
Associations Between Traumatic Brain Injury Characteristics and Memory Outcomes: Insights from the Health and Retirement Study

 ,
,
Abstract
1. Introduction
1.1. Background of Traumatic Brain Injuries and Dementia
1.2. Present Study
2. Materials and Methods
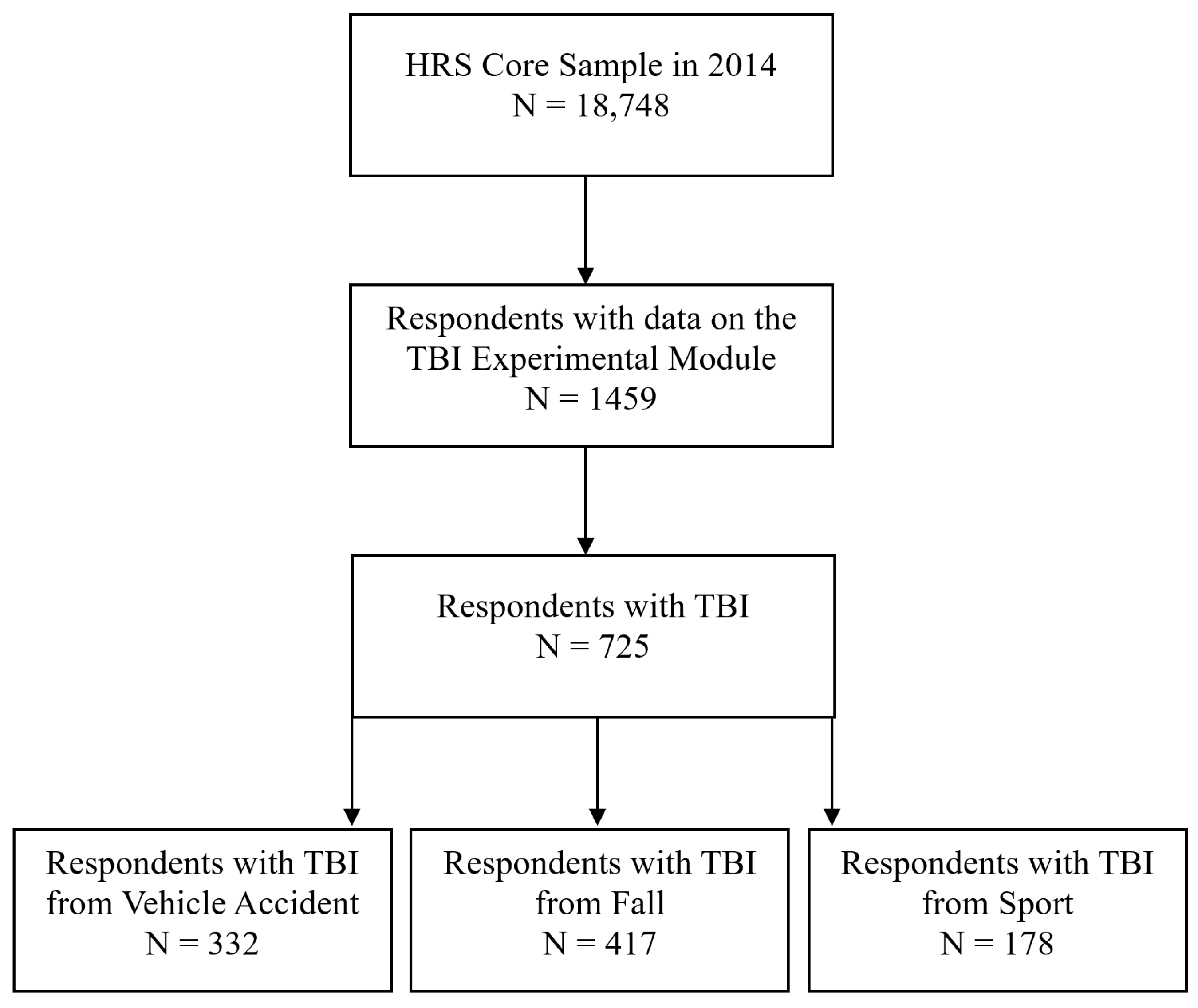
2.1. Participants and Procedure
2.2. Measures
2.3. Analytic Strategy
3. Results
3.1. Associations Between TBI Age of Onset and Memory Outcomes
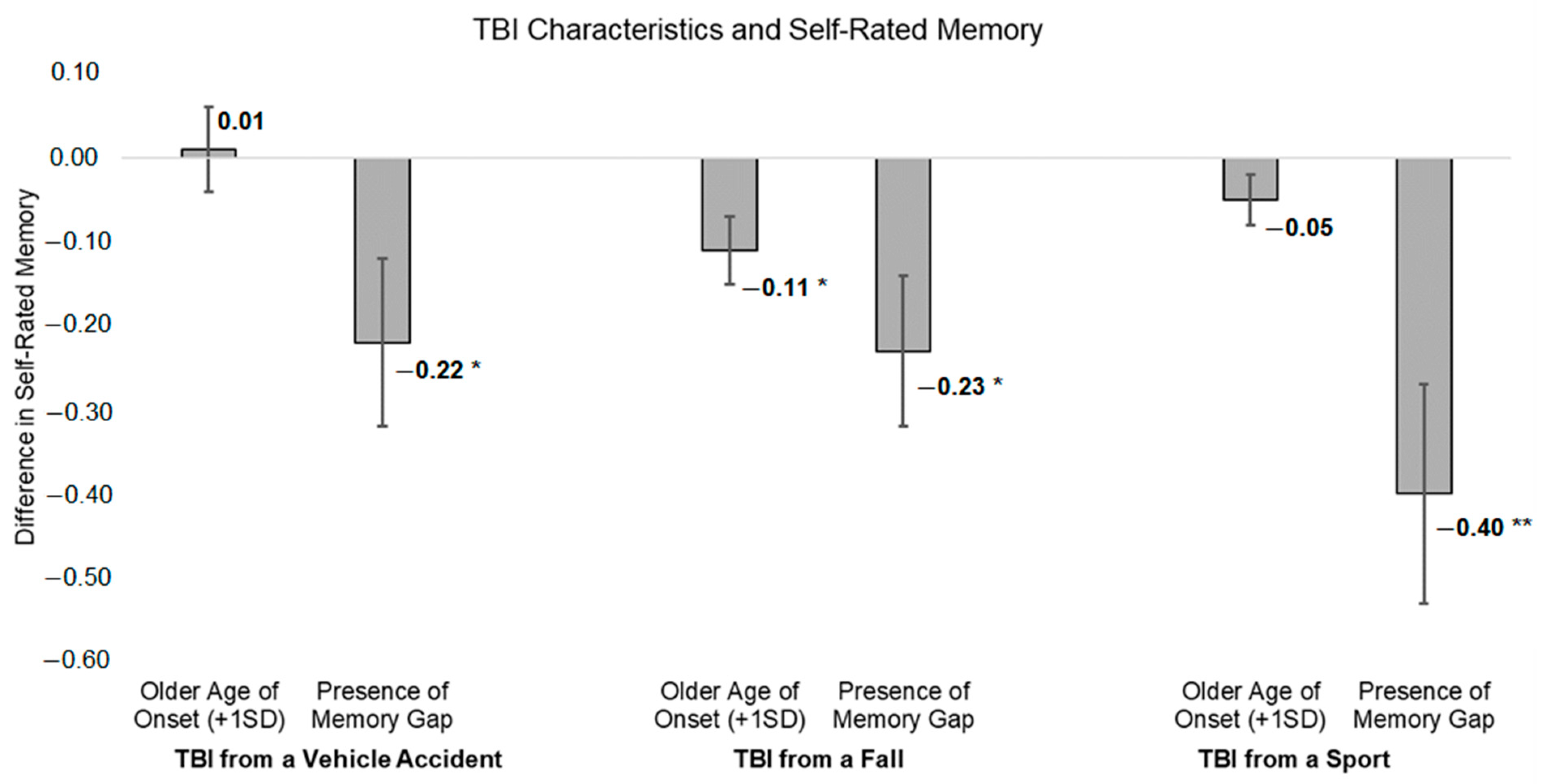
3.1.1. TBI Age of Onset and Self-Rated Memory
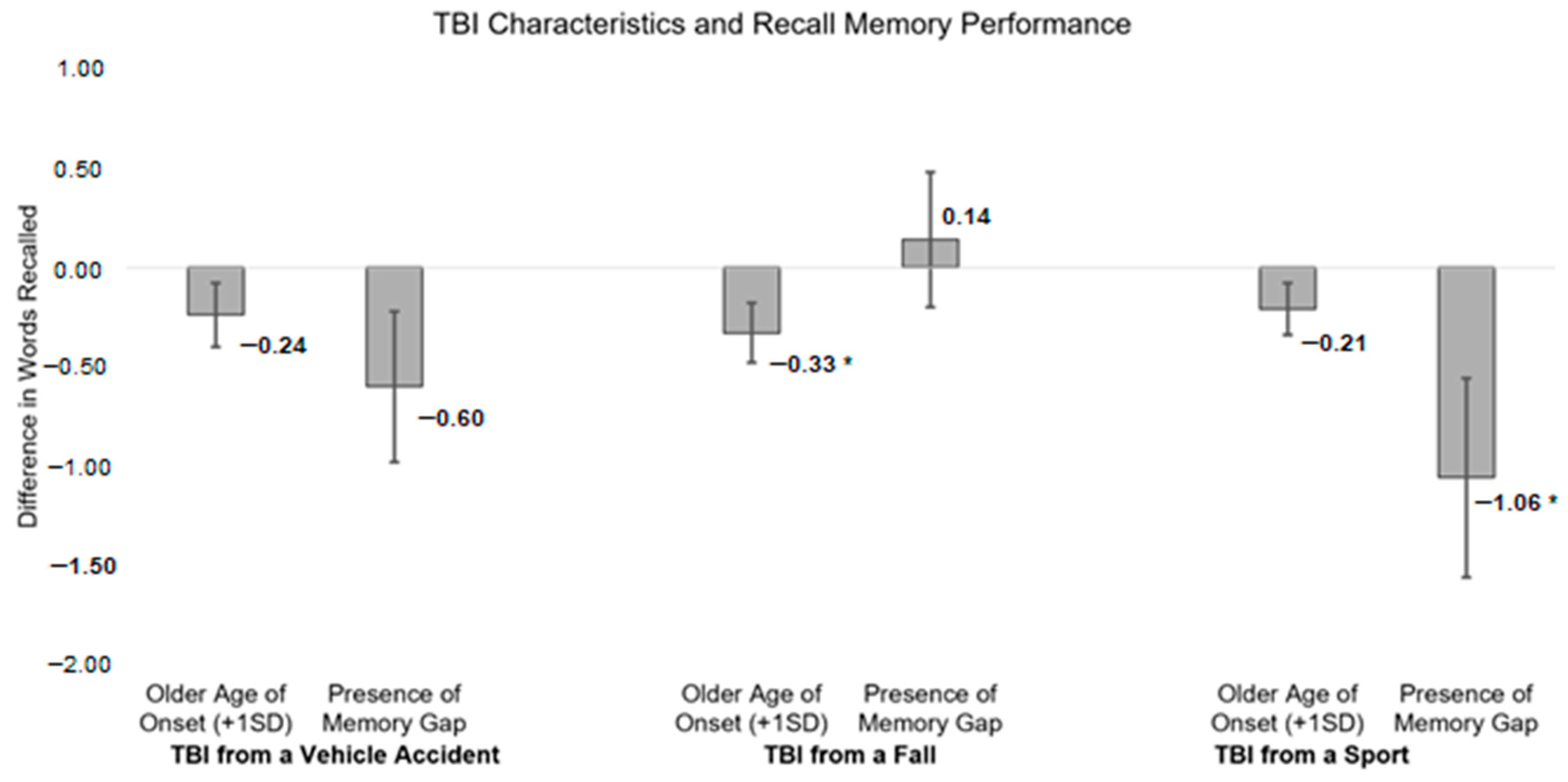
3.1.2. TBI Age of Onset and Recall Memory Performance
3.2. Associations Between Presence of Memory Gap from TBI and Memory Outcomes
3.2.1. Presence of Memory Gap and Self-Rated Memory
3.2.2. Presence of Memory Gap and Recall Memory Performance
3.3. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coburn, K. Traumatic Brain Injury: The Silent Epidemic. AACN Clin. Issues Crit. Care Nurs. 1992, 3, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Conway, F.N.; Domingues, M.; Monaco, R.; Lesnewich, L.M.; Ray, A.E.; Alderman, B.L.; Todaro, S.M.; Buckman, J.F. Concussion Symptom Underreporting Among Incoming National Collegiate Athletic Association Division I College Athletes. Clin. J. Sport Med. 2020, 30, 203. [Google Scholar] [CrossRef] [PubMed]
- Ferdinand Pennock, K.; McKenzie, B.; McClemont Steacy, L.; Mainwaring, L. Under-Reporting of Sport-Related Concussions by Adolescent Athletes: A Systematic Review. Int. Rev. Sport Exerc. Psychol. 2023, 16, 66–92. [Google Scholar] [CrossRef]
- Veliz, P.; McCabe, S.E.; Eckner, J.T.; Schulenberg, J.E. Trends in the Prevalence of Concussion Reported by US Adolescents, 2016–2020. JAMA 2021, 325, 1789. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, J.; DePadilla, L.; Sarmiento, K.; Breiding, M.J. Self-Reported Lifetime Concussion Among Adults: Comparison of 3 Different Survey Questions. J. Head. Trauma. Rehabil. 2020, 35, E136–E143. [Google Scholar] [CrossRef]
- Peterson, A.B.; Hong, Z.; Thomas, K.E.; Daughterty, J. CDC Surveillance Report of Traumatic Brain Injury-Related Hospitalizations and Deaths by Age Group, Sex, and Mechanism of Injury—United States, 2016 and 2017; Department of Health and Human Services: Atlanta, GA, USA, 2021. [Google Scholar]
- Peterson, A.B.; Xu, L.; Daughterty, J.; Breiding, M.J. CDC Surveillance Report of Traumatic Brain Injury-Related Emergency Department Visits, Hospitalizations, and Deaths—United States, 2014; Department of Health and Human Services: Atlanta, GA, USA, 2019. [Google Scholar]
- Alzheimer’s Association. 2022 Alzheimer’s Disease Facts and Figures. Alzheimer’s Dement. 2022, 18, 700–789. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Liu, K.; Costafreda, S.; Selbaek, G.; Alladi, S. Dementia Prevention, Intervention, and Care: 2024 Report of the Lancet Standing Commission. Lancet 2024, 404, 572–627. [Google Scholar] [CrossRef]
- Gardner, R.C.; Burke, J.F.; Nettiksimmons, J.; Kaup, A.; Barnes, D.E.; Yaffe, K. Dementia Risk after Traumatic Brain Injury vs Nonbrain Trauma: The Role of Age and Severity. JAMA Neurol. 2014, 71, 1490–1497. [Google Scholar] [CrossRef]
- Mehta, K.M.; Ott, A.; Kalmijn, S.; Slooter, A.J.; van Duijn, C.M.; Hofman, A.; Breteler, M.M. Head Trauma and Risk of Dementia and Alzheimer’s Disease: The Rotterdam Study. Neurology 1999, 53, 1959–1962. [Google Scholar] [CrossRef]
- Dams-O’Connor, K.; Gibbons, L.E.; Bowen, J.D.; McCurry, S.M.; Larson, E.B.; Crane, P.K. Risk for Late-Life Re-Injury, Dementia and Death among Individuals with Traumatic Brain Injury: A Population-Based Study. J. Neurol. Neurosurg. Psychiatry 2013, 84, 177–182. [Google Scholar] [CrossRef]
- Gardner, R.C.; Bahorik, A.; Kornblith, E.S.; Allen, I.E.; Plassman, B.L.; Yaffe, K. Systematic Review, Meta-Analysis, and Population Attributable Risk of Dementia Associated with Traumatic Brain Injury in Civilians and Veterans. J. Neurotrauma 2023, 40, 620–634. [Google Scholar] [CrossRef] [PubMed]
- Raj, R.; Kaprio, J.; Korja, M.; Mikkonen, E.D.; Jousilahti, P.; Siironen, J. Risk of Hospitalization with Neurodegenerative Disease after Moderate-to-Severe Traumatic Brain Injury in the Working-Age Population: A Retrospective Cohort Study Using the Finnish National Health Registries. PLoS Med. 2017, 14, e1002316. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.-K.; Lin, S.-H.; Sung, P.-S.; Wu, M.-H.; Hung, K.-W.; Wang, L.-C.; Huang, C.-Y.; Lu, K.; Chen, H.-J.; Tsai, K.-J. Population Based Study on Patients with Traumatic Brain Injury Suggests Increased Risk of Dementia. J. Neurol. Neurosurg. Psychiatry 2012, 83, 1080–1085. [Google Scholar] [CrossRef]
- Iacono, D.; Raiciulescu, S.; Olsen, C.; Perl, D.P. Traumatic Brain Injury Exposure Lowers Age of Cognitive Decline in AD and Non-AD Conditions. Front. Neurol. 2021, 12, 573401. [Google Scholar] [CrossRef] [PubMed]
- Sugarman, M.A.; McKee, A.C.; Stein, T.D.; Tripodis, Y.; Besser, L.M.; Martin, B.; Palmisano, J.N.; Steinberg, E.G.; O’Connor, M.K.; Au, R.; et al. Failure to Detect an Association Between Self-Reported Traumatic Brain Injury and Alzheimer’s Disease Neuropathology and Dementia. Alzheimers Dement. 2019, 15, 686–698. [Google Scholar] [CrossRef]
- Godbolt, A.K.; Cancelliere, C.; Hincapié, C.A.; Marras, C.; Boyle, E.; Kristman, V.L.; Coronado, V.G.; Cassidy, J.D. Systematic Review of the Risk of Dementia and Chronic Cognitive Impairment after Mild Traumatic Brain Injury: Results of the International Collaboration on Mild Traumatic Brain Injury Prognosis. Arch. Phys. Med. Rehabil. 2014, 95, S245–S256. [Google Scholar] [CrossRef]
- Hume, C.; Mitra, B.; Wright, B.; Kinsella, G.J. Cognitive Performance in Older People after Mild Traumatic Brain Injury: Trauma Effects and Other Risk Factors. J. Int. Neuropsychol. Soc. 2023, 29, 651–661. [Google Scholar] [CrossRef]
- Patricios, J.S.; Schneider, K.J.; Dvorak, J.; Ahmed, O.H.; Blauwet, C.; Cantu, R.C.; Davis, G.A.; Echemendia, R.J.; Makdissi, M.; McNamee, M.; et al. Consensus Statement on Concussion in Sport: The 6th International Conference on Concussion in Sport–Amsterdam, October 2022. Br. J. Sports Med. 2023, 57, 695–711. [Google Scholar] [CrossRef]
- Australian Institute of Sport. Concussion and Brain Health Position Statement 2024: An Initiative of the Australian Institute of Sport, Sports Medicine Australia, Australian Physiotherapy Association, and Australasian College of Sport and Exercise Physicians; AIS: Bruce, Australia, 2024. [Google Scholar]
- Gryffydd, L.; Mitra, B.; Wright, B.J.; Kinsella, G.J. Cognitive Performance in Older Adults at Three Months Following Mild Traumatic Brain Injury. J. Clin. Exp. Neuropsychol. 2021, 43, 481–496. [Google Scholar] [CrossRef]
- Lennon, M.J.; Brooker, H.; Creese, B.; Thayanandan, T.; Rigney, G.; Aarsland, D.; Hampshire, A.; Ballard, C.; Corbett, A.; Raymont, V. Lifetime Traumatic Brain Injury and Cognitive Domain Deficits in Late Life: The PROTECT-TBI Cohort Study. J. Neurotrauma 2023, 40, 1423–1435. [Google Scholar] [CrossRef]
- Grasset, L.; Glymour, M.M.; Yaffe, K.; Swift, S.L.; Gianattasio, K.Z.; Power, M.C.; Zeki Al Hazzouri, A. Association of Traumatic Brain Injury with Dementia and Memory Decline in Older Adults in the United States. Alzheimer’s Dement. 2020, 16, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.P.; Schaffert, J.; LoBue, C.; Womack, K.B.; Hart, J.; Cullum, C.M. Traumatic Brain Injury and Age of Onset of Dementia with Lewy Bodies. J. Alzheimers Dis. 2018, 66, 717–723. [Google Scholar] [CrossRef]
- Gu, D.; Ou, S.; Liu, G. Traumatic Brain Injury and Risk of Dementia and Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Neuroepidemiology 2022, 56, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Fann, J.R.; Ribe, A.R.; Pedersen, H.S.; Fenger-Grøn, M.; Christensen, J.; Benros, M.E.; Vestergaard, M. Long-Term Risk of Dementia among People with Traumatic Brain Injury in Denmark: A Population-Based Observational Cohort Study. Lancet Psychiatry 2018, 5, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Harmon, K.G.; Clugston, J.R.; Dec, K.; Hainline, B.; Herring, S.; Kane, S.F.; Kontos, A.P.; Leddy, J.J.; McCrea, M.; Poddar, S.K.; et al. American Medical Society for Sports Medicine Position Statement on Concussion in Sport. Br. J. Sports Med. 2019, 53, 213–225. [Google Scholar] [CrossRef]
- Silverberg, N.D.; Crane, P.K.; Dams-O’Connor, K.; Holdnack, J.; Ivins, B.J.; Lange, R.T.; Manley, G.T.; McCrea, M.; Iverson, G.L. Developing a Cognition Endpoint for Traumatic Brain Injury Clinical Trials. J. Neurotrauma 2017, 34, 363–371. [Google Scholar] [CrossRef]
- Permenter, C.M.; Fernández-de Thomas, R.J.; Sherman, A.L. Postconcussive Syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Whiteneck, G.G.; Cuthbert, J.P.; Corrigan, J.D.; Bogner, J.A. Risk of Negative Outcomes After Traumatic Brain Injury: A Statewide Population-Based Survey. J. Head Trauma Rehabil. 2016, 31, E43. [Google Scholar] [CrossRef]
- Gupte, R.; Brooks, W.; Vukas, R.; Pierce, J.; Harris, J. Sex Differences in Traumatic Brain Injury: What We Know and What We Should Know. J. Neurotrauma 2019, 36, 3063–3091. [Google Scholar] [CrossRef]
- Zhu, Y.; Williams, J.; Beyene, K.; Trani, J.-F.; Babulal, G.M. Traumatic Brain Injury, Seizures, and Cognitive Impairment Among Older Adults. JAMA Netw. Open 2024, 7, e2426590. [Google Scholar] [CrossRef]
- Bailey, A.; Funk, J.; Lessley, D.; Sherwood, C.; Crandall, J.; Neale, W.; Rose, N. Validation of a Videogrammetry Technique for Analysing American Football Helmet Kinematics. Sports Biomech. 2020, 19, 678–700. [Google Scholar] [CrossRef]
- Davenport, E.M.; Urban, J.E.; Mokhtari, F.; Lowther, E.L.; Van Horn, J.D.; Vaughan, C.G.; Gioia, G.A.; Whitlow, C.T.; Stitzel, J.D.; Maldjian, J.A. Subconcussive Impacts and Imaging Findings over a Season of Contact Sports. Concussion 2016, 1, CNC19. [Google Scholar] [CrossRef]
- Johnson, B.; Neuberger, T.; Gay, M.; Hallett, M.; Slobounov, S. Effects of Subconcussive Head Trauma on the Default Mode Network of the Brain. J. Neurotrauma 2014, 31, 1907–1913. [Google Scholar] [CrossRef] [PubMed]
- McKee, A.C.; Stein, T.D.; Nowinski, C.J.; Stern, R.A.; Daneshvar, D.H.; Alvarez, V.E.; Lee, H.-S.; Hall, G.; Wojtowicz, S.M.; Baugh, C.M.; et al. The Spectrum of Disease in Chronic Traumatic Encephalopathy. Brain 2013, 136, 43–64. [Google Scholar] [CrossRef] [PubMed]
- Gardner, R.C.; Langa, K.M.; Yaffe, K. Subjective and Objective Cognitive Function among Older Adults with a History of Traumatic Brain Injury: A Population-Based Cohort Study. PLoS Med. 2017, 14, e1002246. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA research framework: Toward a biological definition of Alzheimer’s disease. Alzheimer’s Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | M (SD)/% | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age | 66.28 (9.70) | - | |||||||||||||||
| 2. Female (%) | 0.52 | −0.07 † | − | ||||||||||||||
| 3. Hispanic (%) | 0.11 | −0.19 *** | 0.05 | − | |||||||||||||
| 4. Nonwhite (%) | 0.25 | −0.21 *** | 0.001 | 0.15 *** | − | ||||||||||||
| 5. Some College Education (%) | 0.34 | −0.04 | 0.01 | −0.10 ** | −0.15 *** | − | |||||||||||
| 6. Health | 2.07 (1.07) | 0.01 | 0.01 | −0.08 * | −0.14 *** | 0.17 *** | − | ||||||||||
| 7. Alzheimer’s Disease (%) | 0.003 | 0.09 * | 0.05 | 0.07 † | 0.03 | −0.04 | −0.05 | − | |||||||||
| 8. Dementia (%) | 0.02 | 0.10 ** | 0.04 | −0.03 | 0.01 | −0.02 | −0.16 *** | 0.34 * | − | ||||||||
| 9. Age: Vehicle | 31.67 (18.38) | 0.32 *** | 0.02 | 0.05 | −0.05 | 0.03 | −0.05 | 0.12 * | 0.08 | − | |||||||
| 10. Age: Fall | 30.06 (23.40) | 0.30 *** | 0.14 ** | −0.07 | −0.10 * | −0.06 | −0.13 * | 0.13 ** | 0.10 * | 0.44 *** | − | ||||||
| 11. Age: Sports | 15.94 (9.76) | 0.01 | −0.06 | 0.19* | 0.11 | 0.02 | 0.02 | − | −0.01 | 0.21 | 0.40 *** | − | |||||
| 12. MG: Vehicle (%) | 0.43 | −0.15 ** | −0.17 * | 0.01 | 0.05 | −0.07 | −0.08 | −0.05 | 0.07 | −0.02 | −0.05 | −0.07 | − | ||||
| 13. MG: Fall (%) | 0.50 | −0.10 * | −0.13 * | −0.02 | 0.03 | −0.08 † | −0.16 ** | −0.001 | 0.06 | 0.04 | −0.04 | 0.17 † | 0.50 *** | − | |||
| 14. MG: Sports (%) | 0.49 | −0.01 | −0.17 * | 0.06 | 0.10 | −0.18 * | −0.06 | 0.08 | 0.08 | 0.08 | 0.21 * | 0.05 | 0.62 *** | 0.46 *** | − | ||
| 15. Self-Rated Memory | 1.98 (0.90) | −0.04 | 0.01 | 0.003 | −0.05 | 0.18 *** | 0.32 *** | 0.001 | −0.12 ** | 0.07 | −0.11 * | −0.09 | −0.12 * | −0.13 * | −0.22 ** | − | |
| 16. Recall Memory | 9.91 (3.42) | −0.25 *** | 0.21 *** | −0.04 | −0.09 * | 0.29 *** | 0.24 *** | −0.10 ** | −0.12 ** | −0.08 | −0.10 * | −0.03 | −0.09 | 0.02 | −0.16 * | 0.23 *** | - |
| Variable | TBI from a Vehicle Accident | TBI from a Fall | TBI from a Sport | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1: Unadjusted | Model 2: Sociodemographic and Health Adjustment | Model 1: Unadjusted | Model 2: Sociodemographic and Health Adjustment | Model 1: Unadjusted | Model 2: Sociodemographic and Health Adjustment | |||||||
| B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | |
| Intercept | 2.02 (0.05) *** | [1.92, 2.12] | 1.87 (0.09) *** | [1.70, 2.04] | 1.96 (0.04) *** | [1.87, 2.05] | 1.88 (0.08) *** | [1.73, 2.03] | 1.98 (0.07) *** | [1.85, 2.12] | 1.92 (0.11) *** | [1.70, 2.14] |
| Age (+1SD) | 0.06 (0.05) | [−0.05, 0.16] | 0.002 (0.04) | [−0.08, 0.09] | 0.02 (0.08) | [−0.13, 0.17] | ||||||
| Female | 0.02 (0.10) | [−0.17, 0.21] | −0.03 (0.09) | [−0.20, 0.14] | −0.04 (0.14) | [−0.32, 0.24] | ||||||
| Hispanic | −0.03 (0.15) | [−0.32, 0.27] | 0.27 (0.13) * | [0.01, 0.53] | 0.64 (0.30) * | [0.05, 1.22] | ||||||
| Nonwhite | 0.13 (0.11) | [−0.09, 0.34] | 0.06 (0.11) | [−0.15, 0.27] | 0.04 (0.16) | [−0.27, 0.35] | ||||||
| Some College Education | 0.34 (0.10) ** | [0.14, 0.54] | 0.17 (0.09) † | [−0.01, 0.35] | 0.14 (0.14) | [−0.13, 0.42] | ||||||
| Health | 0.26 (0.04) *** | [0.17, 0.34] | 0.27 (0.04) *** | [0.19, 0.35] | 0.31 (0.06) *** | [0.19, 0.43] | ||||||
| Age of Onset (+1SD) | 0.01 (0.04) | [−0.07, 0.09] | −0.01 (0.04) | [−0.09, 0.07] | −0.11 (0.04) ** | [−0.19, −0.03] | −0.06 (0.04) | [−0.14, 0.02] | −0.05 (0.04) | [−0.12, 0.02] | −0.05 (0.03) | [−0.12, 0.01] |
| Model Statistics | ||||||||||||
| F (DF) | 0.02 (1, 325) | 7.77 (7, 316) *** | 6.96 (1, 410) ** | 9.25 (7, 404) *** | 1.68 (1, 175) | 5.41 (7, 167) *** | ||||||
| R Square | 0.0001 | 0.15 | 0.02 | 0.14 | 0.01 | 0.18 | ||||||
| Omega-Square | 0.00 | [0.00, 0.01] | 0.13 | [0.07, 0.20] | 0.01 | [0.00, 0.05] | 0.12 | [0.07, 0.19] | 0.00 | [0.00, 0.06] | 0.15 | [0.06, 0.26] |
| Variable | TBI from a Vehicle Accident | TBI from a Fall | TBI from a Sport | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1: Unadjusted | Model 2: Sociodemographic and Health Adjustment | Model 1: Unadjusted | Model 2: Sociodemographic and Health Adjustment | Model 1: Unadjusted | Model 2: Sociodemographic and Health Adjustment | |||||||
| B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | |
| Intercept | 10.04 (0.19) *** | [9.66, 10.41] | 8.90 (0.32) *** | [8.27, 9.54] | 9.99 (0.17) *** | [9.66, 10.32] | 8.81 (0.27) *** | [8.28, 9.34] | 10.01 (0.25) *** | [9.51, 10.50] | 9.25 (0.40) *** | [8.47, 10.04] |
| Age (+1SD) | −0.78 (0.20) *** | [−1.17, −0.40] | −0.89 (0.16) *** | [−1.20, −0.58] | −0.55 (0.28) * | [−1.09, −0.002] | ||||||
| Female | 1.07 (0.35) ** | [0.38, 1.77] | 1.14 (0.31) *** | [0.54, 1.75] | 0.57 (0.50) | [−0.42, 1.56] | ||||||
| Hispanic | −0.59 (0.55) | [−1.68, 0.50] | −0.54 (0.48) | [−1.48, 0.40] | −0.74 (1.06) | [−2.83, 1.34] | ||||||
| Nonwhite | −1.03 (0.41) * | [−1.84, −0.23] | −0.58 (0.38) | [−1.32, 0.17] | −0.30 (0.55) | [−1.39, 0.79] | ||||||
| Some College Education | 1.75 (0.38) *** | [1.001, 2.50] | 1.74 (0.33) *** | [1.10, 2.38] | 1.38 (0.49) ** | [0.41, 2.35] | ||||||
| Health | 0.66 (0.16) *** | [0.35, 0.98] | 0.57 (0.15) *** | [0.28, 0.86] | 0.98 (0.22) *** | [0.54, 1.41] | ||||||
| Age of Onset (+1SD) | −0.24 (0.16) | [−0.54, 0.07] | −0.04 (0.15) | [−0.34, 0.25] | −0.33 (0.15) * | [−0.63, −0.03] | −0.09 (0.14) | [−0.38, 0.19] | −0.21 (0.13) | [−0.47, 0.05] | −0.15 (0.12) | [−0.39, 0.09] |
| Model Statistics | ||||||||||||
| F (DF) | 2.31 (1, 324) | 12.04 (7, 315) *** | 4.70 (1, 412) * | 16.79 (7, 406) *** | 2.53 (1, 175) | 6.92 (7, 167) *** | ||||||
| R Square | 0.01 | 0.21 | 0.01 | 0.22 | 0.01 | 0.22 | ||||||
| Omega-Square | 0.00 | [0.00, 0.04] | 0.19 | [0.12, 0.27] | 0.01 | [0.00, 0.04] | 0.21 | [0.15, 0.28] | 0.00 | [0.00, 0.07] | 0.19 | [0.10, 0.30] |
| Variable | TBI from a Vehicle Accident | TBI from a Fall | TBI from a Sport | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1: Unadjusted | Model 2: Sociodemographic and Health Adjustment | Model 1: Unadjusted | Model 2: Sociodemographic and Health Adjustment | Model 1: Unadjusted | Model 2: Sociodemographic and Health Adjustment | |||||||
| B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | |
| Intercept | 2.12 (0.07) *** | [1.99, 2.25] | 2.00 (0.10) *** | [1.80, 2.20] | 2.07 (0.06) *** | [1.95, 2.20] | 1.96 (0.09) *** | [1.78, 2.14] | 2.20 (0.09) *** | [2.02, 2.38] | 2.17 (0.13) *** | [1.91, 2.44] |
| Age (+1SD) | 0.04 (0.05) | [−0.06, 0.14] | −0.02 (0.04) | [−0.11, 0.06] | −0.01 (0.08) | [−0.15, 0.14] | ||||||
| Female | −0.05 (0.10) | [−0.24, 0.14] | −0.07 (0.09) | [−0.24, 0.10] | −0.08 (0.14) | [−0.36, 0.19] | ||||||
| Hispanic | −0.07 (0.14) | [−0.35, 0.22] | 0.27 (0.14) * | [0.002, 0.54] | 0.63 (0.29) * | [0.06, 1.19] | ||||||
| Nonwhite | 0.09 (0.11) | [−0.12, 0.31] | 0.07 (0.11) | [−0.15, 0.28] | 0.03 (0.15) | [−0.27, 0.33] | ||||||
| Some College Education | 0.31 (0.10) ** | [0.11, 0.51] | 0.18 (0.09) † | [−0.003, 0.36] | 0.07 (0.14) | [−0.20, 0.34] | ||||||
| Health | 0.24 (0.04) *** | [0.16, 0.33] | 0.27 (0.04) *** | [0.19, 0.35] | 0.28 (0.06) *** | [0.16, 0.40] | ||||||
| Memory Gap | −0.22 (0.10) * | [−0.42, −0.03] | −0. 14 (0.10) | [−0.33, 0.05] | −0.23 (0.09) * | [−0.41, −0.05] | −0.13 (0.09) | [−0.30, 0.04] | −0.40 (0.13) ** | [−0.66, 0.14] | −0.41 (0.13) ** | [−0.67, −0.16] |
| Model Statistics | ||||||||||||
| F (DF) | 4.93 (1, 320) * | 7.51 (7, 311) *** | 6.54 (1, 404) * | 8.99 (7, 398) *** | 9.17 (1, 173) | 5.88 (7, 165) *** | ||||||
| R Square | 0.02 | 0.14 | 0.02 | 0.14 | 0.05 | 0.20 | ||||||
| Omega-Square | 0.01 | [0.00, 0.05] | 0.13 | [0.06, 0.20] | 0.01 | [0.00, 0.05] | 0.12 | [0.07, 0.19] | 0.04 | [0.01, 0.13] | 0.16 | [0.07, 0.27] |
| Variable | TBI from a Vehicle Accident | TBI from a Fall | TBI from a Sport | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1: Unadjusted | Model 2: Sociodemographic and Health Adjustment | Model 1: Unadjusted | Model 2: Sociodemographic and Health Adjustment | Model 1: Unadjusted | Model 2: Sociodemographic and Health Adjustment | |||||||
| B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI | |
| Intercept | 10.37 (0.25) *** | [9.88, 10.86] | 9.37 (0.37) *** | [8.64, 10.09] | 9.93 (0.24) *** | [9.45, 10.40] | 8.55 (0.33) *** | [7.91, 9.20] | 10.53 (0.35) *** | [9.85, 11.22] | 9.58 (0.48) *** | [8.63, 10.54] |
| Age (+1SD) | −0.90 (0.18) *** | [−1.26, −0.54] | −0.89 (0.15) *** | [−1.20, −0.59] | −0.55 (0.28) * | [−1.09, −0.01] | ||||||
| Female | 0.84 (0.35) ** | [0.15, 1.54] | 1.13 (0.31) *** | [0.53, 1.74] | 0.42 (0.50) | [−0.57, 1.42] | ||||||
| Hispanic | −0.51 (0.52) | [−1.53, 0.52] | −0.59 (0.48) | [−1.54, 0.36] | −0.80 (1.03) | [−2.84, 1.25] | ||||||
| Nonwhite | −1.28 (0.40) ** | [−2.08, −0.49] | −0.55 (0.38) | [−1.30, 0.20] | −0.13 (0.55) | [−1.22, 0.95] | ||||||
| Some College Education | 1.59 (0.37) *** | [0.86, 2.32] | 1.87 (0.33) *** | [1.22, 2.52] | 1.33 (0.49) ** | [0.36, 2.30] | ||||||
| Health | 0.61 (0.16) *** | [0.30, 0.92] | 0.57 (0.15) *** | [0.28, 0.87] | 1.02 (0.22) *** | [0.58, 1.46] | ||||||
| Memory Gap | −0.60 (0.38) | [−1.34, 0.15] | −0.44 (0.35) | [−1.14, 0.25] | 0.14 (0.34) | [−0.53, 0.81] | 0.45 (0.31) | [−0.16, 1.07] | −1.06 (0.50) * | [−2.04, −0.08] | −0.67 (0.47) | [−1.59, 0.26] |
| Model Statistics | ||||||||||||
| F (DF) | 2.50 (1, 318) | 12.27 (7, 309) *** | 0.16 (1, 406) * | 16.77 (7, 400) *** | 4.58 (1, 173) * | 7.42 (7, 165) *** | ||||||
| R Square | 0.01 | 0.22 | 0.00 | 0.23 | 0.03 | 0.24 | ||||||
| Omega-Square | 0.00 | [0.00, 0.04] | 0.20 | [0.13, 0.28] | 0.00 | [0.00, 0.01] | 0.21 | [0.15, 0.28] | 0.02 | [0.00, 0.09] | 0.21 | [0.11, 0.32] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerino, E.S.; Lininger, M.R.; Seaton, T.J.; Porter, G.; Baldwin, J.A. Associations Between Traumatic Brain Injury Characteristics and Memory Outcomes: Insights from the Health and Retirement Study. Int. J. Environ. Res. Public Health 2025, 22, 150. https://doi.org/10.3390/ijerph22020150
Cerino ES, Lininger MR, Seaton TJ, Porter G, Baldwin JA. Associations Between Traumatic Brain Injury Characteristics and Memory Outcomes: Insights from the Health and Retirement Study. International Journal of Environmental Research and Public Health. 2025; 22(2):150. https://doi.org/10.3390/ijerph22020150
Chicago/Turabian StyleCerino, Eric S., Monica R. Lininger, Thomasina J. Seaton, Gillian Porter, and Julie A. Baldwin. 2025. "Associations Between Traumatic Brain Injury Characteristics and Memory Outcomes: Insights from the Health and Retirement Study" International Journal of Environmental Research and Public Health 22, no. 2: 150. https://doi.org/10.3390/ijerph22020150
APA StyleCerino, E. S., Lininger, M. R., Seaton, T. J., Porter, G., & Baldwin, J. A. (2025). Associations Between Traumatic Brain Injury Characteristics and Memory Outcomes: Insights from the Health and Retirement Study. International Journal of Environmental Research and Public Health, 22(2), 150. https://doi.org/10.3390/ijerph22020150