
Increased Risk of Hospitalization for Lower Respiratory Tract Illness (LRTI) in the Elderly Living in Communities near a Newly Established Industrial Estate in Central Thailand

 , ,
, ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Hospitalization Data
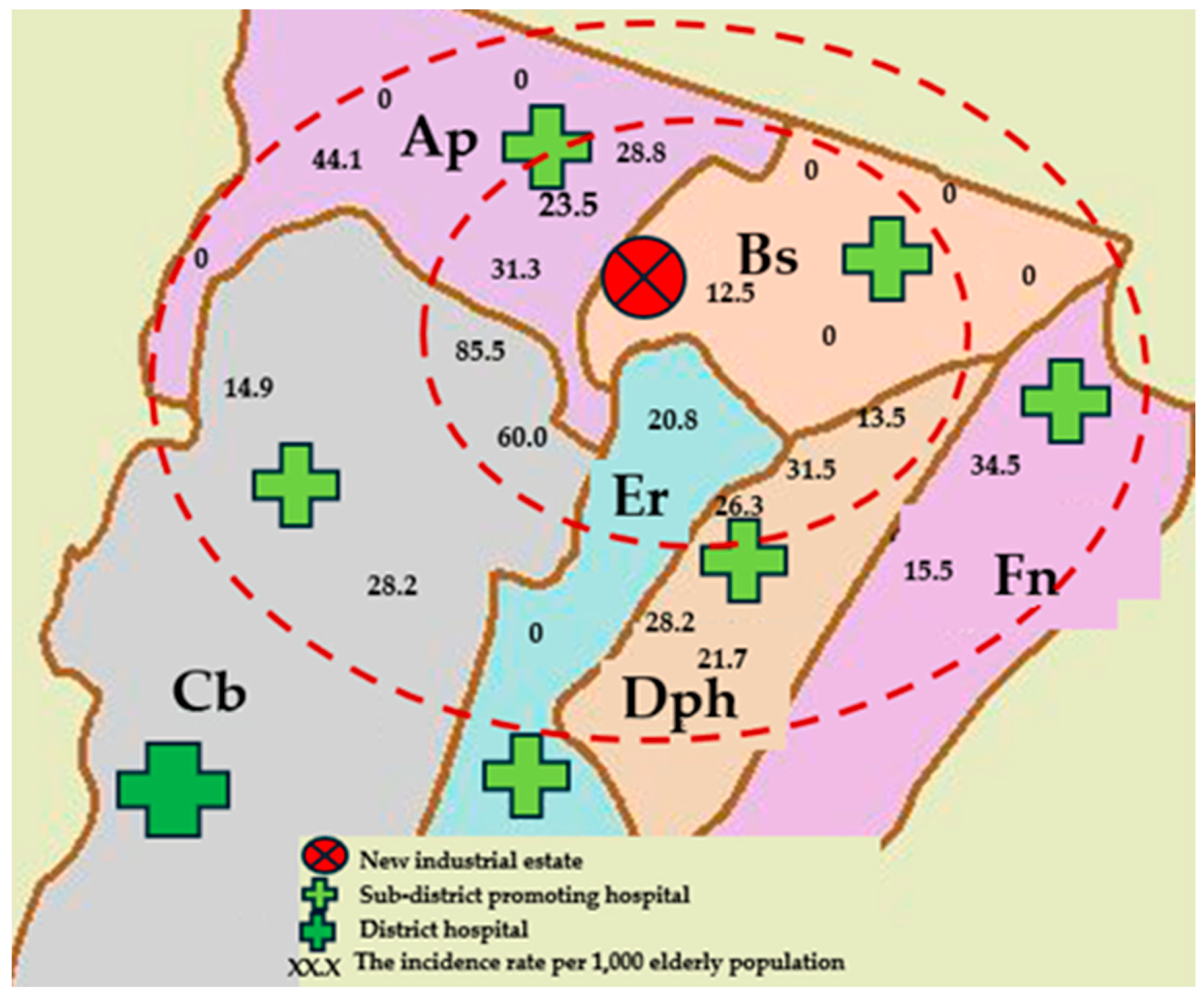
2.2. Study Area: Communities near a New Industrial Estate
2.3. Measurement of Air Pollutants
2.4. Statistical Data Analysis
2.5. Ethics Statement
3. Results
3.1. Study Area and Measured Air Pollutants
3.2. Descriptive Statistics of the Study Population
3.3. The Association Between the Incidence of LRTI Among Elderly People and Living in Communities near the New Industrial Estate
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, Y.; Song, P.; Lin, S.; Peng, L.; Li, Y.; Deng, Y.; Deng, X.; Lou, W.; Yang, S.; Zheng, Y.; et al. Global Burden of Respiratory Diseases Attributable to Ambient Particulate Matter Pollution: Findings From the Global Burden of Disease Study 2019. Front. Public Health 2021, 9, 740800. [Google Scholar] [CrossRef] [PubMed]
- Baptista, E.A.; Dey, S.; Pal, S. Chronic respiratory disease mortality and its associated factors in selected Asian countries: Evidence from panel error correction model. BMC Public Health 2021, 21, 53. [Google Scholar] [CrossRef] [PubMed]
- Requia, W.J.; Adams, M.D.; Koutrakis, P. Association of PM2.5 with diabetes, asthma, and high blood pressure incidence in Canada: A spatiotemporal analysis of the impacts of the energy generation and fuel sales. Sci. Total Environ. 2017, 584–585, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Luong, L.T.M.; Dang, T.N.; Thanh Huong, N.T.; Phung, D.; Tran, L.K.; Van Dung, D.; Thai, P.K. Particulate air pollution in Ho Chi Minh city and risk of hospital admission for acute lower respiratory infection (ALRI) among young children. Environ. Pollut. 2019, 257, 113424. [Google Scholar] [CrossRef]
- García-Pérez, J.; Fernández de Larrea-Baz, N.; Lope, V.; Molina, A.J.; O’Callaghan-Gordo, C.; Alonso, M.H.; Rodríguez-Suárez, M.M.; Mirón-Pozo, B.; Alguacil, J.; Gómez-Acebo, I.; et al. Residential proximity to industrial pollution sources and colorectal cancer risk: A multicase-control study (MCC-Spain). Environ. Int. 2020, 144, 106055. [Google Scholar] [CrossRef]
- Brooks, N.; Biswas, D.; Hossin, R.; Yu, A.; Saha, S.; Saha, S.; Saha, S.K.; Luby, S.P. Health consequences of small-scale industrial pollution: Evidence from the brick sector in Bangladesh. World Dev. 2023, 170, 106318. [Google Scholar] [CrossRef]
- Bano, R.; Khayyam, U. Industrial air pollution and self-reported respiratory and irritant health effects on adjacent residents: A case study of Islamabad Industrial Estate (IEI). Air Qual. Atmos. Health 2021, 14, 1709–1722. [Google Scholar] [CrossRef]
- Chang, W.-W.; Boonhat, H.; Lin, R.-T. Incidence of Respiratory Symptoms for Residents Living Near a Petrochemical Industrial Complex: A Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 2474. [Google Scholar] [CrossRef]
- Herrera, R.; Radon, K.; von Ehrenstein, O.S.; Cifuentes, S.; Muñoz, D.M.; Berger, U. Proximity to mining industry and respiratory diseases in children in a community in Northern Chile: A crosssectional study. Environ. Health 2016, 15, 66. [Google Scholar] [CrossRef]
- Baptista, E.A.; Dey, S.; Pal, S. The effect of industry-related air pollution on lung function and respiratory symptoms in school children. Environ. Health 2018, 17, 30. [Google Scholar]
- Isa, K.N.M.; Som, N.A.N.M.; Jalaludin, J.; Hashim, N.H. Effects of Residential Proximity to Industrial Zone on Respiratory Symptoms among Residents in Parit Raja, Batu Pahat. Malays. J. Med. Health Sci. 2024, 20, 168–174. [Google Scholar]
- Yamsrual, S.; Sasaki, N.; Tsusaka, T.W.; Winijkul, E. Assessment of local perception on eco-industrial estate performances after 17 years of implementation in Thailand. Environ. Dev. 2019, 32, 100457. [Google Scholar] [CrossRef]
- Sillapapiromsuk, S.; Koontoop, G.; Bootdee, S. Health Risk Assessment of Ambient Nitrogen Dioxide Concentrations in Urban and Industrial Area in Rayong Province, Thailand. Trends Sci. 2022, 19, 4476. [Google Scholar] [CrossRef]
- Muenmee, S.; Bootdee, S. Health risk assessment of exposure PM2.5 from industrial area in Pluak Daeng district, Rayong province. Naresuan Phayao J. 2021, 14, 95–110. [Google Scholar]
- Thongsaeng, P.; Karuchit, S.; Pongkiatkul, P. Concentration and chemical composition of PM2.5 in Nakhon Ratchasima city. Eng. J. Res. Dev. 2018, 30, 145–155. [Google Scholar]
- Phantu, S.; Kaenbubpha, K.; Ployprom, N.; Bootdee, S. Health Risk Assessment of PM2.5 exposure in Dry season from Map Ta Phut Town Municility in Rayong Province. J. Sci. Technol. Nakhon Sawan Rajabhat Univ. 2022, 19, 64–82. [Google Scholar]
- Asa, P.; Jinsart, W. Effects of Air Pollution Related Respiratory Symptoms in Schoolchildren in Industrial Areas Rayong, Thailand. Environ. Asia 2016, 9, 116–123. [Google Scholar]
- Polluton Control Department. The state of Air and Noise Pollution in Thailand 2021; Ministry of Natural Resoures and Environment: Bangkok, Thailand, 2021; pp. 5–15. ISBN 978-616-316-726-2.
- Pollution Control Department. Thailand State of Pollution Report 2023; Ministry of Natural Resoures and Environment: Bangkok, Thailand, 2024; pp. 98–120. ISBN 978-616-316-778-1.
- Watson, A.; Wilkinson, T.M.A. Respiratory viral infections in the elderly. Ther. Adv. Respir. Dis. 2021, 15, 1–17. [Google Scholar] [CrossRef]
- National Statistical Office. Summary of the Performance of the Elderly in Thailand 2023; National Statistical Office of Thailand: Bangkok, Thailand, 2024.
- The U.S. Environmental Protection Agency. 40 CFR Part 50, Appendix L—Reference Method for the Determination of Fine Particulate Matter as PM2.5 in the Atmosphere; The U.S. Environmental Protection Agency: Washington, DC, USA, 1997.
- The U.S. Environmental Protection Agency. 40 CFR Part 50—National Ambient Air Quality Standards for Particulate Matter; The U.S. Environmental Protection Agency: Washington, DC, USA, 2019.
- Jawjit, S.; Pibul, P.; Muenrach, N.; Kuakul, A. Risk Assessment of PM10 Exposure of Stone Crushing Plant Nearby and Further Communities in Nakhon Si Thammarat. J. Sci. Technol. 2018, 27, 335–348. [Google Scholar]
- Tantipanjaporn, T.; Srisakultiew, N.; Sukhantho, B. Health Risk Assessment of Inhalation Exposure to Respirable Dust among Workers in a Rice Mill in Kamphaeng Phet Province. Srinagarind Med. J. 2019, 34, 482–489. [Google Scholar]
- Chang, Q.; Zhang, H.; Zhao, Y. Ambient air pollution and daily hospital admissions for respiratory system–related diseases in a heavy polluted city in Northeast China. Environ. Sci. Pollut. Res. 2020, 27, 10055–10064. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.K.; Romeiko, X.X.; Zhang, W.; Feingold, B.J.; Khwaja, H.A.; Zhang, X.; Lin, S. Residential Proximity to Biorefinery Sources of Air Pollution and Respiratory Diseases in New York State. Environ. Sci. Technol. 2021, 55, 10035–10045. [Google Scholar] [CrossRef]
- Wang, M.; Muraki, I.; Liu, K.; Shirai, K.; Tamakoshi, A.; Hu, Y.; Iso, H. Diabetes and Mortality From Respiratory Diseases: The Japan Collaborative Cohort Study. J. Epidemiol. 2020, 30, 457–463. [Google Scholar] [CrossRef] [PubMed]
- George, C.; Ducatman, A.M.; Conway, B.N. Increased risk of respiratory diseases in adults withType 1 and Type 2 diabetes. Diabetes Res. Clin. Pract. 2018, 142, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Do, J.; Park, C.-H.; Lee, Y.-T.; Yoon, K.J. Association between underweight and pulmonary function in 282,135 healthy adults: A cross-sectional study in Korean population. Sci. Rep. 2019, 9, 14308. [Google Scholar] [CrossRef]
- Farihah Mohmad Shamsuddin, A.; Jalaludin, J.; Haslina Hashim, N. Exposure to industrial air pollution and its association with respiratory symptoms among children in Parit Raja, Batu Pahat. Earth Environ. Sci. 2022, 1013, 012008. [Google Scholar] [CrossRef]
- Chen, T.; Chen, F.; Wang, K.; Ma, X.; Wei, X.; Wang, W.; Huang, P.; Yang, D.; Xia, Z.; Zhao, Z. Acute respiratory response to individual particle exposure (PM1.0, PM2.5 and PM10) in the elderly with and without chronic respiratory diseases. Environ. Pollut. 2021, 271, 116329. [Google Scholar] [CrossRef]
- Wang, M.; Fang, H. The effect of health education on knowledge and behavior toward respiratory infectious diseases among students in Gansu, China: A quasi-natural experiment. BMC Public Health 2020, 20, 681. [Google Scholar] [CrossRef]

{kind=link}
| PM2.5 | NO2 | |||||||
|---|---|---|---|---|---|---|---|---|
| Distance | Min | Median | Mean (SD) | Max | Min | Median | Mean (SD) | Max |
| Near (0–3 km) | ||||||||
| Ap | 23.1 | 34.3 | 32.5 (6.8) | 41.4 | 0.004 | 0.005 | 0.005 (0.0002) | 0.005 |
| Bs | 17.5 | 41.6 | 38.8 (10.1) | 49.4 | 0.012 | 0.013 | 0.013 (0.0003) | 0.013 |
| Far (>3–5 km) | ||||||||
| Cb | 29.9 | 34.6 | 38.3 (7.6) | 50.9 | 0.004 | 0.004 | 0.004 (0.0005) | 0.005 |
| Dph | 32.6 | 41.3 | 44.6 (10.7) | 58.5 | 0.002 | 0.002 | 0.002 (0.0004) | 0.003 |
| Factors | Entire Region (n = 2799) | Subregion (n = 1347) | ||
|---|---|---|---|---|
| Number | Percentage (%) | Number | Percentage (%) | |
| LRTI | ||||
| No | 2733 | 97.64 | 1305 | 96.88 |
| Yes | 66 | 2.36 | 42 | 3.12 |
| Gender | ||||
| Female | 1522 | 54.38 | 745 | 55.31 |
| Male | 1277 | 45.62 | 602 | 44.69 |
| Age (years) | ||||
| 60–69 | 1656 | 59.16 | 776 | 57.61 |
| 70–79 | 721 | 25.76 | 344 | 25.54 |
| ≥80 | 422 | 15.08 | 227 | 16.85 |
| Mean (±SD) | 69.48 (±8.36) | 69.71 (±8.43) | ||
| Median (Min:Max) | 67 (60:113) | 68 (60:97) | ||
| BMI (kg/m2) | ||||
| Normal weight (18.50–22.99 kg/m2) | 1187 | 68.66 | 660 | 49.00 |
| Underweight (<18.50 kg/m2) | 152 | 10.66 | 124 | 9.20 |
| Overweight (≥23.00 kg/m2) | 460 | 20.66 | 563 | 41.80 |
| Mean (±SD) | 22.84 (±2.84) | 22.73 (±3.61) | ||
| Median (Min:Max) | 23.11 (10.59:41.87) | 22.35 (10.59:41.87) | ||
| Chronic disease | ||||
| N/A | 1428 | 51.02 | 0 | 0 |
| Any chronic disease | 1043 | 37.26 | 1043 | 77.43 |
| Hypertension | 104 | 3.72 | 94 | 6.98 |
| Diabetes | 89 | 3.18 | 82 | 6.09 |
| Education level | ||||
| N/A | 1428 | 51.02 | 0 | 0 |
| Primary school | 1305 | 46.62 | 1284 | 95.32 |
| Higher than primary school | 66 | 2.07 | 63 | 4.68 |
| Occupation | ||||
| N/A | 1428 | 51.02 | 0 | 0 |
| None | 1287 | 46.38 | 1287 | 95.55 |
| Farmer | 36 | 1.29 | 36 | 2.67 |
| Laborer | 26 | 0.93 | 12 | 0.89 |
| Other | 4 | 0.14 | 10 | 0.74 |
| Smoking cigarettes | ||||
| N/A | 1428 | 51.02 | 0 | 0 |
| No | 1235 | 44.12 | 1211 | 89.90 |
| Yes (current or previous) | 136 | 4.86 | 136 | 10.10 |
| Drinking alcohol | ||||
| N/A | 1428 | 51.02 | 0 | 0 |
| No | 1235 | 44.12 | 1066 | 79.14 |
| Yes (current or previous) | 136 | 4.86 | 281 | 20.86 |
| PM2.5 average concentration (µg/m3) | ||||
| Low (<37.5 µg/m3) | 698 | 24.95 | 0 | 0 |
| High (≥37.5 µg/m3) | 2101 | 75.05 | 1347 | 100 |
| NO2 average concentration (ppm) | ||||
| Low (<0.17 ppm) | 2799 | 100 | 1347 | 100 |
| High (≥0.17 ppm) | 0 | 0 | 0 | 0 |
| Wind direction | ||||
| Upwind | 687 | 24.54 | 285 | 21.16 |
| Downwind | 2112 | 75.46 | 1062 | 78.84 |
| Distance from home to the new estate | ||||
| Far (>3–5 km) | 1488 | 53.16 | 760 | 56.42 |
| Near (0–3 km) | 1311 | 46.84 | 587 | 43.58 |
| Factors | Number | LRTI | Univariable Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|---|---|---|
| n | n | (%) | OR | 95% CI | p-Value | ORadj | 95% CI | p-Value | |
| Overall | 1347 | 42 | 3.12 | ||||||
| Distance | 0.017 | 0.001 | |||||||
| Far (>3–5 km) | 760 | 16 | 2.11 | 1 | 1 | ||||
| Near (0–3 km) | 587 | 26 | 4.43 | 2.15 | 1.15–4.06 | 3.43 | 1.61–7.36 | ||
| Gender | 0.100 | 0.173 | |||||||
| Female | 745 | 18 | 2.42 | 1 | 1 | ||||
| Male | 602 | 24 | 3.99 | 1.67 | 0.90–3.12 | 1.80 | 0.89–3.67 | ||
| Age (Years) | 0.296 | 0.021 | |||||||
| 60–69 | 776 | 21 | 2.71 | 1 | 1 | ||||
| 70–79 | 344 | 10 | 2.91 | 1.08 | 0.50–2.31 | 0.850 | 1.33 | 0.57–3.07 | |
| ≥80 | 227 | 11 | 4.85 | 1.83 | 0.87–3.86 | 0.112 | 2.50 | 1.02–6.10 | |
| BMI | 0.001 | 0.280 | |||||||
| Normal weight | 660 | 12 | 1.82 | 1 | 1 | ||||
| Underweight | 124 | 11 | 8.87 | 5.25 | 2.26–12.20 | <0.001 | 5.39 | 2.00–14.50 | |
| Overweight | 563 | 19 | 3.37 | 1.88 | 0.90–3.92 | 0.089 | 1.89 | 0.85–4.15 | |
| Education | 0.055 | 0.001 | |||||||
| Primary | 1284 | 37 | 2.88 | 1 | 1 | ||||
| Higher than primary | 63 | 5 | 7.94 | 2.90 | 1.10–7.66 | 3.06 | 0.95–9.91 | ||
| Smoking cigarettes | 0.899 | 0.648 | |||||||
| No | 1211 | 38 | 3.14 | 1 | 1 | ||||
| Yes (current or former) | 136 | 4 | 2.94 | 0.94 | 0.33–2.66 | 1.41 | 0.40–5.01 | ||
| Diabetes | <0.001 | <0.001 | |||||||
| No | 1265 | 22 | 1.74 | 1 | 1 | ||||
| Yes | 82 | 20 | 24.39 | 18.22 | 9.45–5.16 | 33.89 | 15.01–76.05 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wangupadcha, P.; Ronsmans, S.; Vanoirbeek, J.; Limmongkon, Y.; Phokee, W.; Jirapornkul, C. Increased Risk of Hospitalization for Lower Respiratory Tract Illness (LRTI) in the Elderly Living in Communities near a Newly Established Industrial Estate in Central Thailand. Int. J. Environ. Res. Public Health 2025, 22, 874. https://doi.org/10.3390/ijerph22060874
Wangupadcha P, Ronsmans S, Vanoirbeek J, Limmongkon Y, Phokee W, Jirapornkul C. Increased Risk of Hospitalization for Lower Respiratory Tract Illness (LRTI) in the Elderly Living in Communities near a Newly Established Industrial Estate in Central Thailand. International Journal of Environmental Research and Public Health. 2025; 22(6):874. https://doi.org/10.3390/ijerph22060874
Chicago/Turabian StyleWangupadcha, Pirawan, Steven Ronsmans, Jeroen Vanoirbeek, Yuparat Limmongkon, Wipharat Phokee, and Chananya Jirapornkul. 2025. "Increased Risk of Hospitalization for Lower Respiratory Tract Illness (LRTI) in the Elderly Living in Communities near a Newly Established Industrial Estate in Central Thailand" International Journal of Environmental Research and Public Health 22, no. 6: 874. https://doi.org/10.3390/ijerph22060874
APA StyleWangupadcha, P., Ronsmans, S., Vanoirbeek, J., Limmongkon, Y., Phokee, W., & Jirapornkul, C. (2025). Increased Risk of Hospitalization for Lower Respiratory Tract Illness (LRTI) in the Elderly Living in Communities near a Newly Established Industrial Estate in Central Thailand. International Journal of Environmental Research and Public Health, 22(6), 874. https://doi.org/10.3390/ijerph22060874