Pathogenic Microorganisms Associated With Childhood Diarrhea in Low-and-Middle Income Countries: Case Study of Yaoundé – Cameroon

Abstract
:1. Introduction
2. Material and Methods
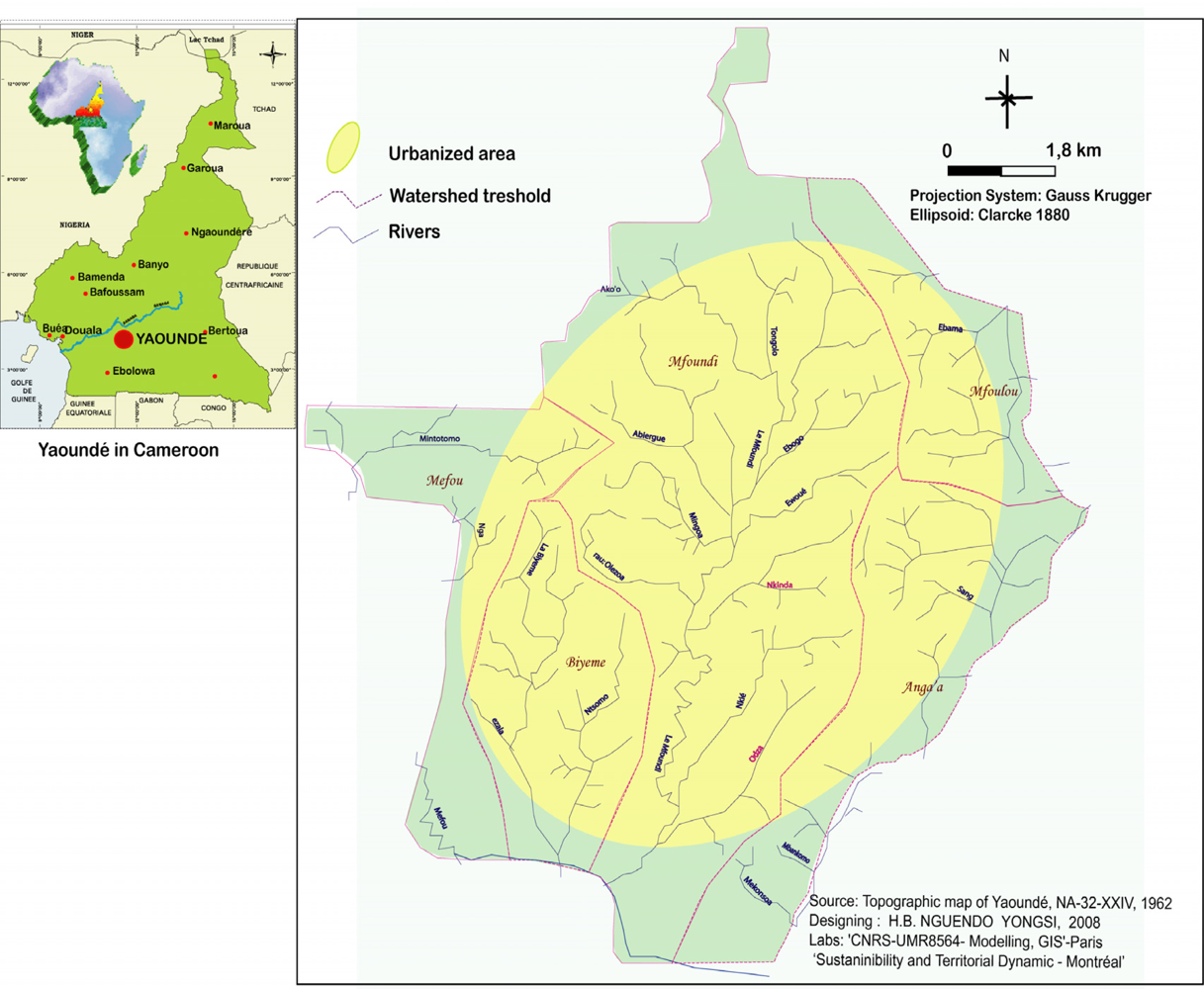
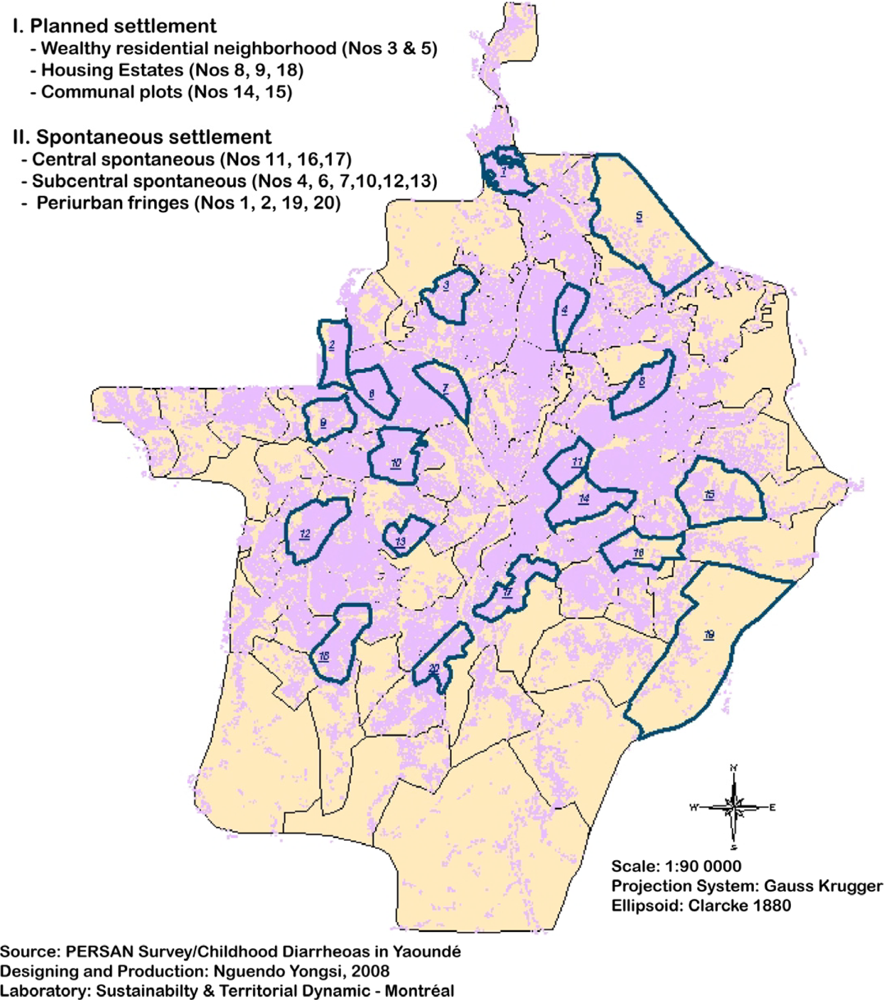
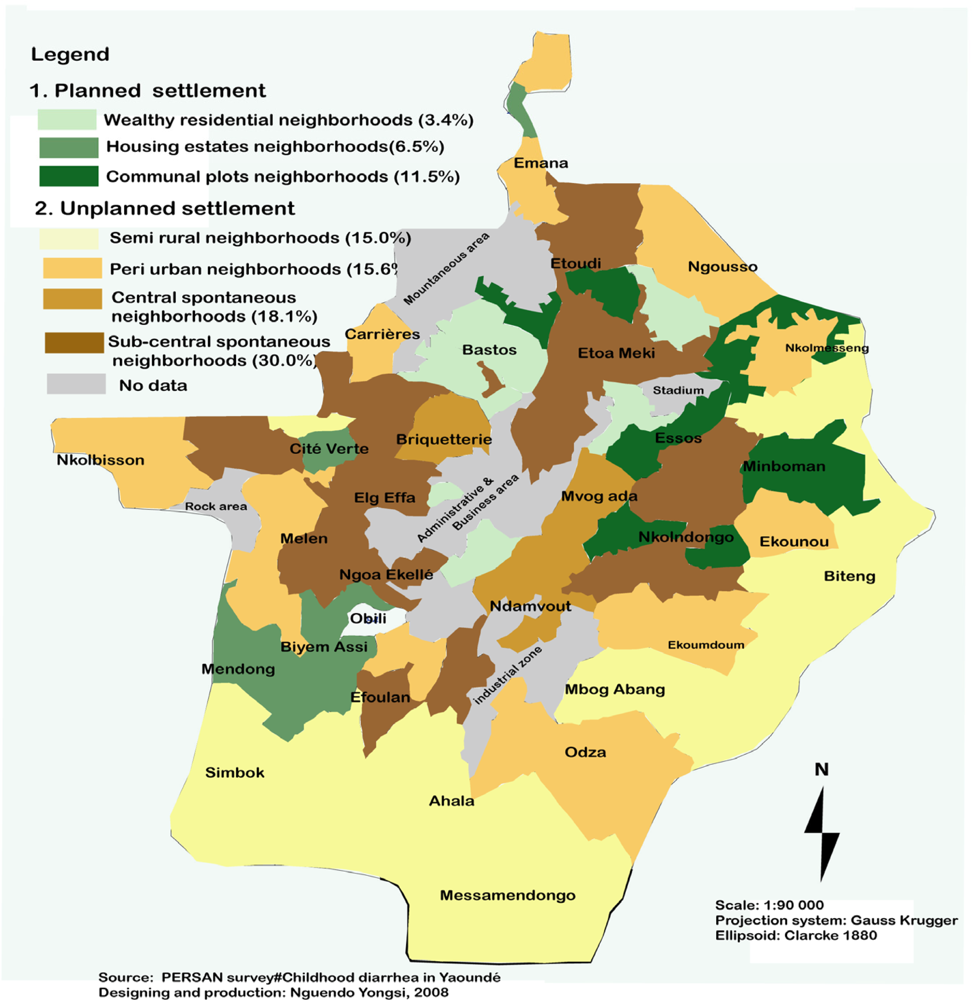
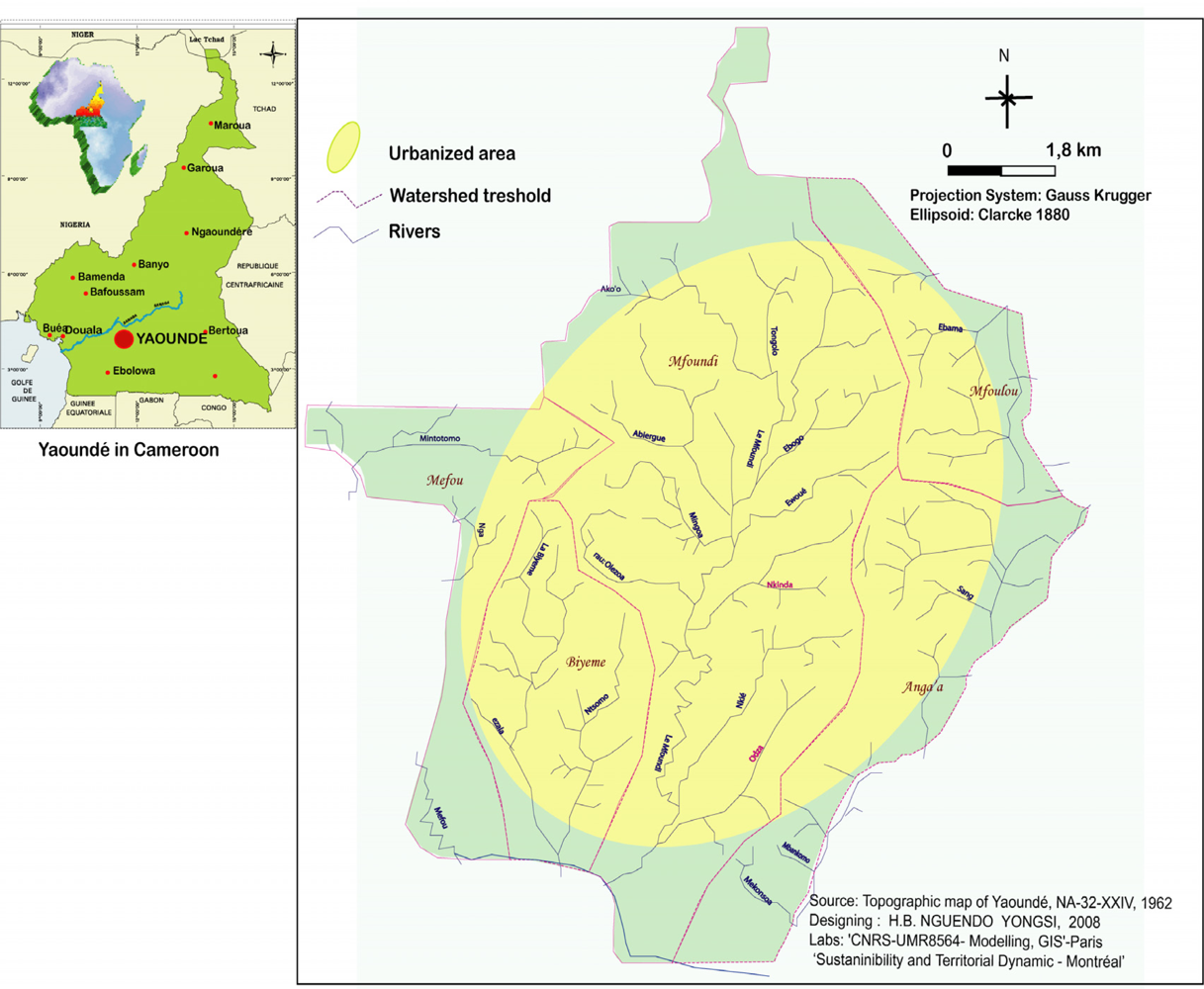
2.1. Location of study
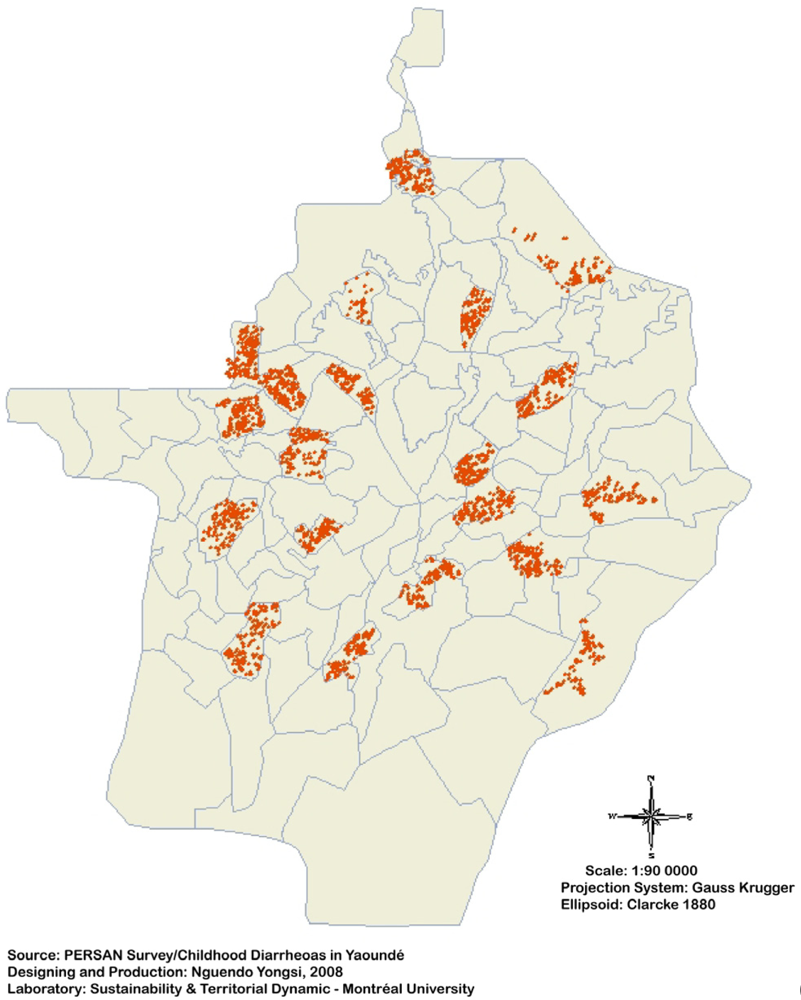
2.2. Data collection
3. Results
4. Discussion
5. Conclusion




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Surveyed individuals | Cases of diarrheas |
|---|---|---|
| Male | 1,564 (51.6%) | 358 (81.9%) |
| Female | 1,470 (48.4%) | 79 (18.1%) |
| Variable coverage | 3,034 (100.0%) | 437 (100.0%) |
| Diarrheal disease? | ||
|---|---|---|
| Strata | Yes | No |
| 06 - 11 months | 72 | 351 |
| 12 - 23 months | 178 | 628 |
| 24 - 35 months | 120 | 709 |
| 36 - 47 months | 43 | 530 |
| 48 - 59 months | 24 | 379 |
| Total | 437 | 2,597 |
| Causative agents | Genus | Frequency | Percentage |
|---|---|---|---|
| Viruses | Rotavirus | 3 | 01.1 |
| Enteric Adenovirus | 7 | 02.7 | |
| Bacteria | Salmonella spp. | 29 | 11.2 |
| Shigella spp. | 23 | 08.8 | |
| Escherichia coli | 19 | 07.3 | |
| Campylobacter jejuni | 25 | 09.6 | |
| Parasites | Ascaris lumbricoides | 46 | 17.8 |
| Trichuris trichiura | 28 | 10.7 | |
| Entamaeba | 22 | 08.4 | |
| Giardia intestinalis | 34 | 13,2 | |
| Trichomonas | 8 | 03.2 | |
| Shistosoma | 5 | 01.9 | |
| Chilomastix | 4 | 01.5 | |
| Cryptosporidium | 7 | 02.6 | |
| Total | 260 | 100.0 | |
| Microorganisms | Prevalence | 06– 11 months | 12–35 months | 36–59 months | P value | ||||
|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | ||
| Rotavirus | 3 | 01.1 | 1 | 33.3 | 2 | 67.6 | 0 | 00.0 | NS |
| Enteric adenovirus | 7 | 02.6 | 4 | 57.1 | 3 | 42.8 | 0 | 00.0 | <0.008 |
| Salmonella spp. | 25 | 09.6 | 6 | 24.0 | 14 | 56.0 | 5 | 20.0 | <0.005 |
| Shigella spp. | 19 | 07.3 | 4 | 21.0 | 9 | 47.3 | 6 | 31.5 | <0.004 |
| Campylobacter spp. | 23 | 08.8 | 3 | 13.0 | 12 | 52.1 | 8 | 34.7 | <0.003 |
| E. coli-EAEC | 8 | 03.1 | 5 | 62.5 | 3 | 37.5 | 0 | 00.0 | NS |
| E. coli-ETEC | 6 | 02.3 | 3 | 50.0 | 2 | 33.3 | 1 | 16.6 | NS |
| E. coli –EPEC | 11 | 04.2 | 2 | 18.1 | 8 | 72.7 | 1 | 09.0 | <0.001 |
| E.coli-VTEC | 4 | 01.5 | 0 | 00.0 | 2 | 50.0 | 2 | 50.0 | NS |
| Ascaris lumbricoides | 46 | 17.8 | 3 | 06.5 | 15 | 32.6 | 28 | 60.8 | <0.001 |
| Trichuris trichiura | 28 | 10.7 | 0 | 00.0 | 19 | 67.8 | 9 | 32.1 | <0.003 |
| Entamoeba histolytica | 22 | 08.4 | 3 | 13.6 | 9 | 40.9 | 5 | 22.7 | NS |
| Giradia lamblia | 34 | 13.1 | 11 | 32.3 | 14 | 41.1 | 9 | 26.4 | <0.002 |
| Trichomnas intestinalis | 8 | 03.1 | 0 | 00.0 | 3 | 37.5 | 5 | 62.5 | NS |
| Shistosoma | 1 | 00.3 | 0 | 00.0 | 0 | 00.0 | 1 | 100 | NS |
| Shistosoma mansoni | 4 | 01.5 | 0 | 00.0 | 4 | 100 | 0 | 00.0 | NS |
| Chilomastix mesnili | 4 | 01.5 | 0 | 00.0 | 3 | 75.0 | 1 | 25.0 | NS |
| Cryptosporidium | 7 | 02.6 | 2 | 28.5 | 4 | 57.1 | 1 | 14.2 | <0.008 |
Acknowledgments
References
- Fernel, J. La pathologie ou discours des maladies; Faculté de Médecine de Paris: Paris, France, 1655. [Google Scholar]
- Colson, J-Cl. Essai sur la diarrhée; Faculté de Médecine de Paris: Paris, France, 1808. [Google Scholar]
- Vignes, P. Traité complet de la dysenterie et de la diarrhée; Rousselon: Paris, France, 1825. [Google Scholar]
- Dufour, A. Dissertation sur la diarrhée idiopathique; Faculté de Médecine de Paris: Paris, France, 1814. [Google Scholar]
- Galien (129-201), Oeuvres anatomiques, physiologiques et médicales; Tome 1; Charles Daremberg: Paris, France, 1854.
- Tralles, A. (de) [525-605]; De arte medicalibri XII; Éditions Johannes Günther Andernach: Bâle, Switzerland, 1566. [Google Scholar]
- Celse, J. [30 ap.J.C.]; Traité de Médecine; Delahays: Paris, France, 1855. [Google Scholar]
- Grall, C; Leger, M; Mathis, C. Traité de pathologie exotique: Diarrhées, dysenterie, hépatite endémique, abcès du foie; J.-B. Baillère et fils: Paris, France, 1920. [Google Scholar]
- Nguendo Yongsi, HB; Delali Dovie, BK. Diarrheal diseases in the history of public health. Arch. Med. Res 2007, 38, 159–163. [Google Scholar]
- Nielly, M. Eléments de pathologie exotique; Delahaye et Lecronier: Paris, France, 1881. [Google Scholar]
- World Health Organization, Manual for the laboratory investigations of acute enteric infections; WHO: Geneva, Switzerland, 1983.
- Farthing, MJ. Diarrhoea: a significant worldwide problem. Int. J. Antimicrob. Agents 2000, 14, 65–69. [Google Scholar]
- WHO. Available at https://www.who.int/water_sanitation_health/publications/facts2004/en/index.html [Accessed: 23 October 2008].
- Schiller, LR. Management of diarrhea in clinical practice: strategies for primary care physicians. Rev. Gastroenterol. Disord 2007, 7, 27–38. [Google Scholar]
- Hamer, DH; Simon, F; Thea, D; Keutsh, GT. Childhood diarrhea in Sub-Saharan Africa. Child. Health Res. Project 1998, 2, 1–32. [Google Scholar]
- Huilan, S; Zhen, LG; Mathan, MM; Mathew, MM; Olarte, J; Espejo, R; Khin, MU; Ghafoor, MA; Khan, MA; Sami, Z; Sutton, RG. Etiology of acute diarrhea among children in developing countries; A multicenter study in five countries. Bull. World Health Organ 1991, 69, 549–555. [Google Scholar]
- Okeke, IN; Ojo, O; Lamikanra, A; Kaper, JB. Etiology of acute diarrhea in adults southeastern Nigeria. J. Clin. Microbiol 2003, 41, 4525–4530. [Google Scholar]
- Hanlon, P; Hanlon, L; Marsh, V; Byass, P; Shenton, F; Sanders, RC; Hassan-King, M; Greenwood, BM. Epidemiology of rotavirus in a periurban Gambian community. Ann. Trop. Paediatr 1987, 7, 238–243. [Google Scholar]
- National Institute of Statistics. CAVIE: Enquête sur le cadre de vie des populations de Yaoundé et Douala. Available at http://www.statistics-cameroon.org [Accessed 27 August 2008].
- Nguendo Yongsi, HB. Prevalence and spatial disparities of infectious diseases with regard to the physical environment in Yaoundé - Cameroon. J. Health Dev 2007, 3, 123–145. [Google Scholar]
- Vargas, M; Gascon, J; Casals, C; Shellenberg, D; Urassa, H; Kahigwa, E; Ruiz, J; Vila, J. Etiology of diarrhea in children less than five years of age in Ifakara, Tanzania. Am. J. Trop. Med. Hyg 2004, 70, 536–539. [Google Scholar]
- Amador, JJ; Vicari, A; Turcios-Ruiz, RM; Melendez, DAC; Malek, M; Michel, F; Aldighieri, S; Kerin, T; Bresee, JS; Glass, RI; Andrus, JK. Outbreak of rotavirus gastroenteritis with high mortality, Nicaragua. Rev. Panam. Salud Publica 2008, 23, 277–284. [Google Scholar]
- Carraturo, A; Catalani, V; Tega, L. Microbiological and epidemiological aspects of rotavirus and enteric adenovirus infections in hospitalized children in Italy. New Microbiol 2008, 31, 329–336. [Google Scholar]
- Kevin, KC; Barteluk, RL; Kelly, M T; He, X; de Hua, G; Ge, YA; Proctor, EM; Byrne, S; Stiver, HG. Etiology of childhood diarrhea in Beijing, China. J. Clin. Microbiol 1991, 29, 90–95. [Google Scholar]
- Vargas, M; Gascon, J; Gallardo, F; Jimenez De Anta, MT; Vila, J. Prevalence of diarrheagenic Escherichia coli strains detected by PCR in patients with traveler diarrhea. Clin. Microbiol. Infect 1998, 4, 682–688. [Google Scholar]
- Moyo, SJ; Gro, N; Kirsti, V; Matee, MI; Kitundu, J; Maselle, SY; Langeland, N; Myrmel, H. Prevalence of enteropathogenic viruses and molecular characterization of group A rotavirus among children with diarrhea in Dar es Salaam Tanzania. BMC Public Health 2007, 27, 359–368. [Google Scholar]
- Mandomando, IM; Macette, EV; Ruiz, J; Sanz, S; Abacassamo, F; Valles, X; Sacarlal, J; Navia, MM; Vila, J; Alonso, PL; Gascon, J. Etiology of diarrhea in children younger than 5 years of age admitted in a rural hospital of southern Mozambique. Am.J. Trop. Med. Hyg 2007, 76, 522–527. [Google Scholar]
- Meridian Bioscience Inc, A Rapid immunoassay for the detection of rotavirus antigen in human stool; Catalog No. 750030 - Meridian Bioscience Inc.: Cincinnati, OH, 1988; p. 14.
- Dennehy, PH; Gauntlett, DR; Spangenberger, SE. Choice of reference assay for the detection of rotavirus in fecal specimens: Electron Microscopy versus Enzyme Immunoassay. J. Clin. Microbiol 1990, 28, 1280–1283. [Google Scholar]
- Zlateva, KT; Maes, P; Rahman, M; Van Ranst, M. Chromatography paper strip sampling for enteric adenoviruses type 40 and 41 positive stool specimens. J. Virol 2005, 2, 1–5. [Google Scholar]
- Guerrant, RL; Bobak, DA. Bacterial and protozoal gastroenteritis. New Engl. J. Med 1991, 325, 327–340. [Google Scholar]
- Bonnin, A; Dei-cas, E; Camerlynk, P. Cryptosporidium and Isospora. In Molecular and cell biology and Opportunistic Infections in Aids; Myint, S, Cann, A, Eds.; Chapman and Hall: London, UK, 1992; pp. 123–135. [Google Scholar]
- Caccio, S; Pinter, E; Fantini, R; Mezzaroma, I; Pozio, E. Human infection with Cryptosporidium feli: case report and literature review. Emerg. Infect. Dis 2002, 8, 85–86. [Google Scholar]
- Steinhauserovà, I; Fojtkovà, K. Serotyping and identification of Campylobacter jejuni and Campylobacter coli strains of human and animal origin using the PCR method. Acta Vet. Brno 1999, 68, 149–154. [Google Scholar]
- Hien, BT; Scheutz, F; Cam, PD; Serichantalergs, O; Huong, TT; Thu, TM; Dalsgaard, A. Diarrheagenic Escherichia coli and Shigella strains isolated from children in a hospital case-control study in Hanoi, Vietnam. J. Clin. Microbiol 2008, 46, 996–1004. [Google Scholar]
- Okoh, AI; Osode, AN. Enterotoxigenic Escherichia coli (ETEC): a recurring decimal in infants' and travelers' diarrhea. Rev. Environ. Health 2008, 23, 135–148. [Google Scholar]
- Levine, MM; Ferrechio, C; Prado, V; Cayazzo, M; Abrego, P; Martinez, J; Maggi, L; Baldini, MM; Martin, W; Maneval, D; Kay, B; Guers, L; Lior, H; Wasserman, SS; Nataro, JP. Epidemiologic studies of Escherichia coli diarrheal infections in a low socioeconomic level peri-urban community in Santiago, Chile. Am. J. Epidemiol 1993, 138, 849–869. [Google Scholar]
- Molbak, K; Wested, N; Hojling, N; Scheutz, F; Gottshau, P; Aaby, P; José da Silva, AP. The etiology of early diarrhea: a community study from Guinea-Bissau. J. Infect. Dis 1994, 169, 581–587. [Google Scholar]
- Sur, D; Manna, B; Deb, AK; Deen, JL; Danovaro-Holliday, MC; von Seidlein, L; Clemens, JD; Bhattacharya, SK. Factors associated with reported diarrhoea episodes and treatment-seeking in an urban slum of Kolkata, India. J. Health Popul. Nutr 2004, 22, 130–138. [Google Scholar]
- Maranhão, HS; Medeiros, MC; Scaletsky, IC; Fagundes-Neto, U; Morais, MB. The epidemiological and clinical characteristics and nutritional development of infants with acute diarrhoea, in north-eastern Brazil. Ann Trop Med Parasitol 2008, 102, 357–365. [Google Scholar]
- Simpson, E; Wittet, S; Bonilla, J; Gamazina, K; Cooley, L; Winkler, JL. Use of formative research in developing a knowledge translation approach to rotavirus vaccine introduction in developing countries. BMC Public Health 2007, 7, 281–292. [Google Scholar]
- McMichael, AJ. The Urban Environment and Health in a World of Increasing Globalization: Issues for Developing Countries. Bull.World Health Organ 2000, 78, 1117–1126. [Google Scholar]
- Bhatnagar, S; Bhan, MK; Sommerfelt, H; Sazawal, S; Kumar, R; Saini, S. Enteroaggregative Escherichia coli may be a new pathogen causing acute and persistent diarrhea. Scand. J. Infect. Dis 1993, 25, 579–583. [Google Scholar]
- Gomes, TAT; Rassi, V; Macdonald, KL. Enteropathogens associated with acute diarrheal diseases in urban infants in Sao paulo, Brazil. J. Infect. Dis 1991, 164, 331–337. [Google Scholar]
- Steele, AD; Peenze, I; de Beer, MC; Pager, CT; Yeats, J; Potgieter, N; Ramsaroop, U; Page, NA; Mitchell, JO; Geyer, A; Bos, P; Alexander, JJ. Anticipating Rotavirus vaccine: epidemiology and surveillance of rotavirus in South Africa. Vaccine 2003, 21, 354–360. [Google Scholar]
- Samal, SK; Khuntia, HK; Nanda, PK; Satapathy, CS; Nayak, SR; Sarangi, AK; Sahoo, N; Pattnaik, SK; Chhotray, GP; Pal, BB. Incidence of bacterial enteropathogens among hospitalized diarrhea patients from Orissa, India. Jpn. J. Infect. Dis 2008, 61, 350–355. [Google Scholar]
- Karki, A; Tiwari, BR. Prevalence of acute diarrhoea in Kathmandu Valley. J. Nepal Assoc 2007, 46, 175–179. [Google Scholar]
- Foy, HM. Adenoviruses. In Viral Infections in Humans: epidemiology and control, 4th Edition; Evans, A, Kaslow, R, Eds.; Plenum: New York, 1997; pp. 119–138. [Google Scholar]
- Gascón, J; Vargas, M; Schellenberg, D; Urassa, H; Casals, C; Kahigwa, J; Aponte; Mshinda, H; Vila, J. Diarrhea in Children under 5 Years of Age from Ifakara, Tanzania: a Case-Control Study. J. Clin. Microbiol 2000, 38, 4459–4462. [Google Scholar]
- Lindblom, GB; Ahren, J; Changalucha, R; Gabone, R; Kaijser, B; Nilsson, LA; Sjögren, E; Svennerholm, AM; Temu, M. Campylobacter jejuni/coli and enterotoxigenic Escherichia coli (ETEC) in faeces from children and adults in Tanzania. Scand. J. Infect. Dis 1995, 27, 589–593. [Google Scholar]
- Vargas, M; Gascon, J; Gallardo, F; Jimenez De Anta, MT; Vila, J. Prevalence of diarrheagenic Esherichia coli strains detected by PCR in patients with traveler diarrhea. Clin. Microbiol. Infect 1998, 4, 682–688. [Google Scholar]
- Urio, EM; Collison, EK; Gashe, BA; Sebunya, TH; Mpuchane, S. Shigela and salmonella strains isolated from children under 5 years of age in Gaborone, Bostwana, and their antibiotic susceptibility patterns. Trop. Med. Intern. Health 2001, 6, 55–59. [Google Scholar]
- Meider, C; Cerf, M. Diarrhées à Shigelles, à Colibacilles entéro-invasifs entéro-hémorragiques et à Colibacilles. In Diarrhées aigues infectieuses; Doin: Paris, 1993; pp. 67–76. [Google Scholar]
- Oyofo, BA; Subekti, D; Tjaniadi, P; Machpud, N; Komalarini, S; Setiawan, B; Simanjuntak, C; Punjabi, N; Corwin, AL; Wasfy, M; Campbell, JR; Lesmana, M. Enteropathogens associated with acute diarrhea in community and hospital patients in Jakarta, Indonesia. FEMS Immunol. Med. Microbiol 2002, 34, 139–146. [Google Scholar]
- Sansonetti, PJ. Mécanismes moléculaires et cellulaires de l’infection du tube digestif par les bactéries entéro-invasives. Des modèles cellulaires à la dysentérie. In Diarrhées aigues infectieuses; Doin: Paris, France, 1993; pp. 43–51. [Google Scholar]
- Gomez, HF; Cleary, TG. E. coli as cause of diarrhea in children. Semin. Pediatr. Infect. Dis 1994, 5, 175–182. [Google Scholar]
- Notario, R; Borda, N; Gambande, T; Sutich, E. Species and serovars of enteropathogenic agents associated with acute diarrheal disease in Rosario, Argentina. Rev. Inst. Med. Trop. S. Paulo 1996, 38, 5–7. [Google Scholar]
- Gray, LD. Escherichia, Salmonella, Shigella and Yersina. In Manual of clinical microbiology; Murray, PR, Baron, EJ, Pfaller, MA, Tenover, FC, Yolken, RH, Eds.; American Society for Microbiology: Washington, DC, 1995; pp. 450–456. [Google Scholar]
- Adhikari, M; Coovadia, Y; Hewitt, J. Enteropathogenic Escherichia coli (EPEC) and enterotoxigenic (ETEC) related diarrhoeal disease in a neonatal unit. An. Trop. Paediatr 1995, 5, 19–22. [Google Scholar]
- Molbak, K; Wested, N; Hojling, N; Scheutz, F; Gottshau, P; Aaby, P; José da Silva, AP. The etiology of early diarrhea: a community study from Guinea-Bissau. J. Infect. Dis 1994, 169, 581–587. [Google Scholar]
- Nataro, JP; Baldini, MM; Kaper, JB; Black, RE; Bravo, N; Levine, MM. Detection of an adherence factor of enteropathogenic Escherichia coli with a DNA probe. J. Infect. Dis 1985, 152, 560–565. [Google Scholar]
- Howard, P. Bacterial, viral and parasitic aetiology of paediatric diarrhoea in the Highlands of Papua-New Guinea. J. Trop. Pediatr 2000, 46, 10–14. [Google Scholar]
- Addy, PA; Antepim, G; Frimpong, EH. Prevalence of pathogenic Escherichia coli and parasites in infants with diarrhoea in Kumasi, Ghana. East Afr. Med. J 2004, 81, 353–357. [Google Scholar]
- Stoffel, V; Chague, F. Declared diseases, observed diseases and health priorities in a Benin rural district. Santé Publique 2001, 13, 17–25. [Google Scholar]
- Pai, M; Kang, G; Ramakrishna, BS; Venkataraman, A; Muliyil, J. An epidemic of diarrhoea in south India caused by enteroaggregative Escherichia coli. Indian J. Med. Res 1997, 106, 7–12. [Google Scholar]
- Presterl, E; Zwick, RH; Reichmann, S; Aichelburg, A; Kremsner, PG; Winkler, S; Graninger, W. Frequency and virulence properties of diarrheagenic Escherichia coli in children with diarrhea in Gabon. Am. J. Trop. Med. Hyg 2003, 69, 406–410. [Google Scholar]
- Gonzalez, R; Diaz, C; Marino, M; Cloralt, R; Pequeneze, M; Perez-Schael, I. Age-specific prevalence of Escherichia coli with localized and aggregative adherence in Venezuelan infants with acute diarrhea. J. Clin. Microbiol 1997, 35, 1103–1107. [Google Scholar]
- Lima, AAM; Fang, G; Schorling, JB; de Albuquerque, L; McAuliffe, JF; Mota, S; Leite, R; Guerrant, RL. Persistent diarrhea in Northeast Brazil: Etiologies and interactions with malnutrition. Acta Pediatr.Scand 1992, 381 Suppl, 39–44. [Google Scholar]
- Kaur, R; Rawat, D; Kakkar, M; Uppal, B; Sharma, VK. Intestinal parasites in children with diarrhea in Delhi, India. Southeast Asian J. Trop. Med. Publ. Health 2002, 33, 725–729. [Google Scholar]
- Tumwine, JK; Thompson, J; Katua-Katua, M; Mujwajuzi, M; Johnstone Porras, I. Diarrhea and effects of different water sources, sanitation and hygiene behavior in East Africa. Trop. Med. Int. Health 2002, 7, 750–756. [Google Scholar]
- Woldemicael, G. Diarrhoeal morbidity among young children in Eritrea: environmental and socio-economic determinants. J. Health Popul. Nutr 2001, 19, 83–90. [Google Scholar]
- Nguendo Yongsi, HB; Herrmann, MT; Lutumba Ntetu, A; Sietchiping, R; Bryant, C. Environmental Sanitation and Health Risks in Tropical Urban Settings: Case Study of Household Refuse and Diarrhea in Yaoundé-Cameroon. Int. J. Soci. Sci 2008, 3, 220–229. [Google Scholar]
- Remon, RA; Thomas, W; Frenck, R; Putnam, SD; Rao, MR; Savarino, SJ; Kamal, KA; Peruski, LF; Abd-El, MIA; El-Alkamy, SA; Naficy, AB; Clemens, JD. Epidemiology of shigella-associated diarrhea in rural Egyptian children. Am. J. Trop. Med. Hyg 2004, 71, 367–372. [Google Scholar]
- Shah, SB; Hanauer, SB. Treatment of diarrhea in patients with inflammatory bowel disease: concepts and cautions. Rev. Gastroenterol. Disord 2007, 7, 3–10. [Google Scholar]
- Dennehy, PH. Transmission of rotavirus and other enteric pathogens in the home. Pediatr. Infect. Dis. J 2000, 19, 103–105. [Google Scholar]
- Huttly, S. The Impact of Inadequate Sanitary Conditions on Health in Developing Countries; London School of Hygiene and Tropical Medicine, Maternal and Child Epidemiology Unit: London, 2002. [Google Scholar]
- Black, M; Fawcett, B. The Last Taboo: Opening the Door on the Global Sanitation Crisis; Earthscan Publications: London, UK, 2008. [Google Scholar]
- Nguendo Yongsi, HB. Urbanization and communicable diseases in Cameroon; University of Paris X: Nanterre, France, 2000; p. 151. [Google Scholar]
© 2008 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license ( http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Yongsi, H.B.N. Pathogenic Microorganisms Associated With Childhood Diarrhea in Low-and-Middle Income Countries: Case Study of Yaoundé – Cameroon. Int. J. Environ. Res. Public Health 2008, 5, 213-229. https://doi.org/10.3390/ijerph5040213
Yongsi HBN. Pathogenic Microorganisms Associated With Childhood Diarrhea in Low-and-Middle Income Countries: Case Study of Yaoundé – Cameroon. International Journal of Environmental Research and Public Health. 2008; 5(4):213-229. https://doi.org/10.3390/ijerph5040213
Chicago/Turabian StyleYongsi, H. B. Nguendo. 2008. "Pathogenic Microorganisms Associated With Childhood Diarrhea in Low-and-Middle Income Countries: Case Study of Yaoundé – Cameroon" International Journal of Environmental Research and Public Health 5, no. 4: 213-229. https://doi.org/10.3390/ijerph5040213
APA StyleYongsi, H. B. N. (2008). Pathogenic Microorganisms Associated With Childhood Diarrhea in Low-and-Middle Income Countries: Case Study of Yaoundé – Cameroon. International Journal of Environmental Research and Public Health, 5(4), 213-229. https://doi.org/10.3390/ijerph5040213