

Rehabilitation Needs Across Heterogenous Brazilian Regions: Secondary Analysis of the Global Burden of Disease Study



Abstract
:1. Introduction
- Determine Brazil’s global burden of disability amenable to rehabilitation, per capita and adjusted for population ageing, their evolution since 1990, and the distribution by the five pre-established impairment categories.
- Identify how these values vary by (a) key age groups and (b) the five major Brazilian regions.
2. Materials and Methods
Data Computation and Synthesis
3. Results
- Brazil-wide rehabilitation needs, including those stratified per main condition groups
- (a)
- Distribution by age groups
- (b)
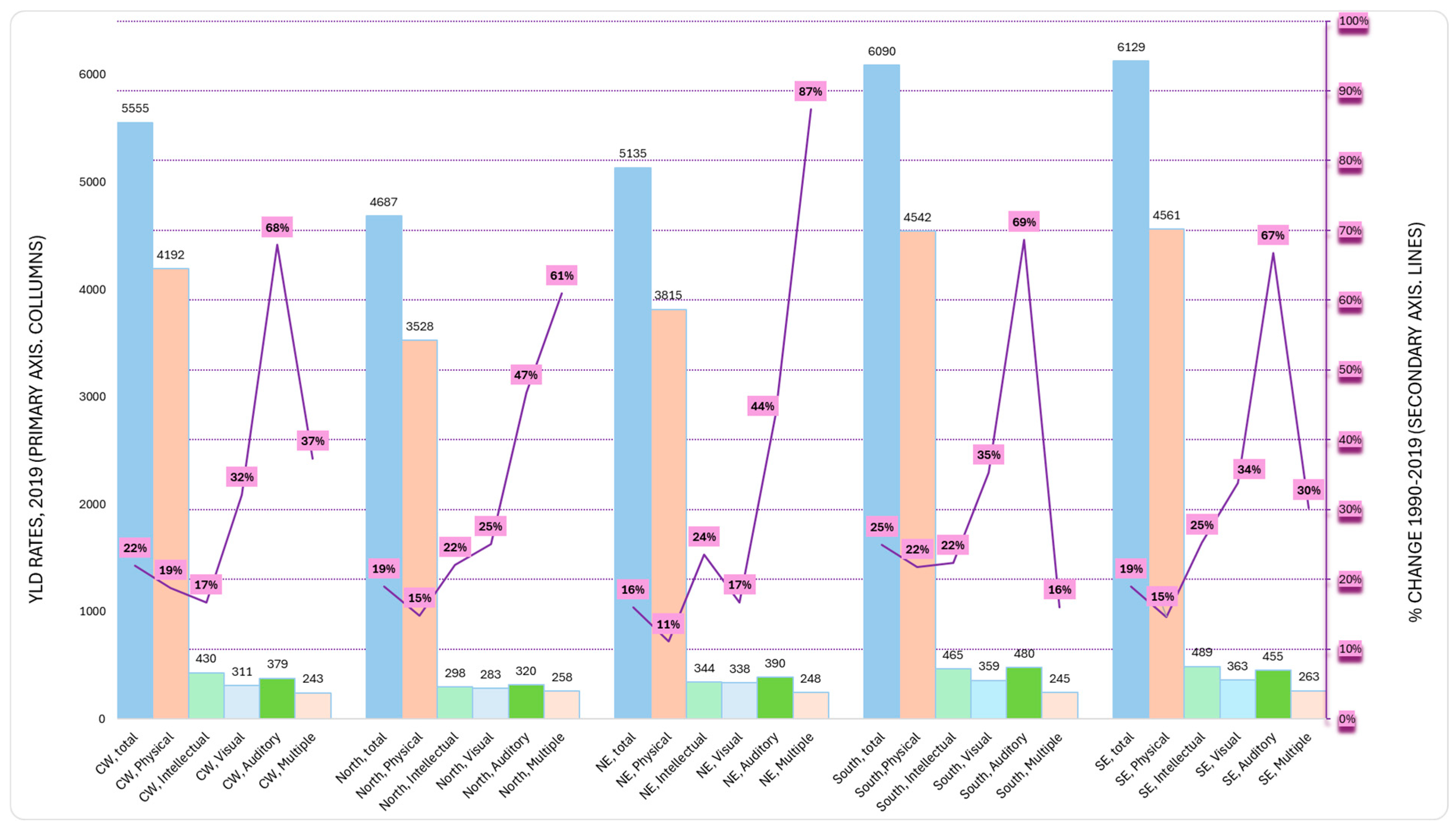
- Distribution by regions
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 2006–2017. [Google Scholar] [CrossRef] [PubMed]
- Jesus, T.S.; Landry, M.D.; Hoenig, H. Global need for physical rehabilitation: Systematic analysis from the global burden of disease study 2017. Int. J. Environ. Res. Public Health 2019, 16, 980. [Google Scholar] [CrossRef]
- Jesus, T.S.; Landry, M.D. Global need: Including rehabilitation in health system strengthening. Lancet 2021, 397, 665–666. [Google Scholar] [CrossRef] [PubMed]
- Kamenov, K.; Mills, J.-A.; Chatterji, S.; Cieza, A. Needs and unmet needs for rehabilitation services: A scoping review. Disabil. Rehabil. 2019, 41, 1227–1237. [Google Scholar] [CrossRef]
- Jesus, T.S.; Landry, M.D.; Brooks, D.; Hoenig, H. Physical Rehabilitation Needs Per Condition Type: Results from the Global Burden of Disease Study 2017. Arch. Phys. Med. Rehabil. 2020, 101, 960–968. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Louw, Q.; Grimmer, K.; Berner, K.; Conradie, T.; Bedada, D.T.; Jesus, T.S. Towards a needs-based design of the physical rehabilitation workforce in South Africa: Trend analysis [1990–2017] and a 5-year forecasting for the most impactful health conditions based on global burden of disease estimates. BMC Public Health 2021, 21, 913. [Google Scholar] [CrossRef]
- Bouziri, H.; Roquelaure, Y.; Descatha, A.; Dab, W.; Jean, K. Temporal and spatial distribution of musculoskeletal disorders from 1990 to 2019: A systematic analysis of the global burden of disease. BMJ Public Health 2023, 1, e000353. [Google Scholar] [CrossRef]
- Al Imam, M.H.; Jahan, I.; Das, M.C.; Muhit, M.; Akbar, D.; Badawi, N.; Khandaker, G. Situation analysis of rehabilitation services for persons with disabilities in Bangladesh: Identifying service gaps and scopes for improvement. Disabil. Rehabil. 2021, 44, 5571–5584. [Google Scholar] [CrossRef]
- Jesus, T.S.; Hoenig, H.; Landry, M.D. Development of the Rehabilitation Health Policy, Systems, and Services Research Field: Quantitative Analyses of Publications over Time (1990–2017) and across Country Type. Int. J. Environ. Res. Public Health 2020, 17, 965. [Google Scholar] [CrossRef]
- Bickenbach, J.; Sabariego, C.; Stucki, G. Beneficiaries of Rehabilitation. Arch. Phys. Med. Rehabil. 2021, 102, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Cieza, A.; Mikkelsen, B.; Ghaffar, A. Advancing rehabilitation through health policy and systems research. Bull. World Health Organ. 2022, 100, 655–655A. [Google Scholar] [CrossRef] [PubMed]
- Brazil Overview: Development News, Research, Data. Available online: https://www.worldbank.org/en/country/brazil/overview (accessed on 21 November 2024).
- Marinho, F.; Passos, V.M.d.A.; Malta, D.C.; França, E.B.; Abreu, D.M.X.; Araújo, V.E.M.; Bustamante-Teixeira, M.T.; Camargos, P.A.M.; da Cunha, C.C.; Duncan, B.B.; et al. Burden of disease in Brazil, 1990–2016: A systematic subnational analysis for the Global Burden of Disease Study 2016. Lancet 2018, 392, 760–775. [Google Scholar] [CrossRef]
- Sixel, T.R.d.S.; Bernardo, D.; Medeiros, A.d.A.; Bousquat, A.; Mota, P.H.d.S.; Schmitt, A.C.B. The rehabilitation workforce in Brazil. Arch. Public Health 2024, 82, 25. [Google Scholar] [CrossRef]
- Falvey, J.R.; Murphy, T.E.; Gill, T.M.; Stevens-Lapsley, J.E.; Ferrante, L.E. Home Health Rehabilitation Utilization Among Medicare Beneficiaries Following Critical Illness. J. Am. Geriatr. Soc. 2020, 68, 1512–1519. [Google Scholar] [CrossRef]
- Kosar, C.M.; Loomer, L.; Ferdows, N.B.; Trivedi, A.N.; Panagiotou, O.A.; Rahman, M. Assessment of Rural-Urban Differences in Postacute Care Utilization and Outcomes Among Older US Adults. JAMA Netw. Open 2020, 3, e1918738. [Google Scholar] [CrossRef]
- Zhao, G.; Okoro, C.A.; Hsia, J.; Garvin, W.S.; Town, M. Prevalence of Disability and Disability Types by Urban–Rural County Classification—U.S., 2016. Am. J. Prev. Med. 2019, 57, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Mroz, T.M.; Meadow, A.; Colantuoni, E.; Leff, B.; Wolff, J.L. Home Health Agency Characteristics and Quality Outcomes for Medicare Beneficiaries with Rehabilitation-Sensitive Conditions. Arch. Phys. Med. Rehabil. 2018, 99, 1090–1098.e4. [Google Scholar] [CrossRef]
- Quigley, D.D.; Chastain, A.M.; Kang, J.A.; Bronstein, D.; Dick, A.W.; Stone, P.W.; Shang, J. Systematic Review of Rural and Urban Differences in Care Provided by Home Health Agencies in the United States. J. Am. Med. Dir. Assoc. 2022, 23, 1653.e1–1653.e13. [Google Scholar] [CrossRef]
- Hong, I.; Goodwin, J.S.; Reistetter, T.A.; Kuo, Y.-F.; Mallinson, T.; Karmarkar, A.; Lin, Y.-L.; Ottenbacher, K.J. Comparison of Functional Status Improvements Among Patients with Stroke Receiving Postacute Care in Inpatient Rehabilitation vs Skilled Nursing Facilities. JAMA Netw. Open 2019, 2, e1916646. [Google Scholar] [CrossRef]
- Coube, M.; Nikoloski, Z.; Mrejen, M.; Mossialos, E. Persistent inequalities in health care services utilisation in Brazil (1998–2019). Int. J. Equity Health 2023, 22, 25. [Google Scholar] [CrossRef] [PubMed]
- Miranda, V.I.A.; Schäfer, A.A.; Tomasi, C.D.; Soratto, J.; Meller, F.d.O.; Silveira, M.P.T. Inequalities in access to medicines for diabetes and hypertension across the capitals in different regions of Brazil: A population-based study. BMC Public Health 2021, 21, 1242. [Google Scholar] [CrossRef]
- Garnelo, L.; Parente, R.C.P.; Puchiarelli, M.L.R.; Correia, P.C.; Torres, M.V.; Herkrath, F.J. Barriers to access and organization of primary health care services for rural riverside populations in the Amazon. Int. J. Equity Health 2020, 19, 54. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.M.A.D.; Triaca, L.M.; Tejaba, C.A.O. Evolution of inequalities in health care use among older people in Brazil: Evidence for the period 1998–2019. J. Econ. Ageing 2021, 20, 100347. [Google Scholar]
- Neill, R.; Shawar, Y.R.; Ashraf, L.; Das, P.; Champagne, S.N.; Kautsar, H.; Zia, N.; Michlig, G.J.; Bachani, A.M. Prioritizing rehabilitation in low- and middle-income country national health systems: A qualitative thematic synthesis and development of a policy framework. Int. J. Equity Health 2023, 22, 91. [Google Scholar] [CrossRef]
- Neill, R.; Rutebemberwa, E.; Tweheyo, R.; Ojulo, S.T.; Okello, G.; Bachani, A.M.; Shawar, Y.R. Generating Political Priority for the Health Needs of the 21st Century: A Qualitative Policy Analysis on the Prioritization of Rehabilitation Services in Uganda. Int. J. Health Policy Manag. 2024, 13, 8347. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, K.S.Q.S.; Medeiros, A.d.A.; da Silva, S.L.A. Redecin Brasil: O Cuidado na Rede de Atenção à Pessoa com Deficiência nos Diferentes Brasis, 1st ed.; Rede Unida: Porto Alegre, Brazil, 2022. [Google Scholar]
- Instituto Brasileiro de Geografia e Estatística—IBGE—Projeções da População. Available online: https://www.ibge.gov.br/estatisticas/sociais/populacao/9109-projecao-da-populacao.html?edicao=41053 (accessed on 25 November 2024).
- Salomon, A.; Haagsma, A.J.; Davis, A.; de Noordhout, C.M.; Polinder, S.; Havelaar, A.H.; Cassini, A.; Devleesschauwer, B.; Kretzschmar, M.; Speybroeck, N.; et al. Disability weights for the Global Burden of Disease 2013 study. Lancet Glob. Health 2015, 3, e712–e723. [Google Scholar] [CrossRef]
- Health Data Overview for the Federative Republic of Brazil. Available online: https://data.who.int/countries/076 (accessed on 26 November 2024).
- Chatterji, S.; Byles, J.; Cutler, D.; Seeman, T.; Verdes, E. Health, functioning, and disability in older adults—Present status and future implications. Lancet 2015, 385, 563–575. [Google Scholar] [CrossRef]
- Kiekens, C.; Peers, K.H. 5.1 Physical and Rehabilitation Medicine in Health-Care Systems: Basic Concepts, Definitions, and Models. J. Int. Soc. Phys. Rehabil. Med. 2019, 2 (Suppl. S1), S70–S75. [Google Scholar] [CrossRef]
- Jesus, T.S.; Landry, M.D.; Hoenig, H.; Dussault, G.; Koh, G.C.; Fronteira, I. Is Physical Rehabilitation Need Associated with the Rehabilitation Workforce Supply? An Ecological Study Across 35 High-Income Countries. Int. J. Health Policy Manag. 2022, 11, 434–442. [Google Scholar] [CrossRef]
- Jesus, T.S.; Landry, M.D.; Dussault, G.; Fronteira, I. Human resources for health (and rehabilitation): Six Rehab-Workforce Challenges for the century. Hum. Resour. Health 2017, 15, 8. [Google Scholar] [CrossRef]
- Hayes, K.; Dos Santos, V.; Costigan, M.; Morante, D. Profile of occupational therapy services in non-urban settings: A global scoping review. Aust. Occup. Ther. J. 2023, 70, 119–141. [Google Scholar] [CrossRef] [PubMed]
- Speyer, R.; Denman, D.; Wilkes-Gillan, S.; Chen, Y.; Bogaardt, H.; Kim, J.; Heckathorn, D.; Cordier, R. Effects of telehealth by allied health professionals and nurses in rural and remote areas: A systematic review and meta-analysis. J. Rehabil. Med. 2018, 50, 225–235. [Google Scholar] [CrossRef] [PubMed]
- NICE. Stroke Rehabilitation in Adults; NICE: London, UK, 2023. [Google Scholar]
- Washington, S.E.; Bollinger, R.M.; Edwards, E.; McGowan, L.; Stephens, S. Telehealth Delivery of Evidence-Based Intervention Within Older Adult Populations: A Scoping Review. OTJR Occup. Ther. J. Res. 2023, 43, 467–477. [Google Scholar] [CrossRef]
- Ho, C.; Atchison, K.; Noonan, V.K.; McKenzie, N.; Cadel, L.; Ganshorn, H.; Rivera, J.M.B.; Yousefi, C.; Guilcher, S.J. Models of Care Delivery from Rehabilitation to Community for Spinal Cord Injury: A Scoping Review. J. Neurotrauma 2021, 38, 677–697. [Google Scholar] [CrossRef] [PubMed]
- Ghaffar, A.; Bachani, A.M.; Hyder, A.A.; Cieza, A.; Bhangu, A.; Bussières, A.; Sanchez-Ramirez, D.C.; Gandhi, D.B.C.; Verbunt, J.; Rasanathan, K.; et al. Role and promise of health policy and systems research in integrating rehabilitation into the health systems. Health Res. Policy Syst. 2024, 22, 143. [Google Scholar] [CrossRef]
- Banks, L.M.; Kuper, H.; Polack, S. Poverty and disability in low- and middle-income countries: A systematic review. PLoS ONE 2017, 12, e0189996. [Google Scholar] [CrossRef]
- Jesus, T.S.; Hoenig, H. Crossing the Global Quality Chasm in Health Care: Where Does Rehabilitation Stand? Arch. Phys. Med. Rehabil. 2019, 100, 2215–2217. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Physical | Musculoskeletal | General musculoskeletal | Osteoarthritis |
| Rheumatoid arthritis | |||
| Gout | |||
| Other musculoskeletal disorders | |||
| Traumatic musculoskeletal | Nature-based injuries—all listed except * and except ** | ||
| Musculoskeletal pain | Lower back pain | ||
| Neck pain | |||
| Neurological | Non-communicable neurological | Tension-type headache | |
| Stroke (cerebrovascular accident—CVA) | |||
| Multiple sclerosis | |||
| Parkinson’s disease | |||
| Motor neuron disease | |||
| Idiopathic epilepsy | |||
| Other neurological disorders | |||
| Epilepsy—except treated (impairment) | |||
| Infectious neurological (communicable) | Meningitis | ||
| Encephalitis | |||
| Tetanus | |||
| Zika | |||
| Leprosy | |||
| Guillain-Barré syndrome (impairment) | |||
| Traumatic neurological | Spinal cord injury (nature-based injury) | ||
| Traumatic brain injury (nature-based injury) | |||
| Drowning (nature-based injury) | |||
| Asphyxiation (nature-based injury) | |||
| Cardiothoracic | Cardiac | Cardiovascular disease—all listed except CVA | |
| Heart failure—except treated, for all health conditions not selected otherwise | |||
| Chagas disease | |||
| Pulmonary | Chronic respiratory disease | ||
| Severe chest injury (nature-based injury) | |||
| Tuberculosis | |||
| Lower respiratory disease | |||
| Other physical | Cancer | Cancer | |
| HIV/AIDS | HIV/AIDS | ||
| Burns | Burns | ||
| Intellectual | Intellectual and dementias | Intellectual and dementias | Intellectual disability (mild, moderate, severe, profound) |
| Alzheimer’s and other dementias | |||
| Autism | |||
| Visual (Only) | Visual | Visual | Blindness and vision loss—except presbyopia (impairment) |
| Auditory (Only) | Auditory | Auditory | Hearing loss—all except mild (impairment) |
| Multiple Impairments | Congenital | Congenital | Other congenital defects |
| Neural tube defects | |||
| Cleft lip and palate | |||
| Down syndrome | |||
| Turner syndrome | |||
| Klinefelter syndrome | |||
| Other chromosomal abnormalities | |||
| Neonatal | Neonatal disorders | Neonatal disorders |
| YLD Rates, All Ages | YLD Rates, Age-Standardized | |||
|---|---|---|---|---|
| Rehabilitation Need Type | 2019 | Percentage Change | 2019 | Percentage Change |
| Overall Rehabilitation Needs | 4986 | 24% | 4667 | −6% |
| Physical—total | 3847 | 20% | 3545 | −9% |
| MSK total | 2657 | 31% | 2401 | −4% |
| MSK general, total | 973 | 43% | 863 | −3% |
| MSK trauma total | 430 | 8% | 398 | −19% |
| MSK pain total | 1255 | 33% | 1140 | 1% |
| Neurological total | 513 | −2% | 484 | −24% |
| Neurological disorders NC—total | 343 | −6% | 330 | −27% |
| Neurological infectious/ communicable—total | 9 | −48% | 9 | −51% |
| Neurological trauma—total | 160 | 16% | 145 | −11% |
| Cardiothoracic—total | 488 | -3% | 488 | −14% |
| Cardiac—total | 151 | 39% | 143 | −5% |
| Pulmonary—total | 336 | −15% | 346 | −18% |
| Other physical—total | 189 | 27% | 171 | −7% |
| Intellectual: developmental and dementias—total | 253 | 28% | 253 | 2% |
| Visual (only)—total | 330 | 29% | 313 | −18% |
| Auditory (only)—total | 259 | 24% | 245 | −22% |
| Congenital and neonatal total | 298 | 78% | 312 | 102% |
| Congenital—physical—total | 23 | −25% | 25 | −12% |
| Neonatal total | 275 | 102% | 287 | 128% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Araújo, R.O.; Fernandes, T.G.; Jesus, T.S. Rehabilitation Needs Across Heterogenous Brazilian Regions: Secondary Analysis of the Global Burden of Disease Study. Int. J. Environ. Res. Public Health 2025, 22, 486. https://doi.org/10.3390/ijerph22040486
de Araújo RO, Fernandes TG, Jesus TS. Rehabilitation Needs Across Heterogenous Brazilian Regions: Secondary Analysis of the Global Burden of Disease Study. International Journal of Environmental Research and Public Health. 2025; 22(4):486. https://doi.org/10.3390/ijerph22040486
Chicago/Turabian Stylede Araújo, Rogério Olmedija, Tiótrefis Gomes Fernandes, and Tiago Silva Jesus. 2025. "Rehabilitation Needs Across Heterogenous Brazilian Regions: Secondary Analysis of the Global Burden of Disease Study" International Journal of Environmental Research and Public Health 22, no. 4: 486. https://doi.org/10.3390/ijerph22040486
APA Stylede Araújo, R. O., Fernandes, T. G., & Jesus, T. S. (2025). Rehabilitation Needs Across Heterogenous Brazilian Regions: Secondary Analysis of the Global Burden of Disease Study. International Journal of Environmental Research and Public Health, 22(4), 486. https://doi.org/10.3390/ijerph22040486