
Brief Interventions for Families Seeking Support from Family Services: A Scoping Review

 ,
,
Abstract
1. Introduction
2. Method
2.1. Review Design
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search Strategy
2.5. Selection and Extraction
2.6. Data Charting
3. Results
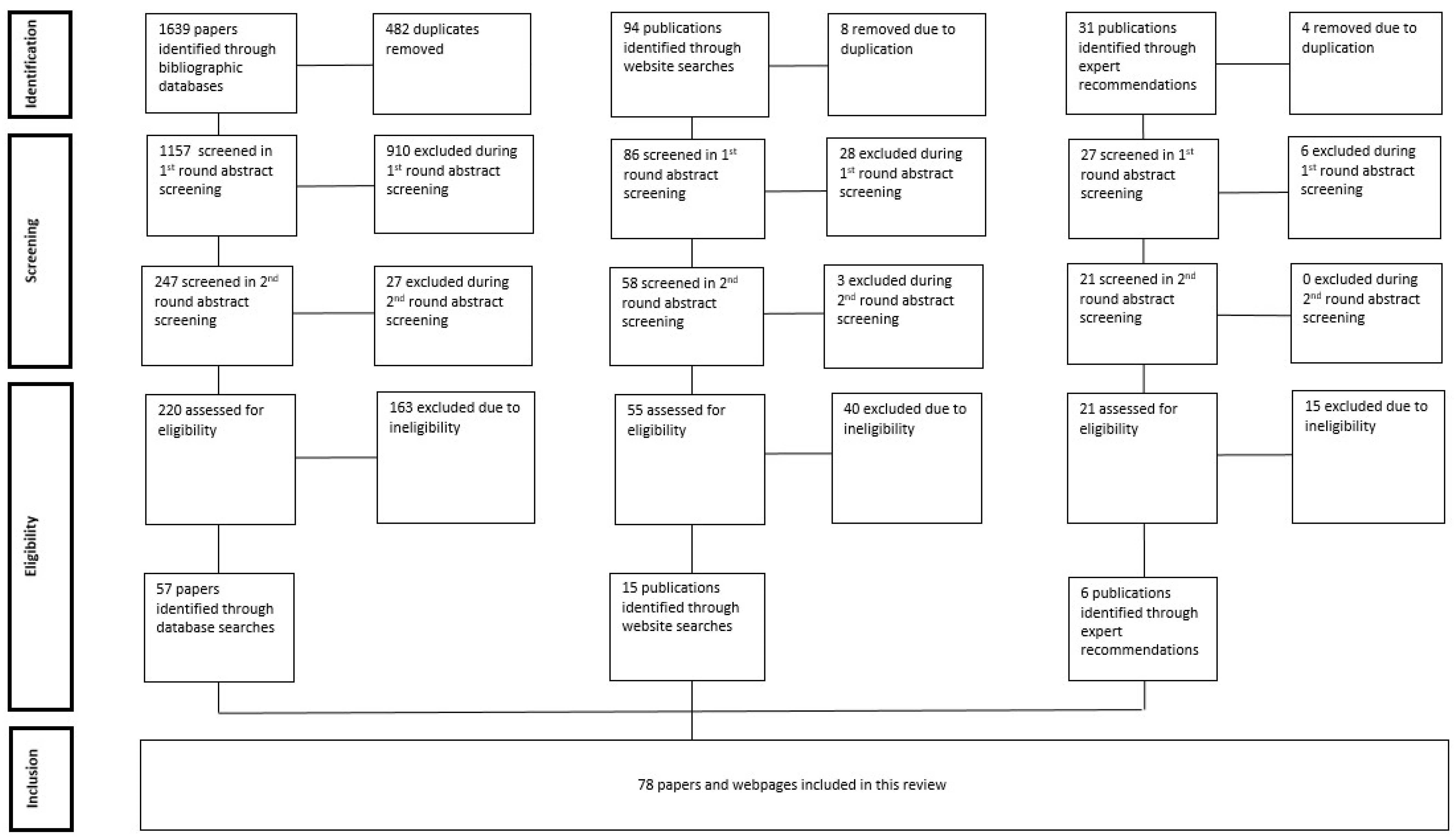
3.1. Search and Selection Results
3.2. Service and Setting Contexts for Brief Interventions
3.3. Purpose and Domains of Brief Interventions
3.4. Families Participating in Brief Interventions
3.5. Duration of Brief Interventions
3.6. Delivery of Brief Interventions
4. Discussion
Limitations of This Review
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| Organisation | Website |
|---|---|
| Act for Kids | https://www.actforkids.com.au accessed on 2 May 2023 |
| Allright | https://www.allright.org.nz/tools/parenting-courses accessed on 10 May 2023 |
| Anglicare Australia | https://www.anglicare.asn.au accessed on 9 May 2023 |
| Anglicare NSW & ACT | https://www.anglicare.com.au/ accessed on 9 May 2023 |
| Anglicare NT | https://www.anglicare-nt.org.au/ accessed on 9 May 2023 |
| Anglicare QLD | https://anglicarecq.org.au/ accessed on 9 May 2023https://www.anglicanchurchsq.org.au/anglicare accessed on 4 May 2023https://www.anglicarenq.org.au/ accessed on 4 May 2023 |
| Anglicare SA | https://anglicaresa.com.au/ accessed on 4 May 2023 |
| Anglicare Tasmania | https://www.anglicare-tas.org.au/ accessed on 9 May 2023 |
| Anglicare Victoria | https://www.anglicarevic.org.au/ accessed on 4 May 2023 |
| Anglicare WA | https://www.anglicarewa.org.au/ accessed on 9 May 2023 |
| Australian Childhood Foundation | https://www.childhood.org.au accessed on 4 May 2023 |
| Australian Indigenous HealthInfoNet | https://healthinfonet.ecu.edu.au accessed on 3 May 2023 |
| Australian Institute of Aboriginal and Torres Strait Islander Studies | https://aiatsis.gov.au/research accessed on 3 May 2023 |
| Australian Institute of Family Studies | https://aifs.gov.au accessed on 3 May 2023 |
| Australian Institute of Health and Welfare | https://www.aihw.gov.au accessed on 3 May 2023 |
| Berry Street | https://www.berrystreet.org.au/ accessed on 2 May 2023 |
| beyondblue | https://www.beyondblue.org.au accessed on 4 May 2023 |
| Black Dog Institute | https://www.blackdoginstitute.org.au accessed on 4 May 2023 |
| BlueKnot Foundation | https://blueknot.org.au accessed on 4 May 2023 |
| Body Matters Australia | https://bodymatters.com.au accessed on 4 May 2023 |
| Bouverie Centre | https://www.latrobe.edu.au/research/centres/health/bouverie accessed on 2 May 2023 |
| Child and Adolescent Mental Health Service (CAMHS) ACT | https://www.canberrahealthservices.act.gov.au/services-and-clinics/services/child-and-adolescent-mental-health-service-camhs-community-teams accessed on 4 May 2023 |
| CAMHS NSW | https://www.health.nsw.gov.au/mentalhealth/Pages/services-camhs.aspx accessed on 4 May 2023 |
| CAMHS SA | https://www.wchn.sa.gov.au/our-network/camhs accessed on 4 May 2023 |
| CAMHS Tasmania | https://www.health.tas.gov.au/health-topics/mental-health/tasmanias-mental-health-system/child-and-adolescent-mental-health-service accessed on 4 May 2023 |
| CAMHS WA | https://cahs.health.wa.gov.au/Our-services/Mental-Health accessed on 4 May 2023 |
| Canadian Child Welfare Research Portal | https://cwrp.ca accessed on 10 May 2023 |
| CatholicCare ACT | https://catholiccare.cg.org.au/ accessed on 9 May 2023 |
| CatholicCare Central QLD | https://catholiccarecq.com/ accessed on 9 May 2023 |
| CatholicCare NSW | https://www.catholiccare.org accessed on 9 May 2023 |
| CentaCare SA | https://www.cccsa.org.au/ accessed on 9 May 2023 |
| CatholicCare Tasmania | https://catholiccaretas.org.au/ accessed on 9 May 2023 |
| CatholicCare Victoria | https://www.catholiccarevic.org.au/ accessed on 9 May 2023 |
| Centre for Excellence in Child and Family Welfare | https://www.cfecfw.asn.au accessed on 10 May 2023 |
| Centre for Integrative Health | https://cfih.com.au accessed on 4 May 2023 |
| Child Welfare Information Gateway | https://www.childwelfare.gov accessed on 10 May 2023 |
| Communicare | https://www.communicare.org.au/Children-Youth-Family/Parenting-Services/Parenting-Support-Services accessed on 4 May 2023 |
| COPE | https://www.cope.org.au accessed on 4 May 2023 |
| Child and Youth Mental Health Service (CYMHS) QLD | https://www.childrens.health.qld.gov.au/services/mental-health accessed on 4 May 2023 |
| CYMHS Victoria | https://www.alfredhealth.org.au/services/child-youth-mental-health-service accessed on 4 May 2023https://www.easternhealth.org.au/mental-health-3/infants-children-and-youth-0-25/ accessed on 4 May 2023 |
| Drummond Street Services | https://ds.org.au/ accessed on 2 May 2023 |
| Family Life | https://www.familylife.com.au accessed on 2 May 2023 |
| ForWhen | https://forwhenhelpline.org.au accessed on 4 May 2023 |
| Headspace | https://headspace.org.au/, Accessed on 2 May 2023 |
| Health Navigator NZ | https://www.healthnavigator.org.nz/healthy-living/p/parenting-resources-courses-and-support/ accessed on 10 May 2023 |
| JewishCare NSW | https://jewishcare.com.au accessed on 9 May 2023 |
| JewishCare QLD | http://www.jcareqld.com/ accessed on 9 May 2023 |
| JewishCare Victoria | https://www.jewishcare.org.au/ accessed on 9 May 2023 |
| Lowitja Institute | https://www.lowitja.org.au accessed on 3 May 2023 |
| MacKillop Family Services | https://www.mackillop.org.au accessed on 3 May 2023 |
| Meerlinga | https://www.meerilinga.org.au/parenting-courses-services/ accessed on 4 May 2023 |
| Mental Health Beacon | https://www.latrobe.edu.au/__data/assets/pdf_file/0006/1153959/Mental-Health-Beacon-Project-Report-March-2015.pdf accessed on 4 May 2023 |
| National Society for the Prevention of Child Cruelty | https://www.nspcc.org.uk/, Accessed on 10 May 2023 |
| Ngala | https://www.ngala.com.au accessed on 9 May 2023 |
| Orygen | https://www.orygen.org.au accessed on 3 May 2023 |
| PANDA | https://panda.org.au/ accessed on 4 May 2023 |
| Relationship Australia | https://relationships.org.au accessed on 3 May 2023 |
| SNAICC | https://www.snaicc.org.au accessed on 3 May 2023 |
| Social Care Institute for Excellence | https://www.scie.org.uk accessed on 10 May 2023 |
| Turning Point | https://www.turningpoint.org.au accessed on 4 May 2023 |
| Uniting SA | https://unitingsa.com.au/ accessed on 10 May 2023 |
| Uniting WA | https://unitingwa.org.au/ accessed on 9 May 2023 |
| UnitingCare Australia | https://unitingcare.org.au, Accessed on 9 May 2023 |
| Uniting NSW & ACT | https://www.uniting.org/home, Accessed on 9 May 2023 |
| UnitingCare QLD | https://www.unitingcareqld.com.au/ accessed on 9 May 2023 |
| Uniting Victoria & Tasmania | https://www.unitingvictas.org.au/services/ accessed on 9 May 2023 |
| Wanslea | https://www.wanslea.org.au/families-and-children/parents-and-grandparent-carers#Parenting-support accessed on 9 May 2023 |
Appendix B
| 1 | Brief N3 (educat* or interven* or therap* or counsel* or facilit* or program* or help* or assist* or guid* or navigat* or helpline* or support* or advisor* or advice or consult* or helpline* or practice* or coach* or interviewing) |
| 2 | Walk-in N3 (educat* or interven* or therap* or counsel* or facilit* or program* or help* or assist* or guid* or navigat* or helpline* or support* or advisor* or advice or consult* or helpline* or practice* or coach* or interviewing) |
| 3 | Drop-in N3 (educat* or interven* or therap* or counsel* or facilit* or program* or help* or assist* or guid* or navigat* or helpline* or support* or advisor* or advice or consult* or helpline* or practice* or coach* or interviewing) |
| 4 | Short N3 (educat* or interven* or therap* or counsel* or facilit* or program* or help* or assist* or guid* or navigat* or helpline* or support* or advisor* or advice or consult* or helpline* or practice* or coach* or interviewing) |
| 5 | Casual N3 (educat* or interven* or therap* or counsel* or facilit* or program* or help* or assist* or guid* or navigat* or helpline* or support* or advisor* or advice or consult* or helpline* or practice* or coach* or interviewing) |
| 6 | Low-intensity N3 (educat* or interven* or therap* or counsel* or facilit* or program* or help* or assist* or guid* or navigat* or helpline* or support* or advisor* or advice or consult* or helpline* or practice* or coach* or interviewing) |
| 7 | Workshop* N3 (educat* or interven* or therap* or counsel* or facilit* or program* or help* or assist* or guid* or navigat* or helpline* or support* or advisor* or advice or consult* or helpline* or practice* or coach* or interviewing) |
| 8 | Single-session N3 (educat* or interven* or therap* or counsel* or facilit* or program* or help* or assist* or guid* or navigat* or helpline* or support* or advisor* or advice or consult* or helpline* or practice* or coach* or interviewing) |
| 9 | One-off N3 (educat* or interven* or therap* or counsel* or facilit* or program* or help* or assist* or guid* or navigat* or helpline* or support* or advisor* or advice or consult* or helpline* or practice* or coach* or interviewing) |
| 10 | One-session N3 (educat* or interven* or therap* or counsel* or facilit* or program* or help* or assist* or guid* or navigat* or helpline* or support* or advisor* or advice or consult* or helpline* or practice* or coach* or interviewing) |
| 11 | Light-touch N3 (educat* or interven* or therap* or counsel* or facilit* or program* or help* or assist* or guid* or navigat* or helpline* or support* or advisor* or advice or consult* or helpline* or practice* or coach* or interviewing) |
| 12 | Parent* or carer* or caregiver* or care-giver* or mother* or father* or family or families or mum* or dad* or mom* or maternal or paternal or stepparent* or guardian* or kin or kith or mob* |
| 13 | 1–11/or |
| 14 | 12 and 13 |
References
- Center for Substance Abuse Treatment. Brief interventions and brief therapies for substance abuse. In Treatment Improvement Protocol (TIP) Servies; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 1999; Volume 34. [Google Scholar]
- Newham, J.J.; McLean, K.; Ginja, S.; Hurt, L.; Molloy, C.; Lingam, R.; Goldfeld, S. Brief evidence-based interventions for universal child health services: A restricted evidence assessment of the literature. BMC Public Health 2020, 20, 993. [Google Scholar] [CrossRef] [PubMed]
- Winters, K.C.; Lee, S.; Botzet, A.; Fahnhorst, T.; Nicholson, A. One-year outcomes and mediators of a brief intervention for drug abusing adolescents. Psychol. Addict. Behav. 2014, 28, 464. [Google Scholar] [CrossRef]
- Stoll, R.D.; Pina, A.A.; Schleider, J. Brief, non-pharmacological, interventions for pediatric anxiety: Meta-analysis and evidence base status. J. Clin. Child Adolesc. Psychol. 2020, 49, 435–459. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE). Behaviour Change: Individual Appoach; NICE: Ra’anana, Israel, 2014; Available online: https://www.nice.org.uk/guidance/ph49/chapter/Recommendations#recommendation-9-deliver-very-brief-brief-extended-brief-and-high-intensity-behaviour-change (accessed on 3 May 2023).
- Schmit, E.L.; Schmit, M.K.; Lenz, A.S. Meta-analysis of solution-focused brief therapy for treating symptoms of internalizing disorders. Couns. Outcome Res. Eval. 2017, 7, 21–39. [Google Scholar] [CrossRef]
- Hsu, K.-S.; Eads, R.; Lee, M.Y.; Wen, Z. Solution-focused brief therapy for behavior problems in children and adolescents: A meta-analysis of treatment effectiveness and family involvement. Child. Youth Serv. Rev. 2021, 120, 105620. [Google Scholar] [CrossRef]
- Ingoldsby, E.M. Review of interventions to improve family engagement and retention in parent and child mental health programs. J. Child Fam. Stud. 2010, 19, 629–645. [Google Scholar] [CrossRef]
- Aggarwal, S.; Patton, G. Engaging families in the management of adolescent self-harm. Evid.-Based Ment. Health 2018, 21, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Hymmen, P.; Stalker, C.A.; Cait, C.A. The case for single-session therapy: Does the empirical evidence support the increased prevalence of this service delivery model? J. Ment. Health 2013, 22, 60–71. [Google Scholar] [CrossRef]
- Schleider, J.L.; Weisz, J.R. Little treatments, promising effects? Meta-analysis of single-session Interventions for youth psychiatric problems. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 107–115. [Google Scholar] [CrossRef]
- Schleider, J.L.; Dobias, M.L.; Sung, J.Y.; Mullarkey, M.C. Future directions in single-session youth mental health interventions. J. Clin. Child Adolesc. Psychol. 2020, 49, 264–278. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- Victorian Department of Families, Fairness and Housing. Individual, Child and Family Support 31435; Department of Families, Fairness and Housing: Melbourne, Australia, 2021. [Google Scholar]
- Jolley, R.J.; Lorenzetti, D.L.; Manalili, K.; Lu, M.; Quan, H.; Santana, M.J. Protocol for a scoping review study to identify and classify patient-centred quality indicators. BMJ Open 2017, 7, e013632. [Google Scholar] [CrossRef]
- Chesterfield, J.A.; Porzig-Drummond, R.; Stevenson, R.J.; Stevenson, C.S. Evaluating a brief behavioral parenting program for parents of school-aged children with ADHD. Parent. Sci. Pract. 2021, 21, 216–240. [Google Scholar] [CrossRef]
- O’Mahen, H.A.; Ramchandani, P.G.; King, D.X.; Lee-Carbon, L.; Wilkinson, E.L.; Thompson-Booth, C.; Ericksen, J.; Milgrom, J.; Dunkley-Bent, J.; Halligan, S.L.; et al. Adapting and testing a brief intervention to reduce maternal anxiety during pregnancy (ACORN): Report of a feasibility randomized controlled trial. BMC Psychiatry 2022, 22, 129. [Google Scholar] [CrossRef]
- Cooney, M.R.; Short, M.A.; Gradisar, M. An open trial of bedtime fading for sleep disturbances in preschool children: A parent group education approach. Sleep Med. 2018, 46, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Villarreal, Y.R.; Spellman, M.L.; Prudon, J.; Northrup, T.F.; Berens, P.D.; Blackwell, S.; Velasquez, M.M.; Stotts, A.L. A brief, hospital-initiated motivational interviewing and acceptance and commitment therapy intervention to link postpartum mothers who use illicit drugs with treatment and reproductive care: A case report. Cogn. Behav. Pract. 2021, 28, 92–106. [Google Scholar] [CrossRef]
- Fung, K.; Lake, J.; Steel, L.; Bryce, K.; Lunsky, Y. ACT processes in group intervention for mothers of children with autism spectrum disorder. J. Autism Dev. Disord. 2018, 48, 2740–2747. [Google Scholar] [CrossRef]
- Hahs, A.D.; Dixon, M.R.; Paliliunas, D. Randomized controlled trial of a brief acceptance and commitment training for parents of individuals diagnosed with autism spectrum disorders. J. Context. Behav. Sci. 2019, 12, 154–159. [Google Scholar] [CrossRef]
- Lunsky, Y.; Fung, K.; Lake, J.; Steel, L.; Bryce, K. Evaluation of acceptance and commitment therapy (ACT) for mothers of children and youth with autism spectrum disorder. Mindfulness 2018, 9, 1110–1116. [Google Scholar] [CrossRef]
- Moyer, D.N.; Page, A.R.; McMakin, D.Q.; Murrell, A.R.; Lester, E.G.; Walker, H.A. The Impact of Acceptance and Commitment Therapy on Positive Parenting Strategies Among Parents Who Have Experienced Relationship Violence. J. Fam. Violence 2018, 33, 269–279. [Google Scholar] [CrossRef]
- Jewell, C.; Wittkowski, A.; Collinge, S.; Pratt, D. A brief cognitive behavioural intervention for parents of anxious children: Feasibility and acceptability study. Child Youth Care Forum 2023, 52, 661–681. [Google Scholar] [CrossRef]
- Giallo, R.; Fogarty, A.; Savopoulos, P.; Cox, A.; Toone, E.; Williams, K.; Jones, A.; Treyvaud, K. Capturing the experiences of clinicians implementing a new brief intervention for parents and children who have experienced family violence in Australia. Health Soc. Care Community 2022, 30, e1599–e1610. [Google Scholar] [CrossRef]
- Fogarty, A.; Treyvaud, K.; Savopoulos, P.; Jones, A.; Cox, A.; Toone, E.; Giallo, R. Facilitators to engagement in a mother–child therapeutic intervention following intimate partner violence. J. Interpers. Violence 2022, 37, 1796–1824. [Google Scholar] [CrossRef]
- Moudi, Z.; Talebi, B.; Pour, M.S. Effect of a brief training program for primigravid adolescents on parenting self-efficacy and mother-infant bonding in the southeast of Iran. Int. J. Adolesc. Med. Health 2020, 32, 20170092. [Google Scholar] [CrossRef]
- Smith, C.H.; Turbitt, E.; Muschelli, J.; Leonard, L.; Lewis, K.L.; Freedman, B.; Muratori, M.; Biesecker, B.B. Feasibility of coping effectiveness training for caregivers of children with autism spectrum disorder: A genetic counseling intervention. J. Genet. Couns. 2018, 27, 252–262. [Google Scholar] [CrossRef] [PubMed]
- McGoron, L.; O’Neal, T.; Savastano, G.E.; Roberts, K.L.; Richardson, P.A.; Bocknek, E.L. Creating Connections: A Feasibility Study of a Technology-Based Intervention to Support Mothers of Newborns during Pediatric Well-Visits. Clin. Pract. Pediatr. Psychol. 2023, 11, 180–185. [Google Scholar] [CrossRef]
- Zachry, A.H.; Jones, T.; Flick, J.; Richey, P. The Early STEPS pilot study: The impact of a brief consultation session on self-reported parenting satisfaction. Matern. Child Health J. 2021, 25, 1923–1929. [Google Scholar] [CrossRef]
- Wilhelmsen-Langeland, A.; Aardal, H.; Hjelmseth, V.; Fyhn, K.H.; Stige, S.H. An Emotion Focused Family Therapy workshop for parents with children 6–12 years increased parental self-efficacy. Emot. Behav. Difficulties 2020, 25, 29–41. [Google Scholar] [CrossRef]
- Nash, P.; Renelli, M.; Stillar, A.; Streich, B.; Lafrance, A. Long-term outcomes of a brief emotion-focused family therapy intervention for eating disorders across the lifespan: A mixed-methods study. Can. J. Couns. Psychother. 2020, 54, 130–149. [Google Scholar]
- Foroughe, M.; Soliman, J.; Bean, B.; Thambipillai, P.; Benyamin, V. Therapist adaptations for online caregiver emotion-focused family therapy during the COVID-19 pandemic. Pers.-Centered Exp. Psychother. 2022, 21, 1–15. [Google Scholar] [CrossRef]
- Foroughe, M.; Browne, D.T.; Thambipillai, P.; Cordeiro, K.; Muller, R.T. Brief emotion-focused family therapy: A 12-month follow-up study. J. Marital. Fam. Ther. 2023, 49, 394–410. [Google Scholar] [CrossRef] [PubMed]
- Feldman, J.S.; Zhou, Y.; Krug, C.W.; Wilson, M.N.; Shaw, D.S. Indirect effects of the Family Check-Up on youth extracurricular involvement at school-age through improvements in maternal positive behavior support in early childhood. Soc. Dev. 2021, 30, 311–328. [Google Scholar] [CrossRef]
- Becker, S.J.; Marceau, K.; Hernandez, L.; Spirito, A. Is it selection or socialization? Disentangling peer influences on heavy drinking and marijuana use among adolescents whose parents received brief interventions. Subst. Abus. Res. Treat. 2019, 13, 1178221819852644. [Google Scholar] [CrossRef]
- Connell, A.M.; Magee, K.; Stormshak, E.; Ha, T.; Westling, E.; Wilson, M.; Shaw, D. Long-term cross-over effects of the family check-up prevention program on child and adolescent depression: Integrative data analysis of three randomized trials. J. Consult. Clin. Psychol. 2021, 89, 773–782. [Google Scholar] [CrossRef]
- Adkins, T.; Reisz, S.; Hasdemir, D.; Fonagy, P. Family Minds: A randomized controlled trial of a group intervention to improve foster parents’ reflective functioning. Dev. Psychopathol. 2021, 34, 1177–1191. [Google Scholar] [CrossRef]
- Adkins, T.; Luyten, P.; Fonagy, P. Development and preliminary evaluation of Family Minds: A mentalization-based psychoeducation program for foster parents. J. Child Fam. Stud. 2018, 27, 2519–2532. [Google Scholar] [CrossRef]
- Hoadley, B.; Falkov, A.; Agalawatta, N. The acceptability of a single session family focused approach for children/young people and their parents attending a child and youth mental health service. Adv. Ment. Health 2019, 17, 44–54. [Google Scholar] [CrossRef]
- Cobham, V.; Radtke, S.; Hawkings, I.; Jordan, M.; Ali, N.R.; Ollendick, T.; Sanders, M. Evaluating a One-Day Parent-Only Intervention in the Treatment of Youth with Anxiety Disorders: Child and Family-Level Outcomes; Research Square: Durham, NC, USA, 2023. [Google Scholar]
- Doyle, O.; Owens, C. Evaluation of Fear-less Triple P in Ireland; International Congress on Evidence-based Parenting Support; ICEPS Conference: Bangkok, Thailand, 2023. [Google Scholar]
- Triple P. Fear-Less Triple P; Triple P International Pty Ltd.: Brisbane, Australia, 2020; Available online: www.triplep.net/files/9515/9477/2089/ENG_Fear-Less_Triple_P_LTR.pdf (accessed on 3 May 2023).
- Georg, A.; Kress, S.; Taubner, S. Strengthening mentalizing in a depressed mother of an infant with sleep disorders. J. Clin. Psychol. 2019, 75, 859–873. [Google Scholar] [CrossRef]
- Esbjørn, B.H.; Breinholst, S.; Christiansen, B.M.; Bukh, L.; Walczak, M. Increasing access to low-intensity interventions for childhood anxiety: A pilot study of a guided self-help program for Scandinavian parents. Scand. J. Psychol. 2019, 60, 323–328. [Google Scholar] [CrossRef]
- Botzet, A.M.; Dittel, C.; Birkeland, R.; Lee, S.; Grabowski, J.; Winters, K.C. Parents as interventionists: Addressing adolescent substance use. J. Subst. Abus. Treat. 2019, 99, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Frank, K.; Sandman, L. Parents as primary sexuality educators for adolescents and adults with Down syndrome: A mixed methods examination of the Home BASE for intellectual disabilities workshop. Am. J. Sex. Educ. 2021, 16, 283–302. [Google Scholar] [CrossRef]
- Holt, C.; Gentilleau, C.; Gemmill, A.W.; Milgrom, J. Improving the mother-infant relationship following postnatal depression: A randomised controlled trial of a brief intervention (HUGS). Arch. Women’s Ment. Health 2021, 24, 913–923. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.H.M.; Wyman Battalen, A.; Sellers, C.M.; Spirito, A.; Yen, S.; Maneta, E.; Ryan, C.A.; Braciszewski, J.M. An mHealth approach to extend a brief intervention for adolescent alcohol use and suicidal behavior: Qualitative analyses of adolescent and parent feedback. J. Technol. Hum. Serv. 2019, 37, 255–285. [Google Scholar] [CrossRef]
- Hansen, S.G.; Raulston, T.J.; Machalicek, W.; Frantz, R. Caregiver-mediated joint attention intervention. Behav. Interv. 2018, 33, 205–211. [Google Scholar] [CrossRef]
- Wirehag Nordh, E.L.; Grip, K.; Thorvaldsson, V.; Priebe, G.; Afzelius, M.; Axberg, U. Preventive interventions for children of parents with depression, anxiety, or bipolar disorder: A quasi-experimental clinical trial. Acta Paediatr. 2023, 112, 132–142. [Google Scholar] [CrossRef]
- The Bouverie Centre. Mental Health Beacon: Implementing Family Inclusive Practices in Victorian Mental Health Services; The Mental Health Program at the Bouverie Centre, La Trobe University: Melbourne, Australia, 2015; Available online: https://www.latrobe.edu.au/research/centres/health/bouverie/practitioners/specialist-areas/family-inclusion/beacon (accessed on 2 May 2023).
- Nicolson, S.; Carron, S.P.; Paul, C. Supporting early infant relationships and reducing maternal distress with the newborn behavioral observations: A randomized controlled effectiveness trial. Infant Ment. Health J. 2022, 43, 455–473. [Google Scholar] [CrossRef]
- Cartwright-Hatton, S.; Ewing, D.; Dash, S.; Hughes, Z.; Thompson, E.J.; Hazell, C.M.; Field, A.P.; Startup, H. Preventing family transmission of anxiety: Feasibility RCT of a brief intervention for parents. Br. J. Clin. Psychol. 2018, 57, 351–366. [Google Scholar] [CrossRef]
- Dixon, J.F.; Akins, R.; Miller, E.; Breslau, J.; Gill, S.; Bisi, E.; Schweitzer, J.B. Changing parental knowledge and treatment acceptance for ADHD: A pilot study. Clin. Pediatr. 2023, 62, 301–308. [Google Scholar] [CrossRef] [PubMed]
- CatholicCare. Parenting and Child Development: Parent Coaching; CatholicCare: Sydney, Australia, 2023; Available online: https://www.catholiccare.org/family-youth-children/parenting/child-development-parenting/ (accessed on 9 May 2023).
- Lai, A.Y.K.; Sit, S.M.M.; Thomas, C.; Cheung, G.O.C.; Wan, A.; Chan, S.S.C.; Lam, T.-h. A randomized controlled trial of a positive family holistic health intervention for probationers in Hong Kong: A mixed-method study. Front. Psychol. 2021, 12, 739418. [Google Scholar] [CrossRef]
- Cullum, K.A.; Goodman, S.H.; Garber, J.; Korelitz, K.; Sutherland, S.; Stewart, J. A positive parenting program to enhance positive affect in children of previously depressed mothers. J. Fam. Psychol. 2022, 36, 692–703. [Google Scholar] [CrossRef] [PubMed]
- Triple, P. Primary Care Stepping Stones Triple P: For Parents of a Child with a Disability; Triple P Positive Parenting Program: QLD, Brisbane, Australia, 2022; Available online: https://www.triplep-parenting.net.au/vic-en/free-parenting-courses/which-course-is-right-for-me/stepping-stones-for-parents-of-a-child-with-a-disability/ (accessed on 3 May 2023).
- Zand, D.H.; Bultas, M.W.; McMillin, S.E.; Halloran, D.; White, T.; McNamara, D.; Pierce, K.J. A pilot of a brief positive parenting program on children newly diagnosed with autism spectrum disorder. Fam. Process 2018, 57, 901–914. [Google Scholar] [CrossRef] [PubMed]
- Carney, T.; Chimbambo, V.; Johnson, K.; Louw, J.; Myers, B. The adaptation of an evidence-based brief intervention for substance-using adolescents and their caregivers. Psychother. Res. 2020, 30, 728–738. [Google Scholar] [CrossRef] [PubMed]
- Distefano, R.; Schubert, E.C.; Finsaas, M.C.; Desjardins, C.D.; Helseth, C.K.; Lister, M.; Carlson, S.M.; Zelazo, P.D.; Masten, A.S. Ready? Set. Go! A school readiness programme designed to boost executive function skills in preschoolers experiencing homelessness and high mobility. Eur. J. Dev. Psychol. 2020, 17, 877–894. [Google Scholar] [CrossRef]
- Dittman, C.K.; Burke, K.; Hodges, J. Brief parenting support for parents of teenagers dealing with family conflict: A pilot randomized controlled trial. Child Youth Care Forum 2020, 49, 799–816. [Google Scholar] [CrossRef]
- Daire, A.P.; Liu, X.; Tucker, K.; Williams, B.; Broyles, A.; Wheeler, N. Positively impacting maternal stress and parental adjustment through community-based relationship education (RE). Marriage Fam. Rev. 2019, 55, 239–257. [Google Scholar] [CrossRef]
- Peterson, J.W.; Almanzar, N.; Chamberlain, L.J.; Huffman, L.; Butze, T.; Marin-Nevarez, P.; Bruce, J.S. School Readiness Coaching in the Pediatric Clinic: Latinx Parent Perspectives. Acad. Pediatr. 2021, 21, 802–808. [Google Scholar] [CrossRef]
- Rooks-Ellis, D.L.; Jones, B.; Sulinski, E.; Howorth, S.; Achey, N. The effectiveness of a brief sexuality education intervention for parents of children with intellectual and developmental disabilities. Am. J. Sex. Educ. 2020, 15, 444–464. [Google Scholar] [CrossRef]
- Salomonsson, B.; Kornaros, K.; Sandell, R.; Nissen, E.; Lilliengren, P. Short-term psychodynamic infant–parent interventions at child health centers: Outcomes on parental depression and infant social–emotional functioning. Infant Ment. Health J. 2021, 42, 109–123. [Google Scholar] [CrossRef]
- Akor, B.O.; Moses, L.A.; Baamlong, N.D.; Shedul, L.L.; Haruna, A.S.; Abu, J.M.; Chira, O.U.; Ripiye, N.R.; Abdulkareem, R.A. Effect of counselling on the family function of intimate partner violence victims attending antenatal clinic in a tertiary hospital in North Central Nigeria. S. Afr. Fam. Pract. 2019, 61, 69–74. [Google Scholar] [CrossRef]
- Elliott, A.; Dokona, J.; von Doussa, H. Following the river’s flow: A conversation about single session approaches with Aboriginal families. Aust. N. Z. J. Fam. Ther. 2020, 41, 249–257. [Google Scholar] [CrossRef]
- Poon, A.W.C.; Harvey, C.; Fuzzard, S.; O’Hanlon, B. Implementing a family-inclusive practice model in youth mental health services in Australia. Early Interv. Psychiatry 2019, 13, 461–468. [Google Scholar] [CrossRef]
- Al-Khatib, B.; Norris, S. A family consultation service: Single session intervention to build the mental health and wellbeing of children and their families. Educ. Child Psychol. 2015, 32, 7–20. [Google Scholar] [CrossRef]
- The Bouverie Centre. Walk-in Together Online Sessions; La Trobe University: Melbourne, Australia, 2022; Available online: https://www.latrobe.edu.au/research/centres/health/bouverie/families-and-communities/therapy/walk-in-together-online-sessions (accessed on 2 May 2023).
- BodyMatters. Single Session Intervention; BodyMatters: Mosman, NSW, Australia, 2022; Available online: https://bodymatters.com.au/single-session-intervention/ (accessed on 4 May 2023).
- Bastida-Pozuelo, M.F.; Sánchez-Ortuño, M.M.; Meltzer, L.J. Nurse-led brief sleep education intervention aimed at parents of school-aged children with neurodevelopmental and mental health disorders: Results from a pilot study. J. Spec. Pediatr. Nurs. 2018, 23, e12228. [Google Scholar] [CrossRef] [PubMed]
- Eltanamly, H.; Leijten, P.; van Roekel, E.; Mouton, B.; Pluess, M.; Overbeek, G. Strengthening parental self-efficacy and resilience: A within-subject experimental study with refugee parents of adolescents. Child Dev. 2023, 94, 187–201. [Google Scholar] [CrossRef]
- Choi, J.J. A case study of solution-focused brief family therapy. Am. J. Fam. Ther. 2020, 48, 195–210. [Google Scholar] [CrossRef]
- Kopcsó, K.; Láng, A.; Coffman, M.F. Reducing the nighttime fears of young children through a brief parent-delivered treatment—Effectiveness of the Hungarian version of Uncle Lightfoot. Child Psychiatry Hum. Dev. 2022, 53, 256–267. [Google Scholar] [CrossRef]
- Sieverson, C.; Olhaberry, M.; Duarte, J.; Morán-Kneer, J.; Costa, S.; León, M.J.; Valenzuela, S.; Leyton, F.; Honorato, C.; Muzard, A. Beyond the outcomes: Generic change indicators in a video-feedback intervention with a depressed mother and her baby: A single case study. Res. Psychother. Psychopathol. Process Outcome 2022, 25, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Ganci, M.; Pradel, M.; Hughes, E.K. Feasibility of a parent education and skills workshop for improving response to family-based treatment of adolescent anorexia nervosa. Int. J. Eat. Disord. 2018, 51, 358–362. [Google Scholar] [CrossRef]
- Rycroft, P.; Young, J. Single session therapy: Capturing the moment. Psychother. Aust. 1977, 4, 18–23. [Google Scholar]
- Young, J.; Weir, S.; Rycroft, P. Implementing single session therapy. Aust. N. Z. J. Fam. Ther. 2012, 33, 84–97. [Google Scholar] [CrossRef]
- Hawker, D.S.J. The case of brief therapy in CAMHS. Clin. Psychol. Forum 2007, 173, 29–32. [Google Scholar] [CrossRef]
- McDermott, B. Child and Adolescent Mental Health Services Review; Tasmanian Department of Health: Hobart, Australia, 2020. Available online: https://www.health.tas.gov.au/sites/default/files/2022-02/Child%20and%20Adolescent%20Mental%20Health%20Services%20Review%20Report.pdf (accessed on 4 May 2023).
- Young, J. Putting single session thinking to work: Conceptual, practical, training, and implementation ideas. Aust. N. Z. J. Fam. Ther. 2020, 41, 231–248. [Google Scholar] [CrossRef]
- Bloom, B.L. Focused single-session psychotherapy: A review of the clinical work and research literature. Brief Treat. Crisis Interv. 2001, 1, 75–86. [Google Scholar] [CrossRef]
| Intervention | Target Populations | Target Outcomes | Service Sectors | Settings | Modalities Used Duration Range |
|---|---|---|---|---|---|
| 1-2-3 Magic [17] | Parents of children aged 6–12 years diagnosed with ADHD | Reduction in child disruptive behaviour, ADHD symptoms, dysfunctional parenting | Mental health | University | 3 × 2 h weekly sessions |
| ACORN [18] | Pregnant women with elevated anxiety symptoms | Reduction in parental anxiety | Prenatal/pregnancy health | Antenatal/parenting classes | 3 × 2 h group sessions for pregnant women and their partners |
| Bedtime Fading for Preschoolers [19] | Children 1.5 years old with sleep difficulties and their mothers | Child sleep onset latency Child wake after sleep onset Child bedtime tantrums | Family services | University | 2 × 90 min sessions with groups of parents |
| Brief Acceptance and Commitment-based interventions [20,21,22,23,24] | Mothers with infants who screen positive for illicit substance use Mothers of autistic children 0–22 years Parents of autistic children 5–13 years Parents who have experienced relationship violence | Substance use treatment uptake Parental depression, stress, social isolation and physical health Positive parenting practices | Health Community Mental health | Hospital Community School | 1–3 × 45 min sessions with individual parents 1.5 day workshop with groups of caregivers followed by a refresher session 2 × 2 h sessions with groups of parents 1 evening session, followed by a 1 full-day session and a refresher session with groups of parents 4 × 1 h sessions with group of parents |
| Brief cognitive behavioural group intervention for parents of anxious children [25] | Parents of primary school children aged 4–10 years, who have reported their child is experiencing symptoms of anxiety without a formal diagnosis | Reduction in child anxiety symptoms Increases in parent self-efficacy | Community | Community: Intended for delivery in schools but due to COVID-19 lockdowns it was delivered online | 3 online sessions with groups of parents (2 × 2 h; 1 × 1.5 h) delivered fortnightly |
| Brief Relationship Intervention and Screening [26,27] | Children 0–17 years who have experienced family violence and their non-offending parent/caregiver | Child emotional behavioural difficulties and traumatic stress response Parental psychological distress, reflective function, sensitivity and responsiveness Positive parent–child interactions Parenting self-efficacy Positive attitudes to help seeking | Community | Community | 4 × 60–90 min sessions with individual parents and child–parent dyad |
| Brief Training Program for Primigravid Adolescents [28] | Married primigravid adolescents | Parenting self-efficacy Mother-infant bonding Social support | Health | University | 3 × 60–90 min sessions with groups of pregnant women |
| Coping Effectiveness Training (CET) [29] | Caregivers of autistic children | Coping self-efficacy Feasibility of the CET intervention | Health | Clinic | 2 sessions with individual parents (1 × 90 min and 1 × 60 min) |
| Creating Connections [30] | Mothers of newborns (1–14 days old) | Feasibility of a technology-based intervention | Paediatric | Ambulatory paediatric centre and home | 10–15 min plus text messages over 4 months |
| Early Screening for Therapy and Empowering Parents (STEPS) [31] | Caregivers and children 0–6 years | Parenting satisfaction Uptake of referrals and follow-on services | Paediatrics/Health | Paediatric clinic | 1 × 45 min sessions with individual parents and children |
| Emotion-Focused Therapy Workshop [32,33,34,35] | Parents of children, young people and other family members with mental health concerns | Parenting self-efficacy Child behaviour Family psychological symptoms Family engagementChild mental health difficulties | Mental health | Clinic Online | 2-day workshop with groups of parents |
| Family Check-up [36,37,38] | Families with children or young people with conduct or behavioural concerns; low income families. | Child substance use Child mental health Child behaviour Family relationships Peer relationships | Health Community Menmintal health | Hospital School Community Clinic | 1–3 × 45 min sessions with individual parents Between 1 and 2 sessions or a 1.5 day workshop with groups of parents |
| Family Minds [39,40] | Foster parents with at least one foster or adopted child who was 4 years or older | Increased parental reflective functioning Reduction in parenting stress | Foster care Child protection | Foster care Child protection | 3 × 3 h classes over 4–6 weeks with groups of foster carers |
| Family Model [41] | Children <18 years experiencing mental illness and a parent/caregiver experiencing mental illness | Development of family-focused care plan | Hospital Child and Youth Mental Health Service | Clinic | 1 × 1–2 h individual session with child and their family |
| Fear-less Triple P [42,43,44] | Parents/caregivers of children 6–14 years with anxiety | Child anxiety Sibling anxiety Parental confidence Child emotion-regulation strategies | Community | Online | 1 × 2 h seminar with group of parents 1 × day (8 h) or 3 days (2.5 h) workshop with groups of parents |
| Focused parent-infant psychotherapy [45] | Depressed mother with an infant with sleep disorder | Infant regulatory behaviours Parenting competence | Family services | Clinic | 4 sessions with individual infant-parent dyad |
| Get a Grip on anxiety [46] | Parents/caregivers of children 7–12 years old with anxiety | Child anxiety and depression | University | University Home | 2 × 2 h workshops with groups of parents 10 × 1 h weekly programme with individual parent and child |
| Home Base Program [47] | Parents/caregivers and their adolescent children aged 12–17 years who use substances | Decreased alcohol use and increased family cohesion | University | University Home or other location for parent delivered sessions Phone for coaching support | 1 × 4 h parent training 3 × sessions delivered by parents to their adolescents3 × “coaching” phone calls (15–20 min) prior to each parent–child session |
| Home Based Adolescent Sexual Education for intellectual Disabilities [48] | Parents of individuals 12–30 years old with Down Syndrome | Parental attitudes surrounding sexuality and disability Parental self-efficacy in discussing sexuality | Intellectual disability | Clinic | 3 × 3 h workshops with groups of parents |
| HUGS Mother-infant Interaction Intervention [49] | Mothers diagnosed with depression and their infants 0–12 months old | Mother-infant relationship Maternal parenting stress Early child development | Mental health | Clinic | 4 × 1.5 h sessions with groups of parent–child dyads |
| Integrated Alcohol and Suicide Intervention for Suicidal Teens [50] | Suicidal adolescents (13–18 years) and their caregivers | Adolescent alcohol consumption Adolescent suicidal thoughts and behaviours | Mental health | Inpatient psychiatry unit | 1 × 60–90 min individual sessions with adolescents1 × 20–30 min family sessions |
| Joint attention training [51] | Caregivers of autistic children (3–6 years old) | Improve joint attention | University | University | 2–3 × 10 min sessions per week with a parent–child dyad |
| Let’s Talk About Children (Let’s Talk) [52,53] | Parents experiencing mental illness | Parenting Family functioning | Mental health | Mental health service | 2 × 1 h sessions with individual parents (preferably both parents) with possible additional 3rd session if more complex issues are present |
| Newborn Behavioural Observations [54] | First time mothers with antenatal distress and at risk of postnatal depression and their babies | Mother-infant interaction quality Maternal anxiety or depression symptoms Depression diagnosis | Healthcare/maternal healthcare | Hospital Home | 3 × 20–40 min sessions |
| One-session group based parenting intervention [55] | Parents with anxiety disorders and their children (3–9 years old) | Child anxiety | Mental health | NHS/University | 1 × 5.5 h interactive workshop |
| One Session Psycho-educational Workshop [56] | Parents/caregivers of children 4–15 years at risk of ADHD or who have been diagnosed with ADHD | Parental beliefs and knowledge about ADHD Treatment acceptance and utilisation | Community | School district office University | 1 × 2 h workshop with groups of parents |
| Parent Coaching [57] | Parents who have already attended parenting courses | Parental knowledge in attachment Parent–child relationship Parental confidence | Family services | Wellbeing and Family Relationship service Online | Up to 3 sessions with individual parents |
| Positive Family Holistic Health Intervention [58] | Children and young people (13 years and older) on probation and their families | Physical activity and fitness performance Self-esteem Happiness Anxiety and depression symptoms Life satisfaction Quality of life Family communication and wellbeing Relationship with probation officers | Probation service | Community | 2 × 1 h sessions with individual clients 1 × 4.5 h activity with groups of families |
| Positive Parenting Intervention [59] | Mothers with history of depression and their children aged 8–10 years | Positive parenting behaviours Child positive affect | Mental health | University | 1 × 90 min session with individual parents and parent–child dyads |
| Primary Care Stepping Stones Triple P and Stepping Stones Triple P Seminars [60,61] | Parents of children with a disability aged 2–12 years | Child behaviours Child developmental issues | Community | School Child care centres | Stepping Stones Triple P Seminar Series—1–3 × 90 min sessions with groups of parents Primary Care Stepping Stones Triple P—4 × 15–20 min individual parent sessions |
| RAD-PAL intervention (adaptation of Teen Intervene) [62] | Adolescents (13–17 years) who use substances and their parents/caregivers | Adolescent substance use | University | Community | 1 × parent session and 2 × adolescent sessions |
| Ready? Set. Go! [63] | Children 3–5 years who experience homelessness and high mobility and their parents | Child executive function | Community | Homelessness shelter Community preschool | 3 × 2 h sessions with groups of parents |
| Reducing Family Conflict Discussion Group [64] | Parents of adolescents 11–16 years where there is a concern about parent-adolescent conflict | Family conflict Adolescent Behaviour Problems Parenting and parent-adolescent relationship | Community | Community | 1 × 2 h sessions with groups of parents |
| Relationship Education [65] | Pregnant women on low income | Relationship distress and satisfaction Parental stress and coping | Community | Community | 4 × 3 h sessions with groups of expectant mothers and their partners |
| School readiness coaching [66] | Parents of children (3–5 years old) attending a well-child clinic | Parents’ perception of school readiness coaching intervention | Paediatrics | Paediatric clinic | 1 h session with a mother and a child (15 min child assessment and 45 min parent coaching) |
| Sexuality Training [67] | Parents/caregivers of children diagnosed with intellectual and developmental disabilities | Parental attitudes and beliefs, level of communication and competence to teach sexuality topics | Education and disability | Autism and developmental disorder conference | 1 × 60 min session with groups of parents |
| Short-term Psychodynamic Infant-Parent Intervention at Child Health Centres [68] | Mothers of children 0–2 years who are experiencing distress | Parental stress Infant socio-emotional functioning | Mental health Child health centres | Child health centres | 4 × 45 min sessions with individual parents or individual parent–child dyads or individual whole families |
| SOS-DoC framework counselling sessions [69] | Pregnant women who experienced intimate partner violence | Family function (family communication, family support, family difficulty) | Antenatal | Hospital/Antenatal clinic | 3 × 1–2 h individual sessions at two-week intervals |
| Single-session interventions * [70] Single Session Family Consultation [71] Single Session Family Therapy [72] Walk-In Together Online Session [73] | Aboriginal families participating in therapy Children and young people with mental health difficulties and their families Children and young people with mental health difficulties and their families Families experiencing various vulnerabilities or adversities | Family-identified goals Family engagement Family-identified goals Family worry Family confidence Family-identified goals | Mental health Mental health Community | Clinic Clinic Community Online | 1–3 × 1–1.5 h sessions with the family and a follow-up phone call 1 or more sessions with the family and a follow up phone call 1 × 60–75 min session with at least two family members |
| Single Session Intervention [74] | Families with children with eating disorders (who are on a waitlist for Family Based Therapy) | Child eating disorder | Counselling and treatment service | Clinic and online | 1 × up to 90 min individual session |
| Single-session parent sleep educational intervention [75] | Parents of school-aged children (7–14 years) with neurodevelopmental or mental health disorders and with a suspicion of a behavioural sleep-problem | Child sleep | Mental health | Clinic | 1 × 45 min session with groups of parents |
| Single Session Personalised Intervention [76] | War refugee parents of adolescents 10–15 years [76] | Parental self-efficacy | University | Home | 1 × session with individual parents |
| Solution-focused Brief Therapy [77] | Families referred for family therapy | Family-identified goals | Family services | Community | 1 × 68 min session with family |
| Uncle Lightfoot [78] | Parents of children 3–8 years with nighttime fears | Child nighttime fears | University | Home | 1 training session with individual parents Each evening × 5 weeks parent delivered therapy (6 hrs per week on average) |
| Video-feedback intervention [79] | Mother with depressive symptoms and her baby | Therapeutic change expression during a mentalisation-informed intervention | MH | Online | 1 pre-intervention session and 4 intervention sessions with mother-child dyad |
| Workshop for Family Based Treatment [80] | Parents of adolescents with restrictive eating disorders | Parental self-efficacy Adolescent weight gain | Health | Specialist service | 1 × 3 h workshop with groups of parents |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamilton, V.; Sartore, G.-M.; Macvean, M.; Avdagic, E.; Petrovic, Z.; Hunter, C.; Wade, C. Brief Interventions for Families Seeking Support from Family Services: A Scoping Review. Int. J. Environ. Res. Public Health 2025, 22, 841. https://doi.org/10.3390/ijerph22060841
Hamilton V, Sartore G-M, Macvean M, Avdagic E, Petrovic Z, Hunter C, Wade C. Brief Interventions for Families Seeking Support from Family Services: A Scoping Review. International Journal of Environmental Research and Public Health. 2025; 22(6):841. https://doi.org/10.3390/ijerph22060841
Chicago/Turabian StyleHamilton, Victoria, Gina-Maree Sartore, Michelle Macvean, Elbina Avdagic, Zvezdana Petrovic, Cathryn Hunter, and Catherine Wade. 2025. "Brief Interventions for Families Seeking Support from Family Services: A Scoping Review" International Journal of Environmental Research and Public Health 22, no. 6: 841. https://doi.org/10.3390/ijerph22060841
APA StyleHamilton, V., Sartore, G.-M., Macvean, M., Avdagic, E., Petrovic, Z., Hunter, C., & Wade, C. (2025). Brief Interventions for Families Seeking Support from Family Services: A Scoping Review. International Journal of Environmental Research and Public Health, 22(6), 841. https://doi.org/10.3390/ijerph22060841