


Disparities in Healthcare Utilization Among Vulnerable Populations During the COVID-19 Pandemic in Brazil: An Intersectional Analysis

 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
- −
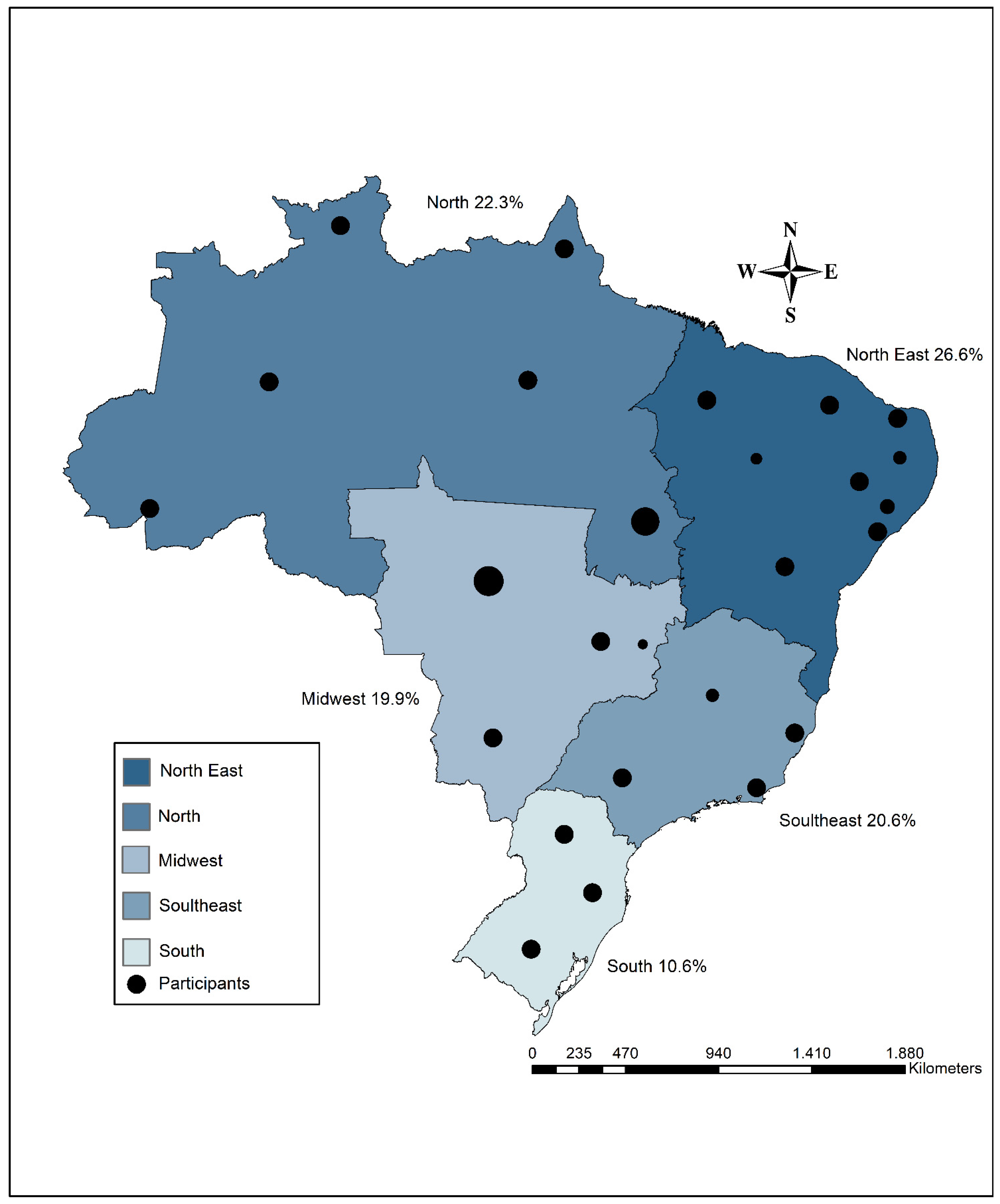
- North (Acre, Amapá, Amazonas, Pará, Rondônia, Roraima, and Tocantins),
- −
- Northeast (Alagoas, Bahia, Ceará, Maranhão, Paraíba, Pernambuco, Piauí, Rio Grande do Norte, and Sergipe),
- −
- Midwest (Goiás, Mato Grosso, and Mato Grosso do Sul),
- −
- Southeast (São Paulo, Minas Gerais, Rio de Janeiro, and Espírito Santo), and
- −
- South (Paraná, Santa Catarina, and Rio Grande do Sul).
2.2. Study Population
- (a)
- homeless individuals—native or naturalized Brazilians who had lived on public streets, in shelters, or in similar locations designated for this population for at least six months during the COVID-19 pandemic;
- (b)
- migrants and refugees—individuals from other countries who had resided in Brazil for at least six months during the pandemic and had basic proficiency in interpreting or understanding the Portuguese language;
- (c)
- residents of slums—native or naturalized Brazilians living in urban areas characterized by inadequate housing and poor infrastructure (such as favelas, informal settlements, or urban occupations) during the pandemic;
- (d)
- residents of camps, settlements, or occupations—native or naturalized Brazilians who had lived in these areas for at least six months during the pandemic.
2.3. Sampling
2.4. Healthcare System in Brazil
2.5. Survey Questionnaire and Data Collection Procedure
2.6. Data Collected and Study Variables
- Sex/Gender: Male, Female, Transgender, or Other;
- Age Group: 18–29 years, 30–59 years, or 60 years and older;
- Race/Ethnicity: White, Black/Brown, Indigenous, or Asian;
- Marital Status: Married/In a Stable Union, Widowed, Separated, or Single;
- Education Level: No Formal Education, Incomplete Primary Education, Complete Primary Education, Incomplete Higher Education, or Higher Education;
- Employment Status: Formal Employment, Informal Employment, Unemployed, Student, Retired, or Other;
- Monthly Income: No income, Less than one minimum wage, One to two minimum wages, Two to three minimum wages, or More than three minimum wages;
- Receipt of Government Assistance: Yes or No.
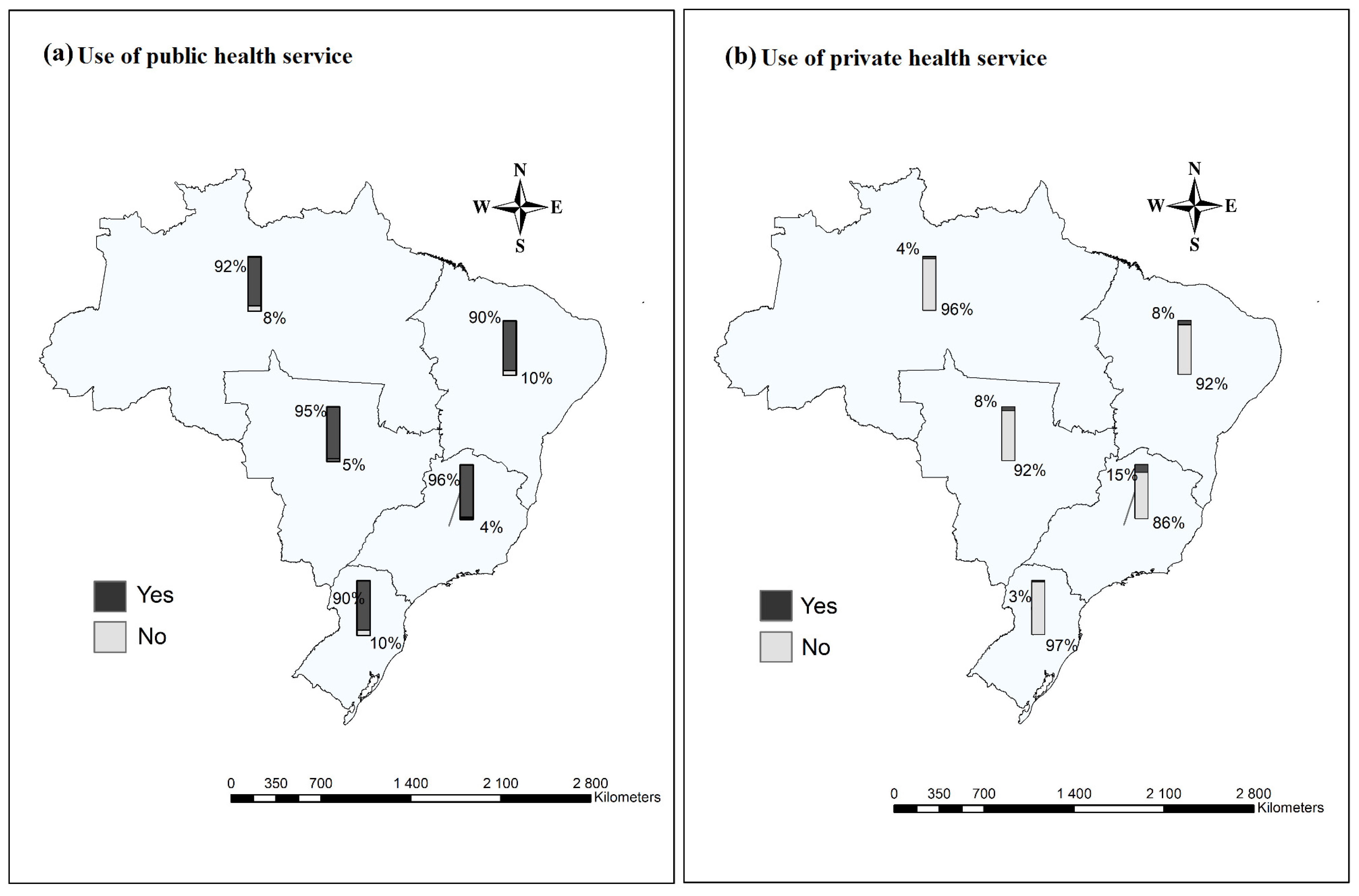
- Utilization of Public Healthcare Services: Yes or No;
- Utilization of Private Healthcare Services: Yes or No.
2.7. Statistical Analysis
2.8. Ethical Aspects
3. Results
3.1. Demographics
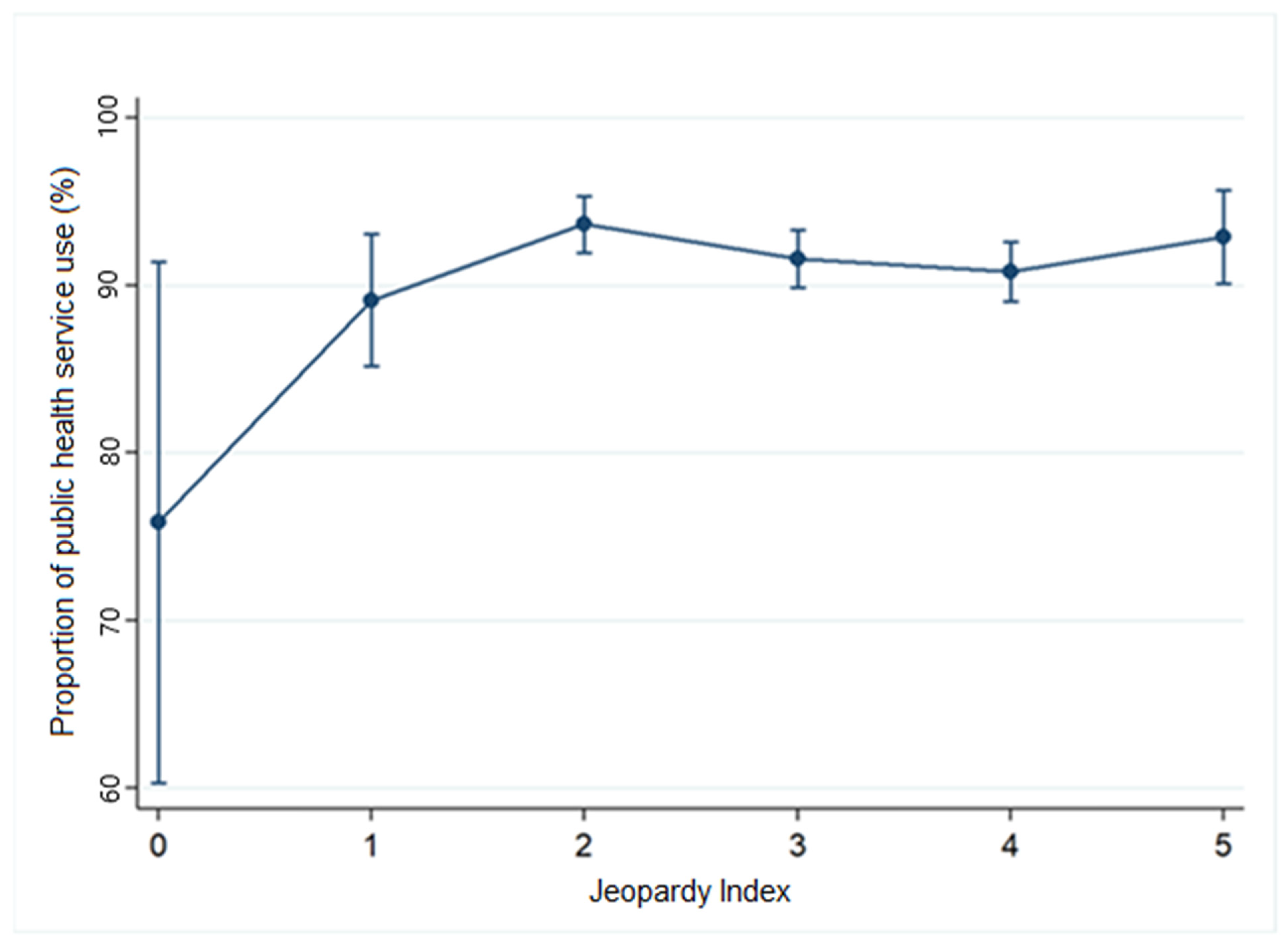
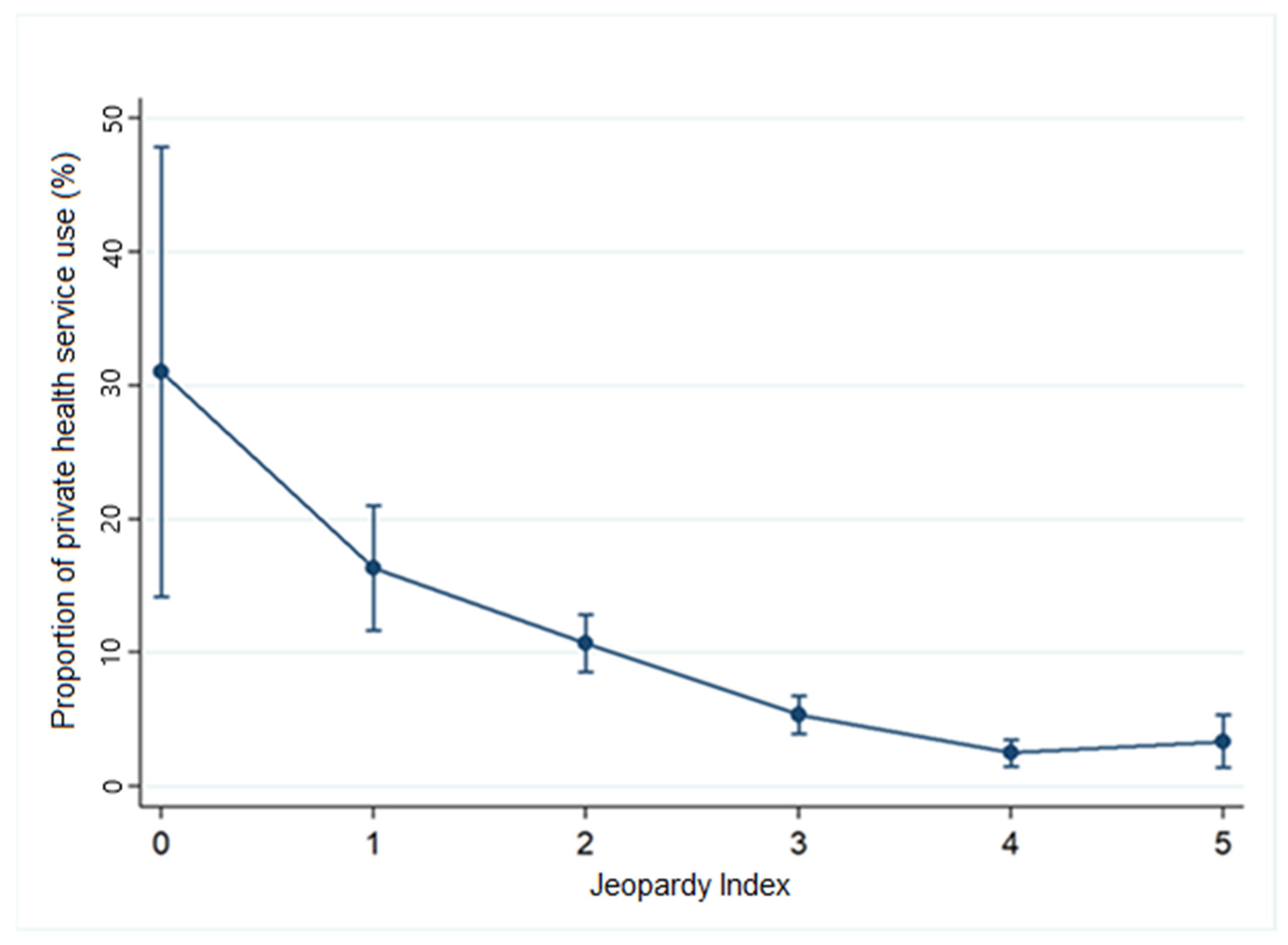
3.2. Regression and Proportions Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lazzari, E.A.; Paschoalotto, M.A.C.; Massuda, A.; Rocha, R.; Castro, M.C. Social determinants of health in Brazil during the COVID-19 pandemic: Strengths and limitations of emergency responses. Health Aff. Sch. 2023, 1, qxad014. [Google Scholar] [CrossRef] [PubMed]
- FGV SOCIAL. Mapa da Nova Pobreza: Retrato da Pobreza No Brasil em 2021. Available online: https://repositorio.fgv.br/server/api/core/bitstreams/80762296-e1b2-46da-8927-2b59438b3acc/content (accessed on 30 April 2025).
- Blundell, R.; Costa Dias, M.; Joyce, R.; Xu, X. COVID-19 and Inequalities. Fisc. Stud. 2020, 41, 291–319. [Google Scholar] [CrossRef] [PubMed]
- Sangra, S.; Razdan, N.; Gupta, S.; Dwivedi, N. A Study on Community Needs, Perceptions, and Demand Regarding the Use of Health Services During the COVID-19 Pandemic in District Kathua, J and K. J. Fam. Med. Prim. Care 2023, 12, 3092–3097. [Google Scholar] [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Síntese de Indicadores Sociais: Uma Análise das Condições de vida da População Brasileira. 2019. Available online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv101681_informativo.pdf (accessed on 30 April 2025).
- Tomasiello, D.B.; Bazzo, J.; Parga, J.; Servo, L.M.S.; Pereira, R.H.M. Desigualdades Raciais e de Renda no Acesso à Saúde nas Cidades Brasileiras; Texto para Discussão nº 2832; Instituto de Pesquisa Econômica Aplicada (IPEA): Brasília, Brazil, 2023. Available online: https://repositorio.ipea.gov.br/handle/11058/11454 (accessed on 30 April 2025).
- Fundação Oswaldo Cruz (FIOCRUZ). COVID-19: Desigualdades Sociais e Saúde. Boletim Observatório COVID-19 Fiocruz; Fiocruz: Rio de Janeiro, Brazil, 2021; Available online: https://portal.fiocruz.br/noticia/fiocruz-analisa-desigualdades-sociais-e-impacto-da-covid-19 (accessed on 30 April 2025).
- Crenshaw, K. Demarginalizing the intersection of race and sex: A Black feminist critique of antidiscrimination doctrine, feminist theory, and antiracist politics. Univ. Chic. Leg. Forum 1989, 1, 139–167. Available online: https://chicagounbound.uchicago.edu/uclf/vol1989/iss1/8 (accessed on 30 April 2025).
- El Arab, R.A.; Somerville, J.; Abuadas, F.H.; Rubinat-Arnaldo, E.; Sagbakken, M. Health and Well-Being of Refugees, Asylum Seekers, Undocumented Migrants, and Internally Displaced Persons under COVID-19: A Scoping Review. Front. Public Health 2023, 11, 1145002. [Google Scholar] [CrossRef]
- Schnittfinke, T.; Greiving, S.; Nyamai, D.N.; Scholz, W.; Schramm, S.; Behrens, R.; Zuidgeest, M.; Rink, B.; Momm, S.; Travassos, L.; et al. Criticality assessment and cascading effects: Impacts of COVID-19 disruptions in public transport on marginalized groups in Dortmund, Germany, São Paulo, Brazil, and Cape Town, South Africa. J. Surveill. Secur. Saf. 2024, 5, 140–159. [Google Scholar] [CrossRef]
- Siersbaek, R.; O’Donnell, C.; Parker, S.; Ford, J.; Burke, S.; Cheallaigh, C.N. Social exclusion and its impact on health over the life course: A realist review protocol. HRB Open Res. 2023, 6, 34. [Google Scholar] [CrossRef]
- Kuran, C.H.A.; Morsut, C.; Kruke, B.I.; Krüger, M.; Segnestam, L.; Orru, K.; Nævestad, T.O.; Airola, M.; Keränen, J.; Gabel, F.; et al. Vulnerability and vulnerable groups from an intersectionality perspective. Int. J. Disaster Risk Reduct. 2020, 50, 101826. [Google Scholar] [CrossRef]
- Garcia, L.F.; Bernuci, M.P.; Marques, A.G.; Bertolini, S.M.M.; Silva, T.M.G.D. A case study of social vulnerability: Thoughts for the promotion of health. Rev. Bioética 2019, 27, 430–438. [Google Scholar] [CrossRef]
- Rohwerder, B.; Szyp, C. The Risks and Outcomes of Getting Help for Marginalised People: Navigating Access to Social Assistance in Crises; Institute of Development Studies: Brighton, UK, 2022. [Google Scholar]
- van Ginneken, E.; Siciliani, L.; Reed, S.; Eriksen, A.; Tille, F.; Zapata, T. Addressing backlogs and managing waiting lists during and beyond the COVID-19 pandemic. Eurohealth 2022, 28, 35–40. [Google Scholar]
- Fausto, M.C.R.; Almeida, P.F.D.; Bousquat, A.; Lima, J.G.; Santos, A.M.D.; Seidl, H.; Mendonça, M.H.M.D.; Cabral, L.M.D.S.; Giovanella, L. Atenção Primária à Saúde em municípios rurais remotos brasileiros: Contexto, organização e acesso à atenção integral no Sistema Único de Saúde. Saúde Soc. 2023, 32, e220382pt. [Google Scholar] [CrossRef]
- Bufrem, L.S. A pandemia da COVID-19 no Brasil: Informações e contradições na atual conjuntura. P2P Inov. 2020, 7, 101–120. [Google Scholar] [CrossRef]
- Khanijahani, A.; Iezadi, S.; Gholipour, K.; Azami-Aghdash, S.; Naghibi, D. A systematic review of racial/ethnic and socioeconomic disparities in COVID-19. Int. J. Equity Health 2021, 20, 248. [Google Scholar] [CrossRef] [PubMed]
- Cappelli, F. Investigating the origins of differentiated vulnerabilities to climate change through the lenses of the Capability Approach. Econ. Polit. 2023, 40, 1051–1074. [Google Scholar] [CrossRef]
- Passos, M.D.C. Emenda Constitucional Nº 95/2016: Uma Análise Desde a Proposta até a sua Aprovação no Legislativo Federal. Master’s Thesis, Universidade do Estado da Bahia, Salvador, Brazil, 2023. [Google Scholar]
- Araújo, C.E.L.; Gonçalves, G.Q.; Machado, J.A. Brazilian municipalities and their own expenditures on health: Some associations. Ciênc. Saúde Colet. 2017, 22, 953–963. [Google Scholar] [CrossRef]
- Soares Filho, A.M.; Vasconcelos, C.H.; Dias, A.C.; Souza, A.C.C.D.; Merchan-Hamann, E.; Silva, M.R.F.D. Primary Health Care in Northern and Northeastern Brazil: Mapping team distribution disparities. Ciênc. Saúde Colet. 2022, 27, 377–386. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action. 2007. Available online: https://www.who.int/publications/i/item/everybody-s-business----strengthening-health-systems-to-improve-health-outcomes (accessed on 20 January 2025).
- Parajuli, J.; Horey, D. Barriers to and Facilitators of Health Services Utilisation by Refugees in Resettlement Countries: An Overview of Systematic Reviews. Aust. Health Rev. 2019, 44, 132–142. [Google Scholar] [CrossRef]
- Baeten, R.; Spasova, S.; Vanhercke, B.; Coster, S. Inequalities in Access to Healthcare. A Study of National Policies, European Social Policy Network (ESPN); European Commission: Brussels, Belgium, 2018. [Google Scholar]
- Rothman, K.J.; Greenland, S.; Lash, T.L. Modern Epidemiology, 3rd ed.; thoroughly rev. and updated; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; Available online: https://www.academia.edu/37995138/Epidemiologia_Moderna_3a_Edi%C3%A7%C3%A3o (accessed on 23 March 2023).
- Romanowski, F.N.d.A.; de Castro, M.B.; Neris, N.W. Manual de Tipos de Estudo. Centro Universitário de Anápolis. Pró-Reitoria de Pós-Graduação, Pesquisa, Extensão e Ação Comunitária. Programa de Pós-Graduação em Odontologia. 2019. Available online: http://repositorio.aee.edu.br/bitstream/aee/15586/1/MANUAL%20DE%20TIPOS%20DE%20ESTUDO.pdf (accessed on 20 January 2025).
- Tavares, V. Revista Poli Debate por que a COVID-19 Atinge Mais os Negros. Agência Fiocruz de Notícias. 6 November 2020. Available online: https://agencia.fiocruz.br/revista-poli-debate-por-que-covid-19-atinge-mais-os-negros (accessed on 28 April 2025).
- Santos, M.P.A.D.; Nery, J.S.; Goes, E.F.; Silva, A.D.; Santos, A.B.S.D.; Batista, L.E.; Araújo, E.; Maria, D. População negra e COVID-19: Reflexões sobre racismo e saúde. Estud. Avançados 2020, 34, 225–244. [Google Scholar] [CrossRef]
- Wise, J. COVID-19: WHO declares end of global health emergency. BMJ 2023, 381, 1041. [Google Scholar] [CrossRef]
- da Fonseca, E.M.; Shadlen, K.C.; Bastos, F.I. The politics of COVID-19 vaccination in middle-income countries: Lessons from Brazil. Soc. Sci. Med. 2021, 281, 114093. [Google Scholar] [CrossRef]
- Aquino, E.M.; Silveira, I.H.; Pescarini, J.M.; Aquino, R.; Souza-Filho, J.A.D.; Rocha, A.D.S.; Ferreira, A.; Victor, A.; Teixeira, C.; Machado, D.B. Social distancing measures to control the COVID-19 pandemic: Potential impacts and challenges in Brazil. Cienc. Saude Coletiva 2020, 25, 2423–2446. [Google Scholar] [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia e Estatística. Áreas Territoriais—Brasil, Grandes Regiões, Unidades da Federação e Municípios. Available online: https://www.ibge.gov.br/geociencias/organizacao-do-territorio/estrutura-territorial/15761-areas-dos-municipios.html (accessed on 30 January 2025).
- Mohamad, M.A.; Sapsis, T.P. Sequential sampling strategy for extreme event statistics in nonlinear dynamical systems. Proc. Natl. Acad. Sci. USA 2018, 115, 11138–11143. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.C.; Massuda, A.; Almeida, G.; Menezes-Filho, N.A.; Andrade, M.V.; de Souza Noronha, K.V.M.; Rocha, R.; Macinko, J.; Hone, T.; Tasca, R.; et al. Brazil’s unified health system: The first 30 years and prospects for the future. Lancet 2019, 394, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Gomes, I. Síntese de Indicadores Sociais. Pobreza cai para 31.6% da População em 2022, após Alcançar 36.7% em 2021. Estatísticas Sociais. Notícias Agência IBGE. 2023. Available online: https://agenciadenoticias.ibge.gov.br/agencia-noticias/2012-agencia-de-noticias/noticias/38545-pobreza-cai-para-31-6-da-populacao-em-2022-apos-alcancar-36-7-em-2021#:~:text=O%20percentual%20de%20pessoas%20em,7%20milh%C3%B5es%20na%20extrema%20pobreza (accessed on 23 July 2024).
- Pereira, B.L.S.; Oliveira Junior, A.C.R.D.; Faleiros, D.R. Ordinance 3992/2017: Challenges and advances for resource management in the Brazilian Unified Health System (SUS). Rev. Saude Publica 2019, 53, 58. [Google Scholar] [CrossRef]
- Canton, H. Organisation for economic co-operation and development—OECD. In The Europa Directory of International Organizations 2021; Routledge: London, UK, 2021; pp. 677–687. [Google Scholar]
- Rocha, R.; Atun, R.; Massuda, A.; Rache, B.; Spinola, P.; Nunes, L.; Lago, M.; Castro, M.C. Effect of socioeconomic inequalities and vulnerabilities on health-system preparedness and response to COVID-19 in Brazil: A comprehensive analysis. Lancet Glob. Health 2021, 9, e782–e792. [Google Scholar] [CrossRef]
- Laires, P.A.; Dias, S.; Gama, A.; Moniz, M.; Pedro, A.R.; Soares, P.; Aguiar, P.; Nunes, C. The association between chronic disease and serious COVID-19 outcomes and its influence on risk perception: Survey study and database analysis. JMIR Public Health Surveill. 2021, 7, e22794. [Google Scholar] [CrossRef]
- Pedro, A.R.; Gama, A.; Soares, P.; Moniz, M.; Laires, P.A.; Dias, S. COVID-19 Barometer: Social Opinion—What Do the Portuguese Think in This Time of COVID-19? Port. J. Public Health 2020, 38, 42–50. [Google Scholar] [CrossRef]
- Soares, P.; Rocha, J.V.; Moniz, M.; Gama, A.; Laires, P.A.; Pedro, A.R.; Dias, S.; Leite, A.; Nunes, C. Factors associated with COVID-19 vaccine hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef]
- Zarili, T.F.T.; Castanheira, E.R.L.; Nunes, L.O.; Sanine, P.R.; Carrapato, J.F.L.; Machado, D.F.; Ramos, N.P.; Mendonça, C.S.; Nasser, M.A.; Andrade, M.C.; et al. Técnica Delphi no processo de validação do Questionário de Avaliação da Atenção Básica (QualiAB) para aplicação nacional. Saúde Soc. 2021, 30, e190505. [Google Scholar] [CrossRef]
- Data collection instrument in Brazilian Portuguese. Termômetro Social COVID-19 Versão 4.0. Available online: https://figshare.com/articles/online_resource/Data_collection_instrument_in_Brazilian_Portuguese/25917571 (accessed on 30 January 2025).
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa Nacional por Amostra de Domicílios Contínua: Principais Resultados 2023; IBGE: Rio de Janeiro, Brazil, 2024. Available online: https://www.ibge.gov.br/ (accessed on 28 April 2025).
- International Labour Organization (ILO). World Employment and Social Outlook: Trends 2021; ILO: Geneva, Switzerland, 2021; Available online: https://www.ilo.org/ (accessed on 28 April 2025).
- World Health Organization (WHO). Guidance on COVID-19 for the Care of Older People and People Living in Long-Term Care Facilities, Other Non-Acute Care Facilities and Home Care; WHO: Geneva, Switzerland, 2020; Available online: https://iris.who.int/handle/10665/331913 (accessed on 28 April 2025).
- Instituto Brasileiro de Geografia e Estatística (IBGE). Síntese de Indicadores Sociais; IBGE: Rio de Janeiro, Brazil, 2022. Available online: https://www.ibge.gov.br/estatisticas/multidominio/condicoes-de-vida-desigualdade-e-pobreza/9221-sintese-de-indicadores-sociais.html (accessed on 21 November 2024).
- Taylor, D.; Richards, D. Triple jeopardy: Complexities of racism, sexism, and ageism on the experiences of mental health stigma among young Canadian black women of Caribbean descent. Front. Sociol. 2019, 4, 43. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, S.; Caraballo, C.; Lu, Y.; Valero-Elizondo, J.; Massey, D.; Annapureddy, A.R.; Roy, B.; Riley, C.; Murugiah, K.; Onuma, O.; et al. Trends in differences in health status and health care access and affordability by race and ethnicity in the United States, 1999–2018. JAMA 2021, 326, 637–648. [Google Scholar] [CrossRef]
- Chandra, A.; Kakani, P.; Sacarny, A. Hospital allocation and racial disparities in health care. Rev. Econ. Stat. 2024, 106, 924–937. [Google Scholar] [CrossRef]
- Thakral, M.; Lacroix, A.Z.; Molton, I.R. Sex/gender disparities in health outcomes of individuals with long-term disabling conditions. Rehabil. Psychol. 2019, 64, 221. [Google Scholar] [CrossRef]
- Gibb, J.K.; DuBois, L.Z.; Williams, S.; McKerracher, L.; Juster, R.; Fields, J. Sexual and gender minority health vulnerabilities during the COVID-19 health crisis. Am. J. Hum. Biol. 2020, 32, e23499. [Google Scholar] [CrossRef]
- Local Burden of Disease Educational Attainment Collaborators. Mapping disparities in education across low-and middle-income countries. Nature 2020, 577, 235–238. [Google Scholar] [CrossRef]
- Artiga, S.; Orgera, K.; Pham, O. Disparities in Health and Health Care: Five Key Questions and Answers; Kaiser Family Foundation: San Francisco, CA, USA, 2020. [Google Scholar]
- Santiago, M.; Akkari, A. Citizenship, social exclusion and education in Latin America: The case of Brazil. In Global Citizenship Education: Critical and International Perspectives; Springer International Publishing: Cham, Switzerland, 2020; pp. 17–30. [Google Scholar]
- Oviedo, D. Making the links between accessibility, social and spatial inequality, and social exclusion: A framework for cities in Latin America. In Advances in Transport Policy and Planning; Academic Press: Cambridge, MA, USA, 2021; pp. 135–172. [Google Scholar]
- Souza, P.H. A history of inequality: Top incomes in Brazil, 1926–2015. Res. Soc. Stratif. Mobil. 2018, 57, 35–45. [Google Scholar] [CrossRef]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pessoas Pretas e Pardas Continuam com Menor Acesso a Emprego, Educação, Segurança e Saneamento. Agência IBGE de Notícias. 2023. Available online: https://agenciadenoticias.ibge.gov.br/agencia-noticias/2012-agencia-de-noticias/noticias/35467-pessoas-pretas-e-pardas-continuam-com-menor-acesso-a-emprego-educacao-seguranca-e-saneamento (accessed on 17 December 2024).
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pobreza cai para 31.6% da População em 2022, após Alcançar 36.7% em 2021. Agência IBGE de Notícias. 2023. Available online: https://agenciadenoticias.ibge.gov.br/agencia-noticias/2012-agencia-de-noticias/noticias/38545-pobreza-cai-para-31-6-da-populacao-em-2022-apos-alcancar-36-7-em-2021 (accessed on 17 December 2024).
- Abramo, L.; Cecchini, S.; Morales, B. Social Programmes, Poverty Eradication and Labour Inclusion Lessons from Latin America and the Caribbean; United Nations: New York, NY, USA, 2019. [Google Scholar]
- Moura, H.S.D.; Berra, T.Z.; Rosa, R.J.; Silva, R.V.d.S.; Soares, D.d.A.; de Araújo, J.S.T.; Costa, F.B.P.; de Souza, R.M.P.; Nascimento, M.C.D.; Teibo, T.K.A.; et al. Health condition, income loss, food insecurity and other social inequities among migrants and refugees during the COVID-19 pandemic in Brazil. BMC Public Health 2023, 23, 1728. [Google Scholar] [CrossRef]
- Chaves, L.A.; Andrade, E.I.G.; Santos, A.D.F.D. Configuração das Redes de Atenção à Saúde no SUS: Análise a partir de componentes da atenção básica e hospitalar. Ciência Saúde Coletiva 2024, 29, e18392022. [Google Scholar] [CrossRef]
- dos Santos, F.F.S.; Daltro Filho, J.; Machado, C.T.; Vasconcelos, J.F.; Feitosa, F.R.S. O desenvolvimento do saneamento básico no Brasil e as consequências para a saúde pública. Rev. Bras. Meio Ambiente 2018, 4. [Google Scholar]
- Figueiredo, D.C.M.M.D.; Shimizu, H.E.; Ramalho, W.M. A Acessibilidade da Atenção Básica no Brasil na avaliação dos usuários. Cad. Saúde Coletiva 2020, 28, 288–301. [Google Scholar] [CrossRef]
- Ferreira, D.C.; Graziele, I.; Marques, R.C.; Gonçalves, J. Investment in drinking water and sanitation infrastructure and its impact on waterborne diseases dissemination: The Brazilian case. Sci. Total Environ. 2021, 779, 146279. [Google Scholar] [CrossRef] [PubMed]
- Razafindrakoto, M.; Roubaud, F.; Saboia, J.; Castilho, M.R.; Pero, V. Municípios in the Time of COVID-19 in Brazil: Socioeconomic Vulnerabilities, Transmission Factors and Public Policies. Eur. J. Dev. Res. 2022, 34, 2730–2758. [Google Scholar] [CrossRef]
- Oliveira, L.G.F.; Fracolli, L.A.; Araújo, S.S.D.; Gryschek, A.L.D.F.P.L.; Silva, G.L.; Lico, F.M.D.C.; Silva, L.A.D.; Farias, L.G.; Fogueira, J.A.L.; Silva, J.C.N. Acesso e uso equitativo dos serviços de saúde: Um desafio para a promoção da universalização em saúde. In Acesso à Saúde: Desafios, Perspectivas, Soluções e Oportunidades na Atenção Primária à Saúde; Pedro & João Editores: Santo Andre, Brazil, 2023. [Google Scholar]
- Arruda, N.M.; Maia, A.G.; Alves, L.C. Desigualdade no acesso à saúde entre as áreas urbanas e rurais do Brasil: Uma decomposição de fatores entre 1998 a 2008. Cad. Saúde Pública 2018, 34, e00213816. [Google Scholar] [CrossRef]
- Massuda, A.; Hone, T.; Leles, F.A.G.; de Castro, M.C.; Atun, R. The Brazilian health system at crossroads: Progress, crisis and resilience. BMJ Glob. Health 2018, 3, e000829. [Google Scholar] [CrossRef]
- Litewka, S.G.; Heitman, E. Latin American healthcare systems in times of pandemic. Dev. World Bioeth. 2020, 20, 69–73. [Google Scholar] [CrossRef]
- Machado, C.V.; e Silva, G.A. Political struggles for a universal health system in Brazil: Successes and limits in the reduction of inequalities. Glob. Health 2019, 15, 1–12. [Google Scholar] [CrossRef]
- Pereira, R.H.; Braga, C.K.V.; Serra, B.; Nadalin, V.G. Desigualdades socioespaciais de acesso a oportunidades nas cidades brasileiras-2019 (No. 2535). Texto para discussão. 2019. Available online: https://repositorio.ipea.gov.br/bitstream/11058/9586/1/td_2535.pdf (accessed on accessed on 28 April 2025).
- Ribeiro, D.F.; Saito, S.M.; dos Santos Alvalá, R.C. Disaster vulnerability analysis of small towns in Brazil. Int. J. Disaster Risk Reduct. 2022, 68, 102726. [Google Scholar] [CrossRef]
- Monteiro, S.; Brigeiro, M. Experiências de acesso de mulheres trans/travestis aos serviços de saúde: Avanços, limites e tensões. Cad. Saúde Pública 2019, 35, e00111318. [Google Scholar] [CrossRef]
- de Souza, I.M.; Anunciação, D.; de Araújo, E.M.; da Silva, H.P.; Pereira, L.L.; Nunes, A.P.N.; Flauzino, R.F. Saúde da população negra: Desafios para a construção da equidade em saúde. Ciência Saúde Coletiva 2024, 29, e00142024. [Google Scholar] [CrossRef] [PubMed]
- da Silva, N.N.; Favacho, V.B.C.; Boska, G.d.A.; Andrade, E.d.C.; das Merces, N.P.; de Oliveira, M.A.F. Acesso da população negra a serviços de saúde: Revisão integrativa. Rev. Bras. Enferm. 2020, 73, e20180834. [Google Scholar]
- da Silva Lopes, I.; de Ulysséa Leal, D.; Melo, P.V. COVID-19 and Necropolitics: The Absence of Race and Gender Intersectional Analysis in Pandemic Data in Brazil. In Black Lives Matter in Latin America: Continuities in Racism, Cross-National Resistance and Mobilization in the Americas; Springer Nature: Cham, Switzerland, 2024; pp. 121–149. [Google Scholar]
- Brito, L.; Borges, L.; Fortes, P.D.; Gomes, A. Impactos Sociais da COVID-19: Uma Perspectiva Sensível às Desigualdades de Gênero. 2020. Available online: https://www.arca.fiocruz.br/handle/icict/41375 (accessed on accessed on 28 April 2025).
- Martins, M.B. Atenção Primária à Saúde e Enquadramentos de Vulnerabilidades na Implementação de Políticas Públicas. 2024. Available online: http://hdl.handle.net/10183/281898 (accessed on accessed on 28 April 2025).
- de Andrade, A.T. O escalonamento do Cuidado como Estratégia de Organização da Rede de Atenção Psicossocial e Fortalecimento da Atenção Primária à Saúde. 2023. Available online: https://repositorio.ufc.br/handle/riufc/78430 (accessed on accessed on 28 April 2025).
- Mezzomo, A.L.; Filho, T.A.G.; Benvindo, S.d.S. Desigualdades Expostas: Reflexões Sobre Racismo Ambiental e Saúde Na Pandemia De COVID-19. J. Humanit. And Soc. Sci. 2024, 29, 6–12. [Google Scholar]
- Jacobovski, R. Reflexão crítica sobre a saúde pública brasileira: Capitalismo, pandemia de COVID-19 e sociedade. Florence Interdiscip. J. Health Sustain. 2023, 1, 1–4. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) |
|---|---|
| Sex/Gender | |
| Male | 2045 (60.0) |
| Female Transgender | 1302 (38.2) 53 (1.6) |
| Others | 5 (0.1) |
| No reply | 1 (0.0) |
| Age (years) | |
| 18 to 29 | 877 (25.7) |
| 30 to 59 | 2218 (65.1) |
| 60 years or older | 311 (9.1) |
| Race/color | |
| White | 747 (22.0) |
| Black/brown | 2460 (72.2) |
| Indigenous | 63 (1.8) |
| Asian | 102 (3.0) |
| No reply | 34 (1.0) |
| Marital status | |
| Married or in a stable union | 987 (29.0) |
| Widowed, separated, or single | 2418 (71.0) |
| No reply | 1 (0.0) |
| Education | |
| No formal education | 145 (4.3) |
| Complete primary education | 1483 (43.5) |
| Completed high school | 1329 (39.0) |
| Complete university or post-graduate degree | 447 (13.1) |
| No reply | 2 (0.1) |
| Occupation/Employment | |
| Formal employment | 490 (14.3) |
| Informal employment | 1102 (32.4) |
| Unemployed | 1328 (39.0) |
| Student | 143 (4.2) |
| Retired/Pensioner | 187 (5.5) |
| Others | 155 (4.6) |
| No reply | 1 (0.0) |
| Monthly income | |
| No income | 833 (24.5) |
| Less than 1 minimum wage | 1267 (37.2) |
| From 1 to 2 minimum wages | 746 (21.9) |
| From 2 to 3 minimum wages | 184 (5.4) |
| Above 3 minimum wages | 116 (3.4) |
| No reply | 260 (7.6) |
| Receives government aid | |
| Yes | 1460 (42.9) |
| No | 1943 (57.0) |
| No reply | 3 (0.1) |
| Utilization of Public Healthcare Services | |
| Yes | 3112 (91.4) |
| No | 284 (8.3) |
| No reply | 10 (0.3) |
| Utilization of Private Healthcare Services | |
| Yes | 222 (6.5) |
| No | 3167 (92.9) |
| No reply | 17 (0.6) |
| Variable | Odds Ratio [95% CI] | Marginal Effect | p-Value |
|---|---|---|---|
| 0—Male, White, Higher Education | - | 0.759 | Ref |
| 1—Woman, White, Higher Education | 4.69 [1.91–11.5] | 0.891 | 0.001 ** |
| 2—Woman, Asian or Black, Incomplete Higher Education | 3.45 [1.43–8.33] | 0.936 | 0.006 ** |
| 3—Cisgender Woman/Transgender person, Asian or Black, Complete Primary Education | 3.15 [1.31–7.58] | 0.916 | 0.010 * |
| 4—Cisgender Woman/Transgender person, Black, Incomplete Primary Education | 4.16 [1.60–10.7] | 0.908 | 0.003 ** |
| 5—Cisgender Woman/Transgender person, Black, No Formal Education | 3.14 [1.34–7.35] | 0.929 | 0.008 ** |
| Variable | Odds Ratio [95% CI] | Marginal Effect | p-Value |
|---|---|---|---|
| 0—Male, White, Higher Education | - | 0.479 | Ref |
| 1—Woman, White, Higher Education | 0.26 [0.11–0.06] | 0.210 | 0.002 ** |
| 2—Woman, Asian or Black, Incomplete Higher Education | 0.12 [0.05–0.28] | 0.128 | 0.00 *** |
| 3—Cisgender Woman/Transgender person, Asian or Black, Complete Primary Education | 0.05 [0.02–0.13] | 0.067 | 0.00 *** |
| 4—Cisgender Woman/Transgender person, Black, Incomplete Primary Education | 0.04 [0.20–0.98] | 0.035 | 0.040 * |
| 5—Cisgender Woman/Transgender person, Black, No Formal Education | 0.07 [0.02–0.20] | 0.053 | 0.00 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferezin, L.P.; Rosa, R.J.; Moura, H.S.D.; de Campos, M.C.T.; Delpino, F.M.; Nascimento, M.C.d.; Araújo, J.S.T.d.; Pinto, I.C.; Arcêncio, R.A. Disparities in Healthcare Utilization Among Vulnerable Populations During the COVID-19 Pandemic in Brazil: An Intersectional Analysis. Int. J. Environ. Res. Public Health 2025, 22, 831. https://doi.org/10.3390/ijerph22060831
Ferezin LP, Rosa RJ, Moura HSD, de Campos MCT, Delpino FM, Nascimento MCd, Araújo JSTd, Pinto IC, Arcêncio RA. Disparities in Healthcare Utilization Among Vulnerable Populations During the COVID-19 Pandemic in Brazil: An Intersectional Analysis. International Journal of Environmental Research and Public Health. 2025; 22(6):831. https://doi.org/10.3390/ijerph22060831
Chicago/Turabian StyleFerezin, Letícia Perticarrara, Rander Junior Rosa, Heriederson Sávio Dias Moura, Mônica Chiodi Toscano de Campos, Felipe Mendes Delpino, Murilo César do Nascimento, Juliana Soares Tenório de Araújo, Ione Carvalho Pinto, and Ricardo Alexandre Arcêncio. 2025. "Disparities in Healthcare Utilization Among Vulnerable Populations During the COVID-19 Pandemic in Brazil: An Intersectional Analysis" International Journal of Environmental Research and Public Health 22, no. 6: 831. https://doi.org/10.3390/ijerph22060831
APA StyleFerezin, L. P., Rosa, R. J., Moura, H. S. D., de Campos, M. C. T., Delpino, F. M., Nascimento, M. C. d., Araújo, J. S. T. d., Pinto, I. C., & Arcêncio, R. A. (2025). Disparities in Healthcare Utilization Among Vulnerable Populations During the COVID-19 Pandemic in Brazil: An Intersectional Analysis. International Journal of Environmental Research and Public Health, 22(6), 831. https://doi.org/10.3390/ijerph22060831