
Public Dental Service Access Policies for People with Autism Spectrum Disorder (ASD) in Salvador, Bahia, Brazil: A Pre-Evaluation Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
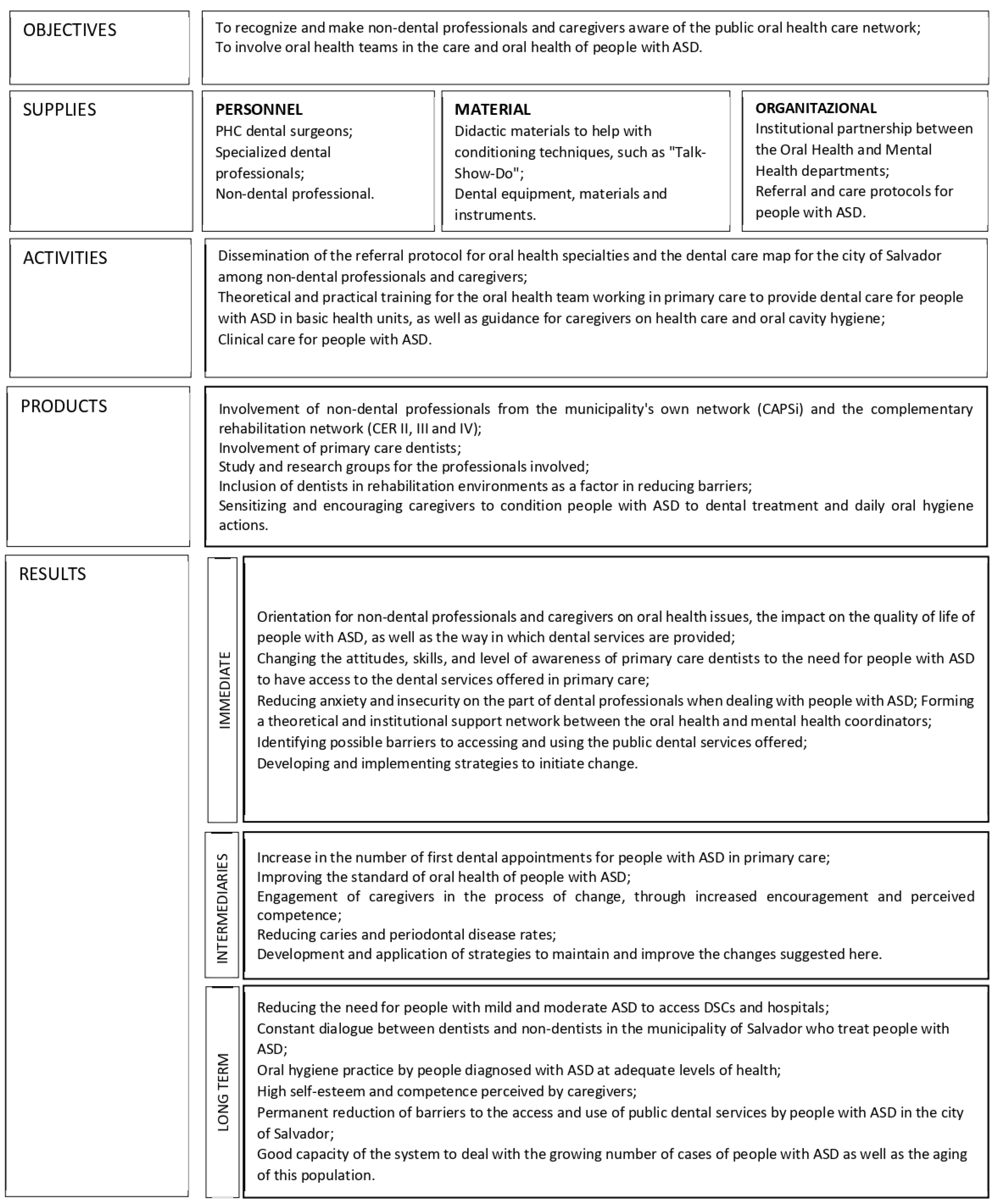
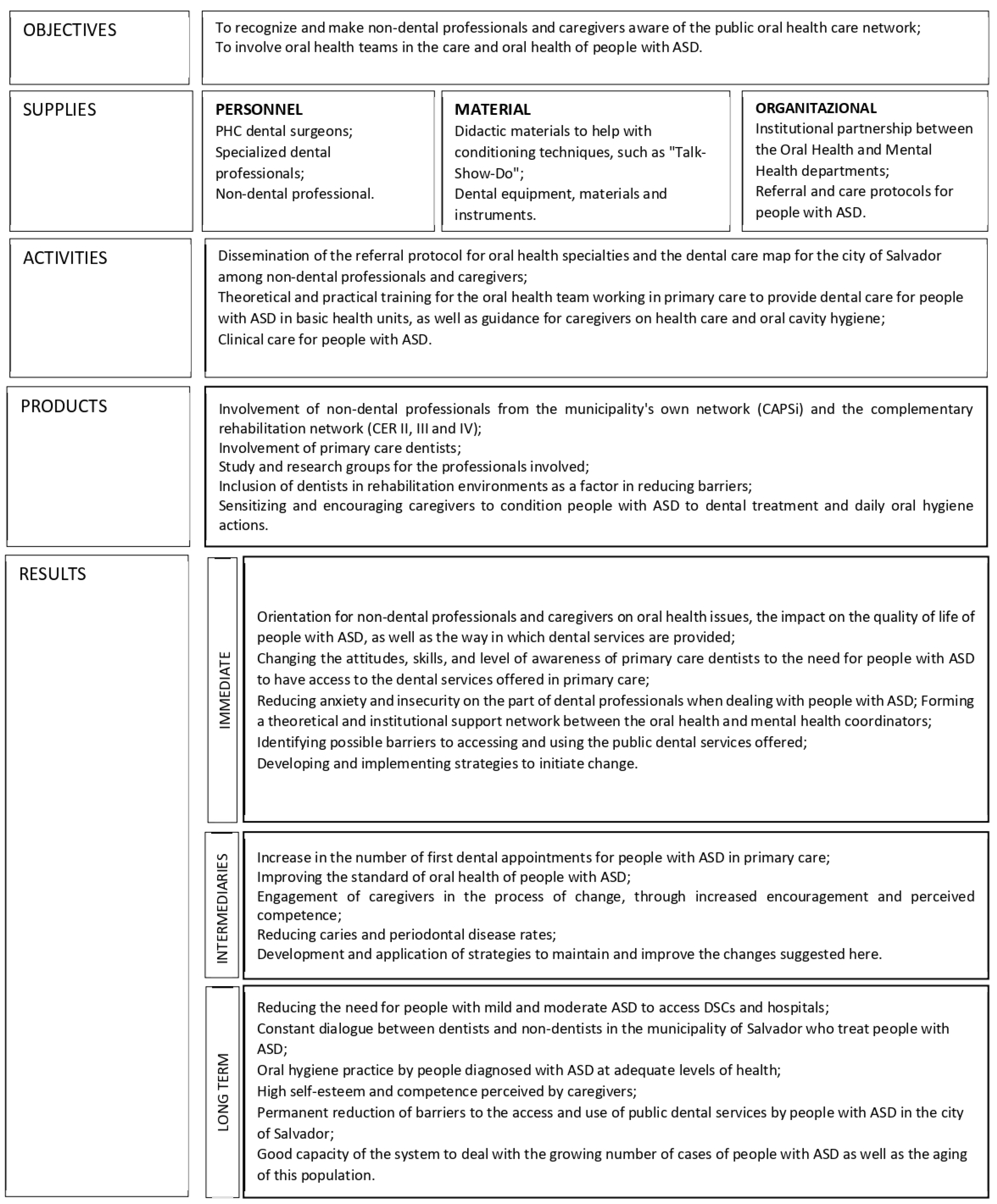
3.1. Modeling of the Policy
3.2. The Policies on Access to Dental Services for People with ASD: Clarifying Their Objectives
3.3. How the Policy Works in Practice
Flows, Protocols, and Continuing Education: Coordination Strategies
[…] There is no institutional flow between these coordinations. […] there is no direct relationship with oral health coordination […].(I1)
[…] The CEOs themselves contact the CAPS, looking for patients with a profile for NAPES, not just those with ASD since many users use the CAPS as a gateway instead of primary health care equipment.(I2)
[…] The functioning of the network is still fragile. Many things are achieved not through formal, institutional means but through personal contact […].(I5)
[…] During Activities of Daily Living (ADL), there should be time for oral hygiene education. […] A psychologist or occupational therapist cannot always carry out oral health education.(I7)
[…] the professional responsible for the care, when called upon […], goes to this PHC Unit to discuss the case with the professional from that health unit or accompany the user to be cared for, as they already have the link created with the CAPS professional.(I1)
There is no specific theme for the dental treatment of people with ASD. […] The strategy would be to have a dialog with the professionals at the CEOs so that they can point out the obstacles to conducting the process as a whole.(E2-SB coordinator)
There has not yet been any matrix support for people with ASD. […].(E3-DSC manager)
Concerning primary care, there has already been an opportunity for matrix support, but adherence is very low […](E4-CD NAPES)
[…] There are reports of family members preferring to wait for a time of urgency and emergency before taking action about oral health conditions, […](I1)
[…] There has been training for people with disabilities in general, not specifically for those with ASD. […].(I2)
[…] The person with ASD needs to be won over; a bond needs to be created between the professional and the autistic person. Health professionals often do not have time for this process. The demand from children who need dental treatment is very high.(I7)
[…] attention is paid to the time the person with the disorder is seen so that waiting times are kept to a minimum […] it is requested that harmony is maintained within the room, avoiding unnecessary movement in and out […]. We also try to keep the same professional assisting each patient so that a certain bond can be created.(I3)
[…] One positive thing we’ve achieved is the possibility of having a permanent assistant to care for people with ASD at NAPES, which helps a lot in forming a bond. […] What really stands out is the need for more structure for complex care.(I4)
The presence of a dentist in institutions that regularly care for people with ASD would enable work on oral health to be carried out […] the environment in which the person with ASD is already inserted would be a way of creating this bond and making care feasible. […] The dental office doesn’t play this role of social inclusion of the person with ASD.(I7)
[…] The user shouldn’t have to stay inside the facility to meet all their demands. […] There should be intersectorality and the capillarity of these people throughout the network, not considering what they can find outside the CAPS. […](I1)
[…] the movement made by mental health professionals is not to “isolate” people with disabilities. […] People with special needs need to circulate in other spaces. […](I5)
[…] The process of acceptance is slower and takes longer for some, which delays the movement towards oral health care as well […](I7)
[…] Some parents say they prefer not to be public with their children […]. Many families avoid taking people with ASD to the health center because they don’t believe they’ll find a qualified professional there.(I1)
[…] some parents don’t want their children to be seen by a professional who isn’t specialized. […] They already bring the demand for hospital-level care under general anesthesia. It turns out that many are surprised by their own children with ASD when they realize that the PHC dentist has managed to perform supervised brushing, for example […](I6)
[…] There is a great deal of ignorance about the dental service offered by the municipality to people with special needs through the CEOs since there is a great deal of complaining about the lack of vacancies by caregivers, while there are vacancies available in the network to be filled.(I3)
3.4. Relationship between Primary, Secondary, and Tertiary Care
[…] PHC still can’t see that people with disabilities live in that community, that they are part of that territory, which is a dynamic territory, and these people aren’t cared for.(I1)
[…] PHC plays a fundamental role in caring for people with ASD, mainly because of the bond created with the family. In addition, the specialist at the CEO needs more time to create this affinity. […](I2)
[…] The health center refers them to the CEO. At the CEO, there are already difficulties in providing care… The delay in referrals from the CEO to the hospitals is even longer.(I7)
Unfortunately, hospital care for patients referred by this center is not working. Patients find it very difficult, even before the pandemic. […](I4)
[…] The town hall has created an agreement with a hospital in the city that receives patients referred directly from PHC in an attempt to reduce the referral time between services. […] the city’s Emergency Care Units have the so-called “Red Room”, with all the technical equipment to carry out conscious sedation, and it is suggested that, if necessary, this procedure be carried out in these municipal facilities.(I2)
The person with special needs is referred via the Referral and Counter-Referral Form. Due to a lack of information, the CEO receives several referrals indicating sedation. So, the user (or their guardian) is instructed at the CEO’s reception desk to present this same form to the hospitals that perform this type of procedure.(I3)
[…] Every referral made by the Referral Form must have a counter-referral from the professional looking after this person […]. Sometimes, telephone and informal contact between services, beyond any form, for example, is potent. […] This is an “implicated” referral when the patient’s origin and destination are directly connected, from professional to professional, from service to service.(I1)
[…] there needs to be more understanding about what a person with special needs is. Hypertensive patients, people with diabetes, and pregnant women are sometimes mistakenly classified as people with special needs. As a result, the CEO does not accept some referrals because the person doesn’t fit the NAPES prerequisites.(I3)
There are various programs and thematic fields that the professionals at the town hall have to carry out. None are specific to people with ASD. Perhaps they include people with disabilities! But autistic people are not disabled people! I think this is a necessary and urgent discussion […].(E6-CD USF)
3.5. Provision of and Access to Dental Services by People with ASD: Results of a Pilot Study
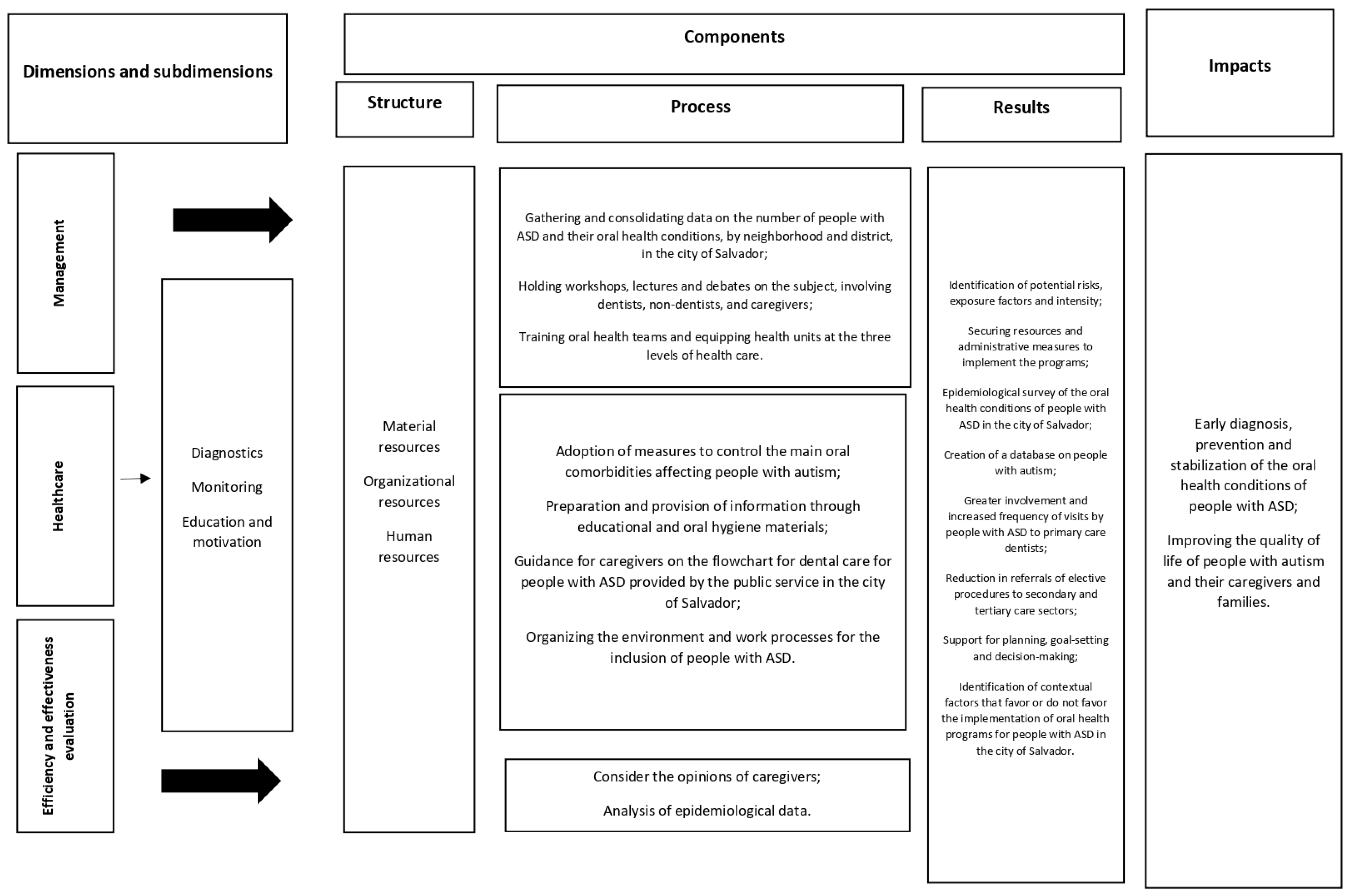
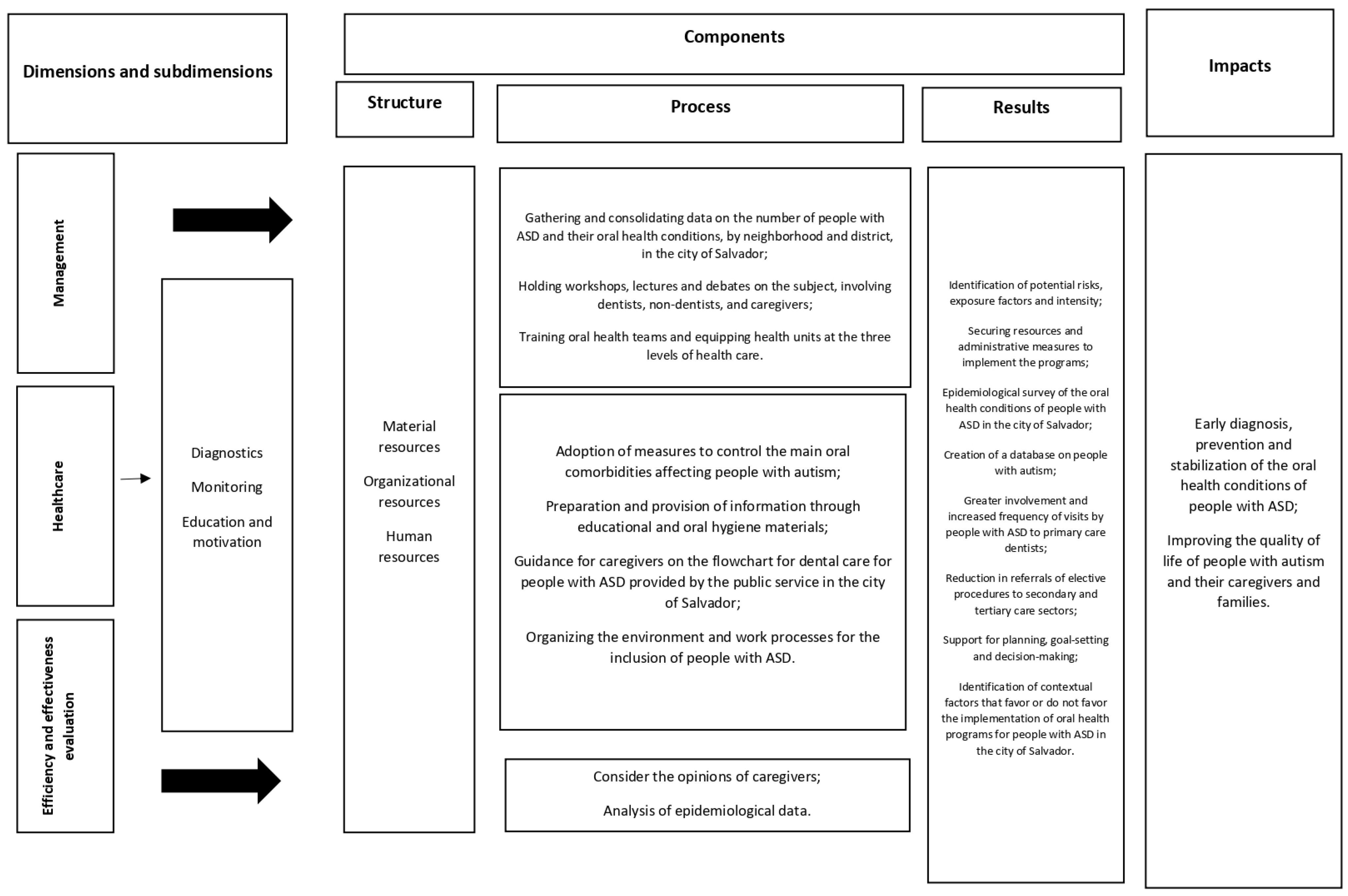
3.6. Ways of Overcoming Weakness and Dimensions and Subdimensions for Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- da Silva, S.N.; Gimenez, T.; Souza, R.C.; Mello-Moura, A.C.V.; Raggio, D.P.; Morimoto, S.; Tedesco, T.K. Oral health status of children and young adults with autism spectrum disorders: Systematic review and meta-analysis. Int. J. Paediatr. Dent. 2017, 27, 388–398. [Google Scholar] [CrossRef] [PubMed]
- De Mattei, R.; Cuvo, A.; Maurizio, S. Oral assessment of children with an autism spectrum disorder. J. Dent. Hyg. 2007, 81, 65. [Google Scholar] [PubMed]
- Jaber, M.A. Dental caries experience, oral health status and treatment needs of dental patients with autism. J. Appl. Oral Sci. 2011, 19, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Du, R.Y.; Yiu, C.C.Y.; Wong, V.C.N.; McGrath, C.P. Autism Developmental Profiles and Cooperation with Oral Health Screening. J. Autism. Dev. Disord. 2015, 45, 2758–2763. [Google Scholar] [CrossRef]
- Loo, C.Y.; Graham, R.M.; Hughes, C.V. Behaviour guidance in dental treatment of patients with autism spectrum disorder. Int. J. Paediatr. Dent. 2009, 19, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Stein, L.I.; Polido, J.C.; Mailloux, Z.; Coleman, G.G.; Cermak, S.A. Oral care and sensory sensitivities in children with autism spectrum disorders. Spec. Care Dentist. 2011, 31, 102–110. [Google Scholar] [CrossRef] [PubMed]
- OPAS/OMSBRASIL. Folha Informativa—Transtorno do Espectro Autista. 2017. Available online: https://www.paho.org/pt/topicos/transtorno-do-espectro-autista (accessed on 8 January 2019).
- Amaral, L.D.; Portillo, J.S.C.; Mendes, S.C.T. Estratégias de acolhimento e condicionamento do paciente autista na Saúde Bucal Coletiva. Rev. Tempus—Actas Saúde Coletiva Brasília 2011, 5, 105–114. [Google Scholar]
- Campos, C.C.; Sabbagh-Haddad, A. Transtornos de comportamento e tratamento odontológico. In Odontologia para Pacientes com Necessidades Especiais; Sabbagh-Haddad, A., Ed.; Santos: São Paulo, Brazil, 2007. [Google Scholar]
- Orellana, L.M.; Martínez-Sanchis, S.; Silvestre, F.J. Training Adults and Children with an Autism Spectrum Disorder to be Compliant with a Clinical Dental Assessment Using a TEACCH-Based Approach. J. Autism Dev. Disord. 2014, 44, 776–785. [Google Scholar] [CrossRef]
- Nelson, T.M.; Sheller, B.; Friedman, C.S.; Bernier, R. Educational and therapeutic behavioral approaches to providing dental care for patients with Autism Spectrum Disorder. Spec. Care Dentist. 2015, 35, 105–113. [Google Scholar] [CrossRef]
- Mcdonald, R.E.; Avery, D.R. Odontopediatria; Guanabara Koogan: Rio de Janeiro, Brazil, 2001. [Google Scholar]
- Ganz, J.B.; Davis, J.L.; Lund, E.M.; Goodwyn, F.D.; Simpson, R.L. Meta-analysis of PECS with individuals with ASD: Investigation of targeted versus non-targeted outcomes, participant characteristics, and implementation phase. Res. Dev. Disabil. 2012, 33, 406–418. [Google Scholar] [CrossRef]
- Ministério da Saúde. Diretrizes da Política Nacional de Saúde Bucal; Ministério da Saúde: Brasília, Brazil, 2004.
- Ministério da Saúde; Secretaria de Atenção à Saúde; Departamento de Atenção Especializada e Temática. Linha de Cuidado para a Atenção às Pessoas com Transtornos do Espectro do Autismo e suas Famílias na Rede de Atenção Psicossocial do Sistema Único de Saúde; Ministério da Saúde: Brasília, Brazil, 2015.
- Oliveira, R.F.R.; Souza, J.G.S.; Haikal, D.S.; Ferreira, E.F.; Martins, A.M.E.B.L. Equity in the use of dental services provided by the Brazilian Unified Health System (SUS) among the elderly: A population-based study. Ciênc Saúde Colet. 2016, 21, 3509–3523. [Google Scholar] [CrossRef]
- Rossi, P.H.; Freeman, H.E. Evaluation, a Systematic Approach; Sage Publications: Beverly Hills, CA, USA, 2004. [Google Scholar]
- Brousselle, A.; Champagne, F.; Contandriopoulos, A.P.; Hartz, Z. Análise de Implantação. In Avaliação Conceitos e Métodos; Broussele, A., Champagne, F., Contandriopoulos, A.P., Hartz, Z., Eds.; FIOCRUZ: Rio de Janeiro, Brazil, 2011; pp. 217–240. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Ministério da Saúde; Secretaria de Atenção à Saúde; Departamento de Ações Programáticas Estratégicas. Diretrizes de Atenção à Reabilitação da Pessoa com Transtornos do Espectro do Autismo (TEA); Ministério da Saúde: Brasília, Brazil, 2014.
- Donabedian, A. Evaluating the quality of medical care. Milbank Q. 2005, 83, 691–729. [Google Scholar] [CrossRef]
- Araujo Jeane, A.M.R.; Veras André, B.; Varella André, A.B. Breves considerações sobre a atenção à pessoa com transtorno do espectro autista na rede pública de saúde. Rev. Psicol. E Saúde 2019, 11, 89–98. [Google Scholar] [CrossRef]
- Gandhi, R.P.; Klein, U. Autism Spectrum Disorders: An update on oral health management. J. Evid.-Based Dent. Pract. Spec. 2014, 14, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Delli, K.; Reichart, P.A.; Bornstein, M.; Livas, C. Management of children with autism spectrum disorder in the dental setting: Concerns, behavioural approaches and Recommendations. Med. Oral Patol. Oral Cir. Bucal. 2013, 18, e862–e868. [Google Scholar] [CrossRef] [PubMed]
- Levy, S.E.; Mandell, D.S.; Schultz, R.T. Autism. Lancet 2009, 374, 1627–1638. [Google Scholar] [CrossRef]
- Pimentel Júnior, N.S.; de Barros, S.G.; de Jesus Filho, E.; Vianna, M.I.P.; Santos, C.M.L.; Cangussu, M.C.T. Oral health-care practices and dental assistance management strategies for people with autism spectrum disorder: An integrative literature review. Autism 2024, 28, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Onol, S.; Kırzıoğlu, Z. Evaluation of oral health status and influential factors in children with autism. Niger. J. Clin. Pract. 2018, 21, 429–435. [Google Scholar] [CrossRef]
- Curi, D.S.C.; Figueiredo, A.C.L.; Jamelli, S.L. Fatores associados à utilização dos serviços de saúde bucal pela população pediátrica: Uma revisão integrativa. Ciência Saúde Coletiva 2018, 23, 1561–1576. [Google Scholar] [CrossRef]
- Andersen, R.M.; Newman, J.F. Societal and individual determinants of medical care utilization in the United States. Milbank Meml. Fund Q. Health Soc. 1973, 51, 95–124. [Google Scholar] [CrossRef]
- The Canadian Academy of Health Sciences (CAHS). Improving Access to Oral Health Care for Vulnerable People Living in Canada; CAHS: Ottawa, ON, Canada, 2005.
- Institute of Medicine and National Research Council (IMNRC). Improving Access to Oral Health Care for Vulnerable and Underserved Populations; IMNRC: Washington, DC, USA, 2011.
- Solano, M.P.; Bulgarelli, P.T.; Dos Santos, C.M.; Mestriner, S.F.; Mestriner, W., Jr.; de Mesquita Lago, L.P.; Bulgarelli, A.F. Utilização de serviços de saúde bucal na atenção primária: Perspectivas dos usuários do SUS de um município do sul do Brasil. Rev. Ciência Plural. 2017, 3, 81–92. [Google Scholar] [CrossRef]
- Lemos, E.L.D.M.D.; Salomão, N.M.R. Jovens com transtorno autista, suas mães e irmãos: Vivências familiares e modelo bioecológico. Psicol. Teor. Pesqui. 2022, 38, e38312. [Google Scholar] [CrossRef]
- American Academy of Pediatric Dentistry. Reference Manual 2010–2011; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2010. [Google Scholar]
- OMS. 67ª Assembléia Mundial da Saúde; OMS: Gêneva, Suiça, 2014. [Google Scholar]
- Pitombeira, D.F.; Oliveira, L.C. Pobreza e desigualdades sociais: Tensões entre direitos, austeridade e suas implicações na atenção primária. Ciênc. Saúde Colet. 2020, 25, 1699–1708. [Google Scholar] [CrossRef] [PubMed]
- Garbois, J.A.; Sodre, F.; Dalbello-Araujo, M. From the notion of social determination to one of social determinants of health. Saúde Debate 2017, 41, 63–76. [Google Scholar] [CrossRef]
- Almeida, E.R.; Sousa, A.N.A.; Brandão, C.C.; Carvalho, F.F.B.; Tavares, G.; Silva, K.C. Política Nacional de Atenção Básica no Brasil: Uma análise do processo de revisão (2015–2017). Rev. Panam. Salud Publ. 2018, 42, 1–8. [Google Scholar] [CrossRef]
- Ministério da Saúde. Cadernos de Atenção Básica, Nº 17; Ministério da Saúde: Brasília, Brazil, 2008.
- Ministério da Saúde; Secretaria de Atenção à Saúde; Departamento de Atenção Básica. Política Nacional de Atenção Básica; Ministério da Saúde: Brasília, Brazil, 2012.
- Damasceno, K.S.M.; Cruz, D.N.; Barros, S.G. Acessibilidade aos serviços odontológicos no SUS: Revisão da literatura. Res. Soc. Dev. 2021, 10, e17610313194. [Google Scholar] [CrossRef]
- Telleen, S.; Rhee Kim, Y.O.; Chavez, N.; Barrett, R.E.; Hall, W.; Gajendra, S. Access to oral health services for urban low-income Latino children: Social ecological influences. J. Public Health Dent. 2012, 72, 8–18. [Google Scholar] [CrossRef]
- Mohinderpal Chadha, G.; Kakodkar, P.; Chaugule, V.; Nimbalkar, V. Dental survey of institutionalized children with autistic disorder. Int. J. Clin. Pediatr. Dent. 2012, 5, 29–32. [Google Scholar]
- Campos, C.D.C.; Frazão, B.B.; Saddi, G.L.; Morais, L.A.; Ferreira, M.G.; Setúbal, P.C.O.; Alcântara, R.T. Manual Prático para o Atendimento Odontológico dos Pacientes com Necessidades Especiais. 2009. Available online: https://cvtpcd.odonto.ufg.br/n/95746-manual-pratico-para-o-atendimento-odontologico-de-pacientes-com-necessidades-especiais (accessed on 23 April 2024).
- Kuhaneck, H.M.; Chisholm, E.C. Improving dental visits for individuals with autism spectrum disorders through an understanding of sensory processing. Spec. Care Dent. 2012, 32, 229–233. [Google Scholar] [CrossRef]
- Zink, A.G.; Diniz, M.B.; Rodrigues Dos Santos, M.T.; Guare, R.O. Use of a Picture Exchange Communication System for preventive procedures in individuals with autism spectrum disorder: Pilot study. Spec. Care Dent. 2016, 36, 254–259. [Google Scholar] [CrossRef]
- Zink, A.G.; Baeder, F.; Pinho, M.Z.; Pinho, M.D.; Fonseca, M.E. Materiais estruturados para instrução de higiene bucal de pessoas com autismo. Rev. Assoc. Paul. Cir. Dent. 2019, 73, 215–220. [Google Scholar]
- Marshall, J.; Sheller, B.; Williams, B.J.; Mancl, L.; Cowan, C. Cooperation predictors for dental patients with autism. Pediatr. Dent. 2007, 29, 369–376. [Google Scholar]
- Zink, A.G.; De Pinho, M.D. Atendimento odontológico do paciente autista—Relato de caso. Rev. ABO Nac. 2008, 16, 313–316. [Google Scholar]
- Marcato, D.; de Lima, T.G. Da Formação Inicial À Carreira Docente: Alternativas Para Superação Dos Desafios Encontrados Por Professores Iniciantes. Rev. Diálogos Interdiscip. 2022, 1, 159–178. [Google Scholar] [CrossRef]
- Chhabra, N.; Chhabra, A. Parental knowledge, attitudes and cultural beliefs regarding oral health and dental care of preschool children in an Indian population: A quantitative study. Eur. Arch. Paediatr. Dent. 2012, 13, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Ferrazzano, G.F.; Salerno, C. Autism spectrum disorders and oral health status: Review of the literature. Eur. J. Paediatr. Dent. 2020, 21, 9–12. [Google Scholar] [PubMed]
- Paim, J.; Travassos, C.; Almeida, C.; Bahia, L.; Macinko, J. The Brazilian health system: History, advances, and challenges. Lancet 2011, 377, 1778–1797. [Google Scholar] [CrossRef] [PubMed]
- Gomes, P.T.; Lima, L.H.; Bueno, M.K.; Araujo, L.A.; Souza, N.M. Autism in Brazil: A systematic review of family challenges and coping strategies. J. Pediatr. 2015, 91, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Andrade, A.P.P.; Eleutéio, A.S.L. Pacientes portadores de necessidades especiais: Abordagem odontológica e anestesia geral. Rev. Bras. Odontol. 2015, 72, 66–69. [Google Scholar] [CrossRef]
- Barry, S.; O’Sullivan, E.A.; Toumba, K.J. Barriers to dental care for children with autism spectrum disorder. Eur. Arch. Paediatr. Dent. 2014, 15, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Brickhouse, T.H.; Farrington, F.H.; Best, A.M.; Ellsworth, C.W. Barriers to Dental Care for Children in Virginia With Autism Spectrum Disorders. J. Dent. Child. 2009, 76, 188–193. [Google Scholar]
- Lai, B.; Milano, M.; Roberts, M.; Hooper, S. Unmet dental needs and barriers to dental care among children with autism spectrum disorders. J. Autism. Dev. Disord. 2012, 42, 1294–1303. [Google Scholar] [CrossRef] [PubMed]
- Chaves, S.C.L.; Soares, F.F.; Rossi, T.R.A.; Cangussu, M.C.T.; Figueiredo , A.C.L.; Cruz, D.N.; Cury, P.R. Características do acesso e utilização de serviços odontológicos em municípios de médio porte. Ciência Saúde Colet. 2012, 17, 3115–3124. [Google Scholar] [CrossRef]
- Melo, A.C.; Braga, C.C.; Forte, F.D. Acessibilidade ao Serviço de Saúde Bucal na Atenção Básica: Desvelando o Absenteísmo em uma Unidade de Saúde da Família de João Pessoa–PB. Rev. Bras. Ciências Saúde 2011, 15, 309–318. [Google Scholar] [CrossRef]
- Cunha, A.B.O.; Vieira-Da-Silva, L.M. Acessibilidade aos serviços de saúde em um município do Estado da Bahia, Brasil, em gestão plena do sistema. Cad. Saúde Pública 2010, 26, 725–737. [Google Scholar] [CrossRef] [PubMed]
- Andrade, R.T.S.; Silva, U.A. O acesso dos trabalhadores aos serviços odontológicos na rede SUS: Uma reflexão crítica. Rev. Bras. Pesq. Em Saúde 2010, 12, 45–51. [Google Scholar]
- Souza, E.C.F.; Vilar, R.L.A.; Rocha, N.S.P.D.; Uchoa, A.C.; Rocha, P.M. Acesso e acolhimento na atenção básica: Uma análise da percepção dos usuários e profissionais de saúde. Cad. Saúde Pública 2008, 24 (Suppl. S1), S100–S110. [Google Scholar] [CrossRef] [PubMed]
- Reis, W.G.; Scherer, M.D.D.A.; Carcereri, D.L. O trabalho do Cirurgião-Dentista na Atenção Primária à Saúde: Entre o prescrito e o real. Saúde Em Debate 2015, 39, 56–64. [Google Scholar] [CrossRef]
- Scherer, M.D.D.A.; Pires, D.; Schwartz, Y. Trabalho coletivo: Um desafio para a gestão em saúde. Rev. Saude Publ. 2009, 43, 721–725. [Google Scholar] [CrossRef]
- Rocha-Buelvas, A. Análisis sobre el acceso a los servicios de la salud bucal: Um indicador de equidad. Rev. Gerenc. Políticas Salud 2013, 12, 96–112. [Google Scholar]
- Ministério da Saúde; Gabinete do Ministro. Portaria no 399/GM, de 22 de Fevereiro de 2006. Divulga o Pacto pela Saúde 2006-Consolidação do SUS e Aprova as Diretrizes Operacionais do Referido Pacto; Diário Oficial da União 23 Fev 2006; Ministério da Saúde: Brasília, Brazil, 2006.
- Pessanha, R.V.; Cunha, F.T.S. A aprendizagem-trabalho e as tecnologias de saúde na Estratégia Saúde da Família. Texto Contexto 2009, 18, 233–240. [Google Scholar] [CrossRef]
- Nicoletti, M.A.; Honda, F.R. Transtorno do Espectro Autista: Uma abordagem sobre as políticas públicas e o acesso à sociedade. Infarma-Ciências Farm. 2021, 33, 117–130. [Google Scholar] [CrossRef]
- de Souza Correa, K.; Barbosa, R.R.B.; Oliveira, F.R. Particularidades, Indivíduo e Transtorno do Espectro Autista: Um Estudo de Caso com Base na Terapia Cognitivo comportamental; TCC (Graduação)—Curso de Psicologia; Unifucamp—Centro Universitário Mário Palmério: Brasília, Brazil, 2021. [Google Scholar]
- Du, R.Y.; Yiu, C.K.Y.; King, N.M. Oral Health Behaviours of Preschool Children with Autism Spectrum Disorders and Their Barriers to Dental Care. J. Autism Dev. Disord. 2019, 49, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Khrautieo, T.; Srimaneekarn, N.; Rirattanapong, P.; Smutkeeree, A. Association of sensory sensitivities and toothbrushing cooperation in autism spectrum disorder. Int. J. Paediatr Dent. 2020, 30, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Lam, P.P.; Du, R.; Peng, S.; McGrath, C.P.; Yiu, C.K. Oral health status of children and adolescents with autism spectrum disorder: A systematic review of case-control studies and meta-analysis. Autism 2020, 24, 1047–1066. [Google Scholar] [CrossRef] [PubMed]
- Robertson, M.D.; Schwendicke, F.; de Araújo, M.P.; Radford, J.R.; Harris, J.C.; McGregor, S.; Innes, N.P.T. Dental caries experience, care index and restorative index in children with learning disabilities and children without learning disabilities; a systematic review and meta-analysis. BMC Oral Health 2019, 19, 146. [Google Scholar] [CrossRef]
- Stein Duker, L.I.; Floríndez, L.I.; Como, D.H.; Tran, C.F.; Henwood, B.F.; Polido, J.C.; Cermak, S.A. Strategies for Success: A Qualitative Study of Caregiver and Dentist Approaches to Improving Oral Care for Children with Autism. Pediatr. Dent. 2019, 41, 4E–12E. [Google Scholar]

{kind=link}
{kind=link}
| N | Document Title | Publication Year | Source |
|---|---|---|---|
| D1 | The Brazilian Federal Constitution | 1988 | Brazilian Federal Government |
| D2 | The Child and Adolescent Statute | 1990 | Brazilian Federal Government |
| D3 | National Oral Health Policy | 2004 | Brazilian Federal Government |
| D4 | Convention on the Rights of Persons with Disabilities | 2006 | United Nations (UN) |
| D5 | National Plan for People with Disabilities–Living without Limits | 2011 | Brazilian Federal Government |
| D6 | Care Network for People with Disabilities | 2012 | Brazilian Federal Government |
| D7 | National Policy for the Protection of the Rights of People with Autism Spectrum Disorders (Berenice Piana Law) | 2012 | Brazilian Federal Government |
| D8 | Guidelines for the Rehabilitation of People with Autism Spectrum Disorders (ASD) | 2014 | Brazilian Federal Government |
| D9 | Care Pathway for People with Autism Spectrum Disorders and their Families in the Psychosocial Care Network of the Unified Health System | 2016 | Brazilian Federal Government |
| D10 | Referral Protocol for Oral Health Specialties in Salvador | 2017 | Salvador City Hall |
| D11 | Oral Health in the Unified Health System | 2018 | Brazilian Federal Government |
| D12 | Guide to Oral Health Care for People with Disabilities 2019 | 2019 | Brazilian Federal Government |
| D13 | The Municipal Health Plan 2018–2021 | 2018 | Salvador City Hall |
| N | Interviewees |
|---|---|
| I1 | Representative of the Coordination of Care for People with Disabilities of the Municipal Health Secretariat of the City of Salvador |
| I2 | Representative of the technical area of Oral Health of the Municipal Health Secretariat of the city of Salvador |
| I3 | Dental Specialty Center Manager |
| I4 | Dental surgeon at the Center for Attention to People with Disabilities |
| I5 | District dentist |
| I6 | Dentist working in the Family Health Strategy |
| I7 | Caregiver of a person with ASD |
| Variables | n | % |
|---|---|---|
| Has the person with ASD ever been to the dentist? | ||
| Yes | 50 | 72.46 |
| No | 18 | 26.09 |
| Didn’t know | 1 | 1.45 |
| Has the person with ASD been to the dentist in the last year? | ||
| Yes | 30 | 42.86 |
| No | 40 | 57.14 |
| Does the person responsible for the person with ASD know of a place for dental care for ASD through the SUS? | ||
| Yes | 22 | 31.88 |
| No | 45 | 65.22 |
| Didn’t know | 2 | 2.90 |
| Does the person with ASD find dental care difficult? | ||
| Yes | 47 | 69.12 |
| No | 14 | 20.59 |
| Didn’t know | 7 | 10.29 |
| What kind of difficulties do people with ASD have in accessing dental treatment? | ||
| Can’t get an appointment | 29 | 52.73 |
| The service location is far from home | 5 | 9.09 |
| Difficulty obtaining referral forms | 8 | 14.55 |
| More than one situation | 11 | 20.00 |
| Never looked for or had no difficulties | 2 | 3.64 |
| Has the person responsible for the person with ASD received oral hygiene advice? | ||
| Yes | 54 | 81.82 |
| No | 11 | 16.67 |
| Didn’t know | 1 | 1.52 |
| Variables | n | % |
|---|---|---|
| Place of research | ||
| CAPSi 1 | 11 | 45.83 |
| CAPSi 2 | 13 | 54.17 |
| Is there an oral health program in the institution? | ||
| Yes | 1 | 4.17 |
| No | 22 | 91.67 |
| Didn’t know | 1 | 4.17 |
| Is oral hygiene practiced in the institution? | ||
| Yes | 2 | 8.33 |
| No | 20 | 83.33 |
| Didn’t know | 2 | 8.33 |
| Does the institution receive material for oral hygiene practice? | ||
| Yes | 6 | 25.00 |
| No | 15 | 62.50 |
| Didn’t know | 3 | 12.25 |
| Is there a place in the institution for practicing oral hygiene? | ||
| Yes | 3 | 12.50 |
| No | 20 | 83.33 |
| Didn’t know | 1 | 4.17 |
| Does the institution distribute oral hygiene materials? | ||
| Yes | 1 | 4.17 |
| No | 21 | 87.50 |
| Didn’t know | 2 | 8.33 |
| Do people with ASD and their guardians receive oral hygiene advice? | ||
| Yes | 3 | 12.50 |
| No | 20 | 83.33 |
| Didn’t know | 1 | 4.17 |
| Does the institution receive visits from dental professionals? | ||
| Yes | 5 | 20.83 |
| No | 17 | 70.83 |
| Didn’t know | 2 | 8.33 |
| If yes, how often? | ||
| Annually | 2 | 66.67 |
| On request | 1 | 33.3 |
| Does the institution receive visits from dental schools? | ||
| Yes | 2 | 8.70 |
| No | 19 | 82.61 |
| Didn’t know/Didn’t answer | 3 | 12.50 |
| Do you know the Municipal Health Secretariat flowchart for dental care for people with ASD? | ||
| Yes | 2 | 8.33 |
| No | 22 | 91.67 |
| Do you know the State Health Secretariat flowchart for dental care for people with ASD? | ||
| No | 24 | 100.00 |
| Do people with ASD in your institution receive dental treatment somewhere? | ||
| Yes | 4 | 16.67 |
| No | 4 | 16.67 |
| Didn’t know | 16 | 66.67 |
| If the patient needs dental care, does the institution refer them for treatment? | ||
| Yes | 16 | 66.67 |
| No | 4 | 16.67 |
| Didn’t know | 4 | 16.67 |
| Which dental treatment facility does the institution refer you to when you need dental care? | ||
| Hospital | 2 | 8.33 |
| Health Center | 16 | 66.67 |
| University | 1 | 4.17 |
| Didn’t know | 5 | 20.83 |
| Should dental treatment for people with ASD happen in the same environment as people without ASD? | ||
| Yes | 19 | 79.17 |
| No | 2 | 8.33 |
| Didn’t know | 3 | 12.50 |
| Variables | n | % |
|---|---|---|
| Differentiated attention for people with ASD about other patients with special needs | ||
| Yes | 5 | 35.71 |
| No | 8 | 57.14 |
| Didn’t know | 1 | 7.14 |
| Differentiated appointment for people with ASD | ||
| Yes | 5 | 35.71 |
| No | 8 | 57.14 |
| Didn’t know | 1 | 7.14 |
| Specific training in caring for people with ASD | ||
| Yes | 5 | 35.71 |
| No | 8 | 57.14 |
| Didn’t know | 1 | 7.14 |
| Places reserved for people with ASD | ||
| Yes | 1 | 7.14 |
| No | 13 | 92.86 |
| Oral health program for people with ASD | ||
| Yes | 1 | 7.14 |
| No | 12 | 85.71 |
| Didn’t know | 1 | 7.14 |
| Qualified to use Nitrous Oxide | ||
| Yes | 4 | 28.57 |
| No | 10 | 71.43 |
| A surgical center available where people with ASD are treated | ||
| Yes | 3 | 21.43 |
| No | 11 | 78.57 |
| Time to First Appointment for Person with ASD | ||
| Up to 01 week | 6 | 46.15 |
| Between 15 and 30 days | 2 | 15.38 |
| More than 30 days | 1 | 7.69 |
| Didn’t know | 4 | 30.77 |
| Guidance on oral health for those responsible for people with ASD | ||
| Yes | 14 | 100.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jesus-Filho, E.d.; Barros, S.G.d.; Vianna, M.I.P.; Cangussu, M.C.T. Public Dental Service Access Policies for People with Autism Spectrum Disorder (ASD) in Salvador, Bahia, Brazil: A Pre-Evaluation Study. Int. J. Environ. Res. Public Health 2024, 21, 555. https://doi.org/10.3390/ijerph21050555
Jesus-Filho Ed, Barros SGd, Vianna MIP, Cangussu MCT. Public Dental Service Access Policies for People with Autism Spectrum Disorder (ASD) in Salvador, Bahia, Brazil: A Pre-Evaluation Study. International Journal of Environmental Research and Public Health. 2024; 21(5):555. https://doi.org/10.3390/ijerph21050555
Chicago/Turabian StyleJesus-Filho, Ednaldo de, Sandra Garrido de Barros, Maria Isabel Pereira Vianna, and Maria Cristina Teixeira Cangussu. 2024. "Public Dental Service Access Policies for People with Autism Spectrum Disorder (ASD) in Salvador, Bahia, Brazil: A Pre-Evaluation Study" International Journal of Environmental Research and Public Health 21, no. 5: 555. https://doi.org/10.3390/ijerph21050555
APA StyleJesus-Filho, E. d., Barros, S. G. d., Vianna, M. I. P., & Cangussu, M. C. T. (2024). Public Dental Service Access Policies for People with Autism Spectrum Disorder (ASD) in Salvador, Bahia, Brazil: A Pre-Evaluation Study. International Journal of Environmental Research and Public Health, 21(5), 555. https://doi.org/10.3390/ijerph21050555