

Sexist, Racist, and Homophobic Violence against Paramedics in a Single Canadian Site

 ,
,  ,
,  and
and
Abstract
1. Introduction
1.1. Violence against Paramedics
1.2. Under-Reporting
1.3. Non-Physical Violence
1.4. The External Violence Incident Report
2. Methods
2.1. Overview and Setting
2.2. Data Collection
2.3. Measures and Outcomes
2.4. Analysis
3. Results
3.1. Note to Readers
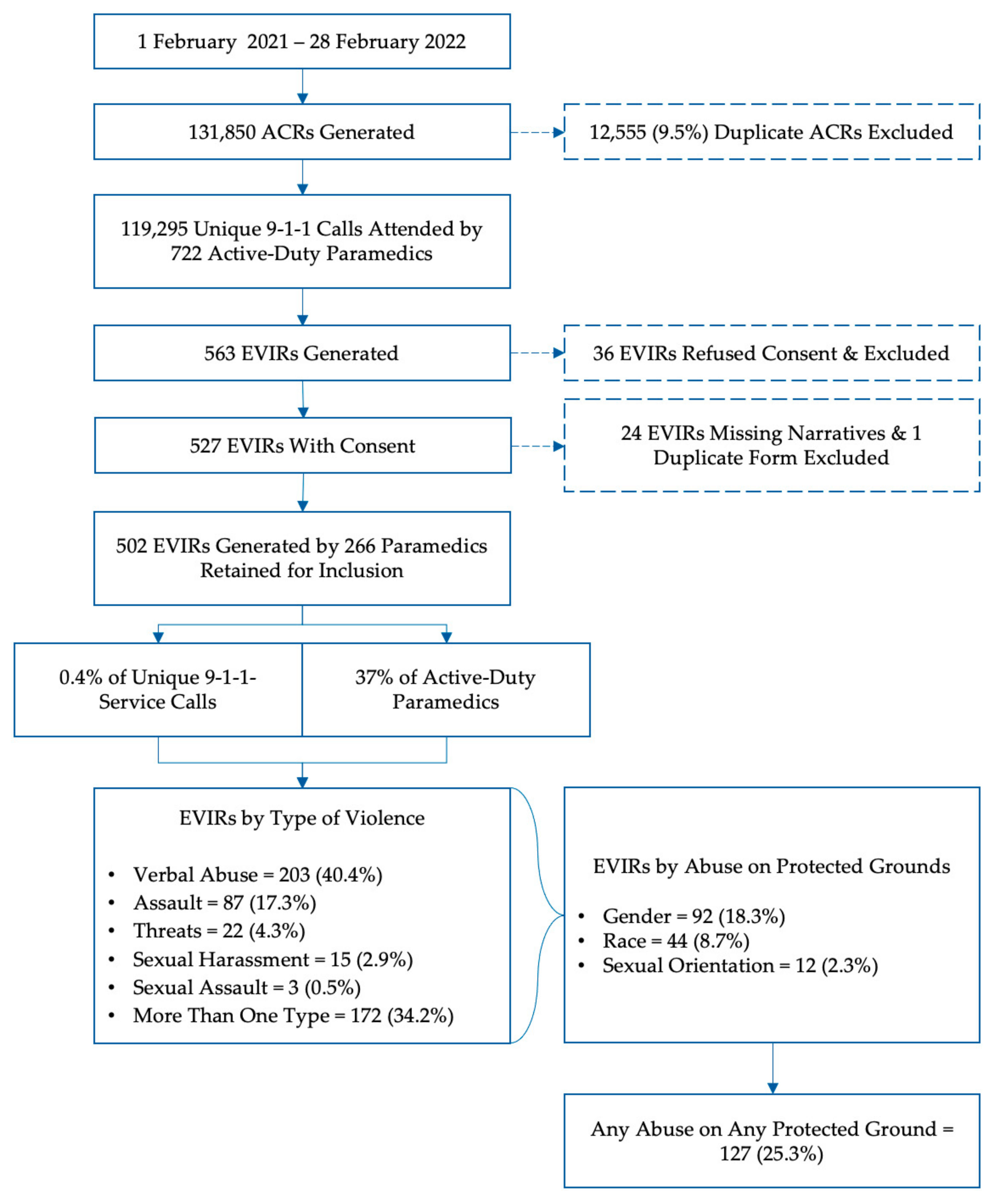
3.2. Overview
3.3. Sexist and Misogynistic Comments
3.4. Racist Comments
3.5. Homophobic Comments
3.6. Impact on Paramedics
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maguire, B.J.; O’Neill, B.J. Emergency Medical Service Personnel’s Risk from Violence While Serving the Community. Am. J. Public Health 2017, 107, 1770–1775. [Google Scholar] [CrossRef] [PubMed]
- Maguire, B.J.; Al Amiry, A.; O’Neill, B.J. Occupational Injuries and Illnesses among Paramedicine Clinicians: Analyses of US Department of Labor Data (2010–2020). Prehospital Disaster Med. 2023, 38, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Bigham, B.; Jensen, J.L.; Tavares, W.; Drennan, I.; Saleem, H.; Dainty, K.N.; Munro, G. Paramedic self-reported exposure to violence in the emergency medical services (EMS) workplace: A mixed-methods cross sectional survey. Prehospital Emerg. Care 2014, 18, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Corbett, S.W.; Grange, J.T.; Thomas, T.T. Exposure of prehospital care providers to violence. Prehospital Emerg. Care Off. J. Natl. Assoc. EMS Physicians Natl. Assoc. State EMS Dir. 1998, 2, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Furin, M.; Eliseo, L.J.; Langlois, B.; Fernandez, W.G.; Mitchell, P.; Dyer, K.S. Self-reported provider safety in an urban emergency medical system. West. J. Emerg. Med. 2015, 16, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Gormley, M.A.; Crowe, R.P.; Bentley, M.A.; Levine, R. A National Description of Violence toward Emergency Medical Services Personnel. Prehospital Emerg. Care 2016, 20, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Maguire, B.J.; Browne, M.; O’Neill, B.J.; Dealy, M.T.; Clare, D.; O’Meara, P. International Survey of Violence against EMS Personnel: Physical Violence Report. Prehospital Disaster Med. 2018, 33, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Setlack, J.; Brais, N.; Keough, M.; Johnson, E.A. Workplace violence and psychopathology in paramedics and firefighters: Mediated by posttraumatic cognitions. Can. J. Behav. Sci./Rev. Can. Sci. Comport. 2021, 53, 211–220. [Google Scholar] [CrossRef]
- Suserud, B.O.; Blomquist, M.; Johansson, I. Experiences of threats and violence in the Swedish ambulance service. Accid. Emerg. Nurs. 2002, 10, 127–135. [Google Scholar] [CrossRef]
- Wongtongkam, N. An exploration of violence against paramedics, burnout and post-traumatic symptoms in two Australian ambulance services. Int. J. Emerg. Serv. 2017, 6, 134–146. [Google Scholar] [CrossRef]
- Ambulance Staff Face Rise in Physical and Verbal Sexual Assaults. The Guardian, 23 April 2018.
- Brampton Man Charged after Female Paramedics Sexually Assaulted in Peel Region. CBC News, 1 April 2023.
- Drewitt-Smith, A.; Fuller, K. NSW Paramedic Steven Tougher Farewelled At Emotional Service in Wollongong. ABC News, 1 May 2023. [Google Scholar]
- Kilgannon, C. Slain paramedic, ‘mother of the station, was near retirement. The New York Times, 20 September 2022. [Google Scholar]
- CBC Radio. Threats, abuse, sexual harassment by the public: Paramedics on the dark side of the job. CBC Radio, 10 January 2020. [Google Scholar]
- Renić, K. Charges laid after paramedic assaulted at Halifax hospital, police say. Global News, 8 October 2022. [Google Scholar]
- Maguire, B.J.; O’Meara, P.; O’Neill, B.J.; Brightwell, R. Violence against emergency medical services personnel: A systematic review of the literature. Am. J. Ind. Med. 2018, 61, 167–180. [Google Scholar] [CrossRef] [PubMed]
- Mausz, J.; Johnston, M.; Donnelly, E.A. The role of organizational culture in normalizing paramedic exposure to violence. J. Aggress. Confl. Peace Res. 2021, 14, 112–122. [Google Scholar] [CrossRef]
- Chary, A.N.; Fofana, M.O.; Kohli, H.S. Racial Discrimination from Patients: Institutional Strategies to Establish Respectful Emergency Department Environments. West. J. Emerg. Med. 2021, 22, 898–902. [Google Scholar] [CrossRef] [PubMed]
- Kaltiso, S.O.; Seitz, R.M.; Zdradzinski, M.J.; Moran, T.P.; Heron, S.; Robertson, J.; Lall, M.D. The impact of racism on emergency health care workers. Acad. Emerg. Med. 2021, 28, 974–981. [Google Scholar] [CrossRef] [PubMed]
- Canpolat, E.K.; Gulacti, U. Changes in violence against healthcare professionals with the COVID-19 pandemic. Disaster Emerg. Med. J. 2022, 7, 75–82. [Google Scholar] [CrossRef]
- Larkin, H. Navigating attacks against health care workers in the COVID-19 era. JAMA J. Am. Med. Assoc. 2021, 325, 1822–1824. [Google Scholar] [CrossRef]
- Ramzi, Z.S.; Fatah, P.W.; Dalvandi, A. Prevalence of Workplace Violence against Healthcare Workers during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Front. Psychol. 2022, 13, 896156. [Google Scholar] [CrossRef]
- Saragih, I.D.; Tarihoran, D.; Rasool, A.; Saragih, I.S.; Tzeng, H.M.; Lin, C.J. Global prevalence of stigmatization and violence against healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. J. Nurs. Sch. 2022, 54, 762–771. [Google Scholar] [CrossRef]
- Mausz, J.; Johnston, M.; Donnelly, E. Development of a reporting process for violence against paramedics. Can. Paramed. 2021, 44, 23–27. [Google Scholar]
- Murray, R.M.; Davis, A.L.; Shepler, L.J.; Moore-Merrell, L.; Troup, W.J.; Allen, J.A.; Taylor, J.A. A Systematic Review of Workplace Violence against Emergency Medical Services Responders. New Solut. 2020, 29, 487–503. [Google Scholar] [CrossRef]
- Mausz, J.; Donnelly, E. Violence against paramedics: Protocol for evaluating one year of reports from a novel, point-of-event reporting process. JMIR Res. Protoc. 2022, 12, e37636. [Google Scholar] [CrossRef]
- Human Rights Code, R.S.O. 1990, c. H.19. 1990. Available online: https://www.ontario.ca/laws/statute/90h19 (accessed on 22 March 2024).
- Ontario Government. Preventing Workplace Violence and Workplace Harassment. Available online: https://www.ontario.ca/page/preventing-workplace-violence-and-workplace-harassment (accessed on 17 January 2024).
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Braun, D.; Reifferscheid, F.; Kerner, T.; Dressler, J.L.; Stuhr, M.; Wenderoth, S.; Petrowski, K. Association between the experience of violence and burnout among paramedics. Int. Arch. Occup. Environ. Health 2021, 94, 1559–1565. [Google Scholar] [CrossRef]
- Kim, J.H.; Lee, N.; Kim, J.Y.; Kim, S.J.; Okechukwu, C.; Kim, S.S. Organizational response to workplace violence, and its association with depressive symptoms: A nationwide survey of 1966 Korean EMS providers. J. Occup. Health 2019, 61, 101–109. [Google Scholar] [CrossRef]
- Maguire, B.J. Violence against ambulance personnel: A retrospective cohort study of national data from Safe Work Australia. Public Health Res. Pract. 2018, 28, e28011805. [Google Scholar] [CrossRef]
- Maguire, B.J.; Smith, S. Injuries and fatalities among emergency medical technicians and paramedics in the United States. Prehospital Disaster Med. 2013, 28, 376–382. [Google Scholar] [CrossRef]
- Garner, D.G., Jr.; DeLuca, M.B.; Crowe, R.P.; Cash, R.E.; Rivard, M.K.; Williams, J.G.; Panchal, A.R.; Cabanas, J.G. Emergency medical services professional behaviors with violent encounters: A prospective study using standardized simulated scenarios. J. Am. Coll. Emerg. Physicians Open 2022, 3, e12727. [Google Scholar] [CrossRef]
- Maguire, B.J.; O’Neill, B.J.; O’Meara, P.; Browne, M.; Dealy, M.T. Preventing EMS workplace violence: A mixed-methods analysis of insights from assaulted medics. Injury 2018, 49, 1258–1265. [Google Scholar] [CrossRef]
- Taylor, J.A.; Murray, R.M.; Davis, A.L.; Shepler, L.J.; Harrison, C.K.; Novinger, N.A.; Allen, J.A. Creation of a Systems-Level Checklist to Address Stress and Violence in Fire-Based Emergency Medical Services Responders. Occup. Health Sci. 2019, 3, 265–295. [Google Scholar] [CrossRef]
- Halpern, J.; Gurevich, M.; Schwartz, B.; Brazeau, P. Interventions for critical incident stress in emergency medical services: A qualitative study. Stress Health 2009, 25, 139–149. [Google Scholar] [CrossRef]
- Halpern, J.; Gurevich, M.; Schwartz, B.; Brazeau, P. What makes an incident critical for ambulance workers? Emotional outcomes and implications for intervention. Work. Stress 2009, 23, 173–189. [Google Scholar] [CrossRef]
- Chirico, F.; Afolabi, A.A.; Ilesanmi, O.S.; Nucera, G.; Ferrari, G.; Szarpak, L.; Yildirim, M.; Magnavita, N. Workplace violence against healthcare workers during the COVID-19 pandemic: A systematic review. J. Health Soc. Sci. 2022, 7, 14–35. [Google Scholar] [CrossRef]
- Ling, J. Far and Widening: The Rise of Polarization in Canada; The Public Policy Forum: Ottawa, ON, Canada, 2023. [Google Scholar]
- Blackwell, A.J. Quality of Employoment and Labour Market Dynamics of Health Care Workers during the COVID-19 Pandemic; Statistics Canada: Ottawa, ON, Canada, 2023. [Google Scholar]
- Duong, D.; Vogel, L. Overworked health workers are “past the point of exhaustion”. Can. Med. Assoc. J. 2023, 195, E309–E310. [Google Scholar] [CrossRef] [PubMed]
- Loriggio, P. Ontario Paramedics Say Ambulance Response Times Are Slower due to Growing Offload Delays. CBC News, 20 July 2023. [Google Scholar]
- Have You Been Affectedby Long Ambulance Wait Times? Let Us Know. CP24, 2 November 2023.
- Shortage of Ambulances in Toronto Means City Not Prepared for Major Disaster, Paramedic Union Says. CBC News, 4 October 2023.
- Government of Ontario. Ontario Helping more Students Become Paramedics. 29 June 2023. Available online: https://wwwn.cdc.gov/WPVHC/Nurses/Course/Slide/Unit5_5 (accessed on 22 March 2024).
- Occupational Safety and Health Administration. Guidelines for Preventing Workplace Violence for Healthcare and Social Servics Workers; OSHA: Boston, MA, USA, 2016. [Google Scholar]
- Nangia, P. Discrimination in the workplace in Canada: An intersectional approach. Can. J. Sociol. 2021, 46, 147–177. [Google Scholar] [CrossRef]


{kind=link}
| Domain | Rater 1 | Rater 2 | K | SE | Lower CI | Upper CI | p |
|---|---|---|---|---|---|---|---|
| Gender | 91 | 78 | 0.837 | 0.03 | 0.77 | 0.90 | <0.001 |
| Race | 49 | 42 | 0.795 | 0.04 | 0.70 | 0.88 | <0.001 |
| Sexual Orientation | 13 | 9 | 0.721 | 0.10 | 0.50 | 0.93 | <0.001 |
| Domain | (A) Complete Agreement | (B) Discrepant Cases | (C) Resolved as ‘No’ | (D) Resolved as ‘Yes’ | Final N (A + D) | % |
|---|---|---|---|---|---|---|
| Gender | 73 | 24 | 5 | 19 | 92 | 18% |
| Race | 37 | 16 | 9 | 7 | 44 | 9% |
| Sexual Orientation | 8 | 5 | 1 | 4 | 12 | 2% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mausz, J.; D’Eath, J.; Jackson, N.A.; Johnston, M.; Batt, A.M.; Donnelly, E.A. Sexist, Racist, and Homophobic Violence against Paramedics in a Single Canadian Site. Int. J. Environ. Res. Public Health 2024, 21, 505. https://doi.org/10.3390/ijerph21040505
Mausz J, D’Eath J, Jackson NA, Johnston M, Batt AM, Donnelly EA. Sexist, Racist, and Homophobic Violence against Paramedics in a Single Canadian Site. International Journal of Environmental Research and Public Health. 2024; 21(4):505. https://doi.org/10.3390/ijerph21040505
Chicago/Turabian StyleMausz, Justin, Joel D’Eath, Nicholas A. Jackson, Mandy Johnston, Alan M. Batt, and Elizabeth A. Donnelly. 2024. "Sexist, Racist, and Homophobic Violence against Paramedics in a Single Canadian Site" International Journal of Environmental Research and Public Health 21, no. 4: 505. https://doi.org/10.3390/ijerph21040505
APA StyleMausz, J., D’Eath, J., Jackson, N. A., Johnston, M., Batt, A. M., & Donnelly, E. A. (2024). Sexist, Racist, and Homophobic Violence against Paramedics in a Single Canadian Site. International Journal of Environmental Research and Public Health, 21(4), 505. https://doi.org/10.3390/ijerph21040505