
SleepShifters: The Co-Development of a Preventative Sleep Management Programme for Shift Workers and Their Employers

 ,
,  , , ,
, , ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Procedure
2.2.1. Theory and Evidence-Based Approach
2.2.2. Partnership Approach: Co-Production
- Stage 1)
- Start-up and Planning
- Stage 2)
- Understanding Stakeholder Needs, Wants, and Preferences
- (1)
- To understand the impact(s) of shift work and identify areas of priority.
- (2)
- To identify potential ways to address priority areas.
- (3)
- To identify potential facilitators and/or modes of intervention delivery.
- (4)
- To identify potential barriers and facilitators to implementation and engagement—what should a good sleep management programme look like?
Employee Co-Production Workshops
Employer Representative Interviews
- Stage 3)
- Expert Review and Consolidation: Protocol Development
- Stage 4)
- Stakeholder Review and Expert Consolidation
Employee Review Workshops
Employer Focus Group
2.3. Ethical Considerations
3. Results
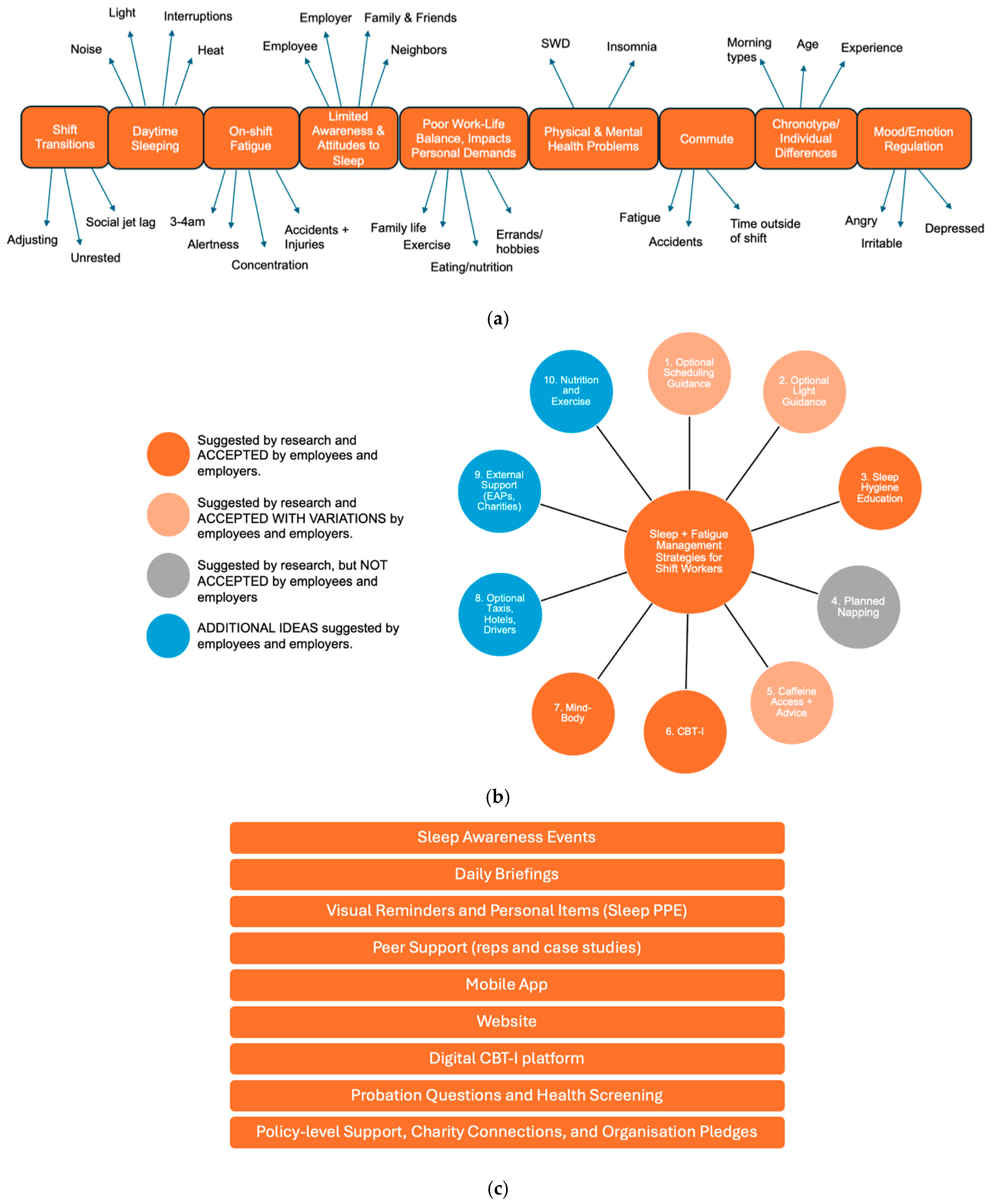
3.1. Understanding Stakeholder Needs, Wants, and Preferences: Input from Employee Co-Production Workshops and Employer Representative Interviews
- (1)
- To understand the impact(s) of shift work and identify areas of priority.
- (2)
- To identify potential ways to address priority areas.
- (3)
- To identify potential facilitators/modes of intervention delivery
- (4)
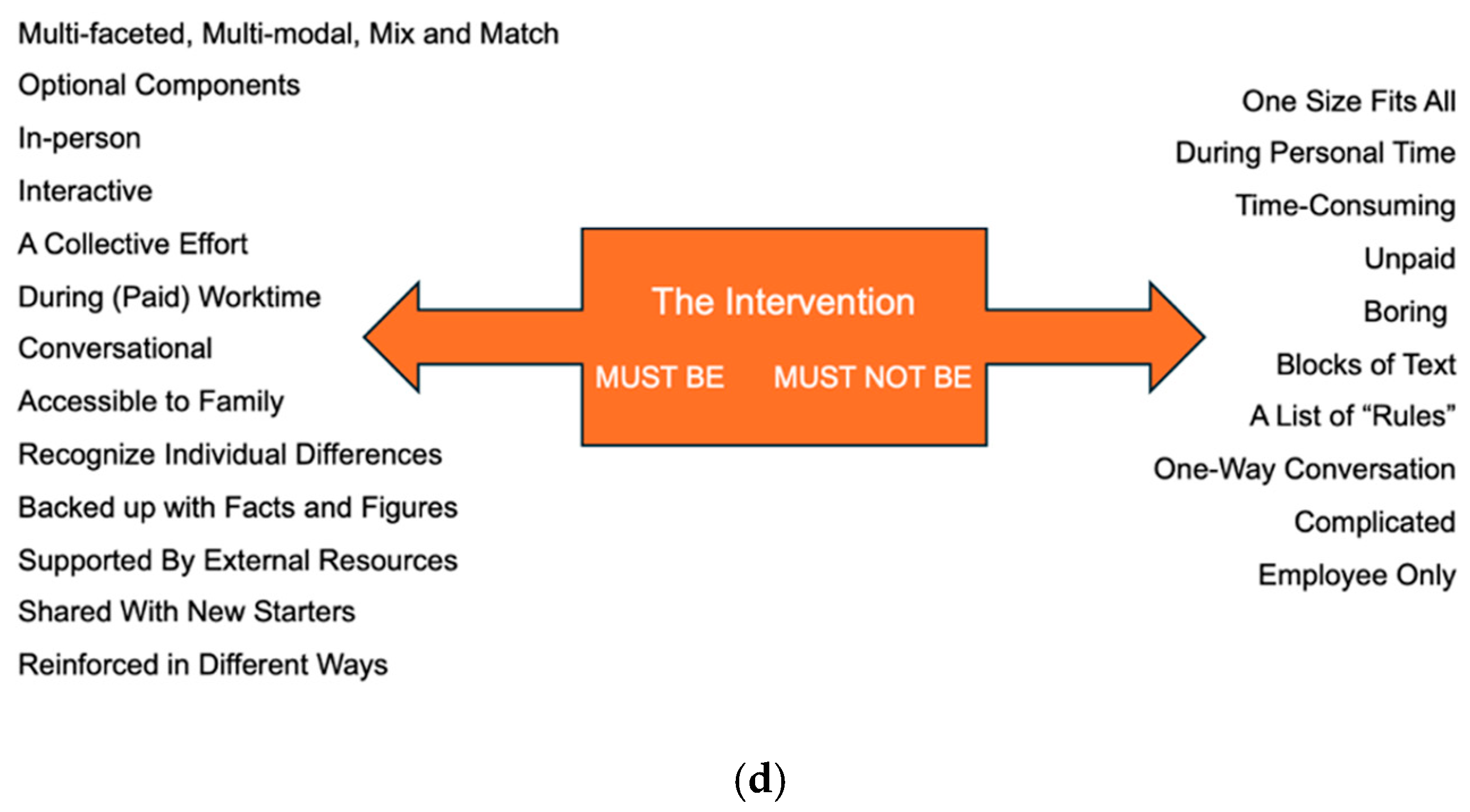
- To identify potential barriers and facilitators to implementation and engagement—what should a good sleep management programme look like?
3.2. Expert Review and Consolidation: Protocol Development
3.3. Stakeholder Review and Expert Refinement
3.3.1. SleepShifters
- (1)
- The Sleep Show:
- (2)
- Sleep Smart Induction:
- (3)
- Sleep Talks Campaign—We Need to Talk About Sleep:
- (4)
- SleepShifters Hub:
- (5)
- SleepSync:
3.3.2. Onboarding and Support with Implementation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rajaratnam, S.M.; Howard, M.E.; Grunstein, R.R. Sleep loss and circadian disruption in shift work: Health burden and management. Med. J. Aust. 2013, 199, S11–S15. [Google Scholar] [CrossRef] [PubMed]
- Pallesen, S.; Bjorvatn, B.; Waage, S.; Harris, A.; Sagoe, D. Prevalence of shift work disorder: A systematic review and meta-analysis. Front. Psychol. 2021, 12, 638252. [Google Scholar] [CrossRef]
- Itani, O.; Kaneita, Y. The association between shift work and health: A review. Sleep Biol. Rhythm. 2016, 14, 231–239. [Google Scholar] [CrossRef]
- Silva, A.; Silva, A.; Duarte, J.; da Costa, J.T. Shift-work: A review of the health consequences. Int. J. Occup. Environ. Saf. 2020, 4, 48–79. [Google Scholar] [CrossRef]
- Torquati, L.; Mielke, G.I.; Brown, W.J.; Burton, N.W.; Kolbe-Alexander, T.L. Shift work and poor mental health: A meta-analysis of longitudinal studies. Am. J. Public Health 2019, 109, e13–e20. [Google Scholar] [CrossRef]
- Walker, W.H.; Walton, J.C.; DeVries, A.C.; Nelson, R.J. Circadian rhythm disruption and mental health. Transl. Psychiatry 2020, 10, 28. [Google Scholar] [CrossRef]
- Hui, S.K.A.; Grandner, M.A. Trouble sleeping associated with lower work performance and greater health care costs: Longitudinal data from Kansas State Employee Wellness Program. J. Occup. Environ. Med. 2015, 57, 1031–1038. [Google Scholar] [CrossRef]
- Ryu, J.; Jung-Choi, K.; Choi, K.H.; Kwon, H.J.; Kang, C.; Kim, H. Associations of shift work and its duration with work-related injury among electronics factory workers in South Korea. Int. J. Environ. Res. Public Health 2017, 14, 1429. [Google Scholar] [CrossRef]
- Wong, I.S.; McLeod, C.B.; Demers, P.A. Shift work trends and risk of work injury among Canadian workers. Scand. J. Work Environ. Health 2011, 37, 54–61. [Google Scholar] [CrossRef]
- Culpepper, L. The social and economic burden of shift-work disorder. J. Fam. Pr. 2010, 59, S3. [Google Scholar]
- Hafner, M.; Stepanek, M.; Taylor, J.; Troxel, W.M.; Van Stolk, C. Why sleep matters—The economic costs of insufficient sleep: A cross-country comparative analysis. Rand Health Q. 2017, 6, 11. [Google Scholar]
- Schroeck, J.L.; Ford, J.; Conway, E.L.; Kurtzhalts, K.E.; Gee, M.E.; Vollmer, K.A.; Mergenhagen, K.A. Review of safety and efficacy of sleep medicines in older adults. Clin. Ther. 2016, 38, 2340–2372. [Google Scholar] [CrossRef]
- Shriane, A.E.; Rigney, G.; Ferguson, S.A.; Bin, Y.S.; Vincent, G.E. Healthy sleep practices for shift workers: Consensus sleep hygiene guidelines using a Delphi methodology. Sleep 2023, 46, zsad182. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.C.; Sweetman, A.; Crowther, M.E.; Paterson, J.L.; Scott, H.; Lechat, B.; Wanstall, S.E.; Brown, B.W.; Lovato, N.; Adams, R.J.; et al. Is cognitive behavioral therapy for insomnia (CBTi) efficacious for treating insomnia symptoms in shift workers? A systematic review and meta-analysis. Sleep Med. Rev. 2023, 67, 101716. [Google Scholar] [CrossRef]
- Koffel, E.; Bramoweth, A.D.; Ulmer, C.S. Increasing access to and utilization of cognitive behavioral therapy for insomnia (CBT-I): A narrative review. J. Gen. Intern. Med. 2018, 33, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Mayer, A.; The Sleepless Job Chart—Amerisleep. Amerisleep. 2023. Available online: https://amerisleep.com/blog/sleepless-job-chart/ (accessed on 20 July 2024).
- Papantoniou, K.; Vetter, C.; Schernhammer, E.S. Shift work practices and opportunities for intervention. Occup. Environ. Med. 2017, 74, 2–3. [Google Scholar] [CrossRef]
- Wong, I.S.; Popkin, S.; Folkard, S. Working Time Society consensus statements: A multi-level approach to managing occupational sleep-related fatigue. Ind. Health 2019, 57, 228–244. [Google Scholar] [CrossRef] [PubMed]
- NHS Employers. The Health, Safety and Wellbeing of Shift Workers in Healthcare Environments. 2025. Available online: https://www.nhsemployers.org/publications/health-safety-and-wellbeing-shift-workers-healthcare-environments (accessed on 22 July 2025).
- SI 1998/1833; The Working Time Regulations 1998. Her Majesty’s Stationery Office: Norwich, UK, 1998.
- Tout, A.F.; Tang, N.K.Y.; Sletten, T.L.; Toro, C.T.; Kershaw, C.; Meyer, C.; Rajaratnam, S.M.W.; Moukhtarian, T.R. Current sleep interventions for shift workers: A mini review to shape a new preventative, multicomponent sleep management programme. Front. Sleep 2024, 3, 1343393. [Google Scholar] [CrossRef]
- Bragge, P.; Burns, J.; Kellner, P.; Allan, M.; Fitzgerald, D.; Grundy, E.; Lennox, A.; Moukhtarian, T.R.; Rajaratnam, M.W.S.; Sletten, T.L. Sleep Health Interventions for Managing Mental Health in Shift Workers: A Systematic Review. In Monash Sustainable Development Institute Evidence Review Service; Monash University: Melbourne, Australia, 2023. [Google Scholar]
- Redeker, N.S.; Caruso, C.C.; Hashmi, S.D.; Mullington, J.M.; Grandner, M.; Morgenthaler, T.I. Workplace interventions to promote sleep health and an alert, healthy workforce. J. Clin. Sleep Med. 2019, 15, 649–657. [Google Scholar] [CrossRef]
- Ray, D. Developing and Testing an Intervention for Shiftwork Sleep Disorder in NHS Workers. Eur. PMC 2023, NIHR203667. Available online: https://www.fundingawards.nihr.ac.uk/award/NIHR203667 (accessed on 22 July 2024).
- Declercq, I.; Van Den Eede, F.; Roelant, E.; Verbraecken, J. SHIFTPLAN: A randomized controlled trial investigating the effects of a multimodal shift-work intervention on drivers’ fatigue, sleep, health, and performance parameters. Trials 2022, 23, 662. [Google Scholar] [CrossRef]
- Damen, M.A.; Detaille, S.I.; Robroek, S.J.; Engels, J.A.; De Lange, A.H. Factors associated with blue-collar workers’ participation in Worksite Health Promotion Programs: A scoping literature review. Health Promot. Int. 2023, 38, daad052. [Google Scholar] [CrossRef]
- Office for Health Improvement Disparities Health disparities health inequalities: Applying All Our Health, GOV.UK. 2022. Available online: https://www.gov.uk/government/publications/health-disparities-and-health-inequalities-applying-all-our-health (accessed on 20 July 2024).
- Duncan, E.; O’Cathain, A.; Rousseau, N.; Croot, L.; Sworn, K.; Turner, K.M.; Yardley, L.; Hoddinott, P. Guidance for reporting intervention development studies in health research (GUIDED): An evidence-based consensus study. BMJ Open 2020, 10, e033516. [Google Scholar] [CrossRef]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Boyd, K.A.; Craig, N.; French, D.P.; McIntosh, E.; et al. Framework for the development and evaluation of complex interventions: Gap analysis, workshop and consultation-informed update. Health Technol. Assess. 2021, 25, 1. [Google Scholar] [CrossRef]
- O’Cathain, A.; Croot, L.; Duncan, E.; Rousseau, N.; Sworn, K.; Turner, K.M.; Yardley, L.; Hoddinott, P. Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open 2019, 9, e029954. [Google Scholar] [CrossRef]
- O’Cathain, A.; Croot, L.; Sworn, K.; Duncan, E.; Rousseau, N.; Turner, K.; Yardley, L.; Hoddinott, P. Taxonomy of approaches to developing interventions to improve health: A systematic methods overview. Pilot Feasibility Stud. 2019, 5, 41. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Hickey, G.; Brearley, S.; Coldham, T.; Denegri, S.; Green, G.; Staniszewska, S.; Tembo, D.; Torok, K.; Turner, K. Guidance on Co-producing a Research Project; Involve: Southampton, UK, 2018. [Google Scholar]
- Farr, M.; Davies, P.; Andrews, H.; Bagnall, D.; Brangan, E.; Davies, R. Co-producing knowledge in health and social care research: Reflections on the challenges and ways to enable more equal relationships. Humanit. Soc. Sci. Commun. 2021, 8, 105. [Google Scholar] [CrossRef]
- NIHR. A Brief Guide to Patient and Public Involvement and Qualitative Methods Within Health and Social Care Research; National Institute for Health Research: Southampton, UK, 2020; Available online: https://www.rds-nw.nihr.ac.uk/wpcontent/uploads/2021/11/RDS_Guide_to_PPI_qualitative_methods.pdf (accessed on 30 June 2023).
- Austin, J.; Van Dijk, J.; Drossaert, C. When theory meets users in co-design: Four strategies towards synergy between bottom-up and top-down input. In Proceedings of the Synergy—DRS International Conference 2020, Online, 11–14 August 2020. [Google Scholar]
- Kaisler, R.E.; Kulnik, S.T.; Klager, E.; Kletecka-Pulker, M.; Schaden, E.; Stainer-Hochgatterer, A. Introducing patient and public involvement practices to healthcare research in Austria: Strategies to promote change at multiple levels. BMJ Open 2021, 11, e045618. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- Järnefelt, H.; Spiegelhalder, K. CBT-I Protocols for Shift Workers and Health Operators. In Cognitive-Behavioural Therapy for Insomnia (CBT-I) Across the Life Span: Guidelines and Clinical Protocols for Health Professionals; Wiley-Blackwell: Hoboken, NJ, USA, 2022; pp. 126–132. [Google Scholar]
- Moukhtarian, T.R.; Patel, K.; Toro, C.; Russel, S.; Daly, G.; Walasek, L.; Tang, N.K.Y.; Meyer, C. Effects of a hybrid digital cognitive–behavioural therapy for insomnia and emotion regulation in the workplace (SLEEP): Study protocol for a randomised waitlist control trial. BMJ Open 2022, 12, e058062. [Google Scholar] [CrossRef]
- Moukhtarian, T.R.; Fletcher, S.; Walasek, L.; Patel, K.; Toro, C.; Hurley-Wallace, A.L.; Kershaw, C.; Russel, S.; Daly, G.; Tang, N.K.Y.; et al. Digital CBT for Insomnia and Emotion Regulation in the Workplace: A randomised waitlist-controlled trial. Psychol. Med. 2025, 55, e52. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.M.; Magee, M.; Giliberto, E.S.; Booker, L.A.; Tucker, A.J.; Galaska, B.; Sibenaller, S.M.; Baer, S.A.; Postnova, S.; Sondag, T.A.; et al. Mobile app for personalized sleep–wake management for shift workers: A user testing trial. Digit. Health 2023, 9, 20552076231165972. [Google Scholar] [CrossRef] [PubMed]
- Varma, P.; Postnova, S.; Knock, S.; Howard, M.E.; Aidman, E.; Rajaratnam, S.W.; Sletten, T.L. SleepSync: Early Testing of a Personalised Sleep–Wake Management Smartphone Application for Improving Sleep and Cognitive Fitness in Defence Shift Workers. Clocks Sleep 2024, 6, 267–280. [Google Scholar] [CrossRef] [PubMed]
- Miguel, C.; Amarnath, A.; Akhtar, A.; Malik, A.; Baranyi, G.; Barbui, C.; Karyotaki, E.; Cuijpers, P. Universal, selective and indicated interventions for supporting mental health at the workplace: An umbrella review of meta-analyses. Occup. Environ. Med. 2023, 80, 225–236. [Google Scholar] [CrossRef]
- Vega-Escaño, J.; Porcel-Gálvez, A.M.; de Diego-Cordero, R.; Romero-Sánchez, J.M.; Romero-Saldaña, M.; Barrientos-Trigo, S. Insomnia interventions in the workplace: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 6401. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Core Element | Considerations at the Development Stage |
|---|---|
| Consider Context | Consider the context of employment for shift workers based on industry type and job role, and how this could impact intervention acceptability. Ensure programme content can be modified and tailored to meet the needs of each organisation and have examples relatable to employees across settings. |
| Develop, Refine, and (Re)test Programme Theory | Through discussion with stakeholders and research team experts, establish a theory of change for the programme and illustrate it via a logic model. Continue to refine the theory of change in subsequent phases through process evaluation with stakeholders. |
| Engaging Stakeholders | Engage shift workers and employer representatives throughout the development phase via interviews, co-production workshops, and focus groups. Use an iterative process to collaboratively identify and co-develop intervention components, their ideal format, and mode(s) of delivery. |
| Identify Key Uncertainties | Identify key uncertainties relating to intervention components, their associated format, and mode(s) of delivery through discussion with stakeholders and research team experts (e.g., appropriateness of language, intervention delivery costs, impact of personal demands on sleep schedules and opportunity). |
| Refine Intervention | Co-develop and refine the intervention protocol in line with stakeholder input and research team experts at all stages of development and beyond (i.e., Phase 2, feasibility trials). |
| Economic Considerations | Explore economic costs associated with intervention delivery through employer interviews and focus groups (e.g., web hosting costs, staff training, time off shifts to participate in programme elements, etc.). Assess cost-effectiveness in subsequent phases. |
| Organisation | Industrial Sector | Size * | Area of Operation | Location of Co-Production | Shift Pattern | Shift Duration |
|---|---|---|---|---|---|---|
| Org A | Manufacturing | Large | International | Midlands, England | 4 on, 4 off (individuals work only nights or only days) | 12 h |
| Org B | Civil engineering/ Construction | Large | United Kingdom, Ireland, and North America | Southeast England | Irregular—mixture of days and nights, up to 14 consecutive shifts | Up to 14 h door-to-door |
| Org C | Civil engineering/ construction/ rail services | Large | United Kingdom | Midlands, England | Irregular—mixture of days and nights, up to 14 consecutive shifts | Up to 14 h door-to-door |
| Org D | Civil engineering/construction/ | Large | United Kingdom | North England | Irregular—mixture of days and nights, nights mostly on weekends | Up to 12 h door-to-door |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tout, A.F.; Tang, N.K.Y.; Toro, C.T.; Sletten, T.L.; Rajaratnam, S.M.W.; Kershaw, C.; Meyer, C.; Moukhtarian, T.R. SleepShifters: The Co-Development of a Preventative Sleep Management Programme for Shift Workers and Their Employers. Int. J. Environ. Res. Public Health 2025, 22, 1178. https://doi.org/10.3390/ijerph22081178
Tout AF, Tang NKY, Toro CT, Sletten TL, Rajaratnam SMW, Kershaw C, Meyer C, Moukhtarian TR. SleepShifters: The Co-Development of a Preventative Sleep Management Programme for Shift Workers and Their Employers. International Journal of Environmental Research and Public Health. 2025; 22(8):1178. https://doi.org/10.3390/ijerph22081178
Chicago/Turabian StyleTout, Amber F., Nicole K. Y. Tang, Carla T. Toro, Tracey L. Sletten, Shantha M. W. Rajaratnam, Charlotte Kershaw, Caroline Meyer, and Talar R. Moukhtarian. 2025. "SleepShifters: The Co-Development of a Preventative Sleep Management Programme for Shift Workers and Their Employers" International Journal of Environmental Research and Public Health 22, no. 8: 1178. https://doi.org/10.3390/ijerph22081178
APA StyleTout, A. F., Tang, N. K. Y., Toro, C. T., Sletten, T. L., Rajaratnam, S. M. W., Kershaw, C., Meyer, C., & Moukhtarian, T. R. (2025). SleepShifters: The Co-Development of a Preventative Sleep Management Programme for Shift Workers and Their Employers. International Journal of Environmental Research and Public Health, 22(8), 1178. https://doi.org/10.3390/ijerph22081178