
Prevalence and Contributing Factors of Occupational Injuries Among Nurses in Oshakati District, Namibia


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Site
2.3. Study Population
2.4. Sampling Strategy
2.5. Sample Size Estimation
2.6. Ethical Considerations
2.7. Data Collection and Management
2.8. Data Analysis
3. Results
3.1. Demographic Characteristics for Primary Data
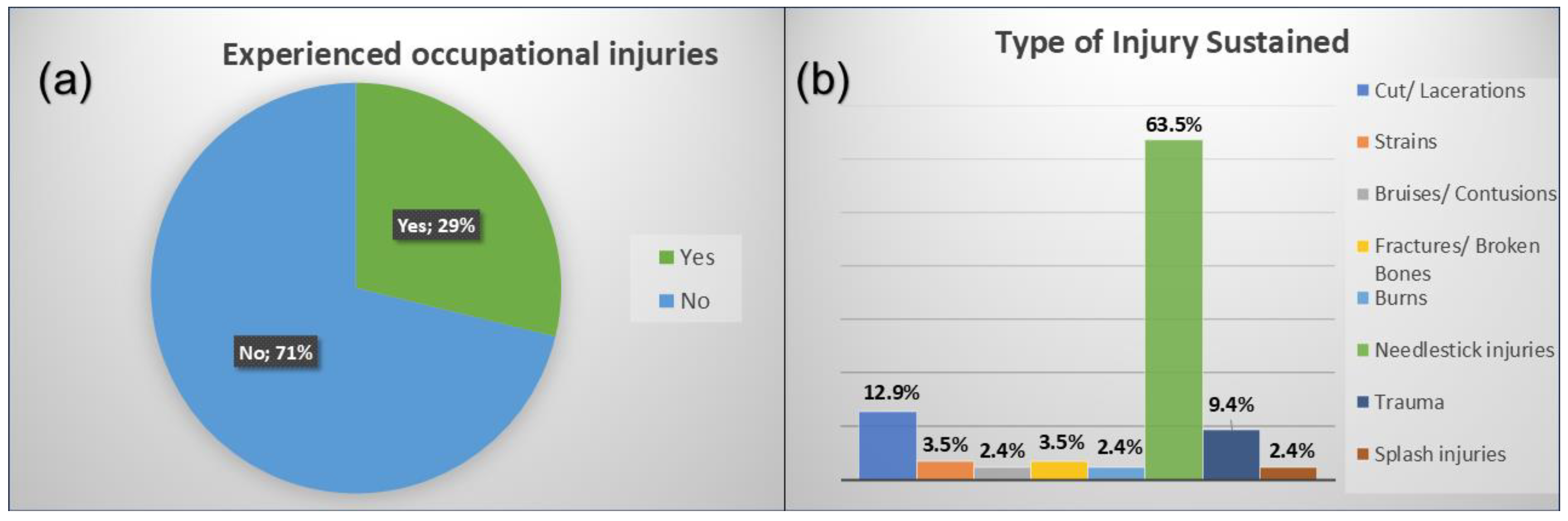
3.2. Prevalence of Occupational Injuries Among Nurses
3.3. Types and Causes of Injuries
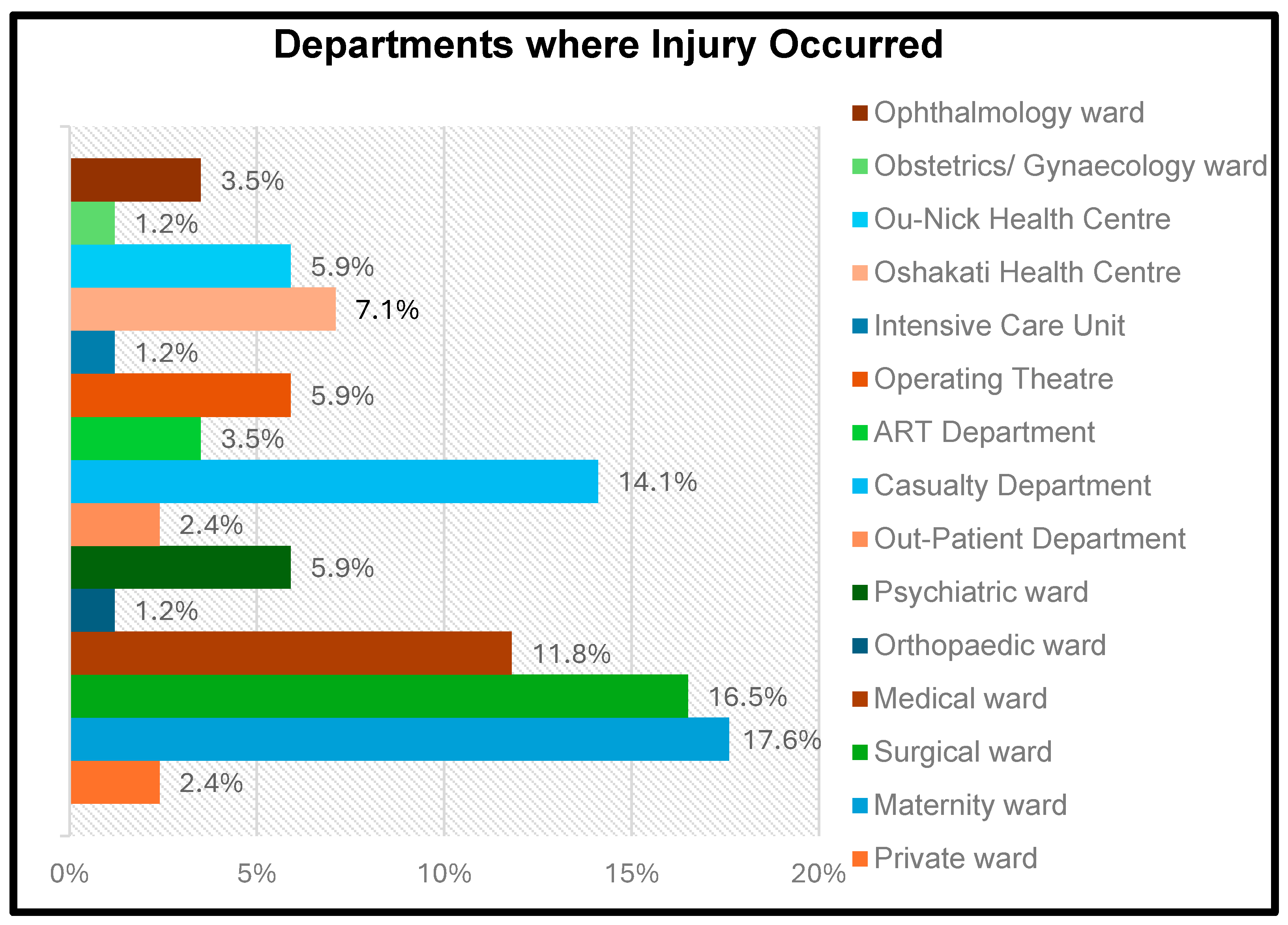
3.4. Department Where Injury Occurred
3.5. Reporting and Medical Attention for Injured Nurses
3.6. Descriptive Statistics for Secondary Data
3.7. Contributing Factors from Secondary Data
3.8. Tests for Normality
3.9. Chi-Square Test Analysis
3.10. Univariate and Multivariate Logistic Regression
3.11. Comparison of Primary and Secondary Data
4. Discussion
4.1. Prevalence of Occupational Injuries
4.2. Types of Injuries
4.3. Causes of Injuries
4.4. Anatomical Sites Affected by Injuries
4.5. Distribution of Injuries Among Hospital Departments
4.6. Comparison of Injuries Among Nurses Working in Different Health Facilities
4.7. Reporting of Injuries to Authorities
4.8. Medical Care Accessed Post-Injury
4.9. Severity of Injuries
4.10. Factors Contributing to Occupational Injuries
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations Global Compact. A Safe and Healthy Working Environment: Improving Safety and Health Through Supply Chains and Building a Culture of Prevention and Protection. 2022. Available online: https://unglobalcompact.org/take-action/safety-andhealth (accessed on 16 October 2023).
- World Health Organisation (WHO). Occupational Health: Health Workers. Key Facts, 7 November 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/occupational-health--health-workers (accessed on 16 October 2023).
- International Labour Organisation. Occupational Safety and Health Statistics (OSH) Database. Occupational Injuries. 2023. Available online: https://ilostat.ilo.org/resources/concepts-and-definitions/description-occupational-safety-and-health-statistics/ (accessed on 17 October 2023).
- WHO. International Statistical Classification of Diseases and Related Health Problems (ICD). 2023. Available online: https://www.who.int/standards/classifications/classification-of-diseases (accessed on 17 October 2023).
- Gu, J.K.; Charles, L.E.; Fekedulegn, D.; Ma, C.C.; Violanti, J.M.; Andrew, M.E. Occupational injury and psychological distress among U.S. workers: The National Health Interview Survey, 2004–2016. J. Saf. Res. 2020, 74, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, D.; Ghaziri, M.E. Violence in health care: Trends and Disparities, Bureau of Labour Statistics Survey Data of Occupational Injuries and Illnesses, 2011–2017. Workplace Health Saf. 2022, 70, 136–147. [Google Scholar] [CrossRef] [PubMed]
- Moyo, E.; Dzinamarira, T.; Mhango, M.; Feresu, S.; Moyo, P. Prevalence of needlestick injuries and factors associated with their occurrence among health care workers at a private hospital in northern Namibia. Hum. Factors Healthc. 2022, 2, 100028. [Google Scholar] [CrossRef]
- Rai, R.; El-Zaemey, S.; Dorji, N.; Rai, B.D.; Fritschi, L. Exposure to occupational hazards among health care workers in low- and middle-income countries: A scoping review. Int. J. Environ. Res. Public Health 2021, 18, 2603. [Google Scholar] [CrossRef]
- Nadalin, V.; Smith, P.M. Examining the impact of occupational health and safety vulnerability on injury claim reporting in three Canadian provinces. Am. J. Ind. Med. 2020, 63, 435–441. [Google Scholar] [CrossRef]
- Debelu, D.; Mengistu, D.A.; Tolera, S.T.; Aschalew, A.; Deriba, W. Occupational-related injuries and associated risk factors among healthcare workers working in developing countries: A Systematic Review. Health Serv. Res. Manag. Epidemiol. 2023, 10, 23333928231192834. [Google Scholar] [CrossRef]
- Appiagyei, H.; Nakua, E.K.; Donkor, P.; Mock, C. Occupational injuries among healthcare workers at a public hospital in Ghana. Pan Afr. Med. J. 2021, 39, 103. [Google Scholar] [CrossRef] [PubMed]
- Erturk Sengel, B.; Tukenmez Tigen, E.; Bilgin, H.; Dogru, A.; Korten, V. Occupation-related injuries among healthcare workers: Incidence, risk groups, and the effect of training. Cureus 2021, 13, e14318. [Google Scholar] [CrossRef]
- WHO & International Labour Organisation (ILO). Caring for Those Who Care: National Programmes for Occupational Health for Health Workers. Policy Brief. World Health Organisation. 2020. Available online: https://apps.who.int/iris/handle/10665/336479 (accessed on 8 September 2023).
- Denge, T.; Rakhudu, M. Perceptions of nurses on occupational health hazards and safety practices in Ditsobotla public hospitals in North-West province. Curationis 2022, 45, e1–e9. [Google Scholar] [CrossRef]
- Che Huei, L.; Ya-Wen, L.; Chiu Ming, Y.; Li Chen, H.; Jong Yi, W.; Ming Hung, L. Occupational health and safety hazards faced by healthcare professionals in Taiwan: A systematic review of risk factors and control strategies. SAGE Open Med. 2020, 8, 2050312120918999. [Google Scholar] [CrossRef]
- Hebo, H.J.; Gemeda, D.H.; Abdusemed, K.A. Hepatitis B and C Viral Infection: Prevalence, knowledge, attitude, practice, and occupational exposure among healthcare workers of Jimma University Medical Center, Southwest Ethiopia. Sci. World J. 2019, 2019, 9482607. [Google Scholar] [CrossRef] [PubMed]
- Mossburg, S.; Agore, A.; Nkimbeng, M.; Commodore-Mensah, Y. Occupational hazards among healthcare workers in Africa: A systematic review. Ann. Glob. Health 2019, 85, 78. [Google Scholar] [CrossRef]
- Godsey, J.A.; Houghton, D.M.; Hayes, T. Registered nurse perceptions of factors contributing to the inconsistent brand image of the nursing profession. Nurs. Outlook 2020, 68, 808–821. [Google Scholar] [CrossRef] [PubMed]
- Christians, F. Country profile—Primary healthcare and family medicine in Namibia. Afr. J. Prim. Health Care Fam. Med. 2020, 12, e1–e3. [Google Scholar] [CrossRef]
- Ashipala, P.S. Organisational Role Stress and Work Engagement Among Nurses Working in Intermediate Hospital Oshakati, Namibia. Master’s Thesis, University of Namibia Scholarly Repository, Windhoek, Namibia, 2022. Available online: https://repository.unam.edu.na/handle/11070/3616 (accessed on 10 September 2023).
- Ministry of Labour, Industrial Relations and Employment Creation. National Profile on Occupational Safety and Health: Namibia. 2021. Available online: https://mol.gov.na/documents/53329/0/National+Occupational+Safety+and+Health+Policy+%282%29.pdf (accessed on 8 September 2023).
- Park, Y.; Konge, L.; Artino, A.R. The Positivism Paradigm of Research. Acad. Med. 2020, 95, 690–694. [Google Scholar] [CrossRef]
- Oshana Regional Council. Oshana Regional Profile. 2024. Available online: https://oshanarc.gov.na/history (accessed on 30 January 2024).
- Magesa, E.; Hanyanya, J.; Erraso, W. Patient’s satisfaction at outpatient pharmacy department in Intermediate Hospital Oshakati, Oshana region, Namibia. GSC Biol. Pharm. Sci. 2021, 14, 22–28. [Google Scholar] [CrossRef]
- Google Maps. Oshakati Geography Population Map. 2023. Available online: https://www.tageo.com/index-e-wa-v-37-d-m3557700.htm (accessed on 20 November 2023).
- Mdluli, P.M. The Relationship Between Cigarette Smoking and Occupational Noise Induced Hearing Loss Among Employees Working at the Royal Swaziland Sugar Corporation, Swaziland, 2018/19. Master’s Thesis, University of Johannesburg, Johannesburg, South Africa, 2020. Available online: https://ujcontent.uj.ac.za/esploro/outputs/graduate/The-relationship-between-cigarette-smoking-and/9912622207691 (accessed on 22 November 2023).
- Khatun, N. Applications of normality test in statistical analysis. Open J. Stat. 2021, 11, 113–122. [Google Scholar] [CrossRef]
- Cooksey, R.W. Descriptive Statistics for Summarising Data. In Illustrating Statistical Procedures: Finding Meaning in Quantitative Data; Springer: Singapore, 2020. [Google Scholar] [CrossRef]
- Alameer, D.S.; Noor, E.I.R. Prevalence and Determinants of Work-Related Injuries Among Healthcare Workers in Jeddah, Saudi Arabia. Cureus 2023, 15, e36679. [Google Scholar] [CrossRef]
- Matthys, D. Government Prepares Workplace Health & Safety Legislation. The Namibian, 26 June 2024. Available online: https://www.namibian.com.na/govt-prepares-workplace-health-safety-legislation (accessed on 20 January 2025).
- Nwoga, H.O.; Ajuba, M.O.; Nwankwo, M.M. Occupational accidents among healthcare workers in a tertiary health facility in Enugu state, South-East Nigeria. Int. J. Community Med. Public Health 2020, 7, 2005–2010. [Google Scholar] [CrossRef]
- Kim, J.S.; Jeong, B.Y. Human errors and occupational injuries of older female workers in residential healthcare facilities for the elderly. Int. J. Occup. Saf. Ergon. 2020, 26, 497–506. [Google Scholar] [CrossRef]
- Courtice, M.N.; Olsson, A.C.; Cherrie, J.W. Less economically developed countries need help to create healthy workplaces. Front. Public Health 2019, 7, 257. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, K.S.; Raju, G.; Shawkataly, O. Prevalence of work-related musculoskeletal disorders: Psychological and physical risk factors. Int. J. Environ. Res. Public Health 2021, 18, 9361. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.; Lee, J.; Kim, H.-R.; Lee, D.-W.; Kang, M.-Y. Comparative analysis of occupational injuries among temporary agency workers and direct contract workers: Findings from the Korea Health Panel 2009–2018. J. Occup. Health 2022, 64, e12326. [Google Scholar] [CrossRef]
- Amuele, E. Safety and Protection at Work. Republikein, 7 June 2022. Available online: https://www.republikein.com.na/focuscareers/safetyandprotectionatwork2022-06-0714859 (accessed on 18 August 2022).
- López Gómez, M.A.; Williams, J.A.R.; Boden, L.; Sorensen, G.; Hopcia, K.; Hashimoto, D.; Sabbath, E. The relationships of occupational injury and use of mental health care. J. Saf. Res. 2020, 74, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Mlambo, M.; Silén, C.; McGrath, C. Lifelong learning and nurses’ continuing professional development, a metasynthesis of the literature. BMC Nurs. 2021, 20, 62. [Google Scholar] [CrossRef]
- Ashipala, D.O.; Nghole, T.M. Factors contributing to burnout among nurses at a district hospital in Namibia: A qualitative perspective of nurses. J. Nurs. Manag. 2022, 30, 2982–2991. [Google Scholar] [CrossRef]
- Imes, C.C.; Barthel, J.N.; Chasens, R.E.; Dunbar-Jacob, J.; Engberg, J.S.; Feeley, A.C.; Fennimore, A.L.; Godzik, M.C.; Klem, L.M.; Luyster, S.F.; et al. Shift work organisation on nurse injuries: A scoping review. Int. J. Nurs. Stud. 2023, 138, 104395. [Google Scholar] [CrossRef]
- Duan, X.; Sun, H.; He, Y.; Yang, J.; Li, X.; Taparia, K.; Zheng, B. Personal Protective Equipment in COVID-19: Impacts on health performance, work-related injuries, and measures for prevention. J. Occup. Environ. Med. 2021, 63, 221–225. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variable | Demographic Factors | Frequency (n) | Percentage (%) |
|---|---|---|---|
| Sex | Male | 45 | 15.3 |
| Female | 250 | 84.7 | |
| Age | 18–25 | 39 | 13.2 |
| 26–35 | 128 | 43.4 | |
| 36–45 | 84 | 28.5 | |
| 46–55 | 28 | 9.5 | |
| 56+ | 16 | 5.4 | |
| Highest educational level | Certificate/diploma | 147 | 49.8 |
| Bachelor’s degree | 123 | 41.7 | |
| Postgraduate degree | 25 | 8.5 | |
| Place of work | Private ward | 6 | 2.0 |
| Maternity ward | 61 | 20.7 | |
| Surgical ward | 30 | 10.2 | |
| Orthopaedic ward | 22 | 7.5 | |
| Psychiatric ward | 9 | 3.1 | |
| Outpatient department (OPD) | 29 | 9.8 | |
| Emergency department (casualty) | 19 | 6.4 | |
| Paediatric medical ward | 4 | 1.4 | |
| X-ray department | 2 | 0.7 | |
| ART department | 9 | 3.1 | |
| Operating theatre | 15 | 5.1 | |
| Intensive care unit (ICU) | 10 | 3.4 | |
| Central Sterile Supply Department (CSSD) | 2 | 0.7 | |
| Oshakati Health Centre | 27 | 9.2 | |
| Ou-Nick Health Centre | 11 | 3.7 | |
| Paediatric surgical ward | 7 | 2.4 | |
| TB ward | 3 | 1.0 | |
| Ophthalmology ward | 5 | 1.7 | |
| Oncology | 6 | 2.0 | |
| Dialysis ward | 1 | 0.3 | |
| Years of experience | 1–5 years | 137 | 46.4 |
| 6–10 years | 83 | 28.1 | |
| 11–15 years | 35 | 11.9 | |
| 16 years or more | 40 | 13.6 | |
| Employment status | Registered nurse | 186 | 63.1 |
| Enrolled nurse | 109 | 36.9 |
| Variable | Demographic Factors | Frequency (n) | Percentage (%) |
|---|---|---|---|
| Sex | Female | 7 | 100 |
| Age | 18–25 | 1 | 14.3 |
| 26–35 | 2 | 28.6 | |
| 36–45 | 3 | 42.9 | |
| 46–55 | 0 | 0 | |
| 56+ | 1 | 14.3 | |
| Employment status | Registered nurse | 6 | 85.7 |
| Enrolled nurse | 1 | 14.3 |
| Factor | p-Value | Significance |
|---|---|---|
| Place of work | <0.001 | Significant; Reject null hypothesis |
| Sex | <0.001 | Significant; Reject null hypothesis |
| Age | <0.001 | Significant; Reject null hypothesis |
| Highest level of education | <0.001 | Significant; Reject null hypothesis |
| Years of experience | <0.001 | Significant; Reject null hypothesis |
| Employment status | <0.001 | Significant; Reject null hypothesis |
| Factor | Pearson Chi-Square (p-Value) | Significance |
|---|---|---|
| Demographic factors | ||
| Place of work | 0.083 | No significant association |
| Sex | 0.990 | No significant association |
| Age | 0.114 | No significant association |
| Highest level of education | 0.027 | Significant association |
| Years of experience | 0.029 | Significant association |
| Employment status | 0.012 | Significant association |
| Contributing factors | ||
| Unsafe work environment | 0.158 | No significant association |
| Work overload | 0.630 | No significant association |
| Lack of proper training and education | 0.001 | Significant association |
| Inadequate staffing levels | 0.009 | Significant association |
| Poor shift patterns | 0.016 | Significant association |
| Inadequate safety equipment | 0.004 | Significant association |
| Work-related stress | 0.201 | No significant association |
| Poor work organisation | 0.011 | Significant association |
| Variable | Univariate Logistic Regression | Multivariate Logistic Regression | ||||
|---|---|---|---|---|---|---|
| p-Value | Crude Odds Ratio | Confidence Interval (95%) | p-Value | Adjusted Odds Ratio | Confidence Interval (95%) | |
| Demographic characteristics | ||||||
| Highest level of education (certificate/diploma) | 0.02 | 2.90 | 1.22–6.88 | 0.80 | 1.16 | 0.38–3.51 |
| Highest level of education (bachelor’s degree) | 0.01 | 3.08 | 1.28–7.44 | 0.03 | 3.30 | 1.11–9.81 |
| Years of experience (1–5 years) | 0.01 | 2.75 | 1.30–5.82 | 0.48 | 1.40 | 0.54–3.63 |
| Years of experience (6–10 years) | 0.23 | 1.62 | 0.74–3.53 | 0.62 | 0.79 | 0.30–2.04 |
| Employment status (registered nurses) | 0.01 | 0.49 | 0.28–0.86 | 0.01 | 0.30 | 0.12–0.74 |
| Contributing factors | ||||||
| Unsafe work environment | 0.16 | 1.44 | 0.87–2.41 | 0.74 | 0.90 | 0.49–1.65 |
| Lack of proper training and education | 0.01 | 3.64 | 1.96–6.77 | 0.01 | 3.27 | 1.62–6.61 |
| Inadequate staffing levels | 0.01 | 2.37 | 1.23–4.59 | 0.12 | 1.89 | 0.85–4.19 |
| Poor shift patterns | 0.02 | 2.91 | 1.18–7.16 | 0.55 | 1.38 | 0.48–3.99 |
| Inadequate safety equipment | 0.01 | 2.12 | 1.26–3.59 | 0.08 | 1.71 | 0.93–3.15 |
| Work-related stress | 0.20 | 1.44 | 0.82–2.51 | 0.76 | 0.90 | 0.45–1.79 |
| Poor workplace organisation | 0.01 | 2.24 | 1.19–4.19 | 0.89 | 1.06 | 0.49–2.28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanjobo, M.L.; Senekane, M.F.; Lebelo, K. Prevalence and Contributing Factors of Occupational Injuries Among Nurses in Oshakati District, Namibia. Int. J. Environ. Res. Public Health 2025, 22, 912. https://doi.org/10.3390/ijerph22060912
Sanjobo ML, Senekane MF, Lebelo K. Prevalence and Contributing Factors of Occupational Injuries Among Nurses in Oshakati District, Namibia. International Journal of Environmental Research and Public Health. 2025; 22(6):912. https://doi.org/10.3390/ijerph22060912
Chicago/Turabian StyleSanjobo, Maliwa Lichaha, Mpinane Flory Senekane, and Kgomotso Lebelo. 2025. "Prevalence and Contributing Factors of Occupational Injuries Among Nurses in Oshakati District, Namibia" International Journal of Environmental Research and Public Health 22, no. 6: 912. https://doi.org/10.3390/ijerph22060912
APA StyleSanjobo, M. L., Senekane, M. F., & Lebelo, K. (2025). Prevalence and Contributing Factors of Occupational Injuries Among Nurses in Oshakati District, Namibia. International Journal of Environmental Research and Public Health, 22(6), 912. https://doi.org/10.3390/ijerph22060912