
Hospital-Related Determinants of Refusal of Organ Donation in France: A Multilevel Study

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Management of Organ Donation in France
2.2. Population
2.3. Data Sources
2.3.1. CRISTAL
2.3.2. ABM Databases Monitoring Hospitals and DCT Staff
2.3.3. External ABM Databases
- Annual Statistics of Health-Care Facilities [19]
- Quality indicators for hospitals
- a.
- Hospital certification
- b.
- An indicator of care quality and safety: e-Satis
2.4. Variable of Interest
2.5. Exposure Factors
2.6. Statistical Analysis
- Step 1: empty model (i.e., a model with no exposure factor) with a random intercept, enabling us to estimate the hospital-related effect without taking particular individual or contextual factors into account. A significant random effect found with this model points in the direction of a crude difference in refusal rates between hospitals. However, if the result is not significant, there is no point in using multilevel models thereafter because the assumption of a hierarchical structure of the data is not verified.
- Step 2: model with a random intercept and donor characteristics. Donor characteristics associated with refusal of organ donation at p < 20% on univariable analysis were included in a backward stepwise logistic regression. Variables associated with refusal at a threshold of 5% were kept in the final step 2 model. This model allows for taking into account clinical variables that may be indirectly linked to the hospital. A significant random effect found with the final step 2 model points in the direction of a structural difference in refusal rates between hospitals, in other words there is a hospital effect not explained by the individual characteristics of donors. However, if the result is not significant, there is no point in using multilevel models thereafter because the assumption of a hierarchical structure of the data is no longer verified once the variables relating to the donor have been taken into account. Hence, donor variables must be included in an intermediate analysis so as not to wrongly conclude that there is a structural effect of the hospital in the refusal to donation.
- Step 3: final model with a random intercept and characteristics of both donors and hospitals. Hospital characteristics associated with refusal of organ donation at p < 20% on univariable analysis were included in a backward stepwise logistic regression with donor characteristics selected in the final step 2 as fixed factors. Variables associated with refusal at a threshold of 5% were kept in the final model. Furthermore, if the p-value associated with the random effect disappeared, this means that the hospital effect is fully explained by the donor and hospital factors included in the final model.
2.7. Sensitivity Analysis
3. Results
3.1. Description of Refusal Rate
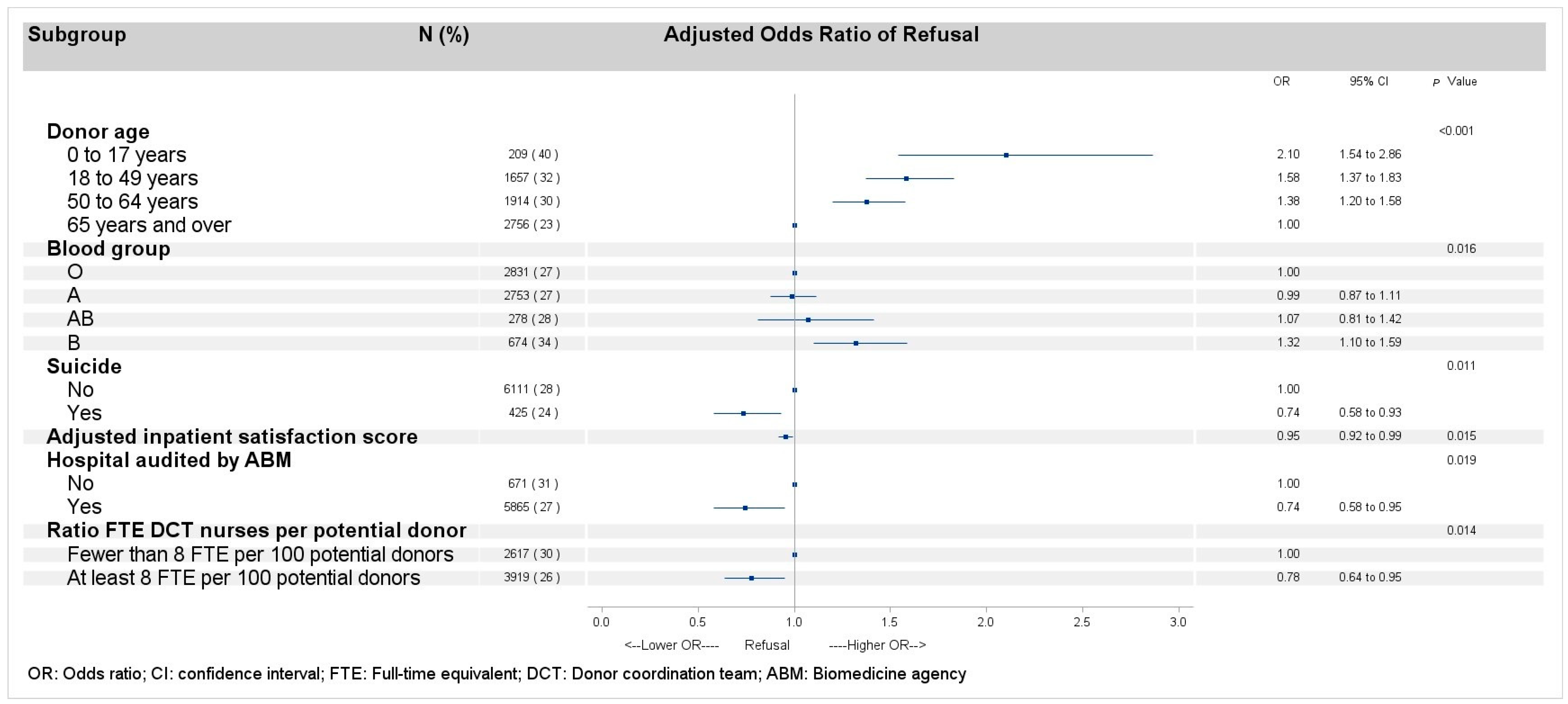
3.2. Refusal of Organ Donation After Adjustment for the Hospital-Related Random Effects
3.3. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ABM | Agence de la biomédecine |
| DCT | Donor coordination team |
| HAS | Haute autorité de santé (national authority for health) |
| FTE | Full-time equivalent |
| DBD | Donation after brain death |
| DCD | Donation after cardiac death |
| pmp | Per million population |
References
- Newsletter Transplant—European Directorate for the Quality of Medicines & HealthCare—EDQM. Available online: https://www.edqm.eu/en/newsletter-transplant (accessed on 23 December 2024).
- Agence de La Biomédecine. Available online: https://rams.agence-biomedecine.fr/organes (accessed on 24 December 2024).
- Greffes et Dons D’organes: Plans D’actions 2022–2026. Available online: https://sante.gouv.fr/soins-et-maladies/autres-produits-de-sante/article/greffes-et-dons-d-organes-plans-d-actions-2022-2026 (accessed on 19 July 2023).
- Becker, F.; Roberts, K.J.; de Nadal, M.; Zink, M.; Stiegler, P.; Pemberger, S.; Castellana, T.P.; Kellner, C.; Murphy, N.; Kaltenborn, A.; et al. Optimizing Organ Donation: Expert Opinion from Austria, Germany, Spain and the U.K. Ann. Transplant. 2020, 25, e921727. [Google Scholar] [CrossRef] [PubMed]
- Williment, C.; Beaulieu, L.; Clarkson, A.; Gunderson, S.; Hartell, D.; Escoto, M.; Ippersiel, R.; Powell, L.; Kirste, G.; Nathan, H.M.; et al. Organ Donation Organization Architecture: Recommendations From an International Consensus Forum. Transplant. Direct 2023, 9, e1440. [Google Scholar] [CrossRef] [PubMed]
- Guide to the Quality and Safety of Organs for Transplantation—European Directorate for the Quality of Medicines & HealthCare—EDQM. Available online: https://www.edqm.eu/en/guide-quality-and-safety-of-organs-for-transplantation (accessed on 3 July 2023).
- Chandler, J.A.; Connors, M.; Holland, G.; Shemie, S.D. “Effective” Requesting: A Scoping Review of the Literature on Asking Families to Consent to Organ and Tissue Donation. Transplantation 2017, 101, S1–S16. [Google Scholar] [CrossRef] [PubMed]
- de Groot, J.; Vernooij-Dassen, M.; Hoedemaekers, C.; Hoitsma, A.; Smeets, W.; van Leeuwen, E. Decision Making by Relatives about Brain Death Organ Donation: An Integrative Review. Transplantation 2012, 93, 1196–1211. [Google Scholar] [CrossRef]
- Le Nobin, J.; Pruvot, F.-R.; Villers, A.; Flamand, V.; Bouye, S. Family refusal of organ donation: A retrospective study in a French organ procurement center. Prog. Urol. 2014, 24, 282–287. [Google Scholar] [CrossRef]
- Rodrigue, J.R.; Cornell, D.L.; Howard, R.J. Organ Donation Decision: Comparison of Donor and Nondonor Families. Am. J. Transplant. 2006, 6, 190–198. [Google Scholar] [CrossRef]
- Siminoff, L.A.; Gordon, N.; Hewlett, J.; Arnold, R.M. Factors Influencing Families’ Consent for Donation of Solid Organs for Transplantation. JAMA 2001, 286, 71–77. [Google Scholar] [CrossRef]
- Simpkin, A.L.; Robertson, L.C.; Barber, V.S.; Young, J.D. Modifiable Factors Influencing Relatives’ Decision to Offer Organ Donation: Systematic Review. BMJ 2009, 338, b991. [Google Scholar] [CrossRef]
- Singh, J.M.; Ball, I.M.; Hartwick, M.; Malus, E.; Soliman, K.; Boyd, J.G.; Dhanani, S.; Healey, A. Facteurs qui influent sur le consentement au don d’organes: Étude rétrospective basée dans la population. Can. Med. Assoc. J. 2022, 194, E134–E142. [Google Scholar] [CrossRef]
- Domínguez-Gil, B.; Delmonico, F.L.; Shaheen, F.A.M.; Matesanz, R.; O’Connor, K.; Minina, M.; Muller, E.; Young, K.; Manyalich, M.; Chapman, J.; et al. The Critical Pathway for Deceased Donation: Reportable Uniformity in the Approach to Deceased Donation. Transpl. Int. 2011, 24, 373–378. [Google Scholar] [CrossRef]
- Arshad, A.; Anderson, B.; Sharif, A. Comparison of Organ Donation and Transplantation Rates between Opt-out and Opt-in Systems. Kidney Int. 2019, 95, 1453–1460. [Google Scholar] [CrossRef] [PubMed]
- Etheredge, H.R. Assessing Global Organ Donation Policies: Opt-In vs Opt-Out. Risk Manag. Healthc. Policy 2021, 14, 1985–1998. [Google Scholar] [CrossRef] [PubMed]
- Décret N° 2016-1118 Du 11 Août 2016 Relatif Aux Modalités D’expression Du Refus de Prélèvement d’organes Après Le Décès. Available online: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000033027728 (accessed on 18 July 2023).
- Arrêté du 16 Août 2016 Portant Homologation des Règles de Bonnes Pratiques Relatives à l’entretien Avec les Proches en Matière de Prélèvement D’organes et de Tissus. Available online: https://www.legifrance.gouv.fr/loda/id/JORFTEXT000033063529 (accessed on 14 November 2023).
- Bases Administratives SAE. Available online: https://drees2-sgsocialgouv.opendatasoft.com/explore/dataset/707_bases-administratives-sae/information/ (accessed on 22 August 2023).
- Certification des Etablissements de Santé pour la Qualité des Soins (Référentiel 2014-2020)—Data.gouv.fr. Available online: https://www.data.gouv.fr/fr/datasets/certification-des-etablissements-de-sante-pour-la-qualite-des-soins-referentiel-2014-2020/ (accessed on 22 August 2023).
- IQSS—E-Satis: Mesure de la Satisfaction et de L’expérience des Patients Hospitalisés. Available online: https://www.has-sante.fr/jcms/c_2030354/fr/iqss-e-satis-mesure-de-la-satisfaction-et-de-l-experience-des-patients-hospitalises (accessed on 18 July 2023).
- Austin, P.C.; Merlo, J. Intermediate and Advanced Topics in Multilevel Logistic Regression Analysis. Stat. Med. 2017, 36, 3257–3277. [Google Scholar] [CrossRef] [PubMed]
- Cowie, S.; Choy, S.-H.; Shah, D.M.; Gomez, M.P.; Yoong, B.-K.; Koong, J.-K. Healthcare System Impact on Deceased Organ Donation and Transplantation: A Comparison Between the Top 10 Organ Donor Countries With 4 Countries in Southeast Asia. Transpl. Int. 2023, 36, 11233. [Google Scholar] [CrossRef]
- Tackmann, E.; Dettmer, S. Measures Influencing Post-Mortem Organ Donation Rates in Germany, the Netherlands, Spain and the UK: A Systematic Review. Anaesthesist 2019, 68, 377–383. [Google Scholar] [CrossRef]
- Streit, S.; Johnston-Webber, C.; Mah, J.; Prionas, A.; Wharton, G.; Casanova, D.; Mossialos, E.; Papalois, V. Ten Lessons From the Spanish Model of Organ Donation and Transplantation. Transpl. Int. 2023, 36, 11009. [Google Scholar] [CrossRef]
- Fernández-Alonso, V.; Palacios-Ceña, D.; Silva-Martín, C.; García-Pozo, A. Facilitators and Barriers in the Organ Donation Process: A Qualitative Study among Nurse Transplant Coordinators. Int. J. Environ. Res. Public Health 2020, 17, 7996. [Google Scholar] [CrossRef]
- Rodrigue, J.R.; Cornell, D.L.; Howard, R.J. The Instability of Organ Donation Decisions by Next-of-Kin and Factors That Predict It. Am. J. Transplant. 2008, 8, 2661–2667. [Google Scholar] [CrossRef]
- Dicks, S.G.; Burkolter, N.; Jackson, L.C.; Northam, H.L.; Boer, D.P.; van Haren, F.M.P. Grief, Stress, Trauma, and Support During the Organ Donation Process. Transplant. Direct 2020, 6, e512. [Google Scholar] [CrossRef]
- Jawoniyi, O.; Gormley, K.; McGleenan, E.; Noble, H.R. Organ Donation and Transplantation: Awareness and Roles of Healthcare Professionals-A Systematic Literature Review. J. Clin. Nurs. 2018, 27, e726–e738. [Google Scholar] [CrossRef]
- Witjes, M.; Jansen, N.E.; van der Hoeven, J.G.; Abdo, W.F. Interventions Aimed at Healthcare Professionals to Increase the Number of Organ Donors: A Systematic Review. Crit. Care 2019, 23, 227. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.; Arora, S.; Dhanani, S.; Rochon, A.; Giorno, L.P.; Jackson, E.; Hornby, L.; Latifi, M.; Lotherington, K.; Luctkar-Flude, M.; et al. Quality Improvement Tools to Manage Deceased Organ Donation Processes: A Scoping Review. BMJ Open 2023, 13, e070333. [Google Scholar] [CrossRef] [PubMed]
- Godino, M.M.; Mizraji, R. Self-Assessment Tool and Clinical Audits: A Way to Manage Organ Donation and Transplantation in Hospital Settings. Transplant. Proc. 2023, 55, 1458–1462. [Google Scholar] [CrossRef] [PubMed]
- Zavalkoff, S.; O’Donnell, S.; Lalani, J.; Karam, I.F.; James, L.; Shemie, S.D. Preventable Harm in the Canadian Organ Donation and Transplantation System: A Descriptive Study of Missed Organ Donor Identification and Referral. Can. J. Anaesth. 2023, 70, 886–892. [Google Scholar] [CrossRef]
- Demiguel, V.; Boileau, C.; Cohen, S.; Noury, D.; Bonnet, F.; Tuppin, P. Factors associated with refusal of organ donation in France from 1996 to 1999. Ann. Fr. Anesth. Reanim. 2001, 20, 826–832. [Google Scholar] [CrossRef]
- Febrero, B.; Almela-Baeza, J.; Ros-Madrid, I.; Arias, J.A.; Ruiz-Manzanera, J.J.; Jiménez-Mascuñán, M.I.; Ramírez, P. The New Age of Organ Donation-What Factors Have an Influence on the Attitude of Older People? An Attitudinal Survey in Southeastern Spain. Int. J. Environ. Res. Public Health 2022, 19, 8524. [Google Scholar] [CrossRef]
- Martínez-Soba, F.; Pérez-Villares, J.M.; Martínez-Camarero, L.; Lara, R.; Monzón, J.L.; Fernández-Carmona, A.; Marco, P.; Coll, E.; Domínguez-Gil, B. Intensive Care to Facilitate Organ Donation: A Report on the Experience of 2 Spanish Centers With a Common Protocol. Transplantation 2019, 103, 558–564. [Google Scholar] [CrossRef]
- Martín-Delgado, M.C.; Martínez-Soba, F.; Masnou, N.; Pérez-Villares, J.M.; Pont, T.; Sánchez Carretero, M.J.; Velasco, J.; De la Calle, B.; Escudero, D.; Estébanez, B.; et al. Summary of Spanish Recommendations on Intensive Care to Facilitate Organ Donation. Am. J. Transplant. 2019, 19, 1782–1791. [Google Scholar] [CrossRef]
- Matesanz, R.; Domínguez-Gil, B.; Coll, E.; Mahíllo, B.; Marazuela, R. How Spain Reached 40 Deceased Organ Donors per Million Population. Am. J. Transplant. 2017, 17, 1447–1454. [Google Scholar] [CrossRef]
- Dean, L. Blood Group Antigens Are Surface Markers on the Red Blood Cell Membrane. In Blood Groups and Red Cell Antigens [Internet]; National Center for Biotechnology Information (US): Bethesda, MS, USA, 2005. [Google Scholar]
- Mourant, A.E.; Kopeć, A.C.; Domaniewska-Sobczak, K. The Distribution of the Human Blood Groups and Other Polymorphisms; Oxford University Press: Oxford, UK, 1976; ISBN 978-0-19-264167-0. [Google Scholar]
- Blood Type by Country 2025. Available online: https://worldpopulationreview.com/country-rankings/blood-type-by-country (accessed on 7 April 2025).
- Qu, Z.; Oedingen, C.; Bartling, T.; Schrem, H.; Krauth, C. Factors Influencing Deceased Organ Donation Rates in OECD Countries: A Panel Data Analysis. BMJ Open 2024, 14, e077765. [Google Scholar] [CrossRef]
- Beauchemin, C.; Hamel, C.; Simon, P. Diversité des origines et émergence des minorités. In Trajectoires et Origines: Enquête sur la Diversité des Populations en France; Ined Éditions: Paris, France, 2016; pp. 607–616. ISBN 978-2-7332-9015-6. [Google Scholar]
- Silva e Silva, V.; Schirmer, J.; Roza, B.D.; de Oliveira, P.C.; Dhanani, S.; Almost, J.; Schafer, M.; Tranmer, J. Defining Quality Criteria for Success in Organ Donation Programs: A Scoping Review. Can. J. Kidney Health Dis. 2021, 8, 205435812199292. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| N | % | |
|---|---|---|
| Context that finally did not result in organ procurement | 876 | 44.8 |
| Refusal by deceased while alive (refusal register or written refusal) | 22 | 1.1 |
| Refusal by legal guardian or representative | 104 | 5.3 |
| Refusal expressed while alive, reported in writing by a family member * after interview with DCT | 954 | 48.8 |
| Empty Model | Model 2 | Model 3 | |
|---|---|---|---|
| Variance random effects | 0.2078 * | 0.1824 * | 0.1554 * |
| PCV | reference | 12.2% | 25.2% |
| VPC (ICC) | 5.9% | 5.3% | 4.6% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bronchard, R.; Santin, G.; Legeai, C.; Bianchi, A.; Grelier, S.; Bogue, C.; Bastien, O.; Kerbaul, F. Hospital-Related Determinants of Refusal of Organ Donation in France: A Multilevel Study. Int. J. Environ. Res. Public Health 2025, 22, 618. https://doi.org/10.3390/ijerph22040618
Bronchard R, Santin G, Legeai C, Bianchi A, Grelier S, Bogue C, Bastien O, Kerbaul F. Hospital-Related Determinants of Refusal of Organ Donation in France: A Multilevel Study. International Journal of Environmental Research and Public Health. 2025; 22(4):618. https://doi.org/10.3390/ijerph22040618
Chicago/Turabian StyleBronchard, Régis, Gaëlle Santin, Camille Legeai, Anne Bianchi, Séverine Grelier, Caroline Bogue, Olivier Bastien, and François Kerbaul. 2025. "Hospital-Related Determinants of Refusal of Organ Donation in France: A Multilevel Study" International Journal of Environmental Research and Public Health 22, no. 4: 618. https://doi.org/10.3390/ijerph22040618
APA StyleBronchard, R., Santin, G., Legeai, C., Bianchi, A., Grelier, S., Bogue, C., Bastien, O., & Kerbaul, F. (2025). Hospital-Related Determinants of Refusal of Organ Donation in France: A Multilevel Study. International Journal of Environmental Research and Public Health, 22(4), 618. https://doi.org/10.3390/ijerph22040618