

Mental Health Outcomes Among Travestis and Transgender Women in Brazil: A Literature Review and a Call to Action for Public Health Policies

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection and Data Extraction
2.4. Data Synthesis
3. Results
3.1. Overview of Included Studies
3.2. Mental Health Outcomes Among Travestis and Transgender Women in Brazil
3.3. Intersecting Social and Health Disparities Faced by Travestis and Transgender Women in Brazil
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Beckwith, N.; McDowell, M.J.; Reisner, S.L.; Zaslow, S.; Weiss, R.D.; Mayer, K.H.; Keuroghlian, A.S. Psychiatric Epidemiology of Transgender and Nonbinary Adult Patients at an Urban Health Center. LGBT Health 2019, 6, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Reisner, S.L.; White Hughto, J.M.; Gamarel, K.E.; Keuroghlian, A.S.; Mizock, L.; Pachankis, J. Discriminatory Experiences Associated with Posttraumatic Stress Disorder Symptoms among Transgender Adults. J. Couns. Psychol. 2016, 63, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Pinna, F.; Paribello, P.; Somaini, G.; Corona, A.; Ventriglio, A.; Corrias, C.; Frau, I.; Murgia, R.; El Kacemi, S.; Galeazzi, G.M.; et al. Mental Health in Transgender Individuals: A Systematic Review. Int. Rev. Psychiatry 2022, 34, 292–359. [Google Scholar] [CrossRef] [PubMed]
- Spizzirri, G.; Eufrásio, R.; Lima, M.C.P.; de Carvalho Nunes, H.R.; Kreukels, B.P.C.; Steensma, T.D.; Abdo, C.H.N. Proportion of People Identified as Transgender and Non-Binary Gender in Brazil. Sci. Rep. 2021, 11, 2240. [Google Scholar] [CrossRef]
- Freitas, F.L.S.; Bermúdez, X.P.C.D.; Merchán-Hamann, E.; Dias dos Santos, A.S.; Vieira, V.F. Social and Programmatic Vulnerability in the Context of Transgender People’s Health: A Scoping Review of Scientific Evidence from Brazil. Int. J. Equity Health 2024, 23, 272. [Google Scholar] [CrossRef]
- Trans Murder Monitoring (TMM). TMM Update TDoR 2022; Transgender Europe (TGEU): Berlin, Germany, 2022; Available online: https://transrespect.org/en/tmm-update-tdor-2022/ (accessed on 19 April 2025).
- Benevides BG (Ed.) Dossiê Assassinatos e Violências Contra Travestis e Transexuais Brasileiras em 2021 [Dossier on Murders and Violence Against Brazilian Travestis and Transgender and Gender Diverse People in 2021]; Distrito Drag: Brasília, Brazil, 2023. [Google Scholar]
- Carvalho, M. “Travesti”, “mulher transexual”, “homem trans” e “não binário”: Interseccionalidades de classe e geração na produção de identidades políticas. Cad. Pagu 2018, 52, e185211. [Google Scholar] [CrossRef]
- Cesar, G.A.; do Lago, B.V.; Ortiz Tanaka, T.S.; Zanini, P.B.; Bandeira, L.M.; Puga, M.A.M.; Pires Fernandes, F.R.; Pinto, C.S.; Castro, L.S.; Bertolacci-Rocha, L.G.; et al. Differences in Risky Sexual Behaviors and HIV Prevalence between Men Who Have Sex with Men and Transgender Women in the Midwest Brazil. PLoS Glob. Public Health 2024, 4, e0003061. [Google Scholar] [CrossRef]
- Leite, B.O.; Magno, L.; Bastos, F.I.; Dourado, I. Association between In-Country Migration and HIV Infection among Transgender Women from Northeastern Brazil: A Respondent-Driven Sampling Survey. BMC Public Health 2024, 24, 589. [Google Scholar] [CrossRef]
- Dourado, I.; Magno, L.; Leite, B.O.; Bastos, F.I.; da Mota, J.C.; Veras, M.A.d.S.M. TransOdara Research Group Prevalence of HIV Infection among Transgender Women and Travestis in Brazil: Data from the TransOdara Study. Rev. Bras. Epidemiol. Braz. J. Epidemiol. 2024, 27 (Suppl. S1), e240004.supl.1. [Google Scholar] [CrossRef]
- Ferreira, A.C.G.; Coelho, L.E.; Jalil, E.M.; Luz, P.M.; Friedman, R.K.; Guimarães, M.R.C.; Moreira, R.C.; Eksterman, L.F.; Cardoso, S.W.; Castro, C.V.; et al. Transcendendo: A Cohort Study of HIV-Infected and Uninfected Transgender Women in Rio de Janeiro, Brazil. Transgender Health 2019, 4, 107–117. [Google Scholar] [CrossRef]
- Eccles, H.; Abramovich, A.; Patte, K.A.; Elton-Marshall, T.; Racine, N.; Ferro, M.A.; Edwards, J.; Anderson, K.K.; Afifi, T.O.; Geoffroy, M.-C.; et al. Mental Disorders and Suicidality in Transgender and Gender-Diverse People. JAMA Netw. Open 2024, 7, e2436883. [Google Scholar] [CrossRef] [PubMed]
- Hochheimer, M.; Glick, J.L.; Garrison-Desany, H.; Huhn, A.S. Transgender Individuals Are at Higher Risk for Suicidal Ideation and Preparation than Cisgender Individuals in Substance Use Treatment. Front. Psychiatry 2023, 14, 1225673. [Google Scholar] [CrossRef] [PubMed]
- Kidd, J.D.; Tettamanti, N.A.; Kaczmarkiewicz, R.; Corbeil, T.E.; Dworkin, J.D.; Jackman, K.B.; Hughes, T.L.; Bockting, W.O.; Meyer, I.H. Prevalence of Substance Use and Mental Health Problems among Transgender and Cisgender U.S. Adults: Results from a National Probability Sample. Psychiatry Res. 2023, 326, 115339. [Google Scholar] [CrossRef] [PubMed]
- Kohnepoushi, P.; Nikouei, M.; Cheraghi, M.; Hasanabadi, P.; Rahmani, H.; Moradi, M.; Moradi, G.; Moradpour, F.; Moradi, Y. Prevalence of Suicidal Thoughts and Attempts in the Transgender Population of the World: A Systematic Review and Meta-Analysis. Ann. Gen. Psychiatry 2023, 22, 28. [Google Scholar] [CrossRef]
- Kattari, S.K.; Kattari, L.; Johnson, I.; Lacombe-Duncan, A.; Misiolek, B.A. Differential Experiences of Mental Health among Trans/Gender Diverse Adults in Michigan. Int. J. Environ. Res. Public Health 2020, 17, 6805. [Google Scholar] [CrossRef]
- Meyer, I.H. Minority Stress and Mental Health in Gay Men. J. Health Soc. Behav. 1995, 36, 38–56. [Google Scholar] [CrossRef]
- Meyer, I.H. Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef]
- Hajek, A.; König, H.-H.; Buczak-Stec, E.; Blessmann, M.; Grupp, K. Prevalence and Determinants of Depressive and Anxiety Symptoms among Transgender People: Results of a Survey. Healthcare 2023, 11, 705. [Google Scholar] [CrossRef]
- Ramos, N.; Marr, M.C. Traumatic Stress and Resilience Among Transgender and Gender Diverse Youth. Child Adolesc. Psychiatr. Clin. N. Am. 2023, 32, 667–682. [Google Scholar] [CrossRef]
- Sherman, A.D.F.; Higgins, M.K.; Balthazar, M.S.; Hill, M.; Klepper, M.; Schneider, J.S.; Adams, D.; Radix, A.; Mayer, K.H.; Cooney, E.E.; et al. Stigma, Social and Structural Vulnerability, and Mental Health among Transgender Women: A Partial Least Square Path Modeling Analysis. J. Nurs. Scholarsh. Off. Publ. Sigma Theta Tau Int. Honor Soc. Nurs. 2024, 56, 42–59. [Google Scholar] [CrossRef]
- Da Silva, S.A.G.; Miranda-Ribeiro, P.; Noronha, K.V.M.d.S.; Guedes, G.R. Exploring the Complexities and Challenges of Healthcare Access for Transgender People in Minas Gerais State: A Qualitative Study a Decade Following the Implementation of the Transsexualization Process in the Brazilian National Health System. Epidemiol. Serviços Saúde 2024, 33, e2024350. [Google Scholar] [CrossRef]
- Castro, M.C.; Massuda, A.; Almeida, G.; Menezes-Filho, N.A.; Andrade, M.V.; de Souza Noronha, K.V.M.; Rocha, R.; Macinko, J.; Hone, T.; Tasca, R.; et al. Brazil’s Unified Health System: The First 30 Years and Prospects for the Future. Lancet 2019, 394, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Bender, M.S.; Paz, I.; Beranger, K.S.; Garcia, E.L. Access Pathways to the Transsexualizing Process in Brazil: A Scoping Review. Epidemiol. Serviços Saúde 2025, 33, e2024311. [Google Scholar] [CrossRef]
- De Lima, R.R.T.; Flor, T.B.M.; Noro, L.R.A. Systematic Review on Health Care for Transvestites and Transsexuals in Brazil. Rev. Saúde Pública 2023, 57, 19. [Google Scholar] [CrossRef]
- Goldsen, K.I.F.; Romanelli, M.; Hoy-Ellis, C.P.; Jung, H. Health, Economic and Social Disparities among Transgender Women, Transgender Men and Transgender Nonbinary Adults: Results from a Population-Based Study. Prev. Med. 2022, 156, 106988. [Google Scholar] [CrossRef]
- Sales, J.M.R.d.; Lopes, G.d.S. Saúde Mental na Comunidade LGBTQIA+: Uma Revisão Narrativa da Literatura. Rev. Contemp. 2023, 3, 30720–30739. [Google Scholar] [CrossRef]
- Silva, L.S.R.d.; Silva, R.d.T.A.e; Moura, D.T.B.d.; Dias, V.D.M.M.; Araújo, N.F.d.; de Alencar, F.S. Cuidados em Saúde Mental da População LGBTQIAPN+ Frente à Assistência à Saúde: Mental health care of the LGBTQIAPN+ population in the face of health care. Cad. Bras. Saúde Ment. J. Ment. Health 2024, 16, 55–77. [Google Scholar]
- Francisco, L.C.F.d.L.; Barros, A.C.; Pacheco, M.D.S.; Nardi, A.E.; Alves, V.d.M. Ansiedade em minorias sexuais e de gênero: Uma revisão integrativa. J. Bras. Psiquiatr. 2020, 69, 48–56. [Google Scholar] [CrossRef]
- Toledo, L.d.S.G.; Palmieri, P.; Ribeiro, G.d.R.; Silva, A.d.; Bastos, F.I. Barriers and Facilitators for HIV Rapid Testing among Transgender Women and Gay and Other Men Who Have Sex with Men in Brazil: A Scoping Review. Glob. Public Health 2024, 19, 2360982. [Google Scholar] [CrossRef]
- Freitas, C.A.M.; Rossi, T.A.; Dourado, I.; Castellanos, M.E.P.; Guimarães, N.S.; Magno, L. Mapping Evidence on Health Promotion in HIV Testing among Men Who Have Sex with Men and Transgender Women Using the Social-Ecological Model and the Vulnerability Theoretical Framework: A Scoping Review. BMC Public Health 2023, 23, 1946. [Google Scholar] [CrossRef]
- Almeida, M.M.d.; Silva, L.A.V.d.; Bastos, F.I.; Guimarães, M.D.C.; Coutinho, C.; de Brito, A.M.; Cavalcante, S.; Dourado, I. Factors Associated with Symptoms of Major Depression Disorder among Transgender Women in Northeast Brazil. PLoS ONE 2022, 17, e0267795. [Google Scholar] [CrossRef] [PubMed]
- De Medeiros, D.S.; Magno, L.; Crosland Guimarães, M.D.; Grangeiro, A.; Filho, M.E.; Soares, F.; Greco, D.; Westin, M.; Ferraz, D.; Zucchi, E.M.; et al. Violence, Discrimination, and High Levels of Symptoms of Depression Among Adolescent Men Who Have Sex with Men and Transgender Women in Brazil. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2023, 73, S19–S25. [Google Scholar] [CrossRef] [PubMed]
- Reis, A.; Sperandei, S.; de Carvalho, P.G.C.; Pinheiro, T.F.; de Moura, F.D.; Gomez, J.L.; Porchat, P.; Bastos, F.I.; McFarland, W.; Wilson, E.C.; et al. A Cross-Sectional Study of Mental Health and Suicidality among Trans Women in São Paulo, Brazil. BMC Psychiatry 2021, 21, 557. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.C.; Salati, L.R.; Villas-Bôas, A.P.; Schwarz, K.; Fontanari, A.M.; Soll, B.; Costa, A.B.; Hirakata, V.; Schneider, M.; Lobato, M.I.R. Factors Associated with Ruminative Thinking in Individuals with Gender Dysphoria. Front. Psychiatry 2021, 12, 602293. [Google Scholar] [CrossRef]
- Sabino, T.E.; Avelino-Silva, V.I.; Cavalcantte, C.; Goulart, S.P.; Luiz, O.C.; Fonseca, L.A.M.; Casseb, J.S. Adherence to Antiretroviral Treatment and Quality of Life among Transgender Women Living with HIV/AIDS in São Paulo, Brazil. AIDS Care 2021, 33, 31–38. [Google Scholar] [CrossRef]
- Rafael, R.d.M.R.; Jalil, E.M.; Luz, P.M.; de Castro, C.R.V.; Wilson, E.C.; Monteiro, L.; Ramos, M.; Moreira, R.I.; Veloso, V.G.; Grinsztejn, B.G.J.; et al. Prevalence and Factors Associated with Suicidal Behavior among Trans Women in Rio de Janeiro, Brazil. PLoS ONE 2021, 16, e0259074. [Google Scholar] [CrossRef]
- Bassichetto, K.C.; Saggese, G.S.R.; Maschião, L.F.; de Carvalho, P.G.C.; Gilmore, H.; Sevelius, J.; Lippman, S.A.; Veras, M.A.d.S.M. Factors Associated with the Retention of Travestis and Transgender Women Living with HIV in a Peer Navigation Intervention in São Paulo, Brazil. Cad. Saude Publica 2023, 39, e00147522. [Google Scholar] [CrossRef]
- Magalhães, L.S.; Dos Santos, K.C.; Diniz E Silva, B.V.; Filho, G.F.S.; Vaddiparti, K.; Gonzalez, R.I.C.; Pillon, S.C.; Carneiro, M.A.D.S.; Caetano, K.A.A.; Cook, R.L.; et al. Alarming Patterns of Moderate and High-Risk Alcohol Use among Transgender Women in Goiás, Central Brazil. Front. Public Health 2024, 12, 1333767. [Google Scholar] [CrossRef]
- da Mota, J.C.; Sperandei, S.; De Boni, R.B.; Dourado, I.; Veras, M.A.d.S.M.; Bastos, F.I. Multiple Substance Use and Associated Factors in Transgender Women and Travestis: Findings from the TransOdara Study, Brazil. Rev. Bras. Epidemiol. Braz. J. Epidemiol. 2024, 27 (Suppl. S1), e240011.supl.1. [Google Scholar] [CrossRef]
- Luz, P.M.; Jalil, E.M.; Castilho, J.; Velasque, L.; Ramos, M.; Ferreira, A.C.G.; Ferreira, A.L.; Wilson, E.C.; Veloso, V.G.; Thombs, B.D.; et al. Association of Discrimination, Violence, and Resilience with Depressive Symptoms Among Transgender Women in Rio de Janeiro, Brazil: A Cross-Sectional Analysis. Transgender Health 2022, 7, 101–106. [Google Scholar] [CrossRef]
- Veras, M.A.d.S.M.; Pinheiro, T.F.; Galan, L.; Magno, L.; Leal, A.F.; Knauth, D.R.; Motta-Castro, A.R.C.; de Queiroz, R.S.B.; Mayaud, P.; McCartney, D.J.; et al. TransOdara Study: The Challenge of Integrating Methods, Settings and Procedures during the COVID-19 Pandemic in Brazil. Rev. Bras. Epidemiol. Braz. J. Epidemiol. 2024, 27 (Suppl. S1), e240002.supl.1. [Google Scholar] [CrossRef]
- Ryngelblum, M.; Grangeiro, A.; Zucchi, E.M.; Couto, M.T.; Dourado, I.; Magno, L.; Tupinambás, U.; Peres, M.F.T. Violence, Discrimination, and Sexual Health Practices among Adolescent Men Who Have Sex with Men, Transgender Women and Travestis in Three Cities in Brazil. Cad. Saúde Pública 2023, 39, e00142922. [Google Scholar] [CrossRef] [PubMed]
- Koreitem, A.; Mocello, A.R.; Gomez, J.L.; Saggese, G.; Neilands, T.; de Sousa Mascena Veras, M.A.; Lippman, S.A.; Sevelius, J. Intersectional Discrimination, Mental Health, and Health Care Access among Transgender Women in Brazil. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2025, 44, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Leite, B.O.; de Medeiros, D.S.; Magno, L.; Bastos, F.I.; Coutinho, C.; de Brito, A.M.; Cavalcante, M.S.; Dourado, I. Association between Gender-Based Discrimination and Medical Visits and HIV Testing in a Large Sample of Transgender Women in Northeast Brazil. Int. J. Equity Health 2021, 20, 199. [Google Scholar] [CrossRef]
- Magno, L.; Leite, B.O.; Sperandei, S.; Pereira, M.; Knauth, D.R.; Leal, A.F.; Veras, M.A.d.S.M.; Dourado, I. Discrimination Based on Gender Identity against Transgender Women and Travestis in Brazil: A Latent Class Analysis and Associated Factors. Rev. Bras. Epidemiol. 2024, 27, e240012.supl.1. [Google Scholar] [CrossRef]
- Depret, D.; Rafael, R.d.M.R.; Acioli, S.; Neto, M.; Velasque, L.d.S.; Knupp, V.M.A.d.O. Relationship between Childhood Abuse and Self-Harm among Transvestites and Transgender Women in Rio de Janeiro State 2019–2020. Epidemiol. Serv. Saude Rev. Sist. Unico Saude Bras. 2025, 33, e2024337. [Google Scholar] [CrossRef]
- de Sousa Mascena Veras, M.A.; Menezes, N.P.; Mocello, A.R.; Leddy, A.M.; Saggese, G.S.R.; Bassichetto, K.C.; Gilmore, H.J.; de Carvalho, P.G.C.; Maschião, L.F.; Neilands, T.B.; et al. Correlation between Gender-Based Violence and Poor Treatment Outcomes among Transgender Women Living with HIV in Brazil. BMC Public Health 2024, 24, 791. [Google Scholar] [CrossRef]
- Costa, M.C.B.; McFarland, W.; Wilson, E.C.; Xie, H.; Arayasirikul, S.; Moura, F.D.; Veras, M.A.S.M. Prevalence and Correlates of Nonprescription Hormone Use Among Trans Women in São Paulo, Brazil. LGBT Health 2021, 8, 162–166. [Google Scholar] [CrossRef]
- Rosário, R.; Dourado, I.; Pereira, M.; Dezanet, L.; Greco, D.; Grangeiro, A.; Magno, L. Factors associated with condomless anal sex among adolescent men who have sex with men and transgender women in three Brazilian state capitals: A PrEP1519 study. Rev. Saude Publica 2024, 58, 8s. [Google Scholar] [CrossRef]
- Leite, B.O.; Magno, L.; Soares, F.; MacCarthy, S.; Brignol, S.; Bastos, F.I.; Dourado, I. HIV Prevalence among Transgender Women in Northeast Brazil—Findings from Two Respondent Driven Sampling Studies. BMC Public Health 2022, 22, 2120. [Google Scholar] [CrossRef]
- Amelia de Sousa Mascena Veras, M.; Roza Saggese, G.S.; Gomez Junior, J.L.; Silveira, P.; Paiatto, B.; Ferreira, D.; Alves de Souza, P.; Calado, R.; Castejon, M.J.; Yamashiro, R.; et al. Brief Report: Young Age and Sex Work Are Associated with HIV Seroconversion Among Transgender Women in São Paulo, Brazil. J. Acquir. Immune Defic. Syndr. 1999 2021, 88, e1–e4. [Google Scholar] [CrossRef] [PubMed]
- Grinsztejn, B.; Jalil, E.M.; Monteiro, L.; Velasque, L.; Moreira, R.I.; Garcia, A.C.F.; Castro, C.V.; Krüger, A.; Luz, P.M.; Liu, A.Y.; et al. Unveiling HIV Dynamics among Transgender Women: A Respondent Driven Sampling Study in Rio de Janeiro, Brazil. Lancet HIV 2017, 4, e169–e176. [Google Scholar] [CrossRef] [PubMed]
- Barros, C.R.D.S.; Matsuda, E.M.; Rocha, A.B.M.d.; López-Lopes, G.I.S.; Campos, N.C.; Brígido, L.F.d.M.; Bassichetto, K.C.; Veras, M.A.d.S.M. Factors Associated with HIV Viremia in Transgender Women and Transvestites in Five Brazilian Capitals, 2019-2021: A Multicenter Study. Epidemiol. Serv. Saude Rev. Sist. Unico Saude Bras. 2024, 33, e2024412. [Google Scholar] [CrossRef]
- Amarante, I.C.J.; Lippman, S.A.; Sevelius, J.M.; Saggese, G.S.R.; da Silva, A.A.M.; Veras, M.A.d.S.M. Anticipated Stigma and Social Barriers to Communication Between Transgender Women Newly Diagnosed with HIV and Health Care Providers: A Mediation Analysis. LGBT Health 2023, 11, 229–238. [Google Scholar] [CrossRef]
- Jalil, E.M.; Torres, T.S.; Luz, P.M.; Monteiro, L.; Moreira, R.I.; de Castro, C.R.V.; Leite, I.d.C.; Cunha, M.; de Cássia Elias Estrela, R.; Ramos, M.; et al. Low PrEP Adherence despite High Retention among Transgender Women in Brazil: The PrEParadas Study. J. Int. AIDS Soc. 2022, 25, e25896. [Google Scholar] [CrossRef]
- Wilson, E.C.; Jalil, E.M.; Moreira, R.I.; Velasque, L.; Castro, C.V.; Monteiro, L.; Veloso, V.G.; Grinsztejn, B. High Risk and Low HIV Prevention Behaviours in a New Generation of Young Trans Women in Brazil. AIDS Care 2021, 33, 997–1001. [Google Scholar] [CrossRef]
- Echeverría-Guevara, A.; Coelho, L.E.; Veloso, V.G.; Pimenta, M.C.; Hoagland, B.; Moreira, R.I.; Leite, I.; Jalil, E.M.; Cardoso, S.W.; Torres, T.S.; et al. Travestis, Transgender Women and Young MSM Are at High Risk for PrEP Early Loss to Follow-up in Rio de Janeiro, Brazil. Braz. J. Infect. Dis. Off. Publ. Braz. Soc. Infect. Dis. 2023, 27, 102733. [Google Scholar] [CrossRef]
- Hintz, A.M.; Gomes-Filho, I.S.; Loomer, P.M.; de Sousa Pinho, P.; de Santana Passos-Soares, J.; Trindade, S.C.; Cerqueira, E.d.M.M.; Alves, C.M.C.; Rios, Y.S.S.; Batista, J.E.T.; et al. Depression and Associated Factors among Brazilian Adults: The 2019 National Healthcare Population-Based Study. BMC Psychiatry 2023, 23, 704. [Google Scholar] [CrossRef]
- WHO. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- da Silva Junior, A.L.S.; Santana, G.M.; Nascimento, M.M.; Cunha, R.L.; Mesquita, P.R.R.; de Jesus, R.M. Illicit Drugs in Brazil: Environmental Consequences and Consumption Patterns. Environ. Sci. Pollut. Res. Int. 2024, 31, 47530–47551. [Google Scholar] [CrossRef]
- Malta, D.C.; Flor, L.S.; Machado, Í.E.; Felisbino-Mendes, M.S.; Brant, L.C.C.; Ribeiro, A.L.P.; Teixeira, R.A.; Macário, E.M.; Reitsma, M.B.; Glenn, S.; et al. Trends in Prevalence and Mortality Burden Attributable to Smoking, Brazil and Federated Units, 1990 and 2017. Popul. Health Metr. 2020, 18, 24. [Google Scholar] [CrossRef]
- da Silva, L.E.S.; Helman, B.; da Luz e Silva, D.C.; de Aquino, É.C.; de Freitas, P.C.; Santos, R.d.O.; Brito, V.C.d.A.; Garcia, L.P.; Sardinha, L.M.V. Prevalence of Heavy Episodic Drinking in the Brazilian Adult Population: National Health Survey 2013 and 2019. Epidemiol. Serviços Saúde Rev. Sist. Unico Saúde Bras. 2022, 31, e2021379. [Google Scholar] [CrossRef]
- Jungerman, F.S.; Menezes, P.R.; Pinsky, I.; Zaleski, M.; Caetano, R.; Laranjeira, R. Prevalence of Cannabis Use in Brazil: Data from the I Brazilian National Alcohol Survey (BNAS). Addict. Behav. 2010, 35, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, R.R.; Madruga, C.S.; Ribeiro, M.; Pinsky, I.; Caetano, R.; Laranjeira, R. Prevalence of Cocaine Use in Brazil: Data from the II Brazilian National Alcohol and Drugs Survey (BNADS). Addict. Behav. 2014, 39, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, T.F.; Carvalho, P.G.C.d.; Nolasco, G.; Santos, L.A.D.; Veras, M.A.d.S.M. Difficulties and Advances in Access to and Use of Health Services by Transgender Women and Travestis in Brazil. Rev. Bras. Epidemiol. Braz. J. Epidemiol. 2024, 27 (Suppl. S1), e240007.supl.1. [Google Scholar] [CrossRef] [PubMed]
- Vermeir, E.; Jackson, L.A.; Marshall, E.G. Improving Healthcare Providers’ Interactions with Trans Patients: Recommendations to Promote Cultural Competence. Healthc. Policy 2018, 14, 11–18. [Google Scholar] [CrossRef]
- Yu, H.; Flores, D.D.; Bonett, S.; Bauermeister, J.A. LGBTQ + Cultural Competency Training for Health Professionals: A Systematic Review. BMC Med. Educ. 2023, 23, 558. [Google Scholar] [CrossRef]
- Coelho, D.R.A.; Chen, A.L.; Keuroghlian, A.S. Advancing Transgender Health amid Rising Policy Threats. N. Engl. J. Med. 2025, 392, 1041–1044. [Google Scholar] [CrossRef]
- Coleman, E.; Radix, A.E.; Bouman, W.P.; Brown, G.R.; de Vries, A.L.C.; Deutsch, M.B.; Ettner, R.; Fraser, L.; Goodman, M.; Green, J.; et al. Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. Int. J. Transgender Health 2022, 23, S1–S259. [Google Scholar] [CrossRef]
- Almazan, A.N.; Keuroghlian, A.S. Association Between Gender-Affirming Surgeries and Mental Health Outcomes. JAMA Surg. 2021, 156, 611–618. [Google Scholar] [CrossRef]
- Simpson, K.; Benevides, B. 20 Years of Trans Visibility, from Mourning to Fighting! Epidemiol. Serv. Saude Rev. Sist. Unico Saude Bras. 2024, 33, e2024034. [Google Scholar] [CrossRef]
- Ferreira, L.C. Brazilian Medical Entities Criticize Veto on Trans Youth Therapies. Brasil de Fato. 28 April 2025. Available online: https://www.brasildefato.com.br/2025/04/28/brazilian-medical-entities-criticize-veto-on-trans-youth-therapies/ (accessed on 8 June 2025).
- Fleury, F.M. Estado, direito, transfobia e cissexismo no Brasil. Rev. Videre 2021, 13. [Google Scholar] [CrossRef]
- Borges Romeiro Caetano, B.; Dias Oliveira, D.; Schaffer Ramos, T.; Serra Bavaresco, C.; Luiz Stefanello Busato, A.; Itzel Acosta Moreno Vinholes, J.; Renato Reis de Moura, F. LGBTQIA+ vs. the Brazilian Unified Health System: Basic Health Unit Use and Associated Factors. J. Homosex. 2024, 71, 3362–3380. [Google Scholar] [CrossRef] [PubMed]
- Malta, M.; da Silva, A.B.; da Silva, C.M.F.; LeGrand, S.; Seixas, M.; Benevides, B.; Kalume, C.; Whetten, K. Addressing discrimination and violence against Lesbian, Gay, Bisexual, Transgender, and Queer (LGBTQ) persons from Brazil: A mobile health intervention. BMC Public Health 2023, 23, 2069. [Google Scholar] [CrossRef] [PubMed]
- Benfeitoria. PreparaNem—CasaNem. Benfeitoria, Rio de Janeiro, Brazil. Available online: https://benfeitoria.com/projeto/PreparaNem (accessed on 19 April 2025).
- Cruz, E.P. Unicamp Aprova Cotas Para Pessoas Trans, Travestis ou Não Binárias [Unicamp Approves Quotas for Trans, Travesti, or Nonbinary People]. Agência Brasil. 2 April 2025. Available online: https://agenciabrasil.ebc.com.br/educacao/noticia/2025-04/unicamp-aprova-cotas-para-pessoas-trans-travestis-ou-nao-binarias (accessed on 19 April 2025).
- TransEmpregos. TransEmpregos Platform. TransEmpregos, São Paulo, Brazil. Available online: https://www.transempregos.com.br (accessed on 19 April 2025).
- Grangeiro, A.; Ferraz, D.; Magno, L.; Zucchi, E.M.; Couto, M.T.; Dourado, I. Forty Years of the Brazilian Response to HIV: Reflections on the Need for a Programmatic Shift and Policy as a Common Good. Cad. Saúde Pública 2023, 39, e00199423. [Google Scholar] [CrossRef]
- Stutterheim, S.E.; van Dijk, M.; Wang, H.; Jonas, K.J. The Worldwide Burden of HIV in Transgender Individuals: An Updated Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0260063. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Author (Year) | City (s) | Sample Size | Main Findings |
|---|---|---|---|
| Almeida et al. (2022) [33] | Fortaleza | 864 | Symptoms of major depressive disorder (70.1%) |
| Recife | |||
| Salvador | |||
| Bassichetto et al. (2023) [39] | São Paulo | 113 | Alcohol use any (72.5%) |
| Illicit substance use (66.4%) | |||
| Suicide attempt (39.8%) | |||
| Ferreira et al. (2019) [12] | Rio de Janeiro | 322 | Depressive symptoms (57.8%) |
| Problematic use of tobacco (56.6%) | |||
| Problematic use of cannabis (28.9%) | |||
| Problematic use of cocaine (23.8%) | |||
| Problematic use of alcohol (21.5%) | |||
| Magalhães et al. (2024) [40] | Goiânia | 440 | Marijuana (68.9%) |
| Itumbiara | Cocaine/crack (59.8%) | ||
| Jataí | Tobacco (59.8%) | ||
| Binge drinking (56.6%) | |||
| Medeiros et al. (2023) [34] | Belo Horizonte | 56 | Overall depressive symptoms (69.6%) |
| Salvador | Severe depressive symptoms (44.6%) | ||
| São Paulo | Mild/moderate depressive symptoms (25%) | ||
| Mota et al. (2024) [41] | Campo Grande | 1317 | Alcohol (65.5%) |
| Manaus | Tobacco (61.6%) | ||
| Marijuana (52%) | |||
| Porto Alegre | Cocaine (42.6%) | ||
| Inhalants (14.6%) | |||
| Salvador | Crack (13.9%) | ||
| Amphetamines/ecstasy (11.8%) | |||
| São Paulo | Other substances, including hypnotics, hallucinogens, and opioids (1.3–13.1%) | ||
| Rafael et al. (2021) [38] | Rio de Janeiro | 345 | Suicidal ideation (47.25%) |
| Suicide attempt (27.25%) | |||
| Reis et al. (2021) [35] | São Paulo | 763 | Alcohol use in the past year (72.7%) |
| Cannabis use in the past year (46.8%) | |||
| Stimulant drug use in the past year (44.4%) | |||
| Suicide attempt (31.2%) | |||
| Anxiety (26.5%) | |||
| Suicidal ideation (25%) | |||
| Depression (19.1%) | |||
| Sabino et al. (2021) [37] | São Paulo | 106 | Any illicit/recreational drugs use (46%) |
| Alcohol use (30%) | |||
| Marijuana (19%) | |||
| Cocaine (15%) | |||
| Depression (16%) | |||
| Crack (6%) | |||
| Silva et al. (2021) [36] | Porto Alegre | 111 | Suicidal ideation (46.4%) |
| Suicide attempt (31.2%) | |||
| Anxiety symptoms (24.8%) | |||
| Depressive symptoms (16.6%) |
| Author (Year) | City (s) | Sample Size | Factor (s) | Main Findings |
|---|---|---|---|---|
| Amarante et al. (2023) [56] | São Paulo | 113 | HIV and health disparities | Fear of public mistreatment was associated with increased difficulty reporting new symptoms to healthcare providers (aOR = 7.42; 95% CI: 1.93–28.5) |
| Almeida et al. (2022) [33] | Fortaleza | 864 | Physical and sexual violence | Sexual (OR = 2.06; 95% CI: 1.15–3.68) and physical violence (OR = 2.09; 95% CI: 1.20–3.67) were associated with increased mild/moderate symptoms of major depressive disorder |
| Recife | ||||
| Barros et al. (2024) [55] | Campo Grande | 425 | HIV and health disparities | 42% had detectable viral load; associated with poor mental health (PR = 1.70; 95% CI: 1.08–2.66), poor housing (PR = 2.72; 95% CI: 1.30–5.68), and younger age (PR = 2.26; 95%CI: 1.13–4.51) |
| Manaus | ||||
| Porto Alegre | ||||
| Salvador | ||||
| São Paulo | ||||
| Bassichetto et al. (2023) [39] | São Paulo | 113 | Sexual violence | 45.1% had suffered sexual violence |
| Cesar et al. (2024) [9] | Campo Grande | 152 | HIV and health disparities | 24% were living with HIV |
| Costa et al. (2021) [50] | São Paulo | 790 | Health disparities | 36.8% used nonprescribed hormones; use was higher among young travestis and transgender women 18–25 (49.1%) |
| Depret et al. (2025) [48] | Rio de Janeiro | 139 | Psychological violence | Emotional abuse in childhood was associated with suicide attempts (OR = 9.00; 95% CI: 1.13–71.34), and emotional neglect in childhood was associated with self-injury behaviors (OR = 11.64; 95% CI: 2.35–57.5) |
| Dourado et al. (2024) [11] | Campo Grande | 1317 | HIV and health disparities | 34% were living with HIV |
| Manaus | ||||
| Porto Alegre | ||||
| Salvador | ||||
| São Paulo | ||||
| Echeverría-Guevara et al. (2023) [59] | Rio de Janeiro | 1463 | HIV and health disparities | Travestis and transgender women had significantly higher odds of early loss to follow-up for PrEP (aOR 2.8; 95% CI: 1.6–4.8) |
| Ferreira et al. (2019) [12] | Rio de Janeiro | 322 | Economic difficulties | 78.6% were current or past sex workers, and 62% earned below USD 10/day |
| HIV and health disparities | 54% were living with HIV | |||
| Grinsztejn et al. (2017) [54] | Rio de Janeiro | 345 | HIV and health disparities | Newly diagnosed cases of HIV were associated with a history of sex work (OR = 30.7; 95% CI: 3.5–267.3) |
| Koreitem et al. (2025) [45] | São Paulo | 392 | Discrimination | Higher anticipated discrimination was associated with psychological distress (aOR = 2.13; 95% CI: 1.57–2.89) and suicidality (aOR = 1.44; 95% CI: 1.08–1.93) |
| Jalil et al. (2022) [57] | Rio de Janeiro | 130 | HIV and health disparities | Only 48.6% had high PrEP adherence; missed visits were associated with younger age (18–24 years) (aOR = 8.76; 95% CI: 2.09–36.7) and stimulant use (aOR = 4.99; 95% CI: 1.37–18.1) |
| Leite et al. (2021) [46] | Fortaleza | 864 | Discrimination | Discrimination was associated with a reduced likelihood of medical visits (OR = 0.29; 95% CI: 0.14–0.63) and HIV testing (OR = 0.41; 95% CI: 0.22–0.78) |
| Recife | ||||
| Salvador | ||||
| Leite et al. (2022) [52] | Salvador | 127 and 166 (Two studies) | HIV and health disparities | HIV prevalence ranged from 9% to 24.3%, respectively, and gender-based discrimination was associated with testing positive for HIV (OR = 8.65; 95% CI: 1.45–51.59) |
| Leite (2024) [10] | FortalezaRecifeSalvador | 864 | HIV and health disparities | 24.5% were living with HIV |
| Luz et al. (2022) [42] | Rio de Janeiro | 489 | Discrimination | 96% had suffered discrimination |
| Physical violence | 52% had suffered physical violence | |||
| Sexual violence | 42% had suffered sexual violence | |||
| Magno et al. (2024) [47] | Campo Grande | 1317 | Sexual violence | 51% had suffered sexual violence |
| Manaus | ||||
| Porto Alegre | Physical violence | 14.2% had suffered physical violence | ||
| Salvador | ||||
| São Paulo | ||||
| Rafael et al. (2021) [38] | Rio de Janeiro | 345 | Physical violence | Physical violence was associated with increased suicidal ideation (aPR = 1.37; 95% CI: 1.09–1.71) and suicide attempt (aPR = 1.92; 95% CI: 1.28–2.88) |
| Reis et al. (2021) [35] | São Paulo | 763 | Sexual violence | Sexual violence was associated with increased suicidal ideation and suicide attempt (OR = 1.69; 95% CI: 1.18–2.44) |
| Rosário et al. (2024) [51] | Belo Horizonte | 121 | HIV and health disparities | 79.3% of travestis and transgender women aged 15–19 reported condomless anal sex in the past 6 months |
| Salvador | ||||
| São Paulo | ||||
| Ryngelblum et al. (2023) [44] | Belo Horizonte | 72 | Discrimination | 50% had suffered discrimination six times or more |
| Salvador | Sexual violence | 45% had suffered sexual violence | ||
| São Paulo | ||||
| Veras et al. (2021) [50] | São Paulo | 545 | HIV and health disparities | Higher prevalence of HIV among travestis and transgender women aged 18–24 (RR = 3.85; 95% CI: 1.24–12.93) and those who engaged in sex work in the last month (RR = 5.90; 95% CI: 1.71–26.62) |
| Veras et al. (2024) [55] | São Paulo | 113 | Physical and sexual violence | 62% and 45% had suffered physical and sexual violence, respectively, and lifetime sexual violence was associated with a 56% reduction in viral suppression (aRR = 0.44; 95% CI: 0.24–0.79) |
| Veras et al. (2024) [43] | Campo Grande | 1317 | Discrimination | 85% reported experiencing discrimination |
| Manaus | ||||
| Porto Alegre | ||||
| Salvador | Economic difficulties | 57% earned ≤ 1 minimum wage and 21.3% reported sex work as main income source | ||
| São Paulo | ||||
| Wilson et al. (2021) [58] | Rio de Janeiro | 345 | HIV and health disparities | Younger ages (18–24 years) were associated with lower odds of PrEP awareness (OR = 0.5; 95% CI: 0.3–0.8) and PEP knowledge (OR = 0.5; 95% CI: 0.3–0.9), as well as higher odds of at-risk substance use (OR = 1.8; 95% CI: 1.1–2.9) and unprotected sex (OR = 1.8; 95% CI: 1.1–3.0) |
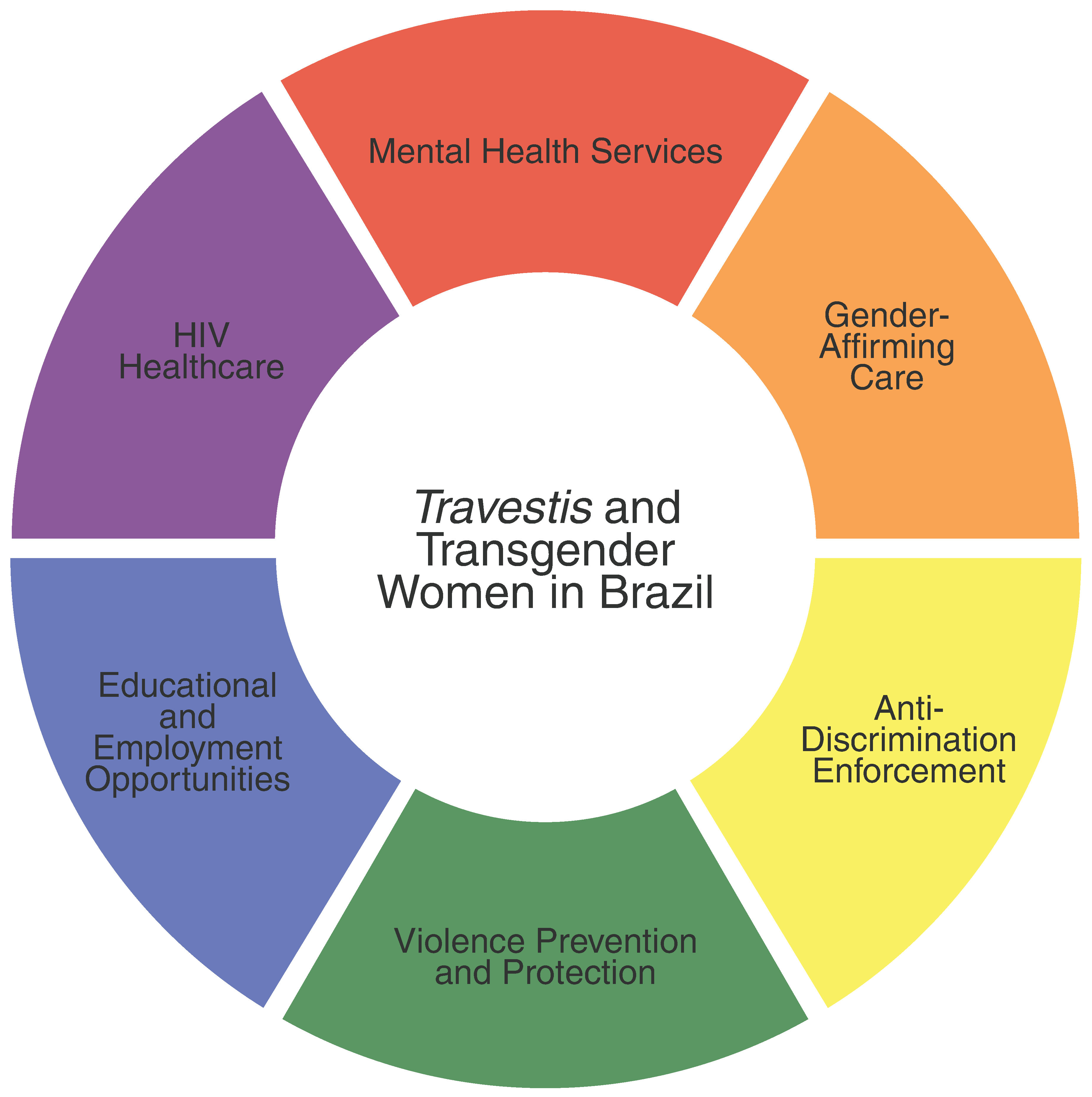
| Policy Area | Recommendations | Key Stakeholders |
|---|---|---|
| Mental health services | Expand mental health services, including psychotherapy, within centers offering gender-affirming care, HIV prevention and care, and primary care settings. Strengthen referral pathways in SUS to improve access, especially in remote areas. Prioritize provider training and sensitization to enhance trust and care navigation for transgender, nonbinary, and gender diverse people. | SUS, Ministry of Health, healthcare professionals, professional medical associations, local governments, and advocacy groups. |
| Gender-affirming care | Integrate gender-affirming care into SUS primary care settings and promote continuous training for healthcare professionals in LGBTQIA+ care. | SUS, Ministry of Health, healthcare professionals, professional medical associations, medical education institutions, local governments, and advocacy groups. |
| Discrimination | Enforce anti-discrimination laws and policies to protect transgender, nonbinary, and gender diverse people in healthcare, education, and employment. Develop and promote public awareness campaigns to combat stigma and discrimination against transgender, nonbinary, and gender diverse people. | Ministry of Justice and Public Security, SUS, Ministry of Health, Ministry of Education, Ministry of Labour and Employment, local governments, and advocacy groups. |
| Violence | Promote the Dandarah app and other initiatives aimed at enhancing safety and providing avenues for reporting incidents. Strengthen law enforcement training on LGBTQIA+ issues to ensure proper handling of cases involving transgender, nonbinary, and gender diverse people. | Ministry of Justice and Public Security, SUS, Ministry of Health, technology developers, law enforcement, social media platforms, local governments, and advocacy groups. |
| Educational opportunities | Establish affirmative policies across all levels of education, from primary schools to universities, to support transgender, nonbinary, and gender diverse students. Expand initiatives such as PreparaNem and other preparatory programs. Integrate LGBTQIA+ awareness into school curriculums to reduce stigma and promote inclusion. | Ministry of Education, universities, schools, NGOs, local governments, and advocacy groups. |
| Employment opportunities | Develop job training programs and enhance NGO initiatives like TransEmpregos to foster economic empowerment. Implement anti-discrimination policies in workplaces. | Ministry of Labour and Employment, Employment agencies, private sector, labor unions, educational institutions, NGOs, local governments, and advocacy groups. |
| HIV healthcare | Expand the use of PrEP and PEP, particularly among younger travestis and transgender women and those engaged in sex work. Maintain high rates of ART adherence while providing mental health support for those living with HIV. Integrate HIV healthcare with mental health services and substance use screening with a harm reduction approach. | SUS, Ministry of Health, healthcare professionals, community health workers, local governments, and advocacy groups. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coelho, D.R.A.; Ferreira, A.L.N.; Vieira, W.F.; Keuroghlian, A.S.; Reisner, S.L. Mental Health Outcomes Among Travestis and Transgender Women in Brazil: A Literature Review and a Call to Action for Public Health Policies. Int. J. Environ. Res. Public Health 2025, 22, 977. https://doi.org/10.3390/ijerph22070977
Coelho DRA, Ferreira ALN, Vieira WF, Keuroghlian AS, Reisner SL. Mental Health Outcomes Among Travestis and Transgender Women in Brazil: A Literature Review and a Call to Action for Public Health Policies. International Journal of Environmental Research and Public Health. 2025; 22(7):977. https://doi.org/10.3390/ijerph22070977
Chicago/Turabian StyleCoelho, David R. A., Ana Luiza N. Ferreira, Willians Fernando Vieira, Alex S. Keuroghlian, and Sari L. Reisner. 2025. "Mental Health Outcomes Among Travestis and Transgender Women in Brazil: A Literature Review and a Call to Action for Public Health Policies" International Journal of Environmental Research and Public Health 22, no. 7: 977. https://doi.org/10.3390/ijerph22070977
APA StyleCoelho, D. R. A., Ferreira, A. L. N., Vieira, W. F., Keuroghlian, A. S., & Reisner, S. L. (2025). Mental Health Outcomes Among Travestis and Transgender Women in Brazil: A Literature Review and a Call to Action for Public Health Policies. International Journal of Environmental Research and Public Health, 22(7), 977. https://doi.org/10.3390/ijerph22070977