories Inc.) and utilizing xMAP technology (Luminex, Austin, TX, USA). The following markers were tested: 24 h culture supernatants: IFN-γ, IL-1β, IL-6, IL-10, MIP-1β, TNF-α, and G-CSF; in vitro immune-training in monocyte cultures: IFN-γ, IL-1β, IL-1ra, IL-6, IL-10, TNF-α, and G-CSF.
2.9. Innate Immune Training In Vitro
A sample of bulk BioGlena™ powder of Euglena gracilis was supplied by Algatechnologies Ltd., Kibbutz Ketura Hevel Eilot, Israel. A stock solution was prepared fresh in phosphate-buffered saline. The stock solution was unfiltered and was introduced into cell cultures as a suspension of all algal components. Pure β-1,3-Glucan from Euglena gracilis was obtained from Sigma-Aldrich Co. (St. Louis, MO, USA) (cat# 89862).
The immune-training effects of the whole algae EG were compared to those of pure EG-derived β-glucan in a classical in vitro model using purified monocytes (
Figure 6) [
9]. Peripheral blood mononuclear cells (PBMCs) were plated in sterile flat-bottom 96-well microplates and incubated for 2 h at 37 °C and 5% CO
2 to allow monocyte adhesion. Lymphocytes were removed and the adherent monocytes were washed in warm PBS after which 0.18 mL fresh culture medium (Roswell Park Memorial Institute (RPMI) medium + 10% fetal calf serum + Penicillin-Streptomycin) was added to the wells. The initial stimulus for monocyte priming consisted of serial dilutions of EG, where each dose was tested in triplicate. One set of untreated cultures served as a negative control, where PBS was added instead of EG or LPS. Another set of untreated control wells was prepared so that the second stimulus could be added on Day 6.
After 24 h, the culture medium was exchanged with fresh medium without EG, thereby initiating the resting phase. After an additional 48 h, 0.08 mL culture medium was removed from each well, and 0.08 mL fresh culture medium was added. On day 6 after the culture was started, 0.1 mL medium was removed from each well and 0.09 mL fresh medium was added. Then, the second stimulus, 0.01 mL of the inflammatory bacterial toxin LPS-EK (cat# tlrl-eklps), was added (10 pg/mL in cell culture). Culture supernatants were harvested at 2 h and 24 h after the addition of the second stimulus and banked frozen for cytokine testing.
2.10. Statistical Analysis
The average and standard deviation for each data set were calculated using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA). Post-consumption changes from baseline to later assessments were evaluated by between-treatment analysis for each time point. This allowed evaluation of changes on the day a person consumed the active product, in the context of the person’s circadian changes on the day he/she consumed a placebo. The evaluation used within-subject analysis and the two-tailed paired t-test where statistical significance was set at p < 0.05, and a high level of significance at p < 0.01.
For the analysis of in vitro data, the average and standard deviation for each data set were calculated using Microsoft Excel. Statistical analysis of in vitro data was performed using the 2-tailed, independent t-test for all data sets, except for the in vitro testing for IL-1β, where the one-tailed test was used, as values were close to baseline. Statistical significance was set at p < 0.05, and a high level of significance at p < 0.01.
4. Discussion
This study evaluated the effects of consuming Euglena gracilis whole algae (EG) on immune cell activation, cellular trafficking, and cytokine levels, which are functions of the cumulative interplay between gut immune tissue, nerve stimulation, and immune cell communication. Secondly, as part of the clinical trial, ex vivo cell cultures were used to evaluate the effects of EG consumption on immune reprogramming and its impact on acute and long-term ex vivo cytokine production, spontaneously and in response to an inflammatory challenge. Finally, to understand the direct effects on purified macrophages, in vitro testing was conducted to evaluate the effects of EG- versus β-glucan-induced immune training on cytokine levels in inflammatory conditions as an in vitro model of the initiating effects at the gut level after consuming EG.
Consuming nutraceutical products represents a unique opportunity to provide rapid support for the natural processes of immune surveillance [
17,
26,
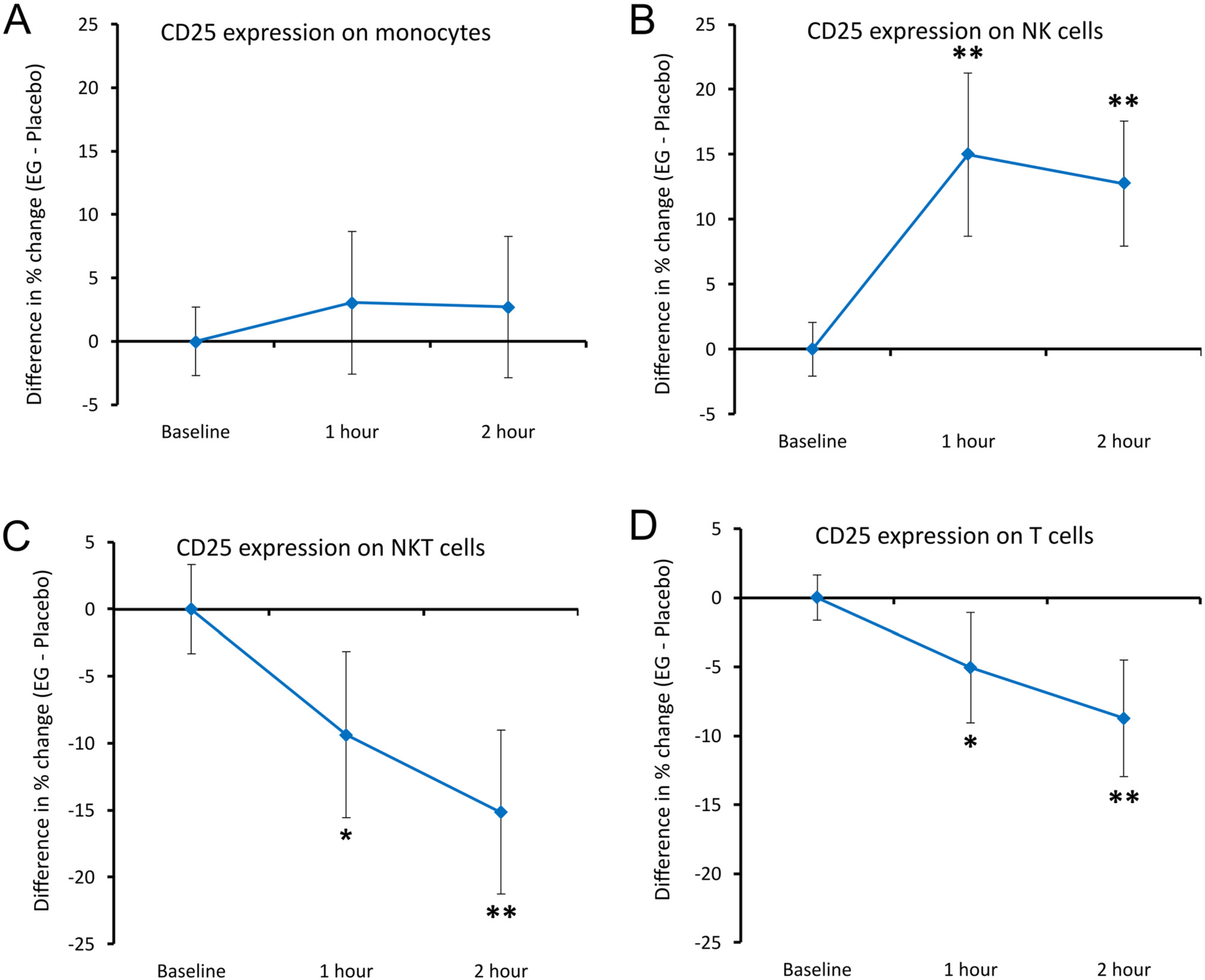
27]. The clinical data presented here showed rapid and highly significant changes to activation markers on NK cells, where the CD25 activation marker was significantly elevated at 1 h after consuming a single dose of EG compared to placebo, suggesting increased NK cell proliferative activity [
28], and possibly cytotoxic activity [
29]. Correlations have been reported between CD25 up-regulation and increased sensitivity to IL-2, where the heightened responsiveness of NK cells to re-stimulation by cytokines and target cells is indicative of a memory-like reactivity [
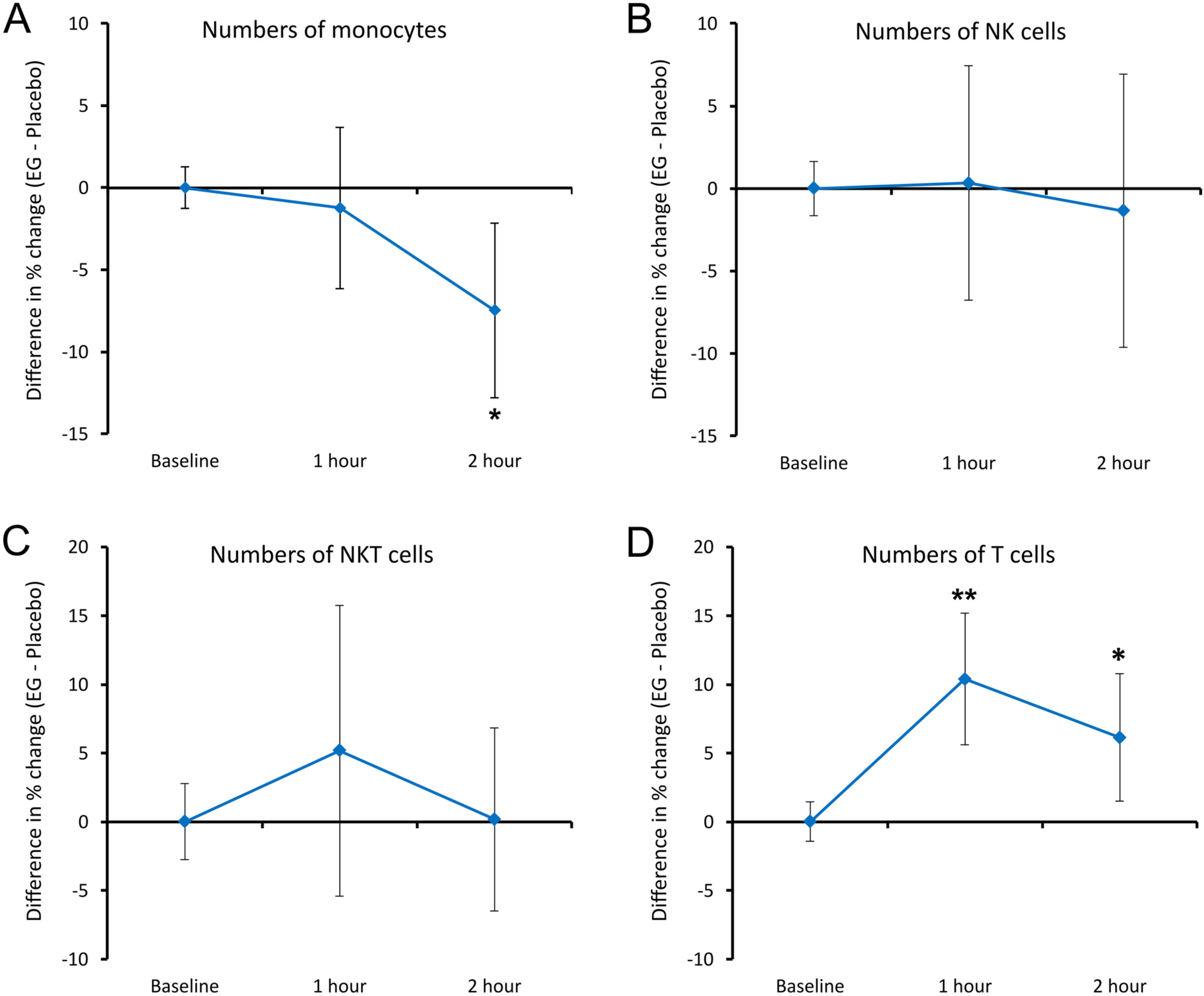
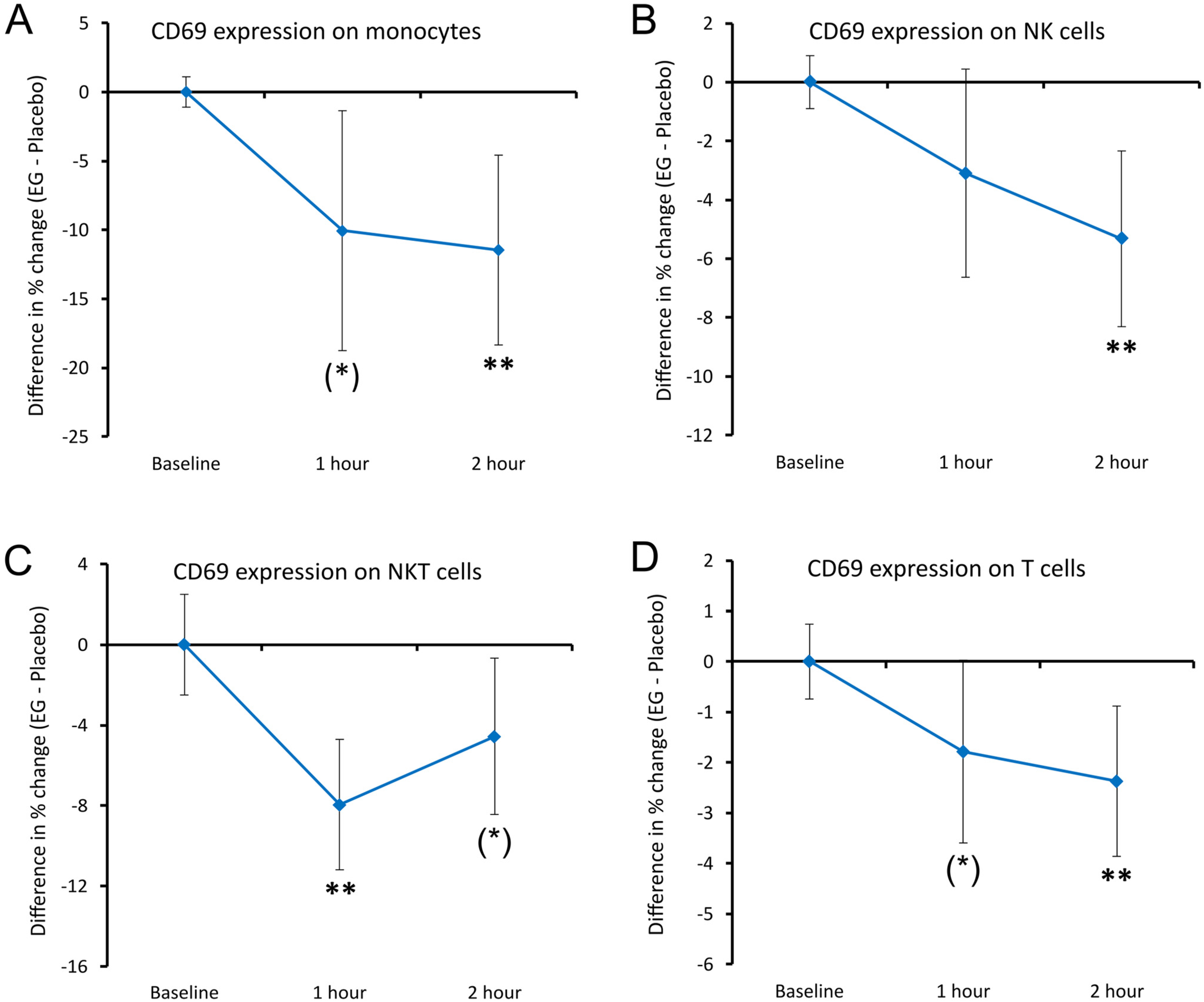
30]. Synchronous to our observations of increased CD25 expression, we also saw significantly reduced expression levels of CD69. This was not associated with changes to the total numbers of natural killer (NK) cells in the blood circulation, suggesting that, if changes to NK cell trafficking were induced, the number of NK cells migrating out of the blood was equal to the number entering back into the circulation. In addition, there was a rapid and highly significant increase in T cell mobilization after consuming a single dose of
Euglena gracilis (EG) whole algae, where T cells in the blood circulation expressed significantly lower levels of CD25 and lower levels of CD69.
In previous studies on nutraceutical modulation of immune surveillance, the changes to cell numbers in the blood circulation were typically associated with changes to cytokine levels. The consumption of a blend of botanicals and medical mushrooms showed rapid increases in IP-10 and MCP-1, in association with monocyte surveillance and increased CD25 expression on NKT and T cells [
17]. Consumption of an immunogenic yeast fermentate was associated with increased CD25 levels as well as T and NK cell migration, associated with significant changes in IFN-γ [
27]. Both these previous studies involved β-glucan-rich ingredients. Therefore, it is unique for the EG study presented here that there were no statistically significant changes to serum cytokines at 1–2 h after consumption. There are several possible reasons for this, where either cytokine changes happened rapidly and lost significance at 1 h, or there may have been individual differences in timing between different participants so the group averages for these changes did not reach significance.
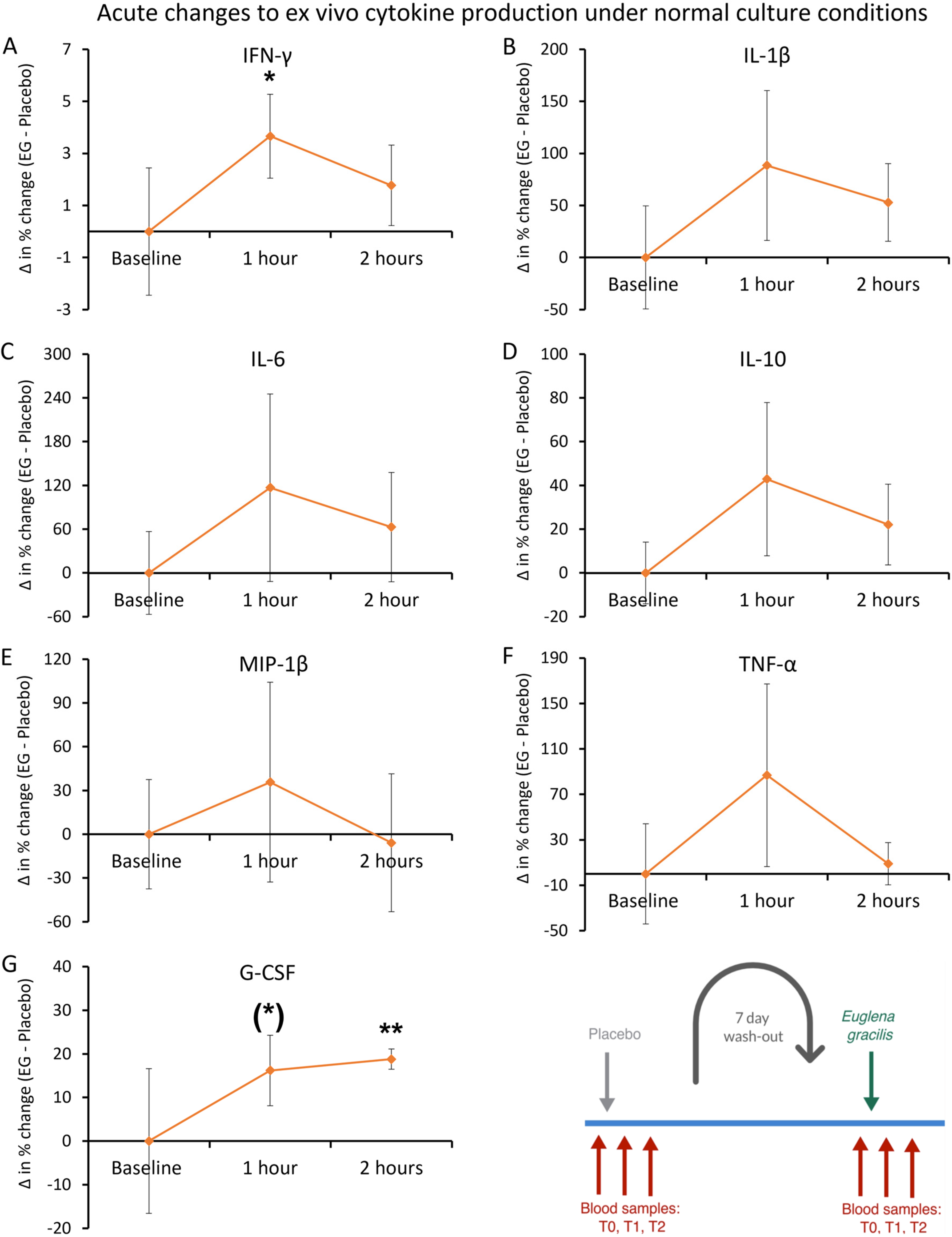
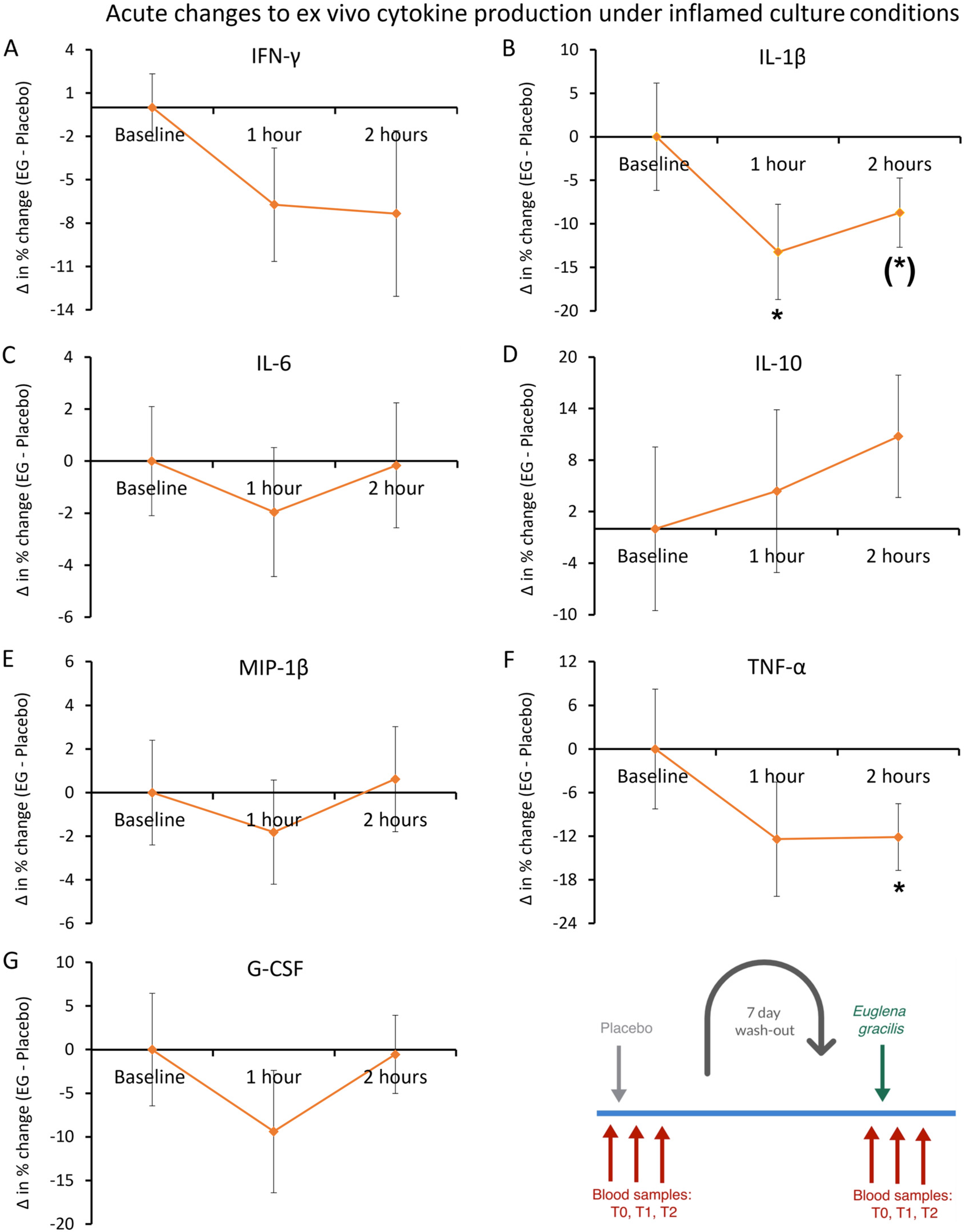
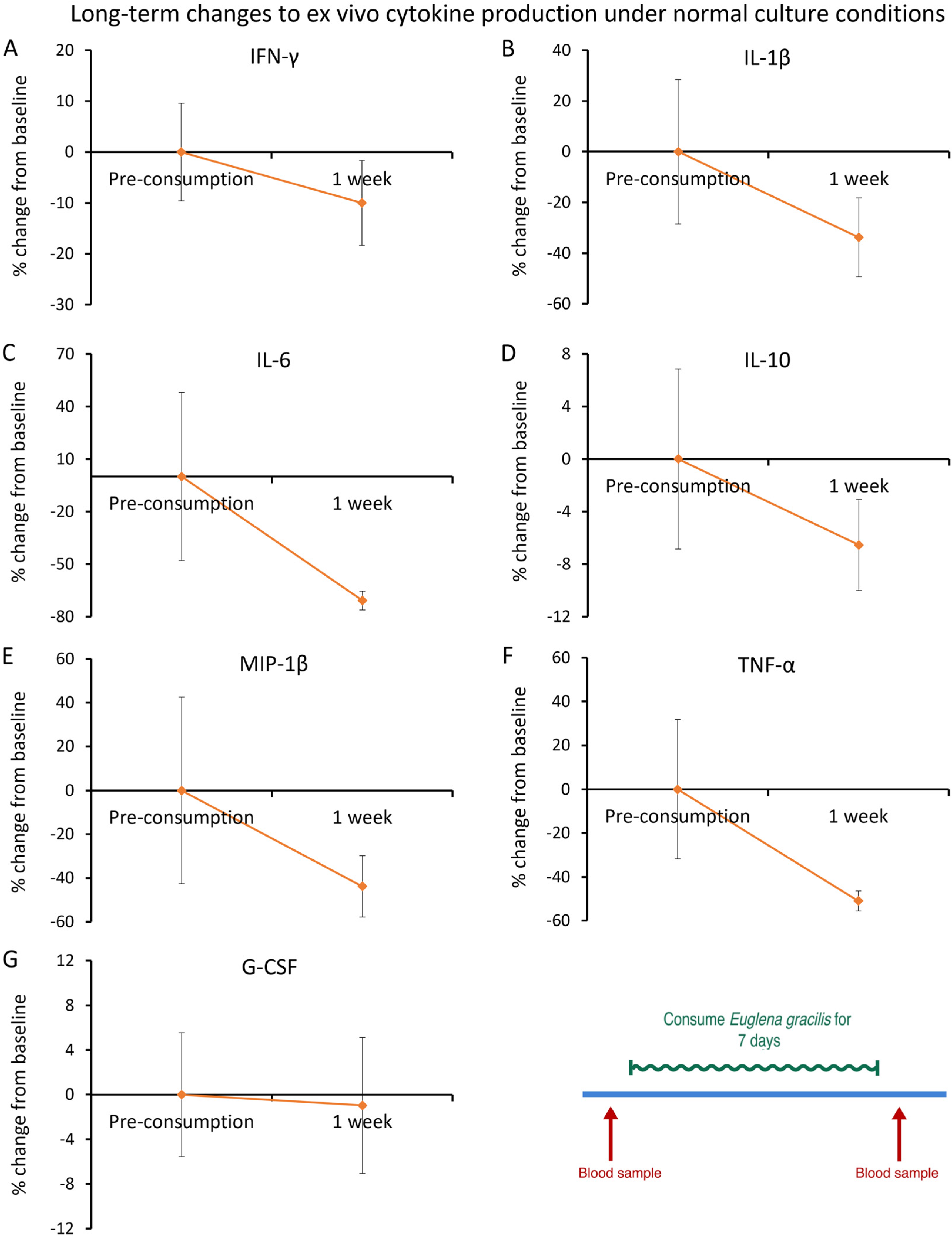
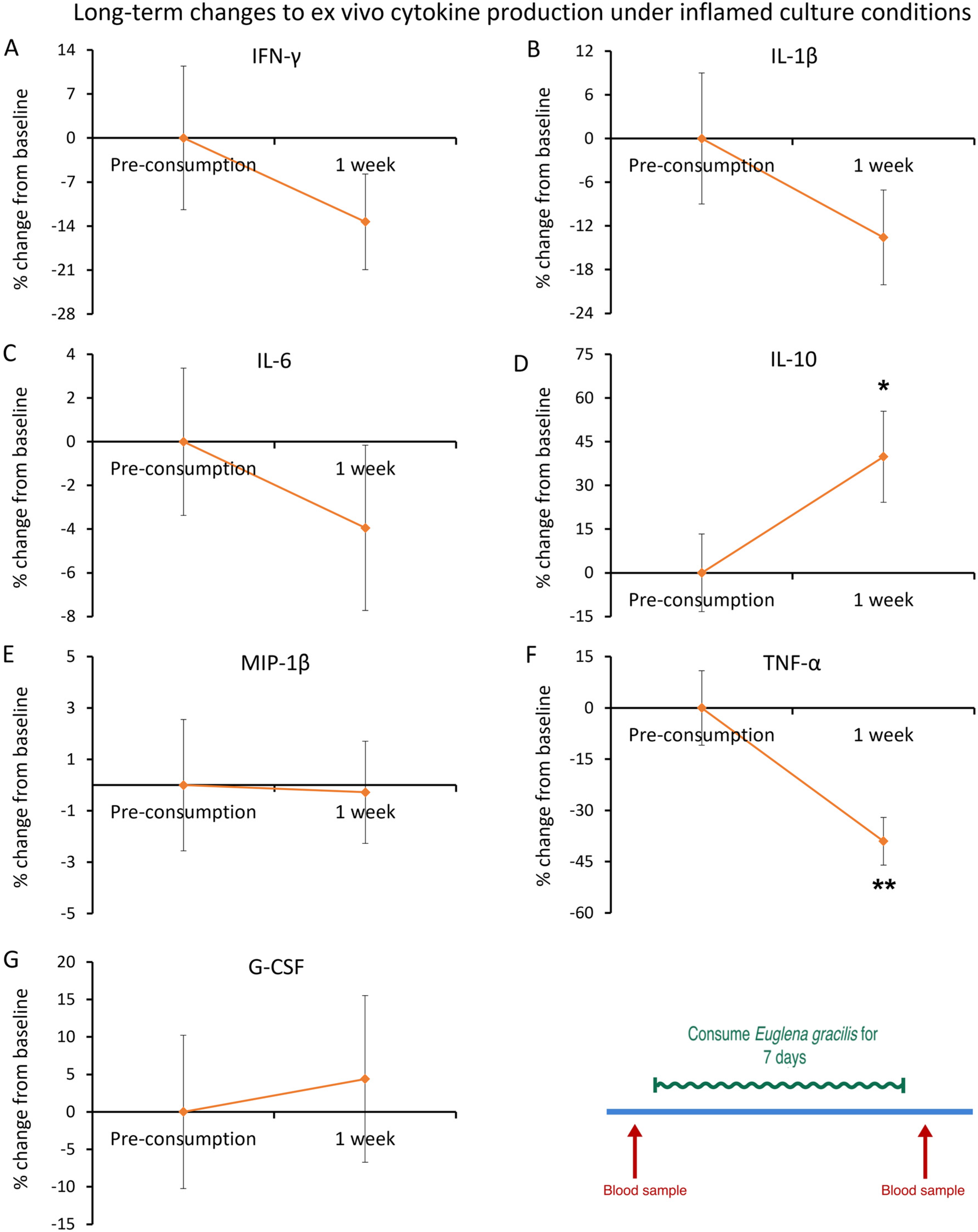
As part of the clinical study reported here, an ex vivo experimental approach was used to evaluate the effect of EG consumption on innate immune cells’ production of cytokines. Changes to spontaneous cytokine production ex vivo after consuming EG included a rapid increase in the levels of IFN-γ and G-CSF, demonstrating a swift epigenetic reprogramming of EG-primed immune cells. Contrary to the direct effects, ex vivo LPS-challenged PBMCs triggered a rapid decrease in the levels of IL-1β and TNF-α, with a concomitant increase in the level of the anti-inflammatory cytokine Interleukin-10 (IL-10) in response to EG priming in vivo. It is noteworthy that rapid and transient reductions in the levels of immune-activating cytokines such as IFN-γ, MIP-1β, and G-CSF were observed ex vivo following LPS-induced inflammation, despite not reaching statistical significance. This suggests the anti-inflammatory effects of EG consumption, resulting in the PBMCs being less responsive to inflammatory stimuli, such as LPS. After one week of EG consumption, the ex vivo PBMC cultures exhibited anti-inflammatory effects after an inflammatory challenge, as seen by a significant increase in the anti-inflammatory cytokine IL-10 and a highly significant decrease in the pro-inflammatory cytokine TNF-α. Our findings indicate the potential of EG to balance the beneficial and harmful effects of inflammation, and this modulation of the immune system may be key to the resolution of uncontrolled or excessive inflammation [
31,
32]. Collectively, this study suggests that priming immune cells with nonspecific stimuli, such as EG, may have protective effects during the inflammatory response to downstream challenges with pathogens unrelated to the original stimulus.
The immune-training effects of the whole algae EG were compared to pure EG-derived β-glucan, in a classical in vitro model using purified monocytes [
9]. When monocytes received EG as the primary stimulus, the cytokine levels after 2 h of the second stimulus showed a more robust increase in the production of IFN-γ, IL-1β, TNF-α, IL-1ra, and IL-10 than when monocytes received pure EG-derived β-glucan as the primary stimulus. The higher level of TNF-α was highly significant when compared to β-glucan-primed monocytes. Only the cytokine IL-6 was induced to similar levels by both EG and β-glucan. This superior burst in cytokine production after the second stimulus of EG-trained monocytes seen at 2 h was less evident at 24 h after the second stimulus. In the 24-h supernatants, only TNF-α remained higher in the EG-trained monocytes than in the β-glucan-trained monocyte cultures. We suggest that multiple synergistic components in the whole-EG algae facilitated the rapid increase while also supporting a faster return to homeostasis than in cultures primed with pure β-glucan. Further testing is needed to elucidate the anti-inflammatory effects of the non-β-glucan fraction of EG.
A number of potential clinical implications may be associated with enhancing the body’s resistance to infections. It is possible that through the rapid epigenetic reprogramming of EG-primed immune cells, trained immunity may be extended beyond innate immune cells and likely impact the generation of more effective adaptive immune responses and antibody production [
33]. Further research is required to understand how the rapid reprogramming of EG-primed immune cells impacts adaptive immunity as well as the potential for the development of effective therapeutic interventions using natural products [
34]. Thus, this presents a unique opportunity for the development of EG-based nutraceutical interventions which may offer non-specific protection and potentially serve as a preventive therapy as well as enhancing immune resistance in immunocompromised populations.


 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}