
Gynaecological Health Patterns and Motherhood Experiences of Female Professional Football Players

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Designs and Ethical Considerations
2.2. Participant Selection
2.3. Dependent Variables
2.4. Descriptive Variables
2.5. Procedures and Data Storage
2.6. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Gynaecological Health Patterns and Body Perception
3.3. Motherhood Experiences and RTT/RTC
4. Discussion
4.1. Menstrual Cycle
4.2. Contraceptive Use
4.3. BD and DT
4.4. Motherhood Experiences
4.5. Practical Implications
4.6. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vogel, K.; Larsen, B.; McLellan, C.; Bird, S.P. Female Athletes and the Menstrual Cycle in Team Sports: Current State of Play and Considerations for Future Research. Sports 2023, 12, 4. [Google Scholar] [CrossRef]
- Elliott-Sale, K.J.; McNulty, K.L.; Ansdell, P.; Goodall, S.; Hicks, K.M.; Thomas, K.; Swinton, P.A.; Dolan, E. The Effects of Oral Contraceptives on Exercise Performance in Women: A Systematic Review and Meta-analysis. Sports Med. 2020, 50, 1785–1812. [Google Scholar] [CrossRef]
- Robles-Palazón, F.J.; López-Valenciano, A.; De Ste Croix, M.; Oliver, J.L.; García-Gómez, A.; Sainz de Baranda, P.; Ayala, F. Epidemiology of injuries in male and female youth football players: A systematic review and meta-analysis. J. Sport Health Sci. 2022, 11, 681–695. [Google Scholar] [CrossRef]
- Wing, C.; Hart, N.H.; McCaskie, C.; Djanis, P.; Ma'ayah, F.; Nosaka, K. Running Performance of Male Versus Female Players in Australian Football Matches: A Systematic Review. Sports Med Open. 2021, 7, 96. [Google Scholar] [CrossRef]
- Bilgoe, S.C.; Janse van Rensburg, D.C.C.; Goedhart, E.; Orhant, E.; Kerkhoffs, G.; Gouttebarge, V. Unmasking mental health symptoms in female professional football players: A 12-month follow-up study. BMJ Open Sport Exerc Med. 2024, 10, e001922. [Google Scholar] [CrossRef]
- Clarke, A.C.; Bruinvels, G.; Julian, R.; Inge, P.; Pedlar, C.R.; Govus, A.D. Hormonal Contraceptive Use in Football Codes in Australia. Front. Sports Act. Living 2021, 3, 634866. [Google Scholar] [CrossRef]
- Baumgartner, S.; Bitterlich, N.; Geboltsberger, S.; Neuenschwander, M.; Matter, S.; Stute, P. Contraception, female cycle disorders and injuries in Swiss female elite athletes—A cross sectional study. Front. Physiol. 2023, 14, 1232656. [Google Scholar] [CrossRef]
- Davenport, M.H.; Nesdoly, A.; Ray, L.; Thornton, J.S.; Khurana, R.; McHugh, T.F. Pushing for change: A qualitative study of the experiences of elite athletes during pregnancy. Br. J. Sports Med. 2022, 56, 452–457. [Google Scholar] [CrossRef]
- Davenport, M.H.; Ray, L.; Nesdoly, A.; Thornton, J.; Khurana, R.; McHugh, T.F. We’re not Superhuman, We’re Human: A Qualitative Description of Elite Athletes’ Experiences of Return to Sport After Childbirth. Sports Med. 2022, 53, 269–279. [Google Scholar] [CrossRef]
- Tekavc, J.; Wylleman, P.; Erpič, S.C. Perceptions of dual career development among elite level swimmers and basketball players. Psychol. Sport Exerc. 2015, 21, 27–41. [Google Scholar] [CrossRef]
- Culvin, A.; Bowes, A. The Incompatibility of Motherhood and Professional Women’s Football in England. Front. Sports Act. Living 2021, 3, 730151. [Google Scholar] [CrossRef] [PubMed]
- Grenier, L.N.; Atkinson, S.A.; Mottola, M.F.; Wahoush, O.; Thabane, L.; Xie, F.; Vickers-Manzin, J.; Moore, C.; Hutton, E.K.; Murray-Davis, B. Be Healthy in Pregnancy: Exploring factors that impact pregnant women’s nutrition and exercise behaviours. Matern. Child Nutr. 2021, 17, e13068. [Google Scholar] [CrossRef]
- Dietz, P.; Legat, L.; Sattler, M.C.; van Poppel, M.N.M. Triple careers of athletes: Exploring the challenges of planning a pregnancy among female elite athletes using semi-structured interviews. BMC Pregnancy Childbirth 2022, 22, 643. [Google Scholar] [CrossRef]
- Physical Activity and Exercise During Pregnancy and the Postpartum Period: ACOG Committee Opinion, Number 804. Obstet Gynecol. 2020, 135, e178–e188. [CrossRef]
- Smith, S.V.M.; Darroch, F.E.; Giles, A.R.; Wykes, D. Fatherhood and Elite Athletics: Sacrifice, Selfishness, and Gaining “Dad Strength”. J. Men’s Stud. 2024, 32, 152–177. [Google Scholar] [CrossRef]
- FIFPRO. Men’s Football: Global Report. 2016. Available online: https://fifpro.org/en/supporting-players/competitions-innovation-and-growth/global-employment-market-for-men-s-football/men-s-global-employment-report (accessed on 25 November 2024).
- Players’ Union; WorldFITPro. 2017 FIFPRO GLOBAL EMPLOYMENT REPORT; The University of Manchester: Manchester, UK, 2017. [Google Scholar]
- FIFPRO. FIFPRO Launches Return to Play Guidelines After Childbirth; FIFPRO World Players’ Union: Hoofddorp, The Netherlands, 2024. [Google Scholar]
- Woodward, M. Epidemiology: Study Design and Data Analysis, 3rd ed.; Chapman & Hall: London, UK, 2014. [Google Scholar]
- Pourhoseingholi, M.A.; Vahedi, M.; Rahimzadeh, M. Sample size calculation in medical studies. Gastroenterol. Hepatol. Bed Bench 2013, 6, 14–17. [Google Scholar]
- Garner, D.M. Eating Disorder Inventory-3 (EDI-3). Int. J. Eat. Disord. 2004, 35, 478–479. [Google Scholar]
- Lang, B.; Ahlich, E.; Verzijl, C.L.; Thompson, J.K.; Rancourt, D. The role of drive for thinness in the association between weight status misperception and disordered eating. Eat. Behav. 2019, 35, 101319. [Google Scholar] [CrossRef]
- Keys, A.; Fidanza, F.; Karvonen, M.J.; Kimura, N.; Taylor, H.L. Indices of relative weight and obesity. J. Chronic Dis. 1972, 25, 329–343. [Google Scholar] [CrossRef]
- Carmody, S.; den Hollander, S.; Elliott-Sale, K.; Mountjoy, M.L.; Thornton, J.S.; Massey, A.; Kerkhoffs, G.; Gouttebarge, V. Self-reported reproductive health of retired elite women’s footballers: A cross-sectional study. BMJ Open Sport Exerc. Med. 2024, 10, e002028. [Google Scholar] [CrossRef]
- Ling, D.I.; Hannafin, J.A.; Prather, H.; Skolnik, H.; Chiaia, T.A.; de Mille, P.; Lewis, C.L.; Casey, E. The Women’s Soccer Health Study: From Head to Toe. Sports Med. 2023, 53, 2001–2010. [Google Scholar] [CrossRef]
- Oxfeldt, M.; Dalgaard, L.B.; Jørgensen, A.A.; Hansen, M. Hormonal Contraceptive Use, Menstrual Dysfunctions, and Self-Reported Side Effects in Elite Athletes in Denmark. Int. J. Sports Physiol. Perform. 2020, 15, 1377–1384. [Google Scholar] [CrossRef]
- Martin, D.; Sale, C.; Cooper, S.B.; Elliott-Sale, K.J. Period Prevalence and Perceived Side Effects of Hormonal Contraceptive Use and the Menstrual Cycle in Elite Athletes. Int. J. Sports Physiol. Perform. 2018, 13, 926–932. [Google Scholar] [CrossRef]
- Findlay, R.J.; Macrae, E.H.R.; Whyte, I.Y.; Easton, C.; Forrest, L.J. How the menstrual cycle and menstruation affect sporting performance: Experiences and perceptions of elite female rugby players. Br. J. Sports Med. 2020, 54, 1108–1113. [Google Scholar] [CrossRef]
- Armour, M.; Parry, K.A.; Steel, K.; Smith, C.A. Australian female athlete perceptions of the challenges associated with training and competing when menstrual symptoms are present. Int. J. Sports Sci. Coach. 2020, 15, 316–323. [Google Scholar] [CrossRef]
- Randell, R.K.; Clifford, T.; Drust, B.; Moss, S.L.; Unnithan, V.B.; De Ste Croix, M.B.A.; Datson, N.; Martin, D.; Mayho, H.; Carter, J.M.; et al. Physiological Characteristics of Female Soccer Players and Health and Performance Considerations: A Narrative Review. Sports Med. 2021, 51, 1377–1399. [Google Scholar] [CrossRef]
- Carmichael, M.A.; Thomson, R.L.; Moran, L.J.; Dunstan, J.R.; Nelson, M.J.; Mathai, M.L.; Wycherley, T.P. A Pilot Study on the Impact of Menstrual Cycle Phase on Elite Australian Football Athletes. Int. J. Environ. Res. Public Health 2021, 18, 9591. [Google Scholar] [CrossRef]
- Godoy-Izquierdo, D.; Díaz, I. Inhabiting the Body(ies) in Female Soccer Players: The Protective Role of Positive Body Image. Front. Psychol. 2021, 12, 718836. [Google Scholar] [CrossRef]
- Zaccagni, L.; Gualdi-Russo, E. The Impact of Sports Involvement on Body Image Perception and Ideals: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 5228. [Google Scholar] [CrossRef]
- Lundqvist, C.; Schary, D.P.; Eklöf, E.; Zand, S.; Jacobsson, J. Elite lean athletes at sports high schools face multiple risks for mental health concerns and are in need of psychosocial support. PLoS ONE 2023, 18, e0284725. [Google Scholar] [CrossRef]
- Joy, E.; Kussman, A.; Nattiv, A. 2016 update on eating disorders in athletes: A comprehensive narrative review with a focus on clinical assessment and management. Br. J. Sports Med. 2016, 50, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Scheid, J.L.; Stefanik, M.E. Drive for Thinness Predicts Musculoskeletal Injuries in Division II NCAA Female Athletes. J. Funct. Morphol. Kinesiol. 2019, 4, 52. [Google Scholar] [CrossRef] [PubMed]
- Maurin, J.; Labossière, S.; Pomerleau-Fontaine, L.; Boudreault, V.; Brassard, S.; Dion, J.; Durand-Bush, N.; Parent, S.; Soulard, A. Personal risk factors and types of sport associated with drive for thinness and drive for muscularity in NextGen athletes. Front. Nutr. 2024, 11, 1392064. [Google Scholar] [CrossRef]
- Abbott, W.; Brett, A.; Brownlee, T.E.; Hammond, K.M.; Harper, L.D.; Naughton, R.J.; Anderson, L.; Munson, E.H.; Sharkey, J.V.; Randell, R.K.; et al. The prevalence of disordered eating in elite male and female soccer players. Eat. Weight. Disord.-Stud. Anorex. Bulim. Obes. 2021, 26, 491–498. [Google Scholar] [CrossRef]
- Sundgot-Borgen, J.; Sundgot-Borgen, C.; Myklebust, G.; Sølvberg, N.; Torstveit, M.K. Elite athletes get pregnant, have healthy babies and return to sport early postpartum. BMJ Open Sport Exerc. Med. 2019, 5, e000652. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | All Participants (n = 74) | |
|---|---|---|
| Age (yrs) mean (SD) | 24.95 (2.69) | |
| Height (cm) mean (SD) | 168.39 (5.38) | |
| Weight (kg) mean (SD) | 62.81 (5.4) | |
| BMI (kg/m2) mean (SD) | 22.14 (1.47) | |
| Stress fractures n (%) | 11 (15) | |
| Low bone density n (%) | 1 (1.35) | |
| Other characteristics | ||
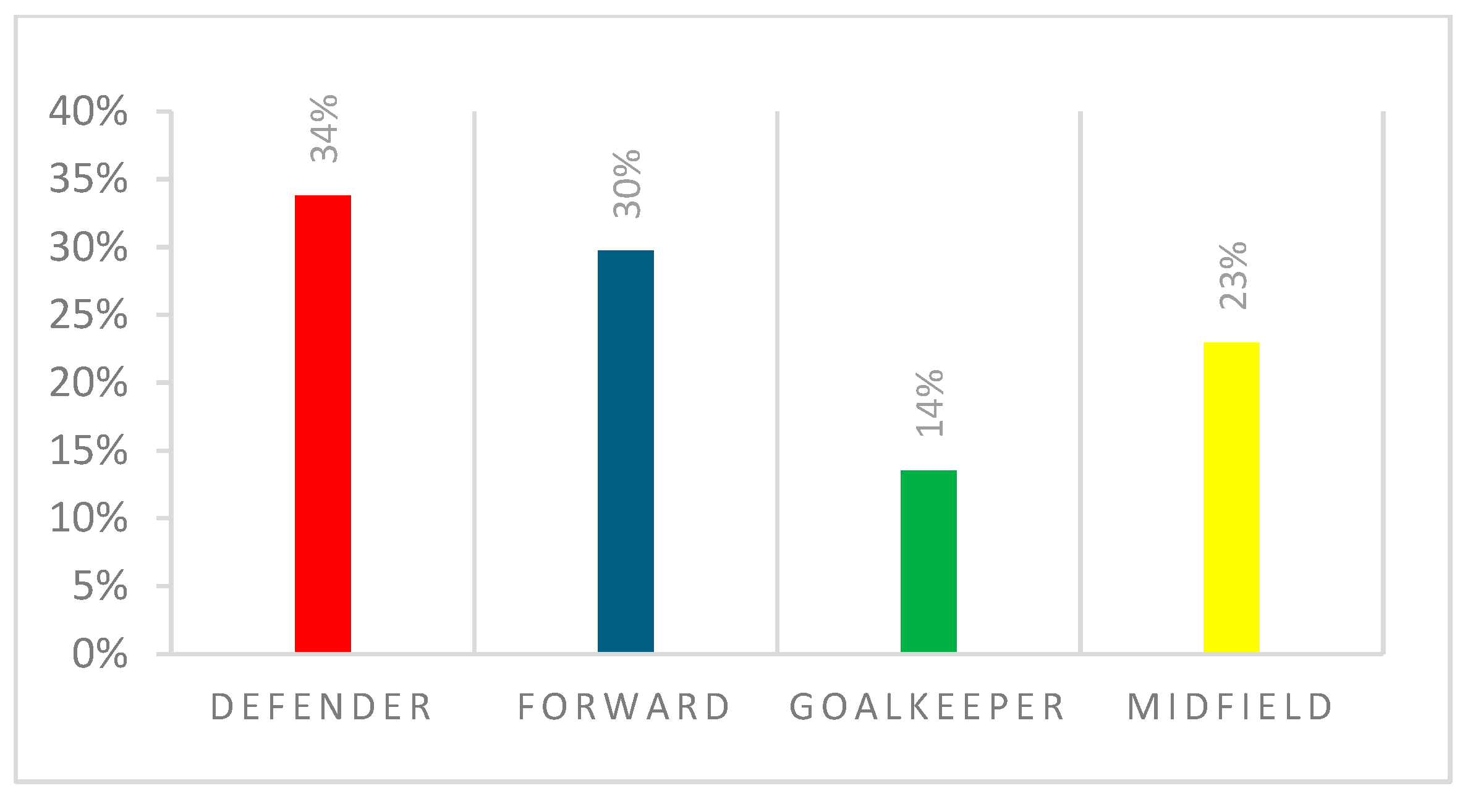
| Field Position n (%) | defender | 25 (34%) |
| forward | 22 (30%) | |
| midfield | 17 (23%) | |
| goalkeeper | 10 (13%) | |
| Number of seasons as a professional player Mean (SD) | 5.74 (3.12) | |
| Employed | yes | 22 (30%) |
| Level of Football n (%) | highest national level | 64 (87%) |
| second highest national level | 6 (8%) | |
| other | 4 (5%) | |
| Variable | Characteristics | All Participants (n = 74) |
|---|---|---|
| Age of Menstruation (yrs) Mean (SD) | 13.47 (1.3) | |
| Duration of menstruation cycle (days) Mean (SD) | 25.81 (13.09) | |
| Duration of menstrual bleeding period (days) Mean (SD) | 5.16 (3.42) | |
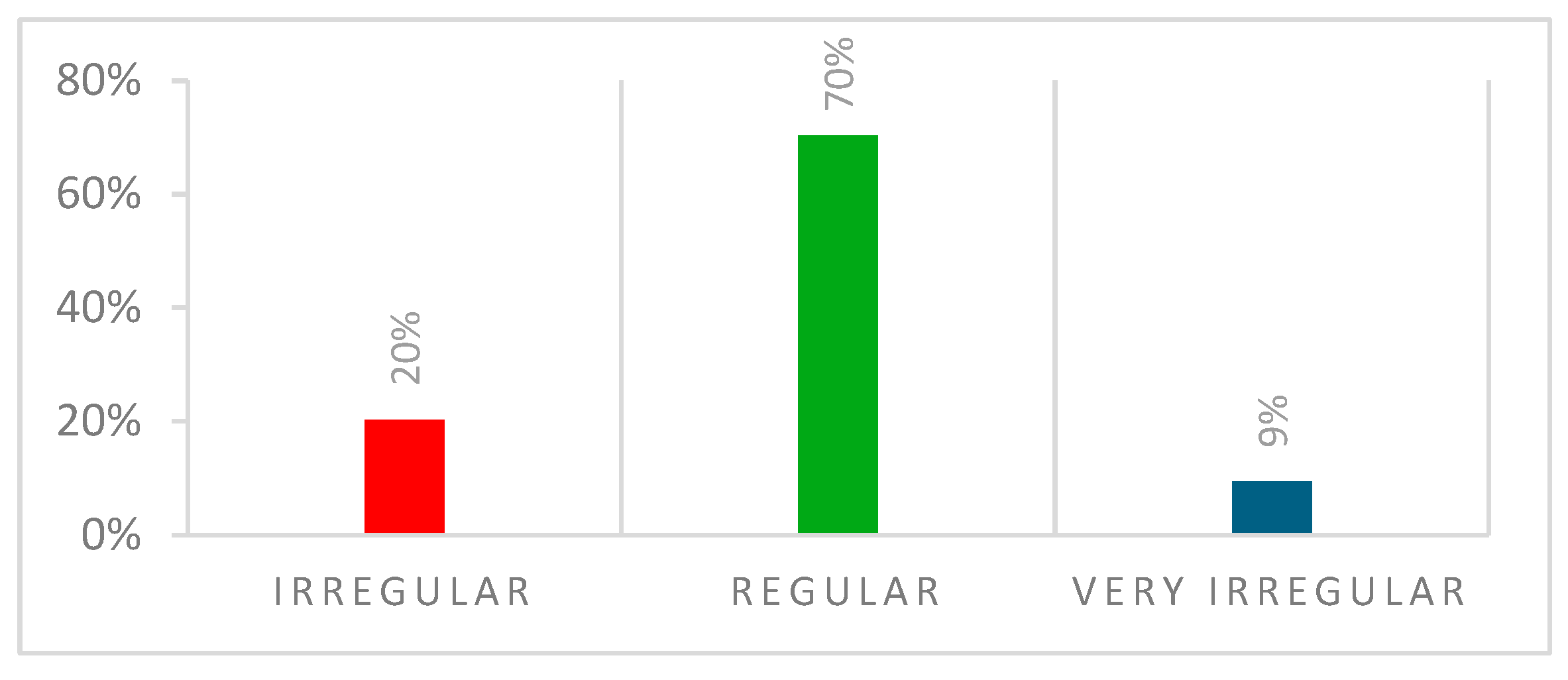
| Description of menstruation cycle n (%) | regular | 52 (70%) |
| irregular | 15 (20%) | |
| very irregular | 7 (10%) | |
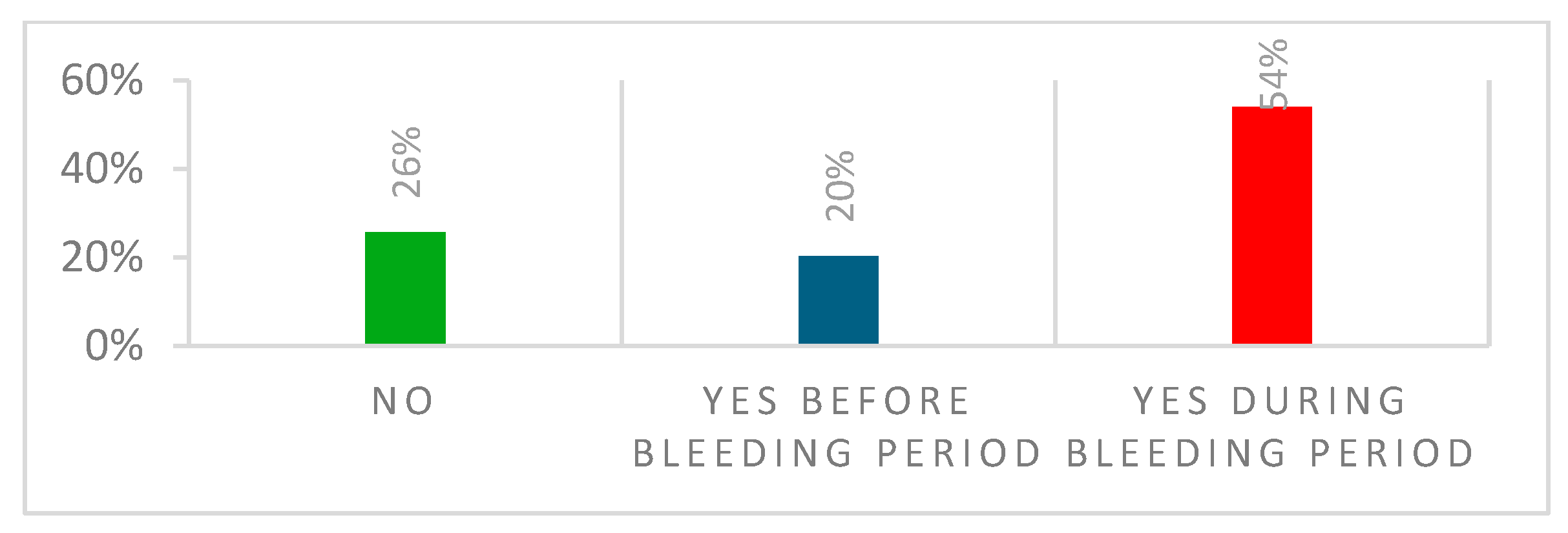
| Pain during menstruation cycle n (%) | during bleeding period | 40 (54%) |
| none | 19 (26%) | |
| before bleeding period | 15 (20%) | |
| none | 37 (50%) | |
| pill | 14 (38%) | |
| Contraception Methods n (%) | condom | 12 (32%) |
| other | 8 (22%) | |
| implant | 7 (20%) | |
| hormone replacement | 4 (10%) | |
| injection | 1 (2%) | |
| Body dissatisfaction Mean (SD) | 4.88 (5.08) | |
| Drive for thinness Mean (SD) | 3.59 (5.04) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramagole, D.A.; van Rensburg, D.C.J.; Cowie, C.; Mehta, R.; Ramkilawon, G.; Pluim, B.M.; Kerkhoffs, G.; Gouttebarge, V. Gynaecological Health Patterns and Motherhood Experiences of Female Professional Football Players. Int. J. Environ. Res. Public Health 2025, 22, 136. https://doi.org/10.3390/ijerph22020136
Ramagole DA, van Rensburg DCJ, Cowie C, Mehta R, Ramkilawon G, Pluim BM, Kerkhoffs G, Gouttebarge V. Gynaecological Health Patterns and Motherhood Experiences of Female Professional Football Players. International Journal of Environmental Research and Public Health. 2025; 22(2):136. https://doi.org/10.3390/ijerph22020136
Chicago/Turabian StyleRamagole, Dimakatso Althea, Dina Christa Janse van Rensburg, Charlotte Cowie, Ritan Mehta, Gopika Ramkilawon, Babette M. Pluim, Gino Kerkhoffs, and Vincent Gouttebarge. 2025. "Gynaecological Health Patterns and Motherhood Experiences of Female Professional Football Players" International Journal of Environmental Research and Public Health 22, no. 2: 136. https://doi.org/10.3390/ijerph22020136
APA StyleRamagole, D. A., van Rensburg, D. C. J., Cowie, C., Mehta, R., Ramkilawon, G., Pluim, B. M., Kerkhoffs, G., & Gouttebarge, V. (2025). Gynaecological Health Patterns and Motherhood Experiences of Female Professional Football Players. International Journal of Environmental Research and Public Health, 22(2), 136. https://doi.org/10.3390/ijerph22020136