
The Effect of Type 2 Diabetes on Bone Quality: A Systematic Review and Meta-Analysis of Cohort Studies

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Method
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ojo, O.; Kalocsányiová, E.; McCrone, P.; Elliott, H.; Milligan, W.; Gkaintatzi, E. Non-Pharmacological Interventions for Type 2 Diabetes in People Living with Severe Mental Illness: Results of a Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2024, 21, 423. [Google Scholar] [CrossRef] [PubMed]
- Cirovic, A.; Vujacic, M.; Petrovic, B.; Cirovic, A.; Zivkovic, V.; Nikolic, S.; Djonic, D.; Bascarevic, Z.; Djuric, M.; Milovanovic, P. Vascular Complications in Individuals with Type 2 Diabetes Mellitus Additionally Increase the Risk of Femoral Neck Fractures Due to Deteriorated Trabecular Microarchitecture. Calcif. Tissue Int. 2022, 110, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Ojo, O.; Boateng, J.; Pacella, R.; Hanrahan, A.; Essex, R.; Dibley, L. Factors Influencing the Care and Management of Diabetic Foot Ulcers: A Scoping Review. Endocr. Pract. 2024, 31, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zhang, Y.; Liu, X.; Chen, B.; Lei, L. Effect of type 2 diabetes on biochemical markers of bone metabolism: A meta-analysis. Front. Physiol. 2024, 15, 1330171. [Google Scholar] [CrossRef]
- Martínez-Montoro, J.I.; García-Fontana, B.; García-Fontana, C.; Muñoz-Torres, M. Evaluation of Quality and Bone Microstructure Alterations in Patients with Type 2 Diabetes: A Narrative Review. J. Clin. Med. 2022, 11, 2206. [Google Scholar] [CrossRef]
- Sheu, A.; Blank, R.D.; Tran, T.; Bliuc, D.; Greenfield, J.R.; White, C.P.; Center, J.R. Associations of Type 2 Diabetes, Body Composition, and Insulin Resistance with Bone Parameters: The Dubbo Osteoporosis Epidemiology Study. JBMR Plus 2023, 7, e10780. [Google Scholar] [CrossRef]
- Donnelly, E. Methods for assessing bone quality: A review. Clin. Orthop. Relat. Res. 2011, 469, 2128–2138. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Morgan, E.F.; Unnikrisnan, G.U.; Hussein, A.I. Bone Mechanical Properties in Healthy and Diseased States. Annu. Rev. Biomed. Eng. 2018, 20, 119–143. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Napoli, N.; Incalzi, R.A.; De Gennaro, G.; Marcocci, C.; Marfella, R.; Papalia, R.; Purrello, F.; Ruggiero, C.; Tarantino, U.; Tramontana, F.; et al. Bone fragility in patients with diabetes mellitus: A consensus statement from the working group of the Italian Diabetes Society (SID), Italian Society of Endocrinology (SIE), Italian Society of Gerontology and Geriatrics (SIGG), Italian Society of Orthopaedics and Traumatology (SIOT). Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1375–1390. [Google Scholar] [CrossRef]
- Weber, D.R.; Long, F.; Zemel, B.S.; Kindler, J.M. Glycemic Control and Bone in Diabetes. Curr. Osteoporos. Rep. 2022, 20, 379–388. [Google Scholar] [CrossRef]
- Misof, B.M.; Blouin, S.; Andrade, V.F.C.; Roschger, P.; Borba, V.Z.C.; Hartmann, M.A.; Zwerina, J.; Recker, R.R.; Moreira, C.A. No evidence of mineralization abnormalities in iliac bone of premenopausal women with type 2 diabetes mellitus. J. Musculoskelet. Neuronal Interact. 2022, 22, 305–315. [Google Scholar] [PubMed]
- Ma, L.; Oei, L.; Jiang, L.; Estrada, K.; Chen, H.; Wang, Z.; Yu, Q.; Zillikens, M.C.; Gao, X.; Rivadeneira, F. Association between bone mineral density and type 2 diabetes mellitus: A meta-analysis of observational studies. Eur. J. Epidemiol. 2012, 27, 319–332. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.V. Epidemiology of fractures in type 2 diabetes. Bone 2016, 82, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Liu, J.; Xiao, L.; Liu, D.; Yan, W.; Hu, T.; Li, K.; Hua, X.; Zeng, X. Comparison of FRAX in postmenopausal Asian women with and without type 2 diabetes mellitus: A retrospective observational study. J. Int. Med. Res. 2020, 48, 300060519879591. [Google Scholar] [CrossRef] [PubMed]
- Sheu, A.; White, C.P.; Center, J.R. Bone metabolism in diabetes: A clinician’s guide to understanding the bone-glucose interplay. Diabetologia 2024, 67, 1493–1506. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Oei, L.; Zillikens, M.C.; Dehghan, A.; Buitendijk, G.H.S.; Castaño-Betancourt, M.C.; Estrada, K.; Stolk, L.; Oei, E.H.G.; van Meurs, J.B.J.; Janssen, J.A.M.J.L.; et al. High bone mineral density and fracture risk in type 2 diabetes as skeletal complications of inadequate glucose control: The Rotterdam Study. Diabetes Care 2013, 36, 1619–1628. [Google Scholar] [CrossRef]
- Trandafir, A.-I.; Sima, O.-C.; Gheorghe, A.-M.; Ciuche, A.; Cucu, A.-P.; Nistor, C.; Carsote, M. Trabecular Bone Score (TBS) in Individuals with Type 2 Diabetes Mellitus: An Updated Review. J. Clin. Med. 2023, 12, 7399. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP Cohort Study Checklist. 2018. Available online: https://casp-uk.net/casp-tools-checklists/cohort-study-checklist/ (accessed on 1 March 2025).
- The Nordic Cochrane Centre. Review Manager (RevMan) [Computer Program]; Version 5.3; The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, Denmark, 2014. [Google Scholar]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Hoboken, NJ, USA, 2009. [Google Scholar]
- Dennison, E.M.; Syddall, H.E.; Aihie Sayer, A.; Craighead, S.; Phillips, D.I.W.; Cooper, C. Type 2 diabetes mellitus is associated with increased axial bone density in men and women from the Hertfordshire Cohort Study: Evidence for an indirect effect of insulin resistance? Diabetologia 2004, 47, 1963–1968. [Google Scholar] [CrossRef]
- Mitama, Y.; Fujiwara, S.; Yoneda, M.; Kira, S.; Kohno, N. Association of type 2 diabetes and an inflammatory marker with incident bone fracture among a Japanese cohort. J. Diabetes Investig. 2017, 8, 709–715. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, L.; Zhao, K.; Zha, X.; Ran, L.; Su, H.; Yang, Y.; Shuang, Q.; Liu, Y.; Xu, L.; Blake, G.M.; et al. Hyperglycemia Is Not Associated With Higher Volumetric BMD in a Chinese Health Check-up Cohort. Front. Endocrinol. 2022, 12, 794066. [Google Scholar] [CrossRef] [PubMed]
- Bonds, D.E.; Larson, J.C.; Schwartz, A.V.; Strotmeyer, E.S.; Robbins, J.; Rodriguez, B.L.; Johnson, K.C.; Margolis, K.L. Risk of fracture in women with type 2 diabetes: The Women’s Health Initiative Observational Study. J. Clin. Endocrinol. Metab. 2006, 91, 3404–3410. [Google Scholar] [CrossRef] [PubMed]
- Heilmeier, U.; Joseph, G.B.; Pasco, C.; Dinh, N.; Torabi, S.; Darakananda, K.; Youm, J.; Carballido-Gamio, J.; Burghardt, A.J.; Link, T.M.; et al. Longitudinal Evolution of Bone Microarchitecture and Bone Strength in Type 2 Diabetic Postmenopausal Women With and Without History of Fragility Fractures-A 5-Year Follow-Up Study Using High Resolution Peripheral Quantitative Computed Tomography. Front. Endocrinol. 2021, 12, 599316. [Google Scholar] [CrossRef]
- Iki, M.; Fujita, Y.; Kouda, K.; Yura, A.; Tachiki, T.; Tamaki, J.; Winzenrieth, R.; Sato, Y.; Moon, J.-S.; Okamoto, N.; et al. Hyperglycemia is associated with increased bone mineral density and decreased trabecular bone score in elderly Japanese men: The Fujiwara-kyo osteoporosis risk in men (FORMEN) study. Bone 2017, 105, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Jawhar, D.S.; Hassan, N.A.; Shamssain, M.H. Dual-energy x-ray absorptiometry scan (DXA) findings in diabetic and non-diabetic female: A retrospective cohort study. Med. J. Malays. 2020, 75, 47–51. [Google Scholar]
- Pritchard, J.M.; Giangregorio, L.M.; Atkinson, S.A.; Beattie, K.A.; Inglis, D.; Ioannidis, G.; Gerstein, H.; Punthakee, Z.; Adachi, J.D.; Papaioannou, A. Changes in trabecular bone microarchitecture in postmenopausal women with and without type 2 diabetes: A two year longitudinal study. BMC Musculoskelet. Disord. 2013, 14, 114. [Google Scholar] [CrossRef]
- Van Hulten, V.; Driessen, J.H.M.; Andersen, S.; Kvist, A.; Viggers, R.; Bliuc, D.; Center, J.R.; Brouwers, M.C.J.G.; Vestergaard, P.; van den Bergh, J.P. Fracture risk revisited: Bone mineral density T-score and fracture risk in type 2 diabetes. Diabetes Obes. Metab. 2024, 26, 5325–5335. [Google Scholar] [CrossRef]
- Sosa, M.; Saavedra, P.; Jódar, E.; Lozano-Tonkin, C.; Quesada, J.M.; Torrijos, A.; Pérez-Cano, R.; Nogués, X.; Díaz-Curiel, M.; Moro, M.J.; et al. Bone mineral density and risk of fractures in aging, obese post-menopausal women with type 2 diabetes. The GIUMO Study. Aging Clin. Exp. Res. 2009, 21, 27–32. [Google Scholar] [CrossRef]
- Sihota, P.; Yadav, R.N.; Dhaliwal, R.; Bose, J.C.; Dhiman, V.; Neradi, D.; Karn, S.; Sharma, S.; Aggarwal, S.; Goni, V.G.; et al. Investigation of Mechanical, Material, and Compositional Determinants of Human Trabecular Bone Quality in Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2021, 106, e2271–e2289. [Google Scholar] [CrossRef]
- La Fontaine, J.; Shibuya, N.; Sampson, H.W.; Valderrama, P. Trabecular quality and cellular characteristics of normal, diabetic, and charcot bone. J. Foot Ankle Surg. 2011, 50, 648–653. [Google Scholar] [CrossRef]
- Li, T.; Hu, L.; Yin, X.-L.; Zou, Y.; Fu, H.-Y.; Li, H.-L. Prevalence and Risk Factors of Osteoporosis in Patients with Type 2 Diabetes Mellitus in Nanchang (China): A Retrospective Cohort Study. Diabetes Metab. Syndr. Obes. Targets Ther. 2022, 15, 3039–3048. [Google Scholar] [CrossRef] [PubMed]
- Starr, J.F.; Bandeira, L.C.; Agarwal, S.; Shah, A.M.; Nishiyama, K.K.; Hu, Y.; McMahon, D.J.; Guo, X.E.; Silverberg, S.J.; Rubin, M.R. Robust Trabecular Microstructure in Type 2 Diabetes Revealed by Individual Trabecula Segmentation Analysis of HR-pQCT Images. J. Bone Miner. Res. 2018, 33, 1665–1675. [Google Scholar] [CrossRef] [PubMed]
- Patsch, J.M.; Burghardt, A.J.; Yap, S.P.; Baum, T.; Schwartz, A.V.; Joseph, G.B.; Link, T.M. Increased cortical porosity in type 2 diabetic postmenopausal women with fragility fractures. J. Bone Miner. Res. 2013, 28, 313–324. [Google Scholar] [CrossRef]
- Wallander, M.; Axelsson, K.F.; Nilsson, A.G.; Lundh, D.; Lorentzon, M. Type 2 diabetes and risk of hip fractures and non-skeletal fall injuries in the elderly: A study from the fractures and fall injuries in the elderly cohort (FRAILCO). J. Bone Miner. Res. 2016, 32, 449–460. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient/Population | Outcomes | Study Design | Combining Search Terms |
|---|---|---|---|
| Type 2 diabetes or type 2 diabetes mellitus or t2dm | Bone mineral density or BMD or trabecular score or bone quality or fracture risk assessment | Cohort study or longitudinal study or observational study | Column 1 and Column 2 and Column 3 |
| Citation/Country of Study and Year | Type of Study | Aim | Participants | Sample Size | Mean Age (Years) | Results/Findings |
|---|---|---|---|---|---|---|
| Bonds et al. [25] USA | Prospective cohort | To determine the risk of fracture in postmenopausal women with type 2 diabetes and determine whether risk varies by fracture site, ethnicity, and baseline bone density. | Postmenopausal women with T2D | Participants with T2D n = 5285 Control = n = 88,120 | T2D 64.9 ± 7.0 Control = 63.5 ± 7.4 | With fracture by location, women with diabetes had higher fracture rates at multiple sites (hip, pelvis, upper leg; lower leg, ankle, knee; foot; upper arm, shoulder, elbow; and spine and tailbone fractures (p < 0.0001)). The rate of fractures to the lower arm, wrist, and hand were equal in both groups. An elevated risk of fracture at multiple sites (hip, pelvis, upper leg; spine and tailbone) was reported among black women with diabetes (RR 1.33, 95% CI 1.00 –1.75) and compared with NHW women who have diabetes (RR 1.18, 95% CI 1.08–1.29). |
| Dennison et al. [22] UK | Hertfordshire Cohort | To explore whether the high bone density observed in Type 2 diabetes may be a result of the indirect effect of insulin resistance. | Men and women with T2D | Total n = 909 Men n = 465 Women n = 444 | Men 64.8 ± 2.6 Women 66.4 ± 2.6 Men diagnosed as T2D n = 33 Women n = 32 diagnosed as T2D | Bone density was higher in newly diagnosed diabetic subjects, with relationships stronger in women (p < 0.001) than men (p < 0.05) and attenuated by adjustment for body mass index. In both sexes, positive correlations were observed between the total femur and femoral neck BMD with measures of insulin resistance (r = 0.17–0.22), with stronger results observed in women. |
| Heilmeier et al. [26] USA | Prospective cohort (Longitudinal cohort study) | To prospectively characterise the 5-year longitudinal changes in bone microarchitecture and strength in T2D postmenopausal women with and without a history of fragility fractures and to compare their changes to non-diabetic healthy postmenopausal controls using HR-pQCT. | Post-menopausal women with T2D | n = 32 women with T2D n = 10 Control n = 12 DMFx n = 10 | DM 59.0 ± 4.1 Control 58.9 ± 5.5 | The control group exhibited significant decreases in total BMD (−3.8%, Tt.BMD, p = 0.001) and Ct.Ar (−3.9% Ct.Ar, p = 0.007), and a significant increase in cortical pore diameter (Co: +8.8% Ct.Po.Dm, p = 0.007). In both the control and T2D groups there was a significant decrease in trabecular number (Tb.N) accompanied by a significant increase in trabecular thickness and trabecular spacing (control: +8.8% Tb.Th, p = 0.024, + 7.5% Tb.Sp, p = 0.017; DM: +8.4% Tb.Th, p = 0.039, 6.0% Tb.Sp, p = 0.032). |
| Iki et al. [27] Japan | Prospective cohort | To clarify associations between glycemic and insulin-resistance indices and TBS in community-dwelling elderly Japanese men, and whether pentosidine, an AGE, and bone turnover marker levels affect these associations. | Elderly Japanese men with T2D | Total n = 1683 Men with T2D n = 313 Control n = 1370 | DM 72.8 ± 5.2 Control 72.9 ± 5.1 | Men with T2D weighed significantly more and had a significantly higher aBMD compared to those without T2D. There was no significant difference in TBS and the frequency of past osteoporotic fractures between the two groups. Hyperglycaemia and elevated insulin resistance were associated with low TBS independently of bone turnover and pentosidine levels. |
| Jawhar et al. [28] United Arab Emirates (UAE) | Retrospective cohort | To assess the association between osteoporosis and T2D in females, with an emphasis on the identification of the major characteristics of BMD, T-score, and Z-score in female diabetic patients. | Women with T2D | Total n = 568 Pre- and postmenopausal women with diabetes n =141 Control n = 428 | T2D 63.55 ± 9.15 Control 58.88 ± 11.71 | The prevalence of osteoporosis was significantly higher (p ≤ 0.01) in the diabetic group. Younger diabetic patients (40–49 years) had significantly higher values (p ≤ 0.05) of BMD, T-score, and Z-score in the left femur and total hip. Diabetic patients in the age range of 50–59 years have significantly higher values of BMD and Z-score in the L3 region of the spine than other groups. Women who are obese have a significantly higher (p ≤ 0.001) BMD than non-obese women in the diabetes and control groups. |
| Mitama et al. [23] Japan | Cohort | To evaluate the combined effect of diabetes mellitus and one inflammatory marker (high-sensitive C-reactive protein [hs-CRP]) on the risk of incident fracture in a large-scale Japanese cohort. | Men and women with T2D | Men with T2D n = 413 Control n = 2110 Women with T2D n = 379 Control n = 3005 | Men with T2D 68.2 ± 6.4 Control 67.6 ± 6.7 Women with T2D 7.3 ± 1.2 Control 68.0 ± 7.6 | For both men and women, ageing, low BMD, previous fractures, and high CRP had significant associations with fracture. Fracture risk was significantly higher among the diabetes mellitus with high CRP group compared with the non-diabetes mellitus with low CRP group. |
| Oei et al. [16] The Netherlands | Prospective population-based cohort | To investigate if the intricate relationships between BMD, bone geometry, and fractures in type 2 diabetes are influenced by glucose control. | T2D | Total n = 4135 Non-diabetic (ND), adequately controlled diabetes (ACD) Inadequately controlled diabetes (ICD) (ICD) n = 217 Control (ACD) n = 203 (ND n = 3715) | ICD 68.5 ± 7.8 ACD Control 71.9 ± 7.6 | Those with diabetes were older, had higher BMI, serum insulin, and creatinine levels, and used diuretics more frequently than those in the non-diabetes group. Participants with ICD had a higher fracture risk than individuals without diabetes. Poor glycaemic control in T2D is associated with fracture risk, high BMD, and thicker femoral cortices in narrower bones. |
| Pritchard et al. [29] Canada | Prospective cohort | To compare two-year changes in trabecular bone microarchitecture in women with and without type 2 diabetes. | Postmenopausal women with T2D | Women with T2D at baseline n = 30 Control n = 30 At follow-up with T2D n = 15 Control n = 22 | Baseline women with T2D 71.1 ± 4.8 Control 70.7 ± 4.9 T2D 73.9 ± 3.6 Control 72.5 ± 4.9 | At both the baseline and follow-up points, lumbar spine BMD was greater (p < 0.05) for women with diabetes than without diabetes. There were no differences in the change in other trabecular bone microarchitecture variables between groups. |
| Wang et al. [24] China | Prospective cohort | To investigate the association of vBMD and fasting plasma glucose in a large cohort of Chinese subjects and compare the vBMD in healthy and diabetic subjects. To compare the relationships between aBMD, vBMD, glucose, and fat mass in a subset of a Chinese cohort. | Men and women with diabetes | Total Men, n = 593 Women n = 444 Men with T2D n = 80 Control n = 513 Women with T2D n = 32 Control n = 412 | Men with T2D 54.7 ± 10.3 Control 49.9 ± 9.6 Women with T2D 61.2 ± 9.7 Control 52.0 ± 9.9 | Both men and women with diabetes were significantly older (p < 0.001). Both had a higher BMI than the non-diabetes women. Both women and men with diabetes had a lower vBMD compared to non-diabetic subjects, but this was non-significant after adjusting for age. In the DXA sub-cohort, aBMD was significantly higher in men with diabetes after adjusting for age. |
| Van Hulten et al. [30] Denmark | Retrospective cohort | To study the association between femoral neck (FN) bone mineral density (BMD), T-score, and fracture risk in individuals with and without type 2 diabetes (T2D). | Men and women with T2D | Total: Men n = 7069 Men with T2D n = 758 Control n = 6311 Women n = 35,129 Women with T2D n = 2362 Control n = 32,767 | Men with T2D 68.5 ± SD 10.6 Control 65.4 ± 13.0 Women with T2D 70.0 ± 10.6 Control 65.5 ± 12.1 | Crude IRs for hip fractures, non-spine fractures, and MOFs were not significantly different in women (age > 30) with T2D not using insulin (IR hip: 8.7; 95% CI 6.8–11.0) or using insulin (IR hip: 11.1; 95% CI 6.8–18.0) compared with women without T2D (IR hip: 7.0; 95% CI 6.6–7.4). For all three fracture types, IRs were not significantly different in men with T2D not using insulin (IR hip: 4.6; 95% CI 2.6–8.0) or using insulin (IR hip: 11.5; 95% CI 6.2–21.4) compared with men without T2D (IR hip: 6.3; 95% CI 5.5–7.1) |
| Citation/Country of Study and Year | Duration of Diabetes (Yrs) | Glycaemic Control Measures | Potential Confounding Medications |
|---|---|---|---|
| Bonds et al. [25] USA | 9.3 ± 10.0 | Insulin usage (16.7%) | Some of the participants included in the study were on: Vitamin D; Oestrogen; Bisphosphonates; Steroids; Thiazide diuretics; Statins; Thyroid hormones. |
| Dennison et al. [22] UK | Not Reported | Not Reported | Participants on medications that alter bone metabolism (such as bisphosphonates) were excluded from the study, while women on hormone replacement therapy were included. |
| Heilmeier et al. [26] USA | 64.4 ± 4.2 | Not Reported | Exclusion criteria included the chronic (>6 months) use of bone-affecting medications (the intake of oestrogens, adrenal or anabolic steroids, antacids, anticoagulants, anticonvulsants, pharmacological doses of Vitamin A, fluorides, bisphosphonates, calcitonin, tamoxifen, parathyroid hormone [PTH], or thiazolidinediones). |
| Iki et al. [27] Japan | A median duration of disease of 10.5 years | Thiazolidinediones and other anti-diabetic drugs | Participants on medications known to affect bone metabolism (such as medications for uncontrolled hyperthyroid disease, parathyroid disease, type 1 diabetes, connective tissue disease, gastrectomy due to cancer or ulcer, prostate cancer with anti-androgen therapy, oral glucocorticoid therapy at any dose, bisphosphonate therapy for >6 months, and activated vitamin D use for >2 years) were excluded from the study. |
| Jawhar et al. [28] United Arab Emirates (UAE) | Not Reported | Oral antidiabetic medications (Not specified) | Not Reported |
| Mitama et al. [23] Japan | Not Reported | Not Reported | Participants who were under treatment for osteoporosis, rheumatoid arthritis, collagen diseases, and other inflammatory diseases were excluded from the study. |
| Oei et al. [16] The Netherlands | Not Reported | Insulin and antidiabetic medications (not specified) | Information on medication use included the use of antidiabetic medication, diuretics, hormonal replacement therapy, and systemic corticosteroids. |
| Pritchard et al. [29] Canada | ≥5 years; At follow-up, women with type 2 diabetes had a diagnosis of diabetes for 18.8 ± 9.7 years. | At follow-up, the majority of participants (12/15 [80.0%]) were taking insulin or insulin in combination with another glucose-lowering intervention. The remaining participants were either taking metformin (2/15 [13.3%]) or no medication (1/15 [6.7%]). | Participants who were taking, or had taken in the past 24 months, any medication known to affect bone, including hormone therapy, calcitonin, selective oestrogen receptor modulator, parathyroid hormone, or bisphosphonate, or were taking oral glucocorticoids (≥2.5 mg/day for ≥3 months) were excluded from the study. |
| Wang et al. [24] China | Not Reported | Information on antidiabetic medication was restricted to insulin and/or oral antidiabetic medications or no medication use. | Not Reported |
| Van Hulten et al. [30] Denmark | 6.1 ± 4.8 | Glucagon-like peptide-1 receptor agonists Insulin Sodium glucose cotransporter 2 inhibitor Sulphonylurea Dipeptidyl-peptidase 4 inhibitor Thiazolidinediones Non-insulin antidiabetic drug | The use of the following medications in the 6 months before the index date was considered a potential cofounder: codeine, opioids, antidepressants, nitrates, loop diuretics, antipsychotics, anti-Parkinson medication, hormone replacement therapy, histamine type-2 receptor antagonists and proton pump inhibitors, anticonvulsants, statins, anti-osteoporotic medication, and corticosteroids. |
| Patients with Type 2 Diabetes | ||||||
|---|---|---|---|---|---|---|
| Outcomes |
Number of Studies or Gender |
Number of Participants |
Statistical Method | Weighted Difference (95% CI) | p-Value | I2 % |
| Trabecular Bone Mineral Density | 1 | 22 | Mean Difference | 2.04 [−1.28, 5.36] | p = 0.23 | |
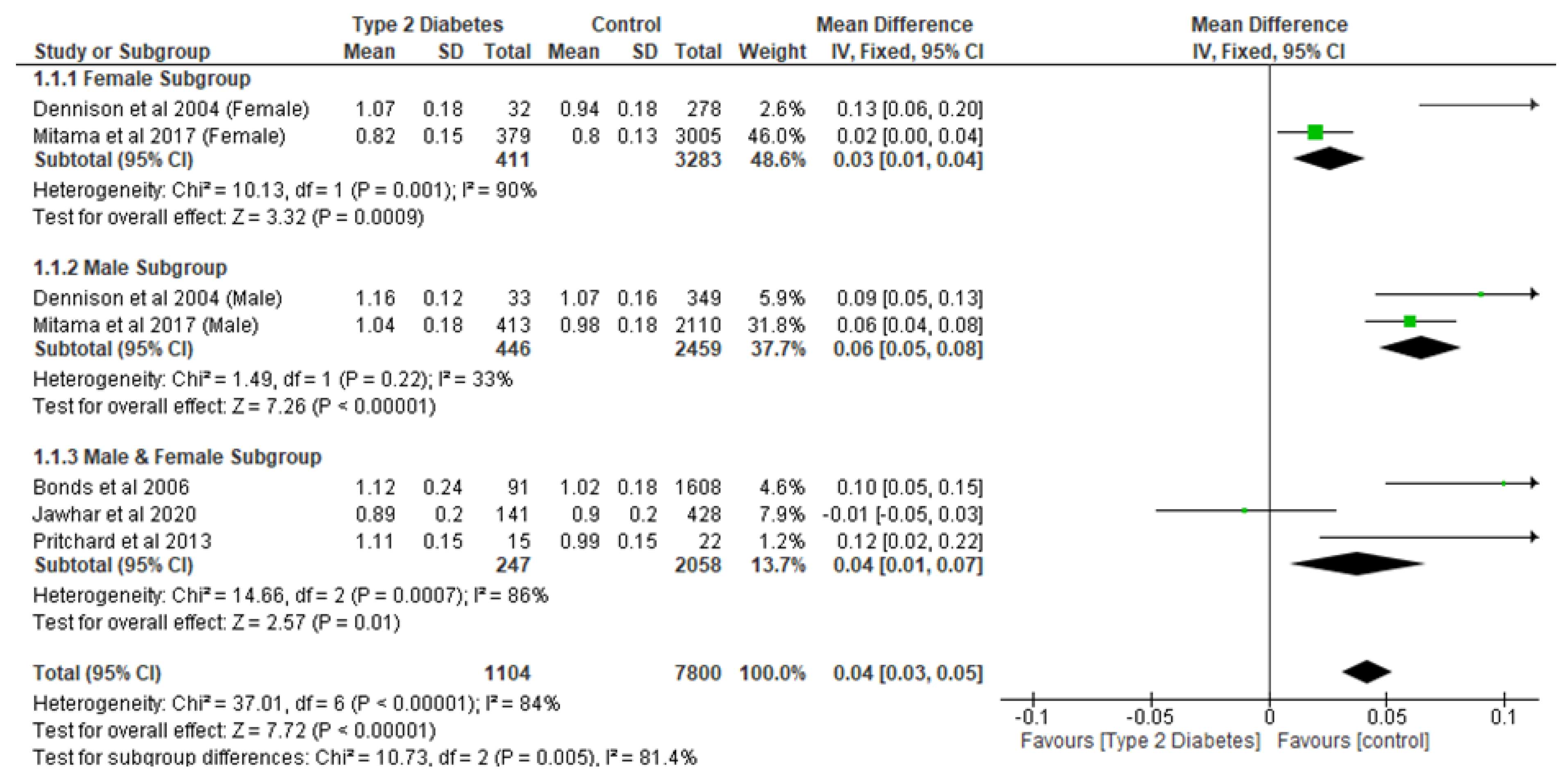
| Areal Bone Mineral Density | 2 | 1037 | Mean Difference | −0.01 [−0.04, 0.02] | p = 0.51 | 95 |
| Total Bone Mineral Density | 1 | 22 | Mean Difference | 5.33 [−1.20, 11.86] | p = 0.11 | |
| Incidence of Non-Spine Fracture | 2 | 6731 | Mean Difference | −0.31 [−3.97, 3.36] | p = 0.87 | 78 |
| Hole Size | 1 | 35 | Mean Difference | −0.04 [−0.31, 0.23] | p = 0.77 | |
| Number of Holes | 1 | 35 | Mean Difference | 1.00 [−9.28, 11.28] | p = 0.85 | |
| Bone Volume Fraction | 1 | 35 | Mean Difference | 0.10 [−0.50, 0.70] | p = 0.74 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ojo, O.; Onilude, Y.; Brooke, J.; Apau, V.; Kazangarare, I.; Ojo, O. The Effect of Type 2 Diabetes on Bone Quality: A Systematic Review and Meta-Analysis of Cohort Studies. Int. J. Environ. Res. Public Health 2025, 22, 910. https://doi.org/10.3390/ijerph22060910
Ojo O, Onilude Y, Brooke J, Apau V, Kazangarare I, Ojo O. The Effect of Type 2 Diabetes on Bone Quality: A Systematic Review and Meta-Analysis of Cohort Studies. International Journal of Environmental Research and Public Health. 2025; 22(6):910. https://doi.org/10.3390/ijerph22060910
Chicago/Turabian StyleOjo, Omorogieva, Yemi Onilude, Joanne Brooke, Victoria Apau, Ivy Kazangarare, and Osarhumwese Ojo. 2025. "The Effect of Type 2 Diabetes on Bone Quality: A Systematic Review and Meta-Analysis of Cohort Studies" International Journal of Environmental Research and Public Health 22, no. 6: 910. https://doi.org/10.3390/ijerph22060910
APA StyleOjo, O., Onilude, Y., Brooke, J., Apau, V., Kazangarare, I., & Ojo, O. (2025). The Effect of Type 2 Diabetes on Bone Quality: A Systematic Review and Meta-Analysis of Cohort Studies. International Journal of Environmental Research and Public Health, 22(6), 910. https://doi.org/10.3390/ijerph22060910