
Medically Attended Outpatient Parainfluenza Virus Infections in Young Children from a Single Site in Machala, Ecuador

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Subject Enrollment
2.2. Meteorologic Data Collection
2.3. Statistical Analysis
3. Results
3.1. All Enrolled Subjects
3.2. Subjects Whose Nasopharyngeal Samples Were Positive for the Detection of PIV
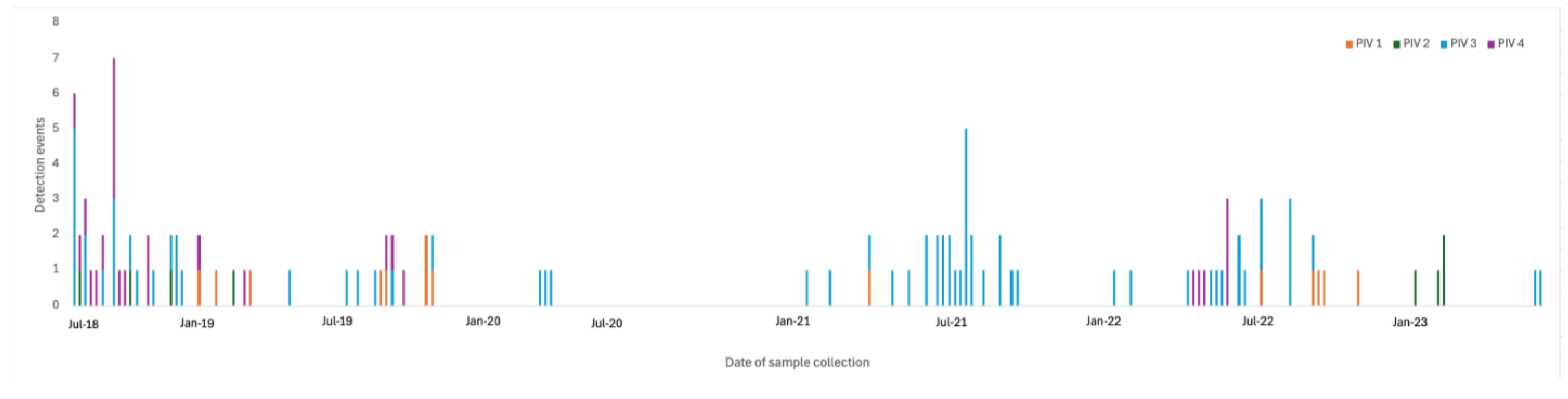
3.3. PIV Seasonality
3.4. Meteorologic Associations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rocha-Filho, C.R.; Ramalho, G.S.; Martins, J.W.L.; Lucchetta, R.C.; Pinto, A.C.P.N.; da Rocha, A.P.; Trevisani, G.F.M.; Reis, F.S.d.A.; Ferla, L.J.; Mastroianni, P.d.C.; et al. Economic burden of respiratory syncytial and parainfluenza viruses in children of upper-middle-income countries: A systematic review. J. Pediatr. 2023, 99, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Branche, A.R.; Falsey, A.R. Parainfluenza virus infection. Semin. Respir. Crit. Care Med. 2016, 37, 538–554. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Reeves, R.M.; Wang, X.; Bassat, Q.; Brooks, W.A.; Cohen, C.; Moore, D.P.; Nunes, M.; Rath, B.; Campbell, H.; et al. Global patterns in monthly activity of influenza virus, respiratory syncytial virus, parainfluenza virus, and metapneumovirus: A systematic analysis. Lancet Glob. Health 2019, 7, e1031–e1045. [Google Scholar] [CrossRef] [PubMed]
- Institute for Health Metrics and Evaluation: Ecuador. Available online: https://www.healthdata.org/research-analysis/health-by-location/profiles/ecuador (accessed on 30 January 2025).
- Ecuadorian National Institute for Statistics and Census. Available online: https://www.ecuadorencifras.gob.ec/documentos/web-inec/Sitios/Defunciones/ (accessed on 30 January 2025).
- Sippy, R.; Prado, E.O.; Fajardo, F.P.; Hidalgo, I.; Aguilar, G.V.; Bonville, C.A.; Aponte, C.C.; Gómez, M.S.; Aponte, J.L.C.; Cordova, M.B.; et al. Medically attended outpatient coronavirus infections in Ecuadorean children during the 20 months preceding countrywide lockdown related to SARS-CoV-2 pandemic of 2020. Pediatr. Infect. Dis. J. 2020, 39, e291–e296. [Google Scholar] [CrossRef] [PubMed]
- Suryadevara, M.; Wang, D.; Fajardo, F.P.; Carrillo Aponte, J.L.; Heras, F.; Aponte, C.C.; Torres, I.; Domachowske, J.B. Clinical, meteorological, and air quality factors associated with ambulatory pediatric respiratory syncytial virus infection in Machala, Ecuador, 2018–2023. Int. J. Environ. Res. Public Health 2025, 22, 272. [Google Scholar] [CrossRef] [PubMed]
- Azziz-Baumgartner, E.; Bruno, A.; Daughtery, M.; Chico, M.E.; Lopez, A.; Arriola, C.S.; de Mora, D.; Ropero, A.M.; Davis, W.W.; McMorrow, M.; et al. Incidence and seasonality of respiratory viruses among medically attended children with acute respiratory infections in an Ecuador birth cohort, 2011–2014. Influenza Other Respir. Viruses 2022, 16, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Caini, S.; de Mora, D.; Olmeda, M.; Portugal, D.; Becerra, M.A.; Mejia, M.; Pacurucu, M.C.; Ojeda, J.; Bonaccorsi, G.; Lorini, C.; et al. The epidemiology and severity of respiratory viral infections in a tropical country: Ecuador, 2009–2016. J. Infect. Public Health 2019, 12, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Jonnalagadda, S.; Rodriguez, O.; Estrella, B.; Sabin, L.L.; Sempertegui, F.; Hamer, D.H. Etiology of severe pneumonia in Ecuadorian children. PLoS ONE 2017, 12, e0171687. [Google Scholar] [CrossRef] [PubMed]
- Dalziel, S.R.; Haskell, L.; O’Brien, S.; Borland, M.L.; Plint, A.C.; Babl, F.E.; Oakley, E. Bronchiolitis. Lancet 2022, 400, 392–406. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Yu, L.J.; Zhang, H.Y.; Shan, C.X.; Lu, Q.B.; Zhang, X.A.; Ren, X.; Zhang, C.H.; Wang, Y.F.; Lin, S.H.; et al. Broad impacts of COVID-19 pandemic on acute respiratory infections in China: An observational study. Clin. Infect. Dis. 2021, 12, ciab942. [Google Scholar]
- Cho, H.J.; Rhee, J.E.; Kang, D.; Choi, E.H.; Lee, N.-J.; Woo, S.; Lee, J.; Lee, S.-W.; Kim, E.-J.; Yun, K.W. Epidemiology of respiratory viruses in Korean children before and after the COVID-19 pandemic: A prospective study from National Surveillance System. J. Korean Med. Sci. 2024, 39, e171. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Zhang, Y.; Wang, J.; Li, Y.; Wang, Y.; Gao, Y.; Zhao, M.; Zhao, M.; Tan, H.; Tie, Y.; et al. Epidemiology of respiratory pathogens in patients with acute respiratory infections during the COVID-19 pandemic and after easing of COVID-19 restrictions. Microbiol. Spectr. 2024, 12, e01161-24. [Google Scholar] [CrossRef] [PubMed]
- Oh, E.J.; Kim, J.M.; Joung, Y.H.; Kim, J.K. Effects of climatic factors on human parainfluenza 1, 2, and 3 infections in Cheonan, Republic of Korea. Environ. Sci. Pollut. Res. 2021, 28, 10018–10026. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Yue, W.; Song, X.; Zeng, L.; Liu, L.; Zheng, J.; Chen, X.; Lv, F.; Wen, S.; Zhang, H. Epidemiological characteristics of parainfluenza virus type 3 and the effects of meteorological factors in hospitalized children with lower respiratory tract infection. Front. Pediatr. 2022, 10, 872199. [Google Scholar] [CrossRef] [PubMed]
- Dong, W.; Chen, Q.; Hu, Y.; He, D.; Liu, J.; Yan, H.; Lan, K.; Zhang, C. Epidemiological and clinical characteristics of respiratory viral infections in children in Shanghai, China. Arch. Virol. 2016, 161, 1907–1913. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Wang, J.; Li, Z.; Xu, C.; Liao, Y.; Hu, M.; Yang, J.; Lai, S.; Wang, L.; Yang, W. Seasonal association between viral causes of hospitalized acute lower respiratory infections and meteorological factors in China: A retrospective study. Lancet Planet. Health 2021, 5, e154–e163. [Google Scholar] [CrossRef] [PubMed]
- Cui, B.; Zhang, D.; Pan, H.; Zhang, F.; Farrar, J.; Law, F.; van Doorn, H.R.; Wu, B.; Ba-Thein, W. Viral aetiology of acute respiratory infections among children and associated meteorological factors in southern China. BMC Infect. Dis. 2015, 15, 124. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Total | PIV * Detected | PIV Not Detected | p ** | |
|---|---|---|---|---|
| Study participants | 1251 | 117 | 1134 | |
| Mean age in months (range) | 19, 1–59 | 18, 1–59 | 19, 1–59 | 0.32 |
| Male gender, n (%) | 695 (56) | 66 (56) | 629 (55) | 0.85 |
| Symptoms | ||||
| Fever, n (%) | 1017 (81) | 95 (81) | 922 (81) | 0.98 |
| Nasal congestion, n (%) | 1186 (95) | 110 (94) | 1076 (95) | 0.69 |
| Cough, n (%) | 641 (51) | 70 (60) | 570 (50) | 0.05 |
| Wheeze, n (%) | 93 (7) | 20 (17) | 73 (6) | <0.0001 |
| Mean symptom duration in days (range) | 3.3, 1–10 | 3.3, 1–7 | 3.3, 1–10 | 0.8 |
| Upper respiratory tract infection, n (%) | 1081 (86) | 96 (82) | 956 (84) | 0.17 |
| Nasopharyngitis, n (%) | 1009 (81) | 92 (79) | 931 (82) | 0.36 |
| Laryngotracheitis, n (%) | 4 (<1) | 4 (3) | 25 (2) | 0.34 |
| Lower respiratory tract infection, n (%) | 124 (10) | 16 (14) | 107 (9) | 0.17 |
| Bronchiolitis, n (%) | 100 (8) | 13 (11) | 87 (8) | 0.19 |
| Bronchitis, n (%) | 8 (1) | 2 (2) | 6 (1) | 0.17 |
| Pneumonia, n (%) | 16 (1) | 1 (1) | 14 (1) | 1 |
| Received antibiotics, n (%) | 176 (14) | 10 (9) | 165 (15) | 0.75 |
| Influenza vaccination, n (%) | 646 (52) | 63 (54) | 583 (51) | 0.62 |
| Pertussis vaccination, n (%) | 1104 (88) | 106 (91) | 998 (88) | 0.41 |
| PIV 1 | PIV 2 | PIV 3 | PIV 4 | p * | |
|---|---|---|---|---|---|
| Study participants, n (%) | 14 (12) | 8 (7) | 71 (61) | 25 (21) | |
| Mean age in months (range) | 23, 1–59 | 20, 3–59 | 18, 1–59 | 13, 1–48 | 0.22 |
| Male gender, n (%) | 8 (57) | 6 (75) | 39 (55) | 14 (56) | 0.76 |
| Symptoms | |||||
| Fever, n (%) | 9 (64) | 8 (100) | 61 (86) | 18 (72) | |
| Nasal congestion, n (%) | 12 (86) | 8 (100) | 68 (96) | 23 (92) | |
| Cough, n (%) | 8 (57) | 5 (63) | 40 (56) | 18 (72) | 0.58 |
| Wheeze, n (%) | 6 (43) | 1 (13) | 6 (8) | 7 (28) | <0.01 |
| Mean symptom duration in days (range) | 3.5, 2–6 | 2.9, 2–7 | 3.1, 1–7 | 3.8, 1–7 | 0.19 |
| Upper respiratory tract infection, n (%) | 7 (50) | 7 (88) | 64 (90) | 18 (72) | 0.02 |
| Nasopharyngitis, n (%) | 7 (50) | 7 (88) | 63 (89) | 16 (60) | <0.001 |
| Laryngotracheitis, n (%) | 0 | 0 | 1 (1) | 3 (12) | |
| Lower respiratory tract infection, n (%) | 4 (29) | 1 (13) | 5 (7) | 7 (28) | 0.02 |
| Bronchiolitis, n (%) | 3 (21) | 0 | 4 (6) | 6 (24) | |
| Bronchitis, n (%) | 1 (7) | 1 (13) | 0 | 1 (4) | |
| Pneumonia, n (%) | 0 | 0 | 1 (1) | 0 | |
| Received antibiotics, n (%) | 1 (7) | 1 (13) | 8 (11) | 0 | |
| Influenza vaccination, n (%) | 10 (71) | 4 (50) | 40 (56) | 10 (40) | 0.27 |
| Pertussis vaccination, n (%) | 13(93) | 8 (100) | 66 (93) | 20 (80) |
| PIV Detected | ||||
|---|---|---|---|---|
| All Subjects Who Tested Positive for PIV Detection | Subjects Enrolled Prior to the Onset of the SARS-CoV-2 Pandemic | Subjects Enrolled After the Onset of the SARS-CoV-2 Pandemic | p * | |
| Number of enrolled subjects | 117 | 57 | 60 | |
| Mean age in months, (range) | 18, 1–60 | 16, 1–60 | 19, 1–60 | 0.22 |
| Male gender, n (%) | 66 (56) | 32 (56) | 34 (57) | 0.95 |
| Symptoms | ||||
| Fever, n (%) | 95 (81) | 37 (65) | 58 (97) | <0.00001 |
| Nasal congestion, n (%) | 110 (94) | 53 (93) | 57 (95) | 0.7 |
| Cough, n (%) | 70 (60) | 45 (79) | 25 (42) | <0.0001 |
| Wheeze, n (%) | 20 (17) | 18 (32) | 2 (3) | 0 |
| Mean symptom duration in days, range | 3.3, 1–7 | 3.6, 1–7 | 3, 1–7 | 0.02 |
| Upper respiratory infection | 96 (82) | 37 (65) | 59 (98) | <0.001 |
| Nasopharyngitis, n (%) | 92 (79) | 34 (60) | 58 (97) | <0.00001 |
| Laryngotracheitis, n (%) | 4 (3) | 3 (5) | 1 (2) | 0.4 |
| Lower respiratory infection | 16 (14) | 14 (25) | 2 (3) | <0.001 |
| Bronchiolitis, n (%) | 13 (11) | 11 (19) | 2 (3) | <0.01 |
| Bronchitis, n (%) | 2 (2) | 2 (4) | 0 | 0.24 |
| Pneumonia, n (%) | 1 (1) | 1 (2) | 0 | 0.5 |
| Received antibiotics, n (%) | 10 (9) | 4 (7) | 6 (10) | 0.7 |
| Influenza vaccination, n (%) | 63 (54) | 33 (58) | 30 (50) | 0.4 |
| Pertussis vaccination, n (%) | 106 (91) | 53 (93) | 53 (88) | 0.53 |
| Variable | PIV Detected | PIV Not Detected | AUC * | p ** |
|---|---|---|---|---|
| Mean temperature | ||||
| n | 72 | 137 | 0.642 | 0.001 |
| Mean (SD) | 25.1 (2.1) | 26.2 (2.1) | ||
| Median (IQR) | 24.6 (3.6) | 26.8 (3.5) | ||
| Min, Max | 22.2, 29.1 | 22, 29.8 | ||
| Q1, Q3 | 23.4, 27 | 24.5, 28 | ||
| Mean dew point | ||||
| n | 72 | 137 | 0.454 | 0.276 |
| Mean (SD) | 21.6 (1.5) | 21.9 (1.6) | ||
| Median (IQR) | 22 (2.3) | 21.9 (2.8) | ||
| Min, Max | 19, 24.7 | 18.8, 24.9 | ||
| Q1, Q3 | 20.2, 22.6 | 20.4, 23.2 | ||
| Mean relative humidity (%) | ||||
| n | 64 | 120 | 0.499 | 0.979 |
| Mean (SD) | 77 (7.5) | 77.1 (6.2) | ||
| Median (IQR) | 77.2 (12.7) | 77.4 (9.1) | ||
| Min, Max | 61.8, 92.2 | 63.3, 88.6 | ||
| Q1, Q3 | 70.2, 82.9 | 72.8, 81.8 | ||
| Humidity Range (%) | ||||
| n | 57 | 118 | 0.61 | 0.019 |
| Mean (SD) | 35.8 (30.4) | 24.5 (22.2) | ||
| Median (IQR) | 21.7 (48.6) | 13.1 (36.7) | ||
| Min, Max | 4.1, 91.7 | 3.6, 91.7 | ||
| Q1, Q3 | 7.9, 56.6 | 6.2, 42.8 | ||
| Mean barometric pressure | ||||
| n | 72 | 137 | 0.612 | 0.008 |
| Mean (SD) | 1011.4 (1.2) | 1010.8 (1.3) | ||
| Median (IQR) | 1011.5 (1.9) | 1010.9 (1.8) | ||
| Min, Max | 1008.7, 1013.5 | 1007.6, 1013.6 | ||
| Q1, Q3 | 1010.3, 1012.3 | 1009.9, 1011.7 | ||
| Min, Max | 0, 0.3 | 0, 0.2 | ||
| Q1, Q3 | 0, 0.07 | 0, 0.04 |
| Univariate Logistic Regression | Multivariate Logistic Regression | |||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p | Odds Ratio | 95% CI | p | |
| Mean temperature (C) | 7.82 × 10−1 | 0.678, 0.898 | 0.001 | 6.32 × 10−1 | 0.473, 0.826 | 0.001 |
| Humidity range (%) | 1.017 | 1.005, 10.3 | 0.007 | 1.051 | 1.025, 1.082 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suryadevara, M.; Wang, D.; Fajardo, F.P.; Carrillo Aponte, J.L.; Heras, F.; Cueva Aponte, C.; Torres, I.; Domachowske, J. Medically Attended Outpatient Parainfluenza Virus Infections in Young Children from a Single Site in Machala, Ecuador. Int. J. Environ. Res. Public Health 2025, 22, 821. https://doi.org/10.3390/ijerph22060821
Suryadevara M, Wang D, Fajardo FP, Carrillo Aponte JL, Heras F, Cueva Aponte C, Torres I, Domachowske J. Medically Attended Outpatient Parainfluenza Virus Infections in Young Children from a Single Site in Machala, Ecuador. International Journal of Environmental Research and Public Health. 2025; 22(6):821. https://doi.org/10.3390/ijerph22060821
Chicago/Turabian StyleSuryadevara, Manika, Dongliang Wang, Freddy Pizarro Fajardo, Jorge Luis Carrillo Aponte, Froilan Heras, Cinthya Cueva Aponte, Irene Torres, and Joseph Domachowske. 2025. "Medically Attended Outpatient Parainfluenza Virus Infections in Young Children from a Single Site in Machala, Ecuador" International Journal of Environmental Research and Public Health 22, no. 6: 821. https://doi.org/10.3390/ijerph22060821
APA StyleSuryadevara, M., Wang, D., Fajardo, F. P., Carrillo Aponte, J. L., Heras, F., Cueva Aponte, C., Torres, I., & Domachowske, J. (2025). Medically Attended Outpatient Parainfluenza Virus Infections in Young Children from a Single Site in Machala, Ecuador. International Journal of Environmental Research and Public Health, 22(6), 821. https://doi.org/10.3390/ijerph22060821