A Multicenter, Randomized, Open-Labeled, Parallel Group Trial of Sildenafil in Alcohol-Associated Erectile Dysfunction: The Impact on Psychosocial Outcomes

Abstract
:
1. Introduction
2. Method
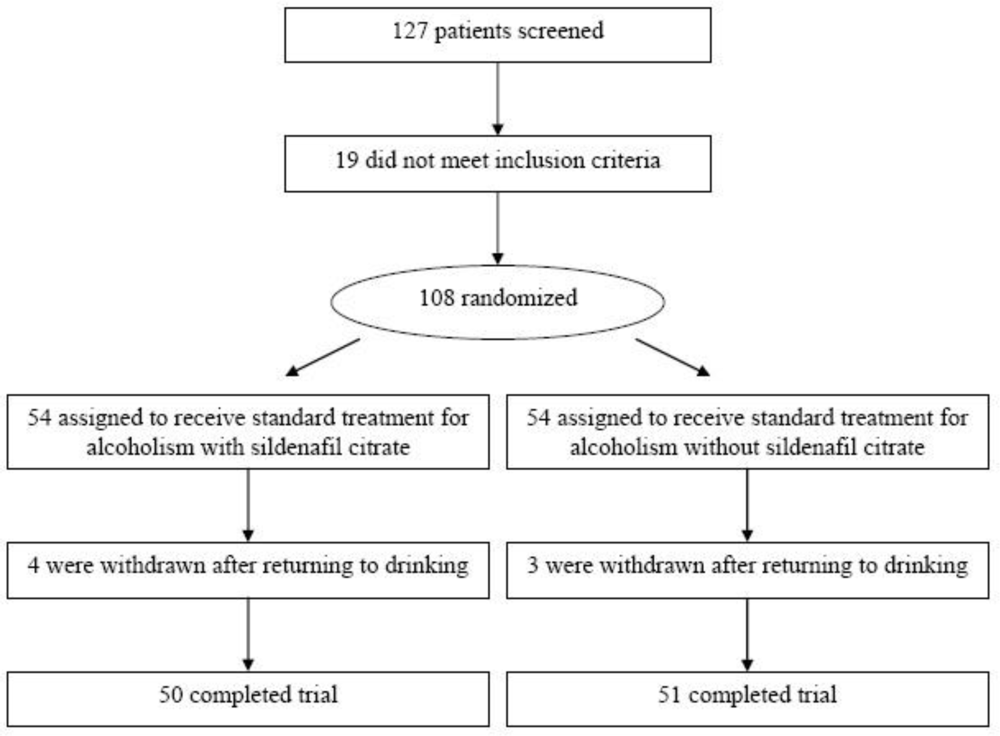
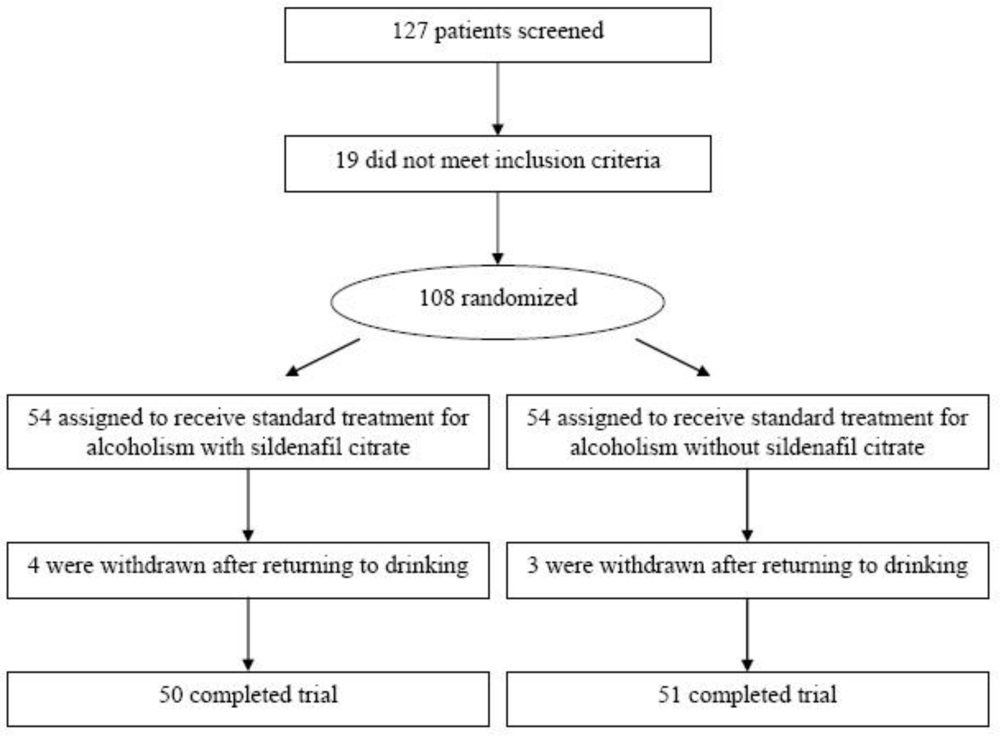
2.1. Study Design
2.2. Patients
2.3. Study Protocol
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
Efficacy
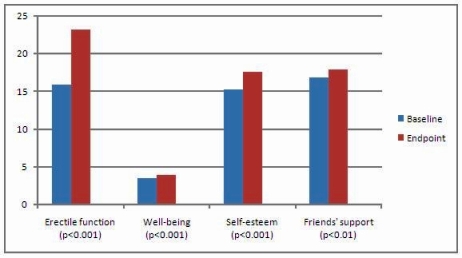
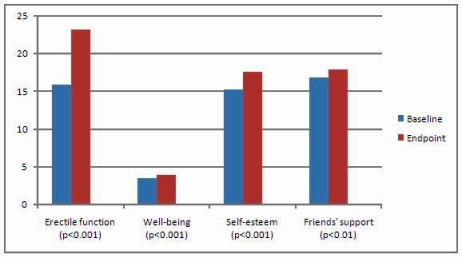
3.1. Sexual Function
3.2. Depression
3.4. Self-Esteem
3.5. Social Support
3.6. Adverse Effects
4. Discussion
Abbreviations:
| ED | erectile dysfunction; |
| AD | alcohol dependence; |
| IIEF | International Index of Erectile Function; |
| PTSD | Post Traumatic Stress Disorder; |
| AASD | Alcohol-associated sexual dysfunction; |
| GLF | Global Life Functioning inventory; |
| BDI | Beck Depression Inventory; |
| RGSES | Rosenberg’s General Self-Esteem Scale: |
| MSPSS | Multidimensional Scale of Perceived Social Support; |
| SD | standard deviations; |
| ES | effect size. |
Acknowledgments
- Disclosure of off-label usage: The authors have determined that, to the best of their knowledge, no investigational information about pharmaceutical agents has been presented in this article that is outside U.S. Food and Drug Administration-approved labeling.
References
- Wetterling, T; Veltrup, C; Driessen, M; John, U. Drinking pattern and alcohol-related medical disorders. Alcohol Alcoholism 1999, 34, 330–336. [Google Scholar]
- O’Farrell, TJ; Kleinke, CL; Cutter, HS. Sexual adjustment of male alcoholics: changes from before to after receiving alcoholism counseling with and without marital therapy. Addict. Behav 1998, 23, 419–425. [Google Scholar]
- van Steenbergen, W. Alcohol, liver cirrhosis and disorders in sex hormone metabolism. Acta Clin. Belg 1993, 48, 269–283. [Google Scholar]
- Fahrner, EM. Sexual dysfunction in male alcohol addicts: prevalence and treatment. Arch. Sex Behav 1987, 16, 247–257. [Google Scholar]
- Jeffcoate, WJ. The investigation of impotence. Br. J. Urol 1991, 68, 449–453. [Google Scholar]
- McCambridge, J; Mitcheson, L; Hunt, N; Winstock, A. The rise of Viagra among British illicit drug users: 5-year survey data. Drug Alcohol Rev 2006, 25, 111–113. [Google Scholar]
- Caspari, D; Huebgen, EM; Derouet, H. Interdisciplinary assessment and follow-up of patients with erectile dysfunction—psychiatric aspects. Int. J. Impot. Res 1999, 11, 213–217. [Google Scholar]
- Cheitlin, MD; Hutter, AM, Jr; Brindis, RG; Ganz, P; Kaul, S; Russell, RO, Jr; Zusman, RM. Use of sildenafil (Viagra) in patients with cardiovascular disease. Circulation 1999, 99, 168–177. [Google Scholar]
- Benchekroun, A; Faik, M; Benjelloun, S; Bennani, S; El Mrini, M; Smires, A. A baseline-controlled, open-label, flexible dose-escalation study to assess the safety and efficacy of sildenafil citrate (Viagra) in patients with erectile dysfunction. Int. J. Impot. Res 2003, 15, S19–24. [Google Scholar]
- Rendell, MS; Rajfer, J; Wicker, PA; Smith, MD. Sildenafil for treatment of erectile dysfunction in men with diabetes. JAMA 1999, 281, 421–426. [Google Scholar]
- Basu, A; Ryder, RE. New treatment options for erectile dysfunction in patients with diabetes mellitus. Drugs 2004, 64, 2667–2688. [Google Scholar]
- Benet, AE; Melman, A. The epidemiology of erectile dysfunction. Urol. Clin. North Am 1995, 22, 699–709. [Google Scholar]
- Feldman, R; Meuleman, EJ; Steers, W. Sildenafil citrate (VIAGRA) in the reatment of erectile dysfunction: analysis of two flexible dose-escalation studies. Sildenafil Study Group. Int. J. Clin. Pract 1999, 102, 10–12. [Google Scholar]
- Ditunno, JF, Jr; Young, W; Donovan, WH; Creasey, G. The international standards booklet for neurological and functional classification of spinal cord injury. Am. Spin. Inj. Ass. Parapleg 1994, 32, 70–80. [Google Scholar]
- Giuliano, F; Hultling, C; El Masry, WS; Smith, MD; Osterloh, IH; Orr, M; Maytom, M. Randomized trial of sildenafil for the treatment of erectile dysfunction in spinal cord injury. Sildenafil Study Group. Ann. Neurol 1999, 46, 15–21. [Google Scholar]
- Hultling, C; Giuliano, F; Quirk, F; Pena, B; Mishra, A; Smith, MD. Quality of life in patients with spinal cord injury receiving Viagra (sildenafil citrate) for the treatment of erectile dysfunction. Spinal Cord 2000, 38, 363–370. [Google Scholar]
- Deforge, D; Blackmer, J; Garritty, C; Yazdi, F; Cronin, V; Barrowman, N; Fang, M; Mamaladze, V; Zhang, L; Sampson, M; Moher, D. Male erectile dysfunction following spinal cord injury: a systematic review. Spinal Cord 2006, 44, 465–473. [Google Scholar]
- Fowler, CJ; Miller, JR; Sharief, MK; Hussain, IF; Stecher, VJ; Sweeney, M. A double blind, randomised study of sildenafil citrate for erectile dysfunction in men with multiple sclerosis. J. Neurol. Neurosurg. Psychiat 2005, 76, 700–705. [Google Scholar]
- Steers, W; Guay, AT; Leriche, A; Gingell, C; Hargreave, TB; Wright, PJ; Price, DE; Feldman, RA. Assessment of the efficacy and safety of Viagra (sildenafil citrate) in men with erectile dysfunction during long-term treatment. Int. J. Impot. Res 2001, 13, 261–267. [Google Scholar]
- Nurnberg, HG; Gelenberg, A; Hargreave, TB; Harrison, WM; Siegel, RL; Smith, MD. Efficacy of sildenafil citrate for the treatment of erectile dysfunction in men taking serotonin reuptake inhibitors. Am. J. Psychiat 2001, 158, 1926–1928. [Google Scholar]
- Seidman, SN; Roose, SP; Menza, MA; Shabsigh, R; Rosen, RC. Treatment of erectile dycfunction in men with depressive symptoms: results of a placebo-controlled trial with sildenafil citrate. Am. J. Psychiat 2001, 158, 1623–1630. [Google Scholar]
- Tignol, J; Furlan, PM; Gomez-Beneyto, M; Opsomer, R; Schreiber, W; Sweeney, M; Wohlhuter, C. Efficacy of sildenafil citrate (Viagra) for the treatment of erectile dysfunction in men in remission from depression. Int. Clin. Psychopharmacol 2004, 19, 191–199. [Google Scholar]
- Rosen, RC; Seidman, SN; Menza, MA; Shabsigh, R; Roose, SP; Tseng, LJ; Orazem, J; Siegel, RL. Quality of life, mood, and sexual function: a path analytic model of treatment effects in men with erectile dysfunction and depressive symptoms. Int. J. Impot. Res 2004, 16, 334–340. [Google Scholar]
- Fava, M; Nurnberg, HG; Seidman, SN; Holloway, W; Nicholas, S; Tseng, LJ; Stecher, VJ. Efficacy and safety of sildenafil in men with serotonergic antidepressant-associated erectile dysfunction: results from a randomized, double-blind, placebo-controlled trial. J. Clin. Psychiat 2006, 67, 240–246. [Google Scholar]
- Orr, G; Weiser, M; Polliack, M; Raviv, G; Tadmor, D; Grunhaus, L. Effectiveness of sildenafil in treating erectile dysfunction in PTSD patients: a double-blind, placebo-controlled crossover study. J. Clin. Psychopharmacol 2006, 26, 426–430. [Google Scholar]
- Aviv, A; Shelef, A; Weizman, A. An open-label trial of sildenafil addition in risperidone-treated male schizophrenia patients with erectile dysfunction. J. Clin. Psychiat 2004, 65, 97–103. [Google Scholar]
- Gopalakrishnan, R; Jacob, KS; Kuruvilla, A; Vasantharaj, B; John, JK. Sildenafil in the treatment of antipsychotic-induced erectile dysfunction: a randomized, double-blind, placebo-controlled, flexible-dose, two-way crossover trial. Am. J. Psychiat 2006, 163, 494–499. [Google Scholar]
- Nandipati, KC; Raina, R; Agarwal, A; Zippe, CD. Erectile dysfunction following radical retropubic prostatectomy: epidemiology, pathophysiology and pharmacological management. Drugs Aging 2006, 23, 101–117. [Google Scholar]
- Sharma, RK; Prasad, N; Gupta, A; Kapoor, R. Treatment of erectile dysfunction with sildenafil citrate in renal allograft recipients: a randomized, double-blind, placebo-controlled, crossover trial. Am. J. Kidney Dis 2006, 48, 128–133. [Google Scholar]
- Dachille, G; Pagliarulo, V; Ludovico, GM; Ralph, D; Pagliarulo, A. Sexual dysfunction in patients under dialytic treatment. Minerva Urol. Nefrol 2006, 58, 195–200. [Google Scholar]
- Wagner, G; Montorsi, F; Auerbach, S; Collins, M. Sildenafil citrate (VIAGRA) improves erectile function in elderly patients with erectile dysfunction: a subgroup analysis. J. Gerontol. A Biol. Sci. Med. Sci 2001, 56, M113–119. [Google Scholar]
- Carson, CC. Erectile dysfunction: evaluation and new treatment options. Psychosom. Med 2004, 66, 664–671. [Google Scholar]
- Morales, A; Gingell, C; Collins, M; Wicker, PA; Osterloh, IH. Clinical safety of oral sildenafil citrate (VIAGRA) in the treatment of erectile dysfunction. Int. J. Impot. Res 1998, 10, 69–73. [Google Scholar]
- Kiroglu, AF; Bayrakli, H; Yuca, K; Cankaya, H; Kiris, M. Nasal obstruction as a common side-effect of sildenafil citrate. Tohoku J. Exp. Med 2006, 208, 251–254. [Google Scholar]
- Laties, A; Sharlip, I. Ocular safety in patients using sildenafil citrate therapy for erectile dysfunction. J. Sex Med 2006, 3, 12–27. [Google Scholar]
- de L Figuerola, M; Bruera, O; Leston, J; Ferreiro, J. Cluster headache attack due to sildenafil intake. Cephalalgia 2006, 26, 617–619. [Google Scholar]
- Grinshpoon, A; Margolis, A; Weizman, A; Ponizovsky, AM. Sildenafil citrate in the treatment of sexual dysfunction and its effect on quality of life in alcohol dependent men: preliminary findings. Alcohol Alcoholism 2007, 42, 340–346. [Google Scholar]
- The ICD-10 Classification of Mental and Behavioural Disorders. Diagnostic Criteria for Research; WHO: Geneva, Switzerland, 1993.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th Edition ed; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Rosen, RC; Riley, A; Wagner, G; Osterloh, IH; Kirkpatrick, J; Mishra, A. The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology 1997, 49, 822–830. [Google Scholar]
- Rosenberger, WF; Lachin, JM. Randomization in Clinical Trials: Theory and Practice; Wiley: New York, NY, USA, 2002. [Google Scholar]
- Elkin, I; Parloff, MB; Hadley, SW; Autry, JH. NIMH Treatment of depression Collaborative Research Program. Background and research plan. Arch. Gen. Psychiat 1985, 42, 305–316. [Google Scholar]
- Beck, AT; Beamesderfer, A. Assessment of depression: the depression inventory. Psychological measurements in psychopharmacology. Modern Probl. Pharmacopsychiat 1974, 7, 151–169. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Zimet, GD; Dahlem, NW; Zimet, SG; Farley, GK. The Multidimensional Scale of Perceived Social Support. J. Pers. Assess 1988, 52, 30–41. [Google Scholar]
- Pedersen, RD; Pallay, AG; Rudolph, RL. Can improvement in well-being and functioning be distinguished from depression improvement in antidepressant clinical trials? Qual. Life Res 2002, 11, 9–17. [Google Scholar]
- Dupuy, HJ. The Psychological General Well-Being (PGWB) Index. In Assessment of Quality of Life in Clinical Trials of Cardiovascular Therapies; Wender, NK, Mattson, ME, Furberg, CD, Elinson, J, Eds.; Le Jacq: New York, NY, USA, 1984; pp. 170–183. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1988. [Google Scholar]
- Middel, B; Stewart, R; Bouma, J; van Sonderen, E; van den Heuvel, WJ. How to validate clinically important change in health-related functional status. Is the magnitude of the effect size consistently related to magnitude of change as indicated by a global question rating? J. Eval. Clin. Pract 2001, 7, 399–410. [Google Scholar]
- Norman, GR; Sloan, JA; Wyrwich, KW. Interpretation of changes in health-related quality of life: the remarkable universality of half a standard deviation. Med. Care 2003, 41, 582–592. [Google Scholar]
- Freitas, D; Athanazio, R; Almeida, D; Dantas, N; Reis, F. Sildenafil improves quality of life in men with heart failure and erectile dysfunction. Int. J. Impot. Res 2006, 18, 210–212. [Google Scholar]
- O’Leary, MP; Althof, SE; Cappelleri, JC; Crowley, A; Sherman, N; Duttagupta, S. The United States Self-Esteem and Relationship Questionnaire Study Group. Self-esteem, confidence and relationship satisfaction of men with erectile dysfunction treated with sildenafil citrate: a multicenter, randomized, parallel group, double-blind, placebo controlled study in the United States. J. Urol 2006, 175, 1058–1062. [Google Scholar]
- Althof, SE; O’Leary, MP; Cappelleri, JC; Glina, S; King, R; Tseng, LJ; Bowler, JL. US and International SEAR study group. Self-esteem, confidence, and relationships in men treated with sildenafil citrate for erectile dysfunction: results of two double-blind, placebo-controlled trials. J. Gen. Intern. Med 2006, 21, 1069–1074. [Google Scholar]
- Tomlinson, J; Wright, D. Impact of erectile dysfunction and its subsequent treatment with sildenafil: qualitative study. Brit. Med. J 2004, 328, 1037–1040. [Google Scholar]
- Ponizovsky, AM. Clinical and psychosocial factors associated with quality of life in alcohol-dependent men with erectile dysfunction. J. Sex Med 2008, 5, 2347–2358. [Google Scholar]
- Montorsi, F; Padma-Nathan, H; Glina, S. Erectile function and assessments of erection hardness correlate positively with measures of emotional well-being, sexual satisfaction, and treatment satisfaction in men with erectile dysfunction treated with sildenafil citrate (Viagra). Urology 2006, 68, 26–37. [Google Scholar]
- Steidle, CP; Stecher, VJ; Pace, C; Tseng, LJ; The SEAR Study Group. Correlation of improved erectile function and rate of successful intercourse with improved emotional well-being assessed with the Self-Esteem and Relationship questionnaire in men treated with sildenafil for erectile dysfunction and stratified by age. Curr. Med. Res. Opin 2006, 22, 939–948. [Google Scholar]
- Cappelleri, JC; Bell, SS; Althof, SE; Siegel, RL; Stecher, VJ. Comparison between sildenafil-treated subjects with erectile dysfunction and control subjects on the Self-Esteem and Relationship questionnaire. J. Sex Med 2006, 3, 274–282. [Google Scholar]
- Rosen, R; Janssen, E; Wiegel, M; Bancroft, J; Althof, S; Wincze, J; Segraves, RT; Barlow, D. Psychological and interpersonal correlates in men with erectile dysfunction and their partners: a pilot study of treatment outcome with sildenafil. J. Sex Marital. Ther 2006, 32, 215–234. [Google Scholar]
- Rubin, N; Wylie, K. Should sildenafil be available over the counter? Br. Med. Bull 2009, 90, 1–10. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Variable | Sildenafil group (n = 50) | Control group (n = 51) | |
|---|---|---|---|
| Age (yr.) | 44.0 (8.7) | 43.5 (5.9) | t = 0.37, df = 99, P = 0.71 |
| Marital status Single Married Divorced/separated/Widowed | 6 (12) 31 (62) 13 (26) | 2 (3.9) 41 (80.4) 8 (15.7) | χ2 = 4.57, df = 2, P = 0.12 |
| Education (yr.) | 11.1 (4.5) | 10.2 (3.5) | t = 1.08, df = 99, P = 0.33 |
| Employment status Employed Unemployed | 16 (32.0) 34 (68.0) | 16 (31.4) 35 (68.6) | χ2 = 0.005, df = 1, P = 1.0 |
| Religious affiliation Jewish Non-Jewish | 31 (62.0) 19 (38.0) | 34 (66.7) 17 (33.3) | χ2 = 0.24, df = 1, P = 0.70 |
| Immigration status Non-immigrant Immigrant | 23 (46.0) 27 (54.0) | 38 (74.5) 13 (25.5) | χ2 = 8.58, df = 1, P = 0.004 |
| Length of immigration (yr.) | 16.4 (13.3) | 18.1 (15.4) | t = 0.42, df = 51, P = 0.68 |
| Age at first alcohol consumption (yr.) | 17.2 (3.4) | 21.3 (7.0) | t = 3.75, df = 99, P < 0.001 |
| Age at first binge (yr.) | 20.5 (6.4) | 26.1 (8.6) | t = 3.68, df = 99, P < 0.001 |
| Duration of harmful alcohol consumption (yr.) | 14.8 (9.7) | 13.0 (10.4) | t = 0.91, df = 99, P = 0.36 |
| No. of prior inpatient detoxification(s) 0 1 2+ | 30 (60.0) 13 (26.0) 7 (14.0) | 28 (54.9) 14 (27.5) 9 (17.6) | χ2 = 0.35, df = 2, P = 0.81 |
| Average alcohol intake in last 6 months (g alcohol/drinking day) | 700 (648.8) | 694 (453.8) | t = 0.048, df = 99, P = 0.96 |
| No. of drinking days in last month | 8.6 (10.8) | 6.8 (10.3) | t = 0.85, df = 99, P = 0.43 |
| Sexual function domain | Sildenafil group (n = 50) | Control group (n = 51) | Effect size | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Endpoint | t-value | P-value | Baseline | Endpoint | t-value | P-value | ||
| Total score | 39.9(16.9) | 56.7 (12.9) | 7.23 | <0.001 | 53.7 (10.8) | 50.9(12.3) | 1.90 | 0.64 | 1.25 |
| Erectile function | 15.9 (7.6) | 23.2 (5.6) | 6.79 | <0.001 | 21.8 (5.3) | 20.8 (5.7) | 1.46 | 0.15 | 1.17 |
| Orgasmic function | 6.1 (3.1) | 8.2 (2.1) | 5.64 | <0.001 | 8.0 (1.8) | 7.4 (2.2) | 2.27 | 0.03 | 1.01 |
| Sexual desire | 6.0 (2.2) | 7.3 (1.4) | 5.11 | <0.001 | 7.1 (1.5) | 6.6 (1.4) | 2.34 | 0.02 | 0.91 |
| Intercourse satisfaction | 7.1 (3.7) | 10.3 (2.8) | 5.51 | <0.001 | 9.5 (2.4) | 9.0 (2.5) | 1.38 | 0.17 | 1.11 |
| Overall satisfaction | 4.7 (2.5) | 7.6 (2.3) | 8.35 | <0.001 | 7.3 (1.9) | 7.0 (2.0) | 1.16 | 0.25 | 1.23 |
| Outcome measure | Sildenafil group (n = 50) | Control group (n = 51) | Effect size | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Changes from baseline to endpoint | t-value | P-value | Baseline | Changes from baseline to endpoint | t-value | P-value | ||
| General Life Functioning | 3.5 (0.7) | −0.5 (0.6) | 5.04 | <0.001 | 3.5 (0.6) | −0.09(0.5) | 1.41 | 0.17 | 0.63 |
| Well-being | 3.4 (0.7) | −0.4 (0.7) | 4.72 | <0.001 | 3.6 (0.7) | −0.009 (0.5) | 1.25 | 0.22 | 0.44 |
| Functioning | 3.5 (0.7) | −0.5 (0.7) | 4.57 | <0.001 | 3.5 (0.7) | −0.1 (0.6) | 1.18 | 0.24 | 0.57 |
| Beck Depression Inventory | 10.5 (6.2) | 4.9 (5.0) | 6.93 | <0.001 | 9.6 (6.1) | 2.0 (4.8) | 2.98 | 0.01 | 0.47 |
| General Self-Esteem Scale | 15.2 (3.7) | −2.4 (3.9) | 4.27 | <0.001 | 15.5(3.6) | −0.2 (3.4) | 0.46 | 0.65 | 0.61 |
| MSPSS, total score | 54.4 (8.9) | −3.2 (8.9) | 2.52 | 0.02 | 51.7(14.2) | 0.5 (9.3) | 0.38 | 0.71 | 0.31 |
| Family | 17.8 (4.7) | −1.0 (4.4) | 1.59 | 0.12 | 17.4 (6.0) | −0.2 (3.8) | 0.30 | 0.77 | 0.15 |
| Friends | 16.8 (4.7) | −1.1 (3.0) | 2.68 | 0.01 | 15.9 (5.9) | 0.2 (3.4) | 0.41 | 0.68 | 0.24 |
| Significant others | 19.8 (3.5) | −1.1 (3.8) | 1.96 | 0.055 | 18.5 (4.6) | 0.5 (3.5) | 0.91 | 0.37 | 0.39 |
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Ponizovsky, A.M.; Averbuch, L.; Radomislensky, I.; Grinshpoon, A. A Multicenter, Randomized, Open-Labeled, Parallel Group Trial of Sildenafil in Alcohol-Associated Erectile Dysfunction: The Impact on Psychosocial Outcomes. Int. J. Environ. Res. Public Health 2009, 6, 2510-2525. https://doi.org/10.3390/ijerph6092510
Ponizovsky AM, Averbuch L, Radomislensky I, Grinshpoon A. A Multicenter, Randomized, Open-Labeled, Parallel Group Trial of Sildenafil in Alcohol-Associated Erectile Dysfunction: The Impact on Psychosocial Outcomes. International Journal of Environmental Research and Public Health. 2009; 6(9):2510-2525. https://doi.org/10.3390/ijerph6092510
Chicago/Turabian StylePonizovsky, Alexander M., Lev Averbuch, Ira Radomislensky, and Alexander Grinshpoon. 2009. "A Multicenter, Randomized, Open-Labeled, Parallel Group Trial of Sildenafil in Alcohol-Associated Erectile Dysfunction: The Impact on Psychosocial Outcomes" International Journal of Environmental Research and Public Health 6, no. 9: 2510-2525. https://doi.org/10.3390/ijerph6092510
APA StylePonizovsky, A. M., Averbuch, L., Radomislensky, I., & Grinshpoon, A. (2009). A Multicenter, Randomized, Open-Labeled, Parallel Group Trial of Sildenafil in Alcohol-Associated Erectile Dysfunction: The Impact on Psychosocial Outcomes. International Journal of Environmental Research and Public Health, 6(9), 2510-2525. https://doi.org/10.3390/ijerph6092510