
The Risk of Aircraft-Acquired SARS-CoV-2 Transmission during Commercial Flights: A Systematic Review

 ,
, _Tsui.png) ,
,
Abstract
1. Introduction
2. Materials and Methods
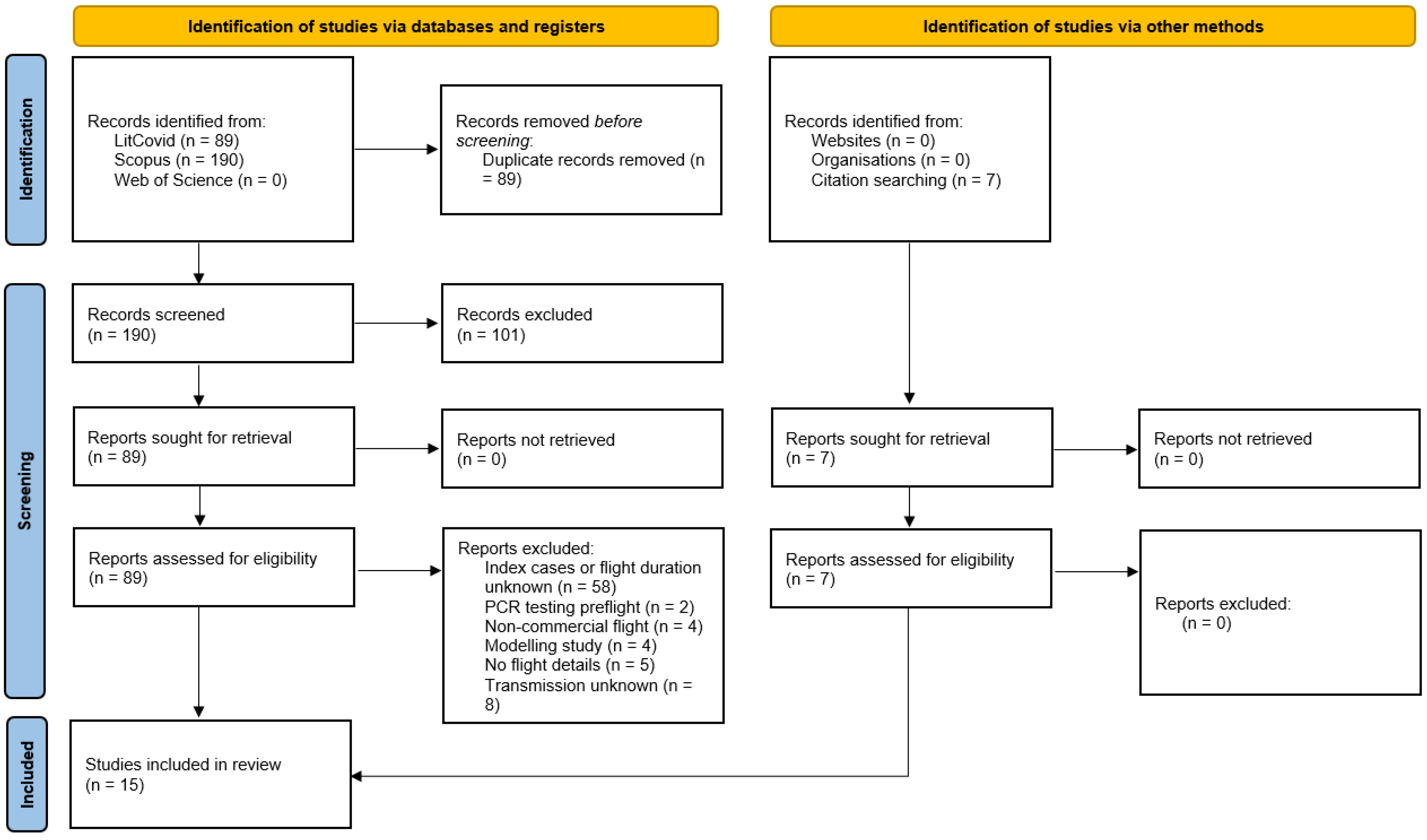
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 13 May 2021).
- United Nations. 2020 Passenger Totals Drop 60 Percent as COVID-19 Assault on International Mobility Continues. Available online: https://www.icao.int/Newsroom/Pages/2020-passenger-totals-drop-60-percent-as-COVID19-assault-on-international-mobility-continues.aspx (accessed on 13 May 2021).
- OECD. COVID-19 and the Aviation Industry: Impact and Policy Responses. Available online: https://www.oecd.org/coronavirus/policy-responses/covid-19-and-the-aviation-industry-impact-and-policy-responses-26d521c1/ (accessed on 13 May 2021).
- Global Air Travel Demand Continued Its Bounce Back in 2023. Available online: https://www.iata.org/en/pressroom/2024-releases/2024-01-31-02/ (accessed on 8 May 2024).
- The Changing Threat of COVID-19|CDC. Available online: https://www.cdc.gov/ncird/whats-new/changing-threat-covid-19.html (accessed on 8 May 2024).
- Airports Council International. The Impact of COVID-19 on the Airport Business and the Path to Recovery. Available online: https://aci.aero/2021/03/25/the-impact-of-covid-19-on-the-airport-business-and-the-path-to-recovery/ (accessed on 22 June 2022).
- CDC; Interim U.S. Guidance for Risk Assessment and Work Restrictions for Healthcare Personnel with Potential Exposure to SARS-CoV-2. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-risk-assesment-hcp.html (accessed on 13 May 2021).
- Bazant, M.Z.; Bush, J.W.M. A guideline to limit indoor airborne transmission of COVID-19. Proc. Natl. Acad. Sci. USA 2021, 118, e2018995118. [Google Scholar] [CrossRef] [PubMed]
- Olsen, S.J.; Chang, H.-L.; Cheung, T.Y.-Y.; Tang, A.F.-Y.; Fisk, T.L.; Ooi, S.P.-L.; Kuo, H.-W.; Jiang, D.D.-S.; Chen, K.-T.; Lando, J.; et al. Transmission of the Severe Acute Respiratory Syndrome on Aircraft. N. Engl. J. Med. 2003, 349, 2416–2422. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.O.; Wilder-Smith, A. In-flight transmission of SARS-CoV-2: A review of the attack rates and available data on the efficacy of face masks. J. Travel. Med. 2020, 27, taaa178. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Allot, A.; Lu, Z. LitCovid: An open database of COVID-19 literature. Nucleic Acids Res. 2021, 49, D1534–D1540. [Google Scholar] [CrossRef] [PubMed]
- Lash, T.L.; VanderWeele, J.; Haneuse, S.; Rothman, K.J. Modern Epidemiology, 4th ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2020. [Google Scholar]
- VanderWeele, T.; Ding, P. Sensitivity analysis in observational research: Introducing the E-value. Ann. Intern. Med. 2017, 167, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Mathur, M.; Ding, P.; Riddell, C.; VanderWeele, T. Website and R package for computing E-values. Epidemiology 2018, 29, e45–e47. [Google Scholar] [CrossRef] [PubMed]
- Eldin, C.; Lagier, J.C.; Mailhe, M.; Gautret, P. Probable aircraft transmission of Covid-19 in-flight from the Central African Republic to France. Travel. Med. Infect. Dis. 2020, 35, 101643. [Google Scholar] [CrossRef]
- Blomquist, P.B.; Bolt, H.; Packer, S.; Schaefer, U.; Platt, S.; Dabrera, G.; Gobin, M.; Oliver, I. Risk of symptomatic COVID-19 due to aircraft transmission: A retrospective cohort study of contact-traced flights during England’s containment phase. Influenza Other Respir. Viruses 2021, 15, 336–344. [Google Scholar] [CrossRef]
- Pavli, A.; Smeti, P.; Hadjianastasiou, S.; Theodoridou, K.; Spilioti, A.; Papadima, K.; Andreopoulou, A.; Gkolfinopoulou, K.; Sapounas, S.; Spanakis, N.; et al. In-flight transmission of COVID-19 on flights to Greece: An epidemiological analysis. Travel. Med. Infect. Dis. 2020, 38, 101882. [Google Scholar] [CrossRef]
- Zhang, X.-A.; Fan, H.; Qi, R.-Z.; Zheng, W.; Zheng, K.; Gong, J.-H.; Fang, L.-Q.; Liu, W. Importing coronavirus disease 2019 (COVID-19) into China after international air travel. Travel. Med. Infect. Dis. 2020, 35, 101620. [Google Scholar] [CrossRef]
- Hoehl, S.; Karaca, O.; Kohmer, N.; Westhaus, S.; Graf, J.; Goetsch, U.; Ciesek, S. Assessment of SARS-CoV-2 Transmission on an International Flight and among a Tourist Group. JAMA Netw. Open 2020, 3, e2018044. [Google Scholar] [CrossRef]
- Chen, J.; He, H.; Cheng, W.; Liu, Y.; Sun, Z.; Chai, C.; Kong, Q.; Sun, W.; Zhang, J.; Guo, S.; et al. Potential transmission of SARS-CoV-2 on a flight from Singapore to Hanghzou, China: An epidemiologicalinvestigation. Travel. Med. Infect. Dis. 2020, 36, 101816. [Google Scholar] [CrossRef] [PubMed]
- Yang, N.; Shen, Y.; Shi, C.; Ma, A.H.Y.; Zhang, X.; Jian, X.; Wang, L.; Shi, J.; Wu, C.; Li, G.; et al. In-flight transmission cluster of COVID-19: A retrospective case series. Infect. Dis. 2020, 52, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Speake, H.; Phillips, A.; Chong, T.; Sikazwe, C.; Levy, A.; Lang, J.; Scalley, B.; Speers, D.J.; Smith, D.W.; Effler, P.; et al. Flight-associated transmission of severe acute respiratory syndrome coronavirus 2 corroborated by whole-genome sequencing. Emerg. Infect. Dis. 2020, 26, 2872–2880. [Google Scholar] [CrossRef]
- Murphy, N.; Boland, M.; Bambury, N.; Fitzgerald, M.; Comerford, L.; Dever, N.; O’sullivan, M.B.; Petty-Saphon, N.; Kiernan, R.; Jensen, M.; et al. A large national outbreak of COVID-19 linked to air travel, Ireland, summer 2020. Euro Surveill. 2020, 25, 2001624. [Google Scholar] [CrossRef] [PubMed]
- Khanh, N.C.; Thai, P.Q.; Quach, H.-L.; Thi, N.-A.H.; Dinh, P.C.; Duong, T.N.; Mai, L.T.Q.; Nghia, N.D.; Tu, T.A.; Quang, L.N.; et al. Transmission of SARS-CoV 2 During Long-Haul Flight. Emerg. Infect. Dis. 2020, 26, 2617–2624. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.H.; Shin, H.; Koo, H.Y.; Lee, S.W.; Yang, J.M.; Yon, D.K. Asymptomatic transmission of SARS-CoV-2 on evacuation flight. Emerg. Infect. Dis. 2020, 26, 2705–2708. [Google Scholar] [CrossRef]
- Choi, E.M.; Chu, D.K.W.; Cheng, P.K.C.; Tsang, D.N.C.; Peiris, M.; Bausch, D.G.; Poon, L.L.M.; Watson-Jones, D. In-Flight Transmission of SARS-CoV-2. Emerg. Infect. Dis. 2020, 26, 2713–2716. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, K.L.; Murti, M.; Finkelstein, M.; Leis, J.A.; Fitzgerald-Husek, A.; Bourns, L.; Meghani, H.; Saunders, A.; Allen, V.; Yaffe, B. Lack of COVID-19 transmission on an international flight. CMAJ 2020, 192, E410. [Google Scholar] [CrossRef]
- Nir-Paz, R.; Grotto, I.; Strolov, I.; Salmon, A.; Mandelboim, M.; Mendelson, E.; Regev-Yochay, G. Absence of in-flight transmission of SARS-CoV-2 likely due to use of face masks on board. J. Travel. Med. 2020, 27, 1–3. [Google Scholar] [CrossRef]
- Haneuse, S.; VanderWeele, T.; Arterburn, D. Using the E-value to assess the potentia effect of unmeasured confounding in observational studies. JAMA 2019, 321, 602–603. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Jimenez, J.L.; Prather, K.A.; Tufekci, Z.; Fisman, D.; Schooley, R. Ten scientific reasons in support of airborne transmission of SARS-CoV-2. Lancet 2021, 397, 1603–1605. [Google Scholar] [CrossRef] [PubMed]
- Prather, K.A.; Marr, L.C.; Schooley, R.T.; McDiarmid, M.A.; Wilson, M.E.; Milton, D.K. Airborne transmission of SARS-CoV-2. Science 2020, 370, 303–304. [Google Scholar] [CrossRef] [PubMed]
- Stadnytskyi, V.; Bax, C.E.; Bax, A.; Anfinrud, P. The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. Proc. Natl. Acad. Sci. USA 2020, 117, 11875–11877. [Google Scholar] [CrossRef] [PubMed]
- The National Academies of Sciences, Engineering and Medicine. Video 31-CQ1 Reflection and Syntheses: Airborne Transmission of SARS-CoV-2: A Virtual Workshop, 26 to 27 August 2020. Available online: https://www.nationalacademies.org/event/08-26-2020/airborne-transmission-of-sars-cov-2-a-virtual-workshop (accessed on 14 May 2021).
- AFAR; Which U.S. Airlines Are Still Blocking Middle Seats? Available online: https://www.afar.com/magazine/which-airlines-are-blocking-middle-seats (accessed on 14 May 2021).
- CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/travelers/testing-international-air-travelers.html (accessed on 14 May 2021).

{kind=link}
{kind=link}
{kind=link}
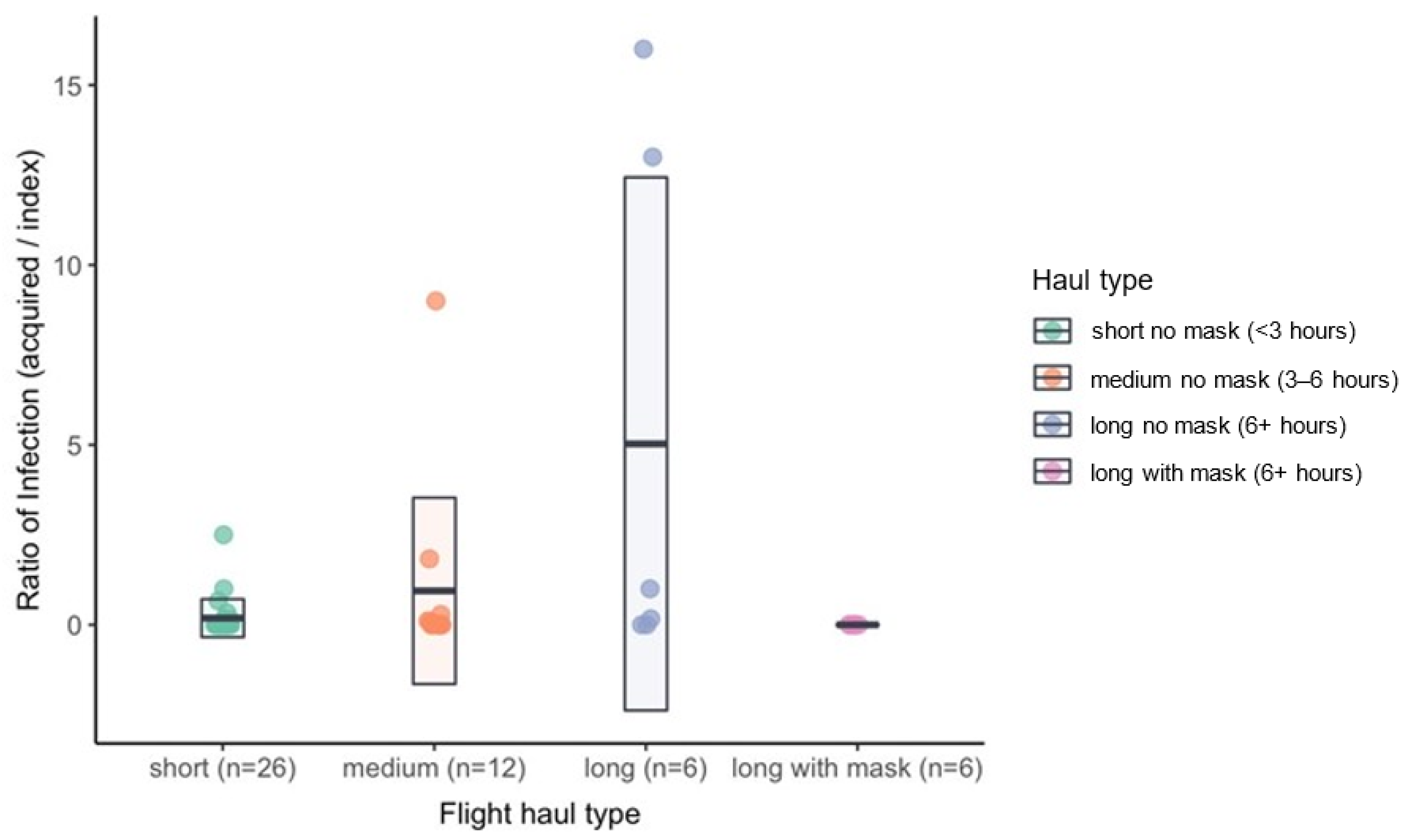
| Flight Haul Type | Number of Flights | Masking Mentioned on Flights | Enforced Masking |
|---|---|---|---|
| Short (<3 h) | 26 | 0 | 0 |
| Medium (3–6 h) | 12 | 0 | 0 |
| Long (>6 h) | 12 | 8 | 6 |
| Total flights | 50 | 8 | 6 |
| Flight Number | Approximate Flight Date | Flight Duration (h) | Index Cases (per Flight) | Aircraft-Acquired Cases (per Flight) | Masking |
|---|---|---|---|---|---|
| 1 | 24 February 2020 | 1.5 | 1 | 1 | Unenforced |
| 2 | 31 January 2020 to 3 December 2020 | 1.58 | 1 | 0 | Unenforced |
| 3 | 1.75 | 7 | 1 | Unenforced | |
| 4 | 1.83 | 2 | 0 | Unenforced | |
| 5 | 1.83 | 2 | 0 | Unenforced | |
| 6 | 1.83 | 2 | 0 | Unenforced | |
| 7 | 1.83 | 2 | 0 | Unenforced | |
| 8 | 1.83 | 9 | 0 | Unenforced | |
| 9 | 1.83 | 3 | 1 | Unenforced | |
| 10 | 2 | 3 | 0 | Unenforced | |
| 11 | 2 | 3 | 2 | Unenforced | |
| 12 | 2 | 6 | 1 | Unenforced | |
| 13 | 2 | 3 | 0 | Unenforced | |
| 14 | 2 | 5 | 0 | Unenforced | |
| 15 | 2 | 1 | 0 | Unenforced | |
| 16 | 2 | 1 | 0 | Unenforced | |
| 17 | 2 | 2 | 0 | Unenforced | |
| 18 | 4 | 2 | 0 | Unenforced | |
| 19 | 4.33 | 1 | 0 | Unenforced | |
| 20 | 27 February 2020 | 2 | 2 | 5 | Unenforced |
| 21 | 1 March 2020 | 2 | 1 | 0 | Unenforced |
| 22 | 3 March 2020 | 2 | 1 | 0 | Unenforced |
| 23 | 6 March 2020 | 2 | 1 | 0 | Unenforced |
| 24 | 22 February 2020 | 2.33 | 1 | 0 | Unenforced |
| 25 | 23 February 2020 | 2.33 | 1 | 0 | Unenforced |
| 26 | 26 February 2020 | 2.33 | 1 | 0 | Unenforced |
| 27 | 26 February 2020 | 2.42 | 2 | 0 | Unenforced |
| 28 | 28 February 2020 | 2.83 | 1 | 0 | Unenforced |
| 29 | 3 March 2020 | 3.5 | 1 | 0 | Unenforced |
| 30 | 4 March 2020 | 3.5 | 1 | 0 | Unenforced |
| 31 | 7 March 2020 | 3.5 | 1 | 0 | Unenforced |
| 32 | 8 March 2020 | 3.5 | 1 | 0 | Unenforced |
| 33 | 8 March 2020 | 3.5 | 2 | 0 | Unenforced |
| 34 | 1 March 2020 | 9.75 | 1 | 0 | Unenforced |
| 35 | 24 January 2020 | 4 | 9 | 1 | Unenforced |
| 36 | 9 March 2020 | 4.7 | 7 | 2 | Unenforced |
| 37 | 24 January 2020 | 4.8 | 12 | 1 | Reported |
| 38 | 24 January 2020 | 5 | 1 | 9 | Unenforced |
| 39 | 19 March 2020 | 5 | 6 | 11 | Unenforced |
| 40 | Summer-2020 | 7.5 | 1 (likely) | 13 | Unenforced |
| 41 | 2 March 2020 | 10 | 1 | 16 | Unenforced |
| 42 | 31 March to 1 April 2020 | 11 | 6 | 1 | Unenforced |
| 43 | 9 to 10 March 2020 | 15 | 2 | 2 | Unenforced |
| 44 | 22 January 2020 | 15 | 1 | 0 | Reported |
| 45 | 16 June 2020 | 8 | 6 | 0 | Mandatory, Enforced |
| 46 | 21 June 2020 | 8 | 29 | 0 | Mandatory, Enforced |
| 47 | 23 June 2020 | 8 | 16 | 0 | Mandatory, Enforced |
| 48 | 3 July 2020 | 8 | 9 | 0 | Mandatory, Enforced |
| 49 | 4 July 2020 | 8 | 7 | 0 | Mandatory, Enforced |
| 50 | 20 February 2020 | 13.5 | 2 | 0 | Mandatory, Enforced |
| Flight Number | Study Design | Observations |
|---|---|---|
| 1 | Case report (retrospective) | From Bangui to Yaounde [15] |
| 2 to 19 | Retrospective cohort study | From Innsbruck, Berlin, Milan, Turin, Verona, Tenerife, Basel, Geneva, and Istanbul to England. Of the aircraft-acquired COVID-19 cases, 4 passengers sat within 2 seats of the index case, and 1 sat 5 rows away of the index case. There were a total of 55 index cases among 18 flights, which led to 5 aircraft-acquired cases. Flights averaged 1–7 index cases [16]. |
| 20 to 34 | Retrospective | From Northern Italy, Israel, and the UK to Greece, as well as departures to and from Greece. On a flight from Israel to Athens (27 February 2020), 5 aircraft-acquired cases occurred in close contact with an index case (within 2 seats) and less than 2 m away for greater than 15 min. 1 case was a flight attendant, while 4 were passengers [17]. |
| 35 | Retrospective | From Malaysia to Hangzhou. 3 index cases were symptomatic, and 6 index cases were asymptomatic [18]. |
| 36 | Retrospective | From Tel Aviv, Israel to Frankfurt, Germany. The aircraft-acquired cases were seated within 2 rows of the index case [19]. |
| 37 | Retrospective | From Singapore to Hangzhou. The aircraft-acquired case was seated next to 4 infectious passengers. Meals were served. A total of 16 passengers tested positive after the flight, but not everyone who tested positive was interviewed [20]. |
| 38 | Retrospective | From Singapore to Hangzhou. There were 2 additional likely aircraft-acquired cases who the authors were unable to interview [21]. |
| 39 | Retrospective | From Sydney to Perth, Australia. For the aircraft-acquired cases, 8 passengers sat within 2 rows of the index cases, 2 passengers sat 3 rows away, and 1 was 6 rows away. Of the 11 aircraft-acquired cases, the authors categorized 8 as confirmed and 3 as probable [22]. |
| 40 | Retrospective | From 3 different continents (unspecified) into Ireland. Of the aircraft-acquired cases, 9 sat in a close contact range to the index case while 4 fell outside a close contact range (greater than 2 m). 9 out of 13 (69%) of the aircraft-acquired cases self-reported mask-wearing [23]. |
| 41 | Retrospective | From London to Hanoi. Of the aircraft-acquired cases, 13 were in business class with the index case, while 2 passengers and 1 flight attendant were in economy class. Among those in business class, 11 were within 2 m of index case (2 seats), while 1 was greater than 2 m away. Aircraft-acquired cases in economy class fell out of a close contact range to the index case [24]. |
| 42 | Prospective | From Milan, Italy to South Korea. An aircraft-acquired case was seated 3 rows away from an index case, and shared a bathroom with the index case. Index cases were asymptomatic [25]. |
| 43 | Retrospective | From Boston, Massachusetts to Hong Kong. 2 aircraft-acquired cases were flight attendants who served index cases [26]. |
| 44 | Letter, retrospective | From Wuhan, China to Guangzhou, China to Toronto, Canada. No transmission. The index case was mild [27]. |
| 45–49 | Review (prospective, retrospective) | From Dubai to Hong Kong. No transmission. All infected passengers originated from Pakistan. Emirates flights were known to be rigorous with their mask enforcement [10]. |
| 50 | Prospective | From Japan to Israel. No transmission. Passengers took off masks when eating meals, for ~15 min each time. There were 2 meals served on the flight. There were only 11 passengers on the flight [28]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, D.; Cheng, S.; Tsui, F.R.; Mathur, M.B.; Wang, C.-H.J. The Risk of Aircraft-Acquired SARS-CoV-2 Transmission during Commercial Flights: A Systematic Review. Int. J. Environ. Res. Public Health 2024, 21, 654. https://doi.org/10.3390/ijerph21060654
Zhao D, Cheng S, Tsui FR, Mathur MB, Wang C-HJ. The Risk of Aircraft-Acquired SARS-CoV-2 Transmission during Commercial Flights: A Systematic Review. International Journal of Environmental Research and Public Health. 2024; 21(6):654. https://doi.org/10.3390/ijerph21060654
Chicago/Turabian StyleZhao, Diana, Stephanie Cheng, Fuchiang R. Tsui, Maya B. Mathur, and Chih-Hung Jason Wang. 2024. "The Risk of Aircraft-Acquired SARS-CoV-2 Transmission during Commercial Flights: A Systematic Review" International Journal of Environmental Research and Public Health 21, no. 6: 654. https://doi.org/10.3390/ijerph21060654
APA StyleZhao, D., Cheng, S., Tsui, F. R., Mathur, M. B., & Wang, C.-H. J. (2024). The Risk of Aircraft-Acquired SARS-CoV-2 Transmission during Commercial Flights: A Systematic Review. International Journal of Environmental Research and Public Health, 21(6), 654. https://doi.org/10.3390/ijerph21060654