
Exploration of Providers’ Perceptions and Attitudes Toward Phage Therapy and Intentions for Future Adoption as an Alternative to Traditional Antibiotics in the US—A Cross-Sectional Study


Abstract

1. Introduction
- What is the present understanding and level of concern among healthcare providers regarding antibiotic resistance?
- If phage therapy were to become available in the United States, how receptive would providers be to its adoption?
- Does a provider’s likelihood of considering phage therapy correlate with specific demographic characteristics, knowledge levels, or intention-related factors?
2. Materials and Methods
2.1. Survey Design, Instrument, Inclusion Criteria, and Ethics
- Part I: Demographic questions included variables such as age, gender, race, ethnicity, employment status, political affiliation, and marital status.
- Part II: Profession-related questions inquired about the zip code of respondents’ current practice, the professional degree obtained (e.g., M.D., D.O.), the location of practice, and the year of licensure attainment.
- Part III: Questions evaluated knowledge of phage therapy and the respondents’ willingness to adopt phage therapy in the future.
2.2. Statistical Analysis
2.3. Human Subjects Protection
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Questionnaire
- I. Demographics
- What is your age in years?
- _____________(years)
- 2.
- What is your gender identity
- ○
- Male
- ○
- Female
- ○
- Transgender man
- ○
- Transgender women
- ○
- Gender non-conforming
- ○
- Intersex
- ○
- Other
- ○
- Prefer not to answer
- 3.
- Race
- ○
- White/Caucasian
- ○
- Black or African American
- ○
- Middle Eastern or North African
- ○
- Native American, American Indian, or Alaskan Native
- ○
- Asian
- ○
- Native Hawaiian or Pacific Islander
- ○
- Two or more races
- ○
- Other/Unknown
- ○
- Prefer not to answer
- 4.
- Ethnicity
- ○
- Hispanic or Latino
- ○
- Non-Hispanic or Latino
- 5.
- What is your employment status?
- ○
- Employed full-time
- ○
- Employed part-time
- ○
- Retried
- 6.
- What is your political affiliation?
- ○
- Very conservative
- ○
- Moderately conservative
- ○
- Lightly conservative
- ○
- Neutral
- ○
- Lightly liberal
- ○
- Moderately liberal
- ○
- Very liberal
- ○
- Prefer not to answer
- 7.
- What is your marital status?
- ○
- Married
- ○
- Marries, but not cohabitating
- ○
- Not married, but cohabiting
- ○
- Not married or cohabitating
- II. Profession-related questions
- 8.
- What is your zip code of practice?
- __________________________________
- 9.
- What is your professional degree?
- ○
- Doctor of Medicine (MD)
- ○
- Doctor of Osteopathic Medicine (DO)
- ○
- Podiatrist (DPM)
- ○
- Licensed Nurse Practitioner (LNP)
- ○
- Other_________________
- 10.
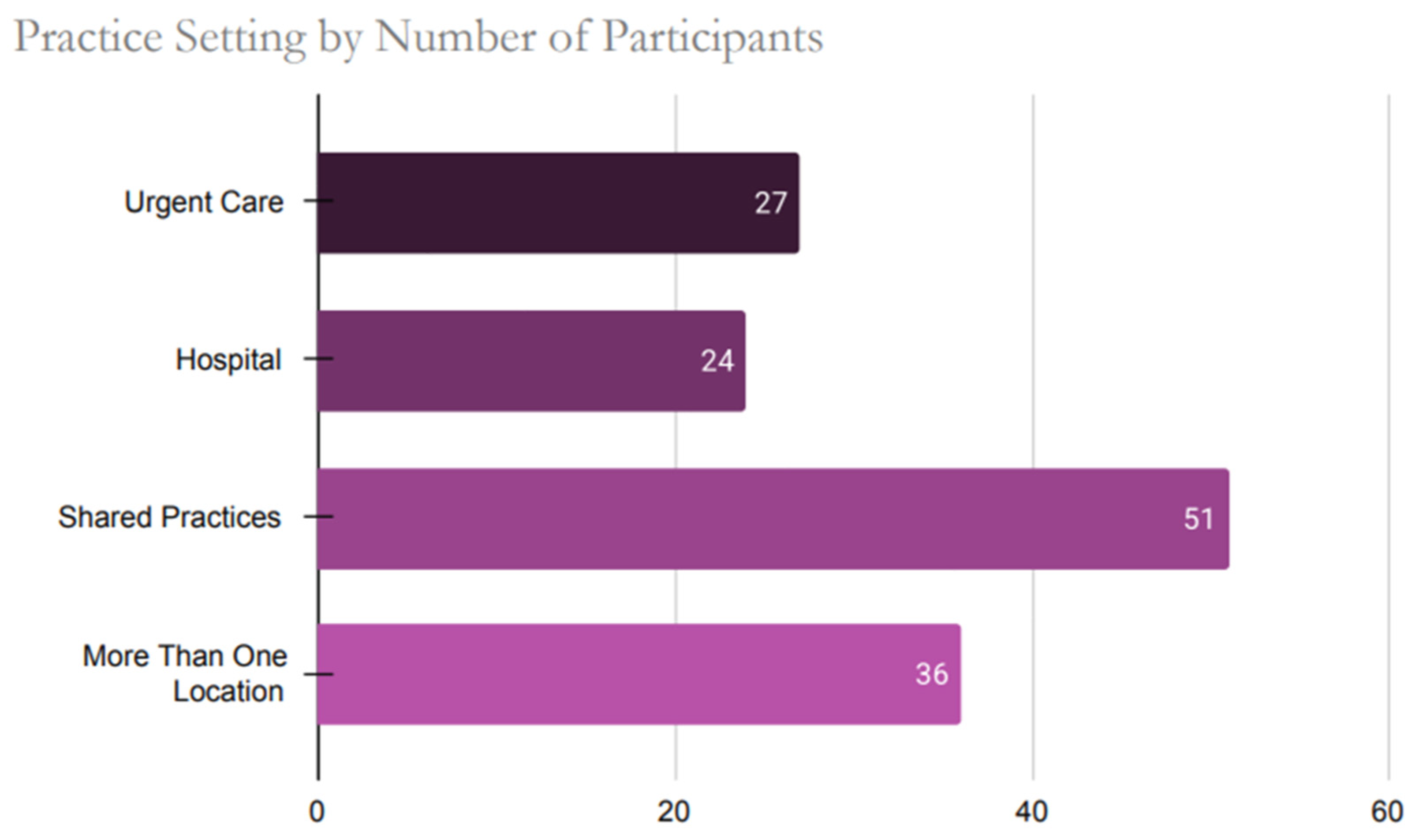
- What is your primary location of practice? Select those that apply.
- ○
- Hospital
- ○
- Private practice/clinic
- ○
- Urgent care clinic
- ○
- Hospice
- ○
- Ambulatory surgical center
- ○
- Group practice
- ○
- Skilled nursing home
- ○
- Nursing home
- ○
- Home health
- ○
- Other (please explain) ________________________
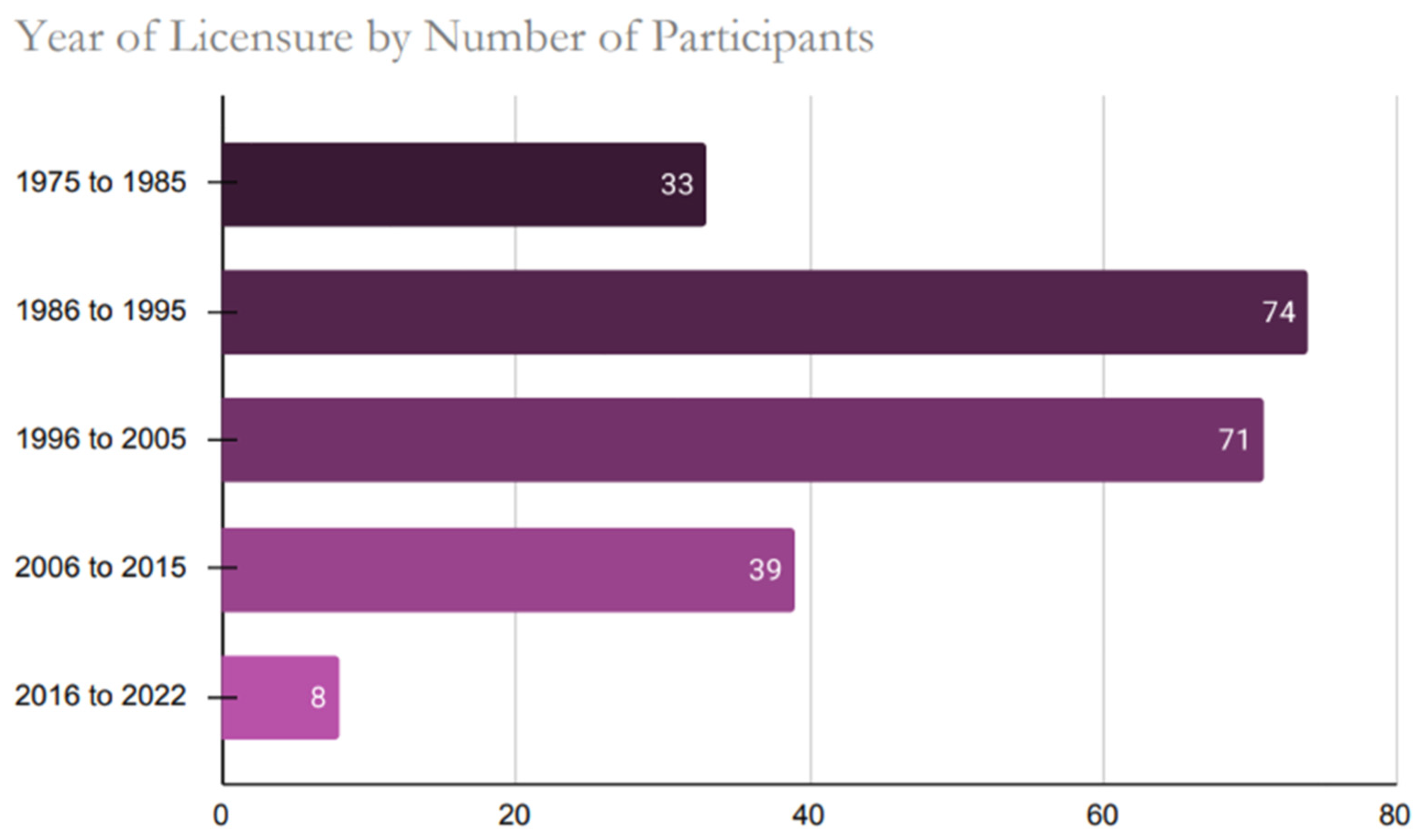
- 11.
- In which year did you achieve a license or licensure to practice medicine (Example—1970, 1985)?
- ______________
- III. Antibiotic Resistance and Phage-related Questions
- 12.
- Have you heard of the term “antibiotic resistance” before this survey?
- ○
- Yes
- ○
- No
- 13.
- How concerned are you about the current state of antibiotic resistance and its public health burden in the US?
- ○
- Not concerned
- ○
- Slightly concerned
- ○
- Moderately concerned
- ○
- Extremely concerned
- 14.
- How important do you feel about finding an alternative therapy option for treating antibiotic-resistant bacteria (ARB) in the US?
- ○
- Very Important
- ○
- Important
- ○
- Moderately Important
- ○
- Slightly Important
- ○
- Not Important
- 15.
- Have you heard of “bacteriophage therapy” or “phage therapy” as an alternative method to treat resistant bacterial infections in animals and/or humans?
- ○
- Yes
- ○
- No
- ○
- Not sure
- 16.
- Where did you learn about “bacteriophage therapy” or “phage therapy”?
- ○
- Professional school
- ○
- Conference
- ○
- Clinical Practice
- ○
- Other (please explain) ________________________
- 17.
- Will your patients accept “bacteriophage therapy” or “phage therapy” if you recommend them as an alternative therapy to treat their resistant bacterial conditions?
- ○
- Very likely
- ○
- Likely
- ○
- Somewhat
- ○
- Not at all
- 18.
- I am willing to treat patients with “bacteriophage therapy” or “phage therapy” instead of traditional antibiotics when necessary, in the future.
- ○
- Yes
- ○
- No
- ○
- Not sure
- 19.
- I am willing to learn more about “bacteriophage therapy” or “phage therapy” in the near future for consideration as an alternative therapy in my practice.
- ○
- Very likely
- ○
- Likely
- ○
- Somewhat
- ○
- Not at all
- 20.
- I am already using “bacteriophage therapy” or “phage therapy” in my clinical practice.
- ○
- Yes
- ○
- No
- ○
- Not sure
- Thank you for your participation in this survey!
Appendix B
Appendix B.1


References
- Murray, C.J.L.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- CDC. What Exactly Is Antibiotic Resistance? Available online: https://www.cdc.gov/antimicrobial-resistance/about/?CDC_AAref_Val=https://www.cdc.gov/drugresistance/about.html (accessed on 2 December 2023).
- Antimicrobial Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 2 December 2023).
- Salam, M.A.; Al-Amin, M.Y.; Salam, M.T.; Pawar, J.S.; Akhter, N.; Rabaan, A.A.; Alqumber, M.A.A. Antimicrobial Resistance: A Growing Serious Threat for Global Public Health. Healthcare 2023, 11, 1946. [Google Scholar] [CrossRef] [PubMed]
- Antibiotic Resistance Threats in the United States, 2019; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019.
- Martens, E.; Demain, A.L. The Antibiotic Resistance Crisis, with a Focus on the United States. J. Antibiot. 2017, 70, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Ventola, C.L. The Antibiotic Resistance Crisis: Part 1: Causes and Threats. P T Peer-Rev. J. Formul. Manag. 2015, 40, 277–283. [Google Scholar]
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial Resistance: A Global Multifaceted Phenomenon. Pathog. Glob. Health 2015, 109, 309–318. [Google Scholar] [CrossRef] [PubMed]
- CDC. Antimicrobial Resistance. Available online: https://www.cdc.gov/drugresistance/index.html (accessed on 4 July 2025).
- Available online: https://www.gao.gov/assets/820/819518.pdf (accessed on 4 July 2025).
- CDC. Others Antibiotic Resistance Threats in the United States; US Department of Health and Human Services: Washington, DC, USA, 2019.
- Kline, A.; Cobián Güemes, A.G.; Yore, J.; Ghose, C.; Van Tyne, D.; Whiteson, K.; Pride, D.T. Current Clinical Laboratory Challenges to Widespread Adoption of Phage Therapy in the United States. Antibiotics 2025, 14, 553. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Lack of New Antibiotics Threatens Global Efforts to Contain Drug-Resistant Infections. New Release Geneva, 17 January 2020. [Google Scholar]
- Markovskaya, Y.; Gavioli, E.M.; Cusumano, J.A.; Glatt, A.E. Coronavirus Disease 2019 (COVID-19): Secondary Bacterial Infections and the Impact on Antimicrobial Resistance during the COVID-19 Pandemic. Antimicrob. Steward. Healthc. Epidemiol. 2022, 2, e114. [Google Scholar] [CrossRef] [PubMed]
- Abedon, S.T.; García, P.; Mullany, P.; Aminov, R. Editorial: Phage Therapy: Past, Present and Future. Front. Microbiol. 2017, 8, 981. [Google Scholar] [CrossRef] [PubMed]
- Hatfull, G.F.; Dedrick, R.M.; Schooley, R.T. Phage Therapy for Antibiotic-Resistant Bacterial Infections. Annu. Rev. Med. 2022, 73, 197–211. [Google Scholar] [CrossRef] [PubMed]
- Fabijan, A.P.; Iredell, J.; Danis-Wlodarczyk, K.; Kebriaei, R.; Abedon, S.T. Translating Phage Therapy into the Clinic: Recent Accomplishments but Continuing Challenges. PLoS Biol. 2023, 21, e3002119. [Google Scholar] [CrossRef]
- Simpson, E.A.; Stacey, H.J.; Langley, R.J.; Jones, J.D. Phage Therapy: Awareness and Demand among Clinicians in the United Kingdom. PLoS ONE 2023, 18, e0294190. [Google Scholar] [CrossRef] [PubMed]
- Altamirano, F.L.G.; Barr, J.J. Phage Therapy in the Postantibiotic Era. Clin. Microbiol. Rev. 2019, 32, e00066-18. [Google Scholar] [CrossRef] [PubMed]
- Suh, G.A.; Lodise, T.P.; Tamma, P.D.; Knisely, J.M.; Alexander, J.; Aslam, S.; Barton, K.D.; Bizzell, E.; Totten, K.M.C.; Campbell, J.L.; et al. Considerations for the Use of Phage Therapy in Clinical Practice. Antimicrob. Agents Chemother. 2022, 66, e0207121. [Google Scholar] [CrossRef] [PubMed]
- Strathdee, S.A.; Hatfull, G.F.; Mutalik, V.K.; Schooley, R.T. Phage Therapy: From Biological Mechanisms to Future Directions. Cell 2023, 186, 17–31. [Google Scholar] [CrossRef] [PubMed]
- d’Hérelle, F. Sur un microbe invisible antagoniste des bacilles dysentériques. Comptes Rendus Hebd. Séances Acad. Sci. 1917, 165, 373–375. [Google Scholar]
- Twort, F.W. Further Investigations on the Nature of Ultra-Microscopic Viruses and Their Cultivation. J. Hyg. 1936, 36, 204–235. [Google Scholar] [CrossRef] [PubMed]
- McCallin, S.; Sacher, J.C.; Zheng, J.; Chan, B.K. Current State of Compassionate Phage Therapy. Viruses 2019, 11, 343. [Google Scholar] [CrossRef] [PubMed]
- Abedon, S.T.; Danis-Wlodarczyk, K.M.; Alves, D.R. Phage Therapy in the 21st Century: Is There Modern, Clinical Evidence of Phage-Mediated Efficacy? Pharmaceuticals 2021, 14, 1157. [Google Scholar] [CrossRef] [PubMed]
- Schooley, R.T.; Biswas, B.; Gill, J.J.; Hernandez-Morales, A.; Lancaster, J.; Lessor, L.; Barr, J.J.; Reed, S.L.; Rohwer, F.; Benler, S.; et al. Development and Use of Personalized Bacteriophage-Based Therapeutic Cocktails to Treat a Patient with a Disseminated Resistant Acinetobacter Baumannii Infection. Antimicrob. Agents Chemother. 2017, 61, e00954-17. [Google Scholar] [CrossRef] [PubMed]
- Rimon, A.; Gelman, D.; Yerushalmy, O.; Coppenhagen-Glazer, S.; Katvan, E.; Nir-Paz, R.; Hazan, R. Phage Therapy in Israel, Past, Present, and Future. Phage 2022, 3, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Chanishvili, N. Chapter 1—Phage Therapy-History from Twort and d’Herelle Through Soviet Experience to Current Approaches. In Advances in Virus Research; Łobocka, M., Szybalski, W., Eds.; Academic Press: New York, NY, USA, 2012; Volume 83, pp. 3–40. [Google Scholar]
- Kutateladze, M.; Adamia, R. Bacteriophages as Potential New Therapeutics to Replace or Supplement Antibiotics. Trends Biotechnol. 2010, 28, 591–595. [Google Scholar] [CrossRef] [PubMed]
- Weber-Dąbrowska, B.; Mulczyk, M.; Górski, A. Bacteriophage Therapy of Bacterial Infections: An Update of Our Institute’s Experience. In Inflammation; Springer: Dordrecht, The Netherlands, 2001; pp. 201–209. [Google Scholar]
- Międzybrodzki, R.; Borysowski, J.; Weber-Dąbrowska, B.; Fortuna, W.; Letkiewicz, S.; Szufnarowski, K.; Pawełczyk, Z.; Rogóż, P.; Kłak, M.; Wojtasik, E.; et al. Clinical Aspects of Phage Therapy. Adv. Virus Res. 2012, 83, 73–121. [Google Scholar] [CrossRef] [PubMed]
- Terwilliger, A.L.; Liu, C.G.; Green, S.I.; Clark, J.R.; Salazar, K.C.; Hernandez Santos, H.; Heckmann, E.R.; Trautner, B.W.; Ramig, R.F.; Maresso, A.W. Tailored Antibacterials and Innovative Laboratories for Phage (Φ) Research: Personalized Infectious Disease Medicine for the Most Vulnerable at-Risk Patients. Phage 2020, 1, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Le, T.; Nang, S.C.; Zhao, J.; Yu, H.H.; Li, J.; Gill, J.J.; Liu, M.; Aslam, S. Therapeutic Potential of Intravenous Phage as Standalone Therapy for Recurrent Drug-Resistant Urinary Tract Infections. Antimicrob. Agents Chemother. 2023, 67, e0003723. [Google Scholar] [CrossRef] [PubMed]
- Kortright, K.E.; Chan, B.K.; Koff, J.L.; Turner, P.E. Phage Therapy: A Renewed Approach to Combat Antibiotic-Resistant Bacteria. Cell Host Microbe 2019, 25, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Nagel, T.; Musila, L.; Muthoni, M.; Nikolich, M.; Nakavuma, J.L.; Clokie, M.R. Phage Banks as Potential Tools to Rapidly and Cost-Effectively Manage Antimicrobial Resistance in the Developing World. Curr. Opin. Virol. 2022, 53, 101208. [Google Scholar] [CrossRef] [PubMed]
- Dedrick, R.M.; Guerrero-Bustamante, C.A.; Garlena, R.A.; Russell, D.A.; Ford, K.; Harris, K.; Gilmour, K.C.; Soothill, J.; Jacobs-Sera, D.; Schooley, R.T.; et al. Engineered Bacteriophages for Treatment of a Patient with a Disseminated Drug-Resistant Mycobacterium Abscessus. Nat. Med. 2019, 25, 730–733. [Google Scholar] [CrossRef] [PubMed]
- Viertel, T.M.; Ritter, K.; Horz, H.-P. Viruses versus Bacteria-Novel Approaches to Phage Therapy as a Tool against Multidrug-Resistant Pathogens. J. Antimicrob. Chemother. 2014, 69, 2326–2336. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.M. Antimicrobial Stewardship Programs: Appropriate Measures and Metrics to Study Their Impact. Curr. Treat. Options Infect. Dis. 2014, 6, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Cunha, C.B.; Cunha, B.A. Infectious Diseases and Antimicrobial Stewardship in Critical Care Medicine; CRC Press: Boca Raton, FL, USA, 2020; ISBN 9781351583381. [Google Scholar]
- Charani, E.; Castro-Sanchez, E.; Sevdalis, N.; Kyratsis, Y.; Drumright, L.; Shah, N.; Holmes, A. Understanding the Determinants of Antimicrobial Prescribing within Hospitals: The Role of “Prescribing Etiquette”. Clin. Infect. Dis. 2013, 57, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, G.V.; Fleming-Dutra, K.E.; Roberts, R.M.; Hicks, L.A. Core Elements of Outpatient Antibiotic Stewardship. MMWR. Recomm. Rep. 2016, 65, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Pulcini, C.; Gyssens, I.C. How to Educate Prescribers in Antimicrobial Stewardship Practices. Virulence 2013, 4, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Voelker, R. FDA Approves Bacteriophage Trial. J. Am. Med. Assoc. 2019, 321, 638. [Google Scholar] [CrossRef] [PubMed]
- Office of the Commissioner Bacteriophage. Are Viruses That Target and Kill Specific Bacterial Spec. Available online: https://www.fda.gov/science-research/fda-science-forum/impact-various-routes-administered-phages-host-microbial-community (accessed on 21 November 2023).
- Plymoth, M.; Lynch, S.A.; Khatami, A.; Sinclair, H.A.; Sacher, J.C.; Zheng, J.; Lin, R.C.Y.; Iredell, J.R. Attitudes to Phage Therapy among Australian Infectious Diseases Physicians. bioRxiv 2023. [Google Scholar] [CrossRef]
- Żaczek, M.; Zieliński, M.W.; Górski, A.; Weber-Dąbrowska, B.; Międzybrodzki, R. Perception of Phage Therapy and Research across Selected Professional and Social Groups in Poland. Front. Public. Health 2025, 13, 1490737. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, S. Response to Phage Therapy in Korea: A Prescribers’ Survey of Attitudes amongst Korean Infectious Diseases Specialists towards Phage Therapy. Infect. Chemother. 2024, 56, 278–279. [Google Scholar] [CrossRef] [PubMed]
- Aslam, S.; Lampley, E.; Wooten, D.; Karris, M.; Benson, C.; Strathdee, S.; Schooley, R.T. Lessons Learned from the First 10 Consecutive Cases of Intravenous Bacteriophage Therapy to Treat Multidrug-Resistant Bacterial Infections at a Single Center in the United States. Open Forum Infect. Dis. 2020, 7, ofaa389. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, K.; Meshram, S. The Evolution of Phage Therapy: A Comprehensive Review of Current Applications and Future Innovations. Cureus 2024, 16, e70414. [Google Scholar] [CrossRef] [PubMed]
- Abedon, S.T.; Kuhl, S.J.; Blasdel, B.G.; Kutter, E.M. Phage Treatment of Human Infections. Bacteriophage 2011, 1, 66–85. [Google Scholar] [CrossRef] [PubMed]
- Pirnay, J.-P.; Blasdel, B.G.; Bretaudeau, L.; Buckling, A.; Chanishvili, N.; Clark, J.R.; Corte-Real, S.; Debarbieux, L.; Dublanchet, A.; De Vos, D.; et al. Quality and Safety Requirements for Sustainable Phage Therapy Products. Pharm. Res. 2015, 32, 2173–2179. [Google Scholar] [CrossRef] [PubMed]
- German, G.J.; Kus, J.V.; Schwartz, K.L.; Webster, D.; Yamamura, D.L. Experience and Interest in Bacteriophage Therapy in Canada: An AMMI Canada Survey. 2022 Annual Conference Conférence Annuelle. Off. J. Assoc. Med. Microbiol. Infect. Dis. Can. 2022, 7, 1–131. [Google Scholar] [CrossRef]
- Althubaiti, A. Information Bias in Health Research: Definition, Pitfalls, and Adjustment Methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Robinson, R.; Nguyen, E.; Wright, M.; Holmes, J.; Oliphant, C.; Cleveland, K.; Nies, M.A. Factors Contributing to Vaccine Hesitancy and Reduced Vaccine Confidence in Rural Underserved Populations. Humanit. Soc. Sci. Commun. 2022, 9, 416. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, A.; Gandhi, S.; Lehman, D.; Jacobs, K.J. Redefining the Vulnerable Population in Public Health Research: Incorporating Ideological Determinants of Anti-Vaccination Attitudes. In Social Factors, Health Care Inequities and Vaccination; Kronenfeld, J.J., Ed.; Emerald Publishing Limited: Somerville, MA, USA, 2023; Volume 40, pp. 65–79. [Google Scholar]
- Callaghan, T.; Washburn, D.; Goidel, K.; Nuzhath, T.; Spiegelman, A.; Scobee, J.; Moghtaderi, A.; Motta, M. Imperfect Messengers? An Analysis of Vaccine Confidence among Primary Care Physicians. Vaccine 2022, 40, 2588–2603. [Google Scholar] [CrossRef] [PubMed]
- Martensen, R.L. The Effect of Medical Conservatism on the Acceptance of Important Medical Discoveries. J. Am. Med. Assoc. 1996, 276, 1933. [Google Scholar] [CrossRef]
- Mandrola, J.; Cifu, A.; Prasad, V.; Foy, A. The Case for Being a Medical Conservative. Am. J. Med. 2019, 132, 900–901. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean | Std Deviation |
|---|---|---|
| Age (Years) | ||
| Overall | 54.29 | 9.99 |
| Male | 55.72 | 9.91 |
| Female | 51.38 | 9.68 |
| Frequency (n) | Percentage (%) | |
| Gender | ||
| Male | 148 | 65.8 |
| Female | 74 | 32.9 |
| Others | 3 | 1.3 |
| Race | ||
| White | 171 | 76.0 |
| Black | 6 | 2.7 |
| Asian | 36 | 16.0 |
| Others | 12 | 5.3 |
| Ethnicity | ||
| Hispanic or Latino | 4 | 1.8 |
| Non-Hispanic or Latino | 221 | 98.2 |
| Employment Status | ||
| Employed full-time | 206 | 91.6 |
| Employed part-time | 14 | 6.2 |
| Retired and other | 5 | 2.2 |
| Political Affiliation | ||
| Conservative (very) | 11 | 4.9 |
| Conservative (moderate) | 43 | 19.1 |
| Conservative (light) | 28 | 12.4 |
| Neutral | 50 | 22.2 |
| Liberal (light) | 23 | 10.2 |
| Liberal (moderate) | 34 | 15.1 |
| Liberal (very) | 10 | 4.4 |
| Prefer not to answer | 26 | 11.6 |
| Marital Status | ||
| Married/Not married, but cohabiting | 189 | 84.0 |
| Married, but not cohabitating | 4 | 1.8 |
| Not married or cohabitating | 29 | 12.9 |
| Other | 3 | 1.3 |
| Professional Degree | ||
| Doctor of Medicine (MD) | 161 | 71.6 |
| Doctor of Osteopathic Medicine (DO) | 58 | 25.8 |
| Others (e.g., DPM, LNP) | 6 | 2.7 |
| Willing N (%) | Unsure N (%) | 𝜒2 | p | |
|---|---|---|---|---|
| Age (years) | 0.286 | 0.59 | ||
| <50 | 39 (18.1) | 26 (12.0) | ||
| ≥50 years | 83 (38.4) | 68 (31.5) | ||
| Gender | 0.398 | 0.53 | ||
| Male | 84 (38.9) | 60 (27.8) | ||
| Female | 38 (17.6) | 34 (15.7) | ||
| Race | 0.681 | 0.71 | ||
| White | 92 (42.6) | 73 (33.8) | ||
| Asian | 20 (9.3) | 16 (7.4) | ||
| Others | 10 (4.6) | 5 (2.3) | ||
| Employment Status | 0.110 | 0.74 | ||
| Employed full-time | 113 (52.3) | 85 (39.4) | ||
| Employed part-time, retired, other | 9 (4.2) | 9 (4.2) | ||
| Political Affiliation | 4.73 | 0.19 | ||
| Conservative | 35 (16.2) | 40 (18.5) | ||
| Neutral | 32 (14.8) | 18 (8.3) | ||
| Liberal | 41 (19.0) | 26 (12.0) | ||
| Prefer not to answer | 14 (6.5) | 10 (4.6) | ||
| Marital Status | 1.035 | 0.31 | ||
| Married/Not married, but cohabiting | 99 (45.8) | 82 (38.0) | ||
| Married, but not cohabitating/Not married or cohabitating | 23 (10.6) | 12 (5.6) | ||
| Year of Licensure Attainment | 1.304 | 0.25 | ||
| Before 1999 | 70 (32.4) | 62 (28.7) | ||
| After 2000 | 52 (24.1) | 32 (14.8) | ||
| Location of Practice | 0.000 | 1.00 | ||
| Rural zip codes | 16 (7.4) | 12 (5.6) | ||
| Non-rural zip codes | 98 (45.4) | 75 (34.7) | ||
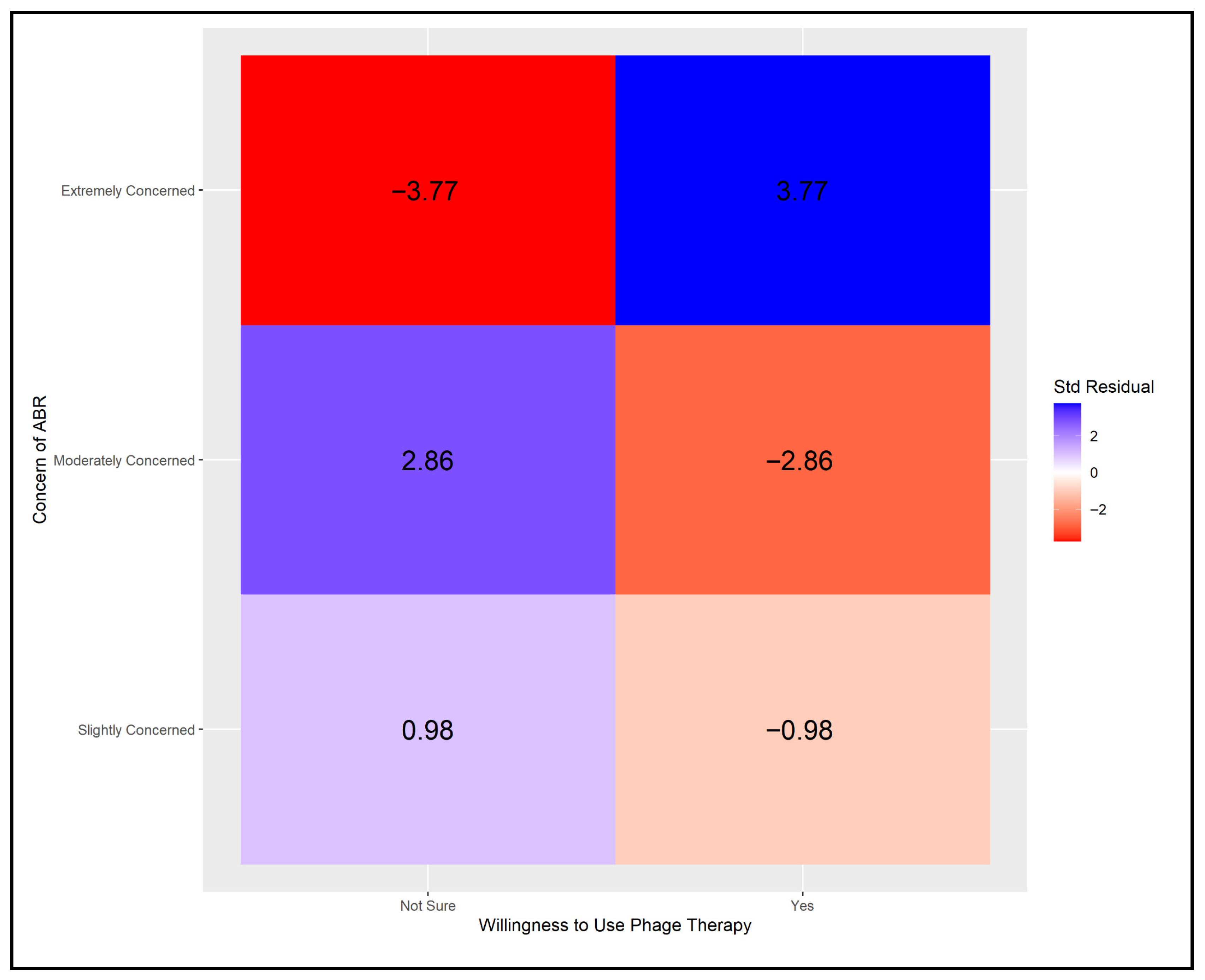
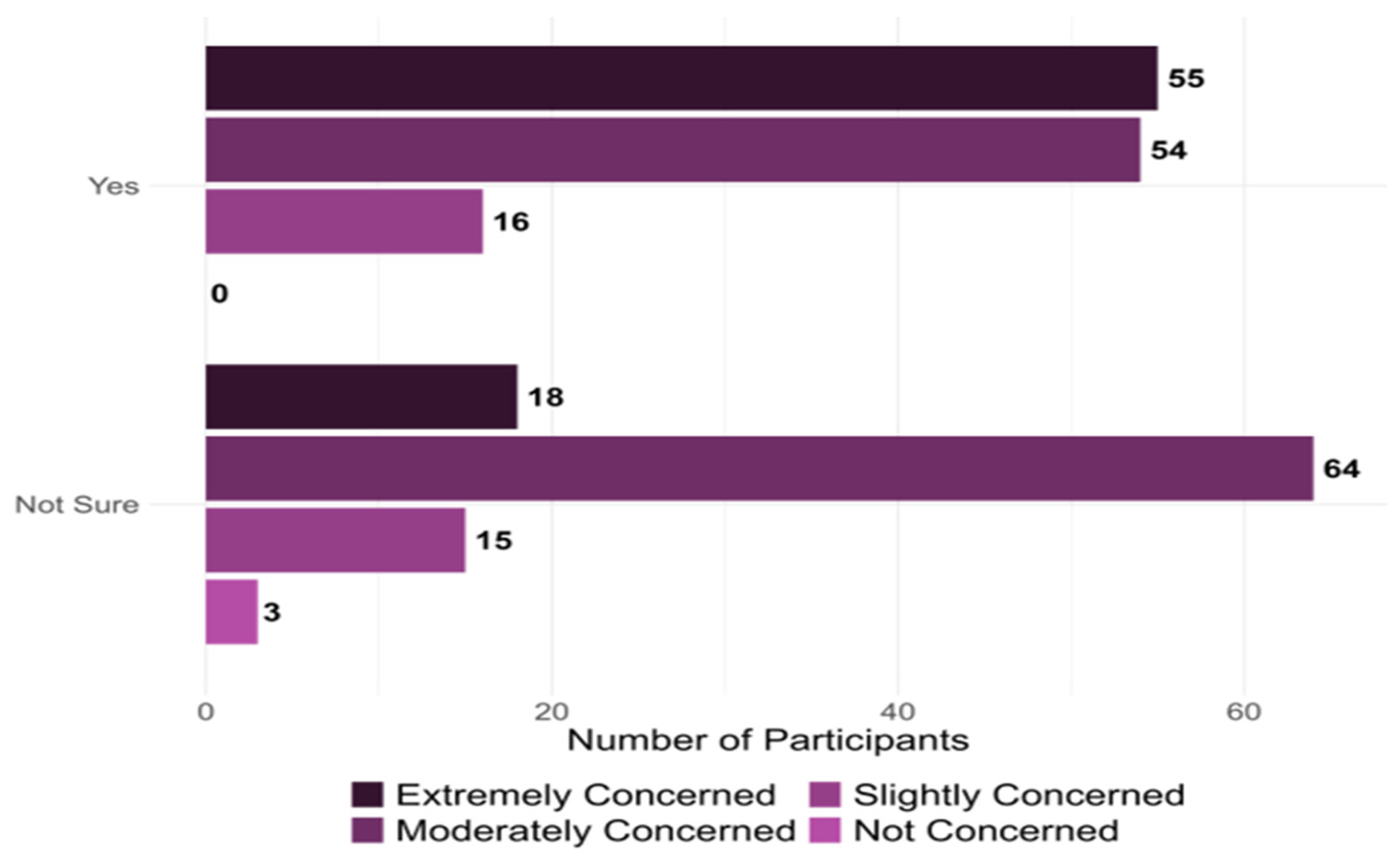
| Providers’ Concerns about Antibiotic Resistance * | 14.211 | 0.00 * | ||
| Slightly Concerned | 15 (6.9) | 16 (7.4) | ||
| Moderately Concerned | 54 (25.0) | 60 (27.8) | ||
| Extremely Concerned | 53 (24.5) | 18 (8.3) | ||
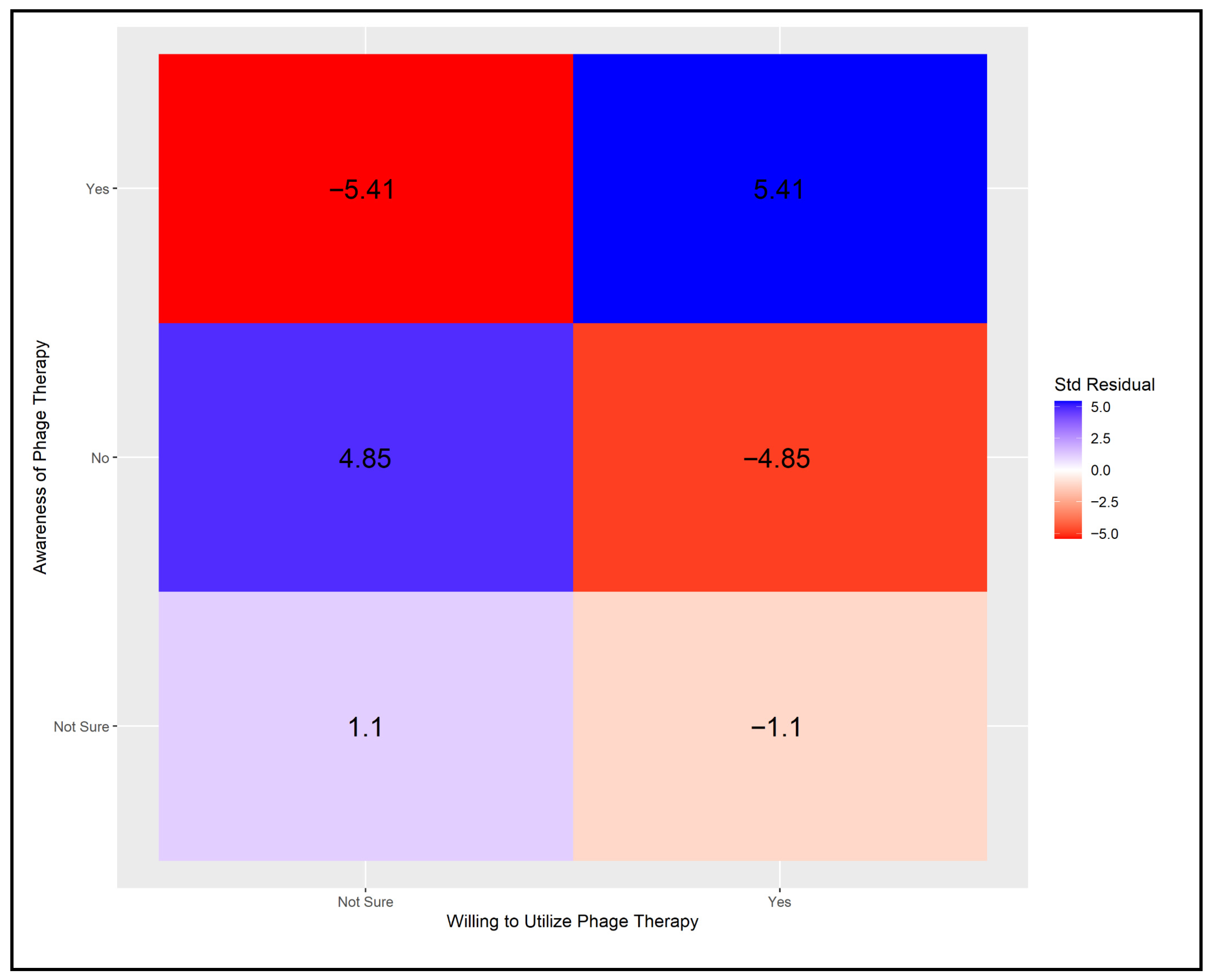
| Providers’ Knowledge of Phage Therapy | 31.912 | 0.00 * | ||
| Yes | 79 (36.6) | 26 (12.0) | ||
| No | 23 (10.6) | 47 (21.8) | ||
| Not Sure | 20 (9.3) | 21 (9.7) | ||
| Event/Training Where Providers Learned About Phage Therapy | 29.283 | 0.00 * | ||
| Professional School | 21 (9.7) | 4 (1.9) | ||
| Conference | 44 (20.4) | 17 (7.9) | ||
| Clinical Practice | 23 (10.6) | 14 (6.5) | ||
| Other | 34 (15.7) | 59 (27.3) | ||
| Patients Willing to Accept Phage Therapy If Endorsed By Physicians * | 30.04 | 0.00 * | ||
| Very likely | 21 (9.7) | 2 (0.9) | ||
| Likely | 63 (29.2) | 30 (13.9) | ||
| Somewhat | 38 (17.6) | 62 (28.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gandhi, S.; Edwards, D.; Emmert, K.; Large, B. Exploration of Providers’ Perceptions and Attitudes Toward Phage Therapy and Intentions for Future Adoption as an Alternative to Traditional Antibiotics in the US—A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2025, 22, 1139. https://doi.org/10.3390/ijerph22071139
Gandhi S, Edwards D, Emmert K, Large B. Exploration of Providers’ Perceptions and Attitudes Toward Phage Therapy and Intentions for Future Adoption as an Alternative to Traditional Antibiotics in the US—A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2025; 22(7):1139. https://doi.org/10.3390/ijerph22071139
Chicago/Turabian StyleGandhi, Subi, Dustin Edwards, Keith Emmert, and Bonnie Large. 2025. "Exploration of Providers’ Perceptions and Attitudes Toward Phage Therapy and Intentions for Future Adoption as an Alternative to Traditional Antibiotics in the US—A Cross-Sectional Study" International Journal of Environmental Research and Public Health 22, no. 7: 1139. https://doi.org/10.3390/ijerph22071139
APA StyleGandhi, S., Edwards, D., Emmert, K., & Large, B. (2025). Exploration of Providers’ Perceptions and Attitudes Toward Phage Therapy and Intentions for Future Adoption as an Alternative to Traditional Antibiotics in the US—A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 22(7), 1139. https://doi.org/10.3390/ijerph22071139