
Chronic Stress Indicator: A Novel Tool for Comprehensive Stress Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Population for the Study
2.2. Operationalization of Study Variables
2.3. Overview of Research Variables and Associated Factors
2.4. Operationalizing the Chronic Stress Indicator and Allostatic Load
2.5. Statistical Analyses
3. Results
3.1. Overview of Research Participants
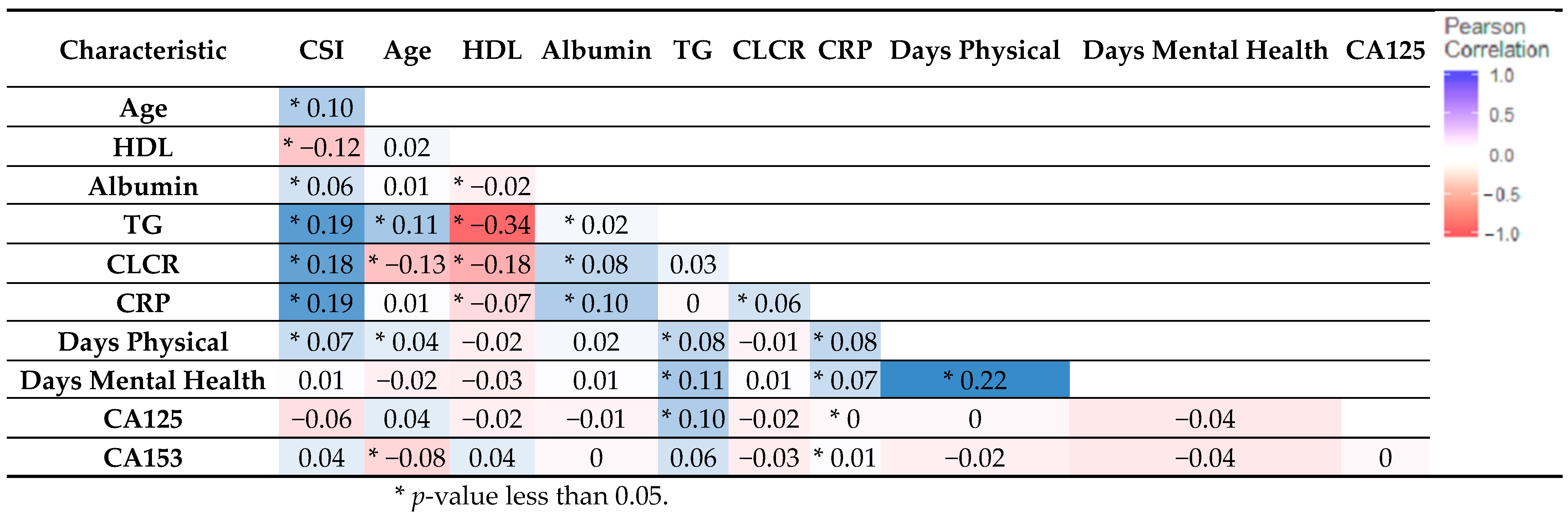
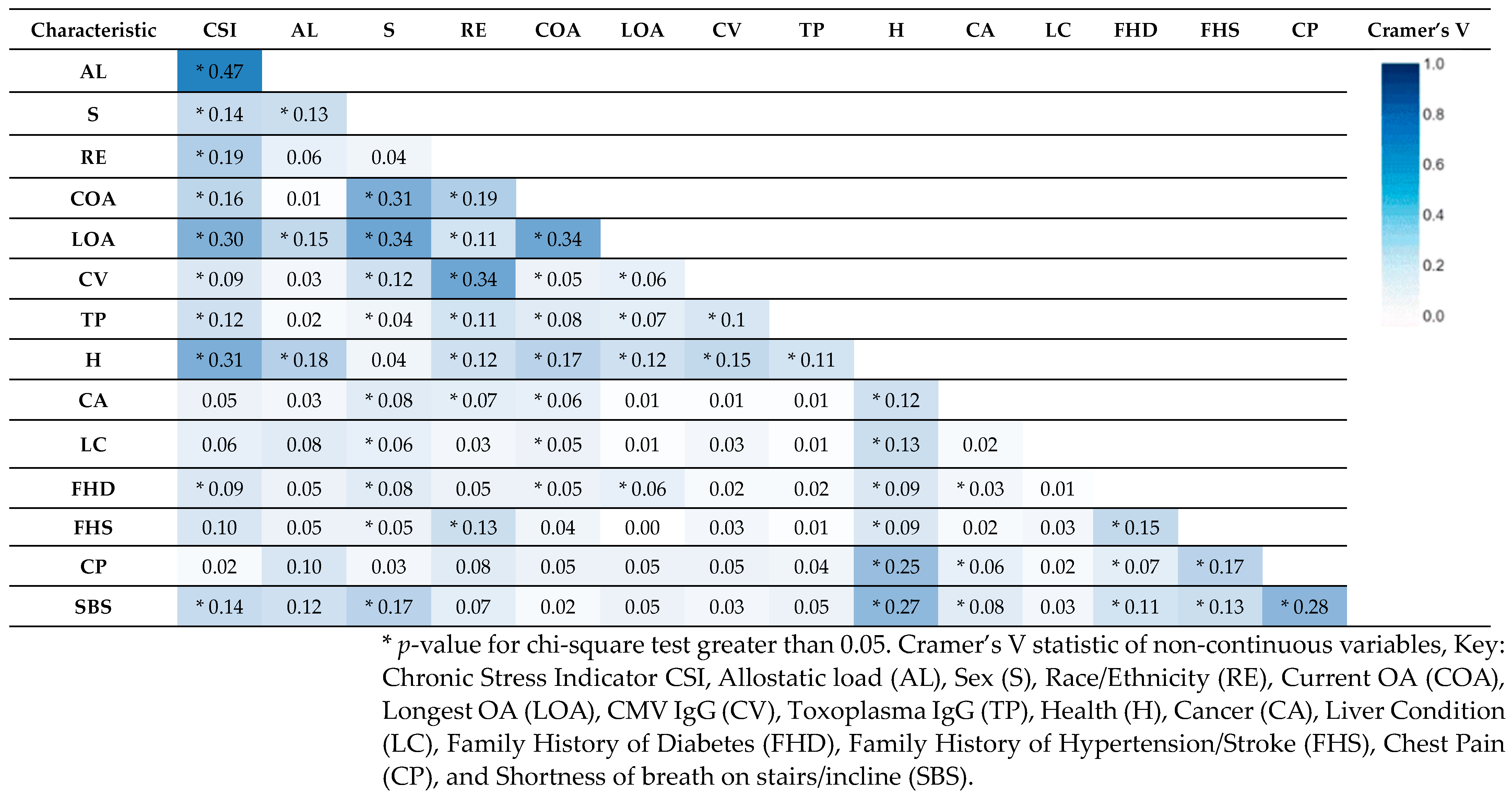
3.2. Tests of Association
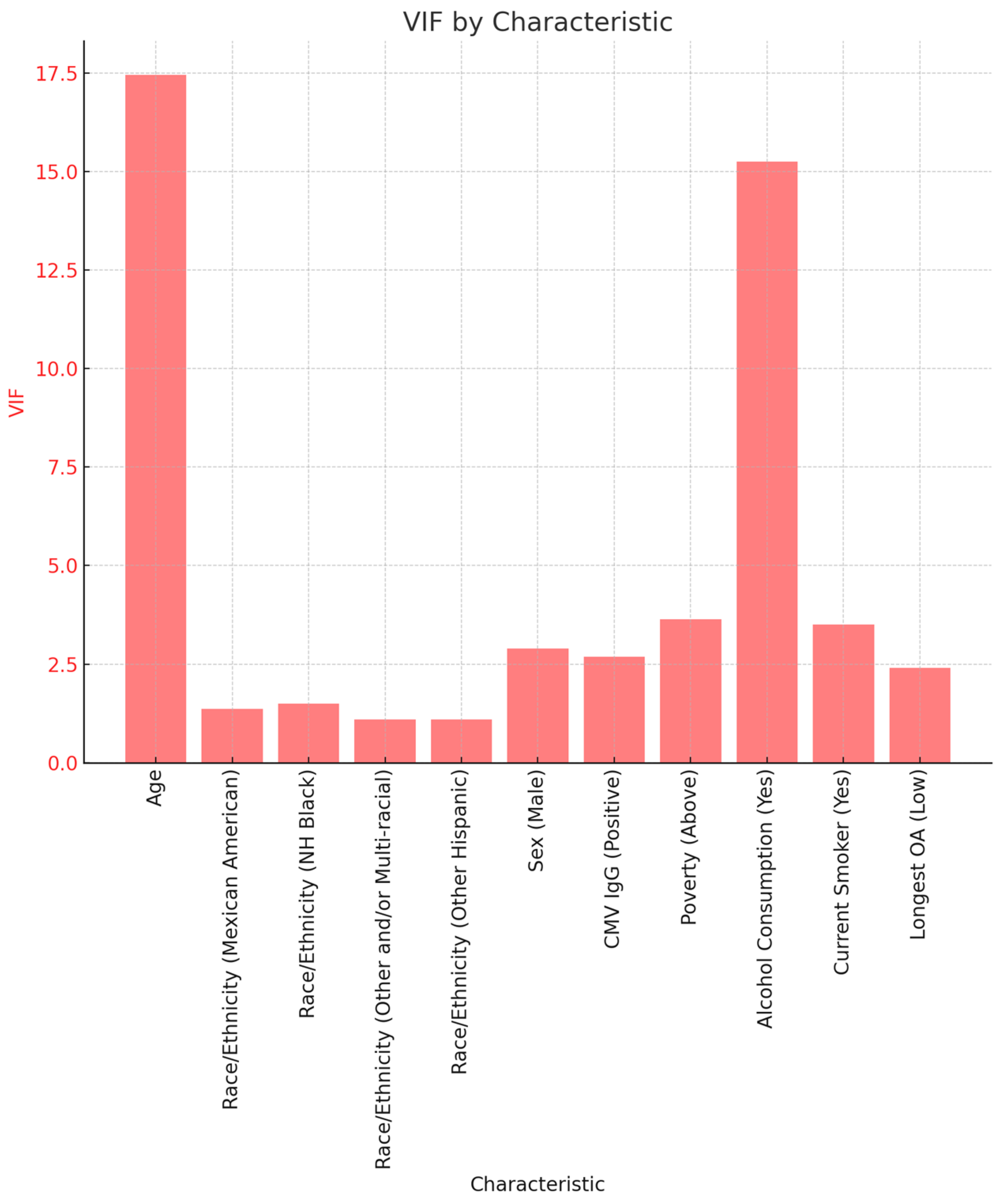
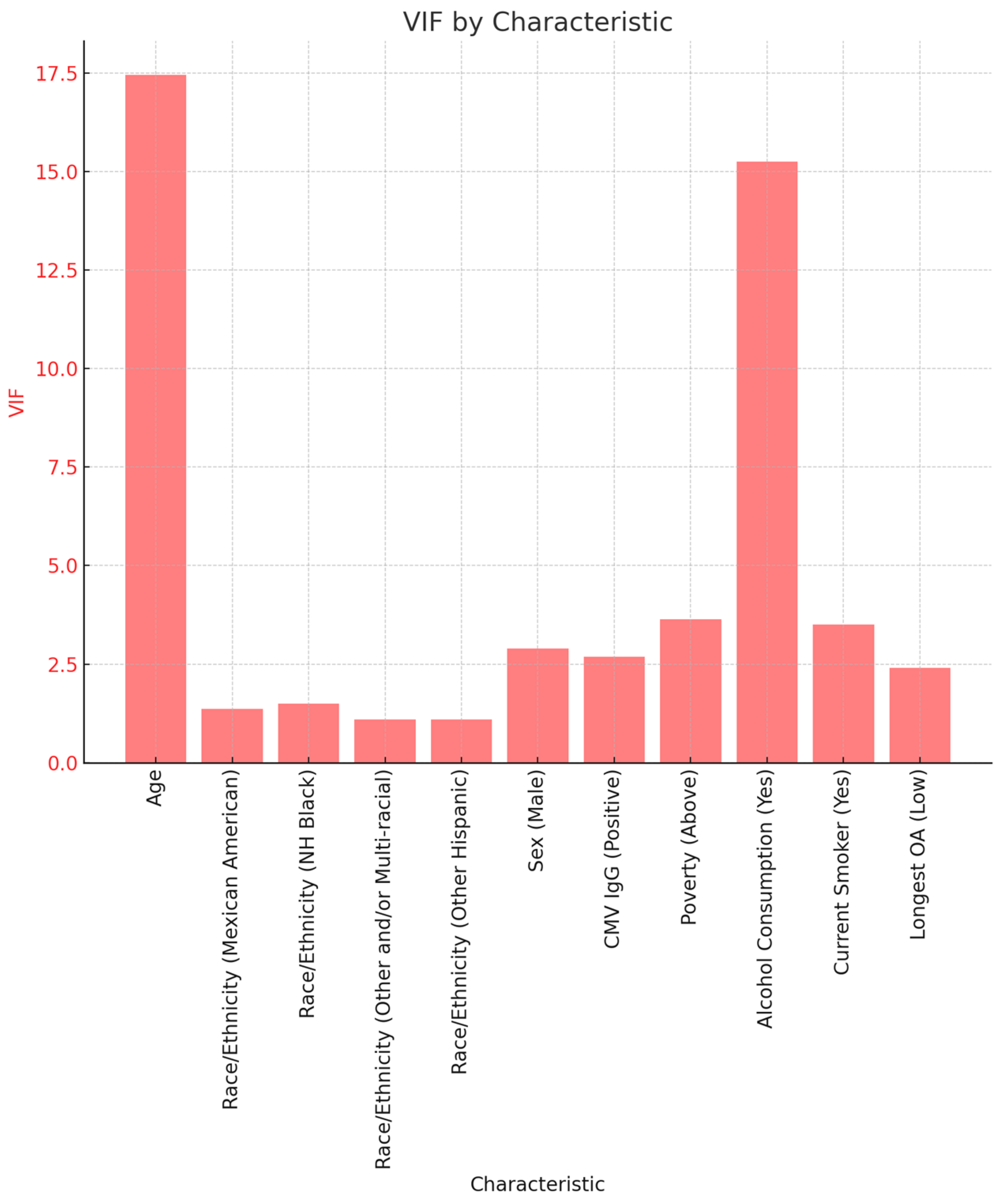
3.2.1. Variance Inflation Factor
3.2.2. Binary Logistic Regression
3.2.3. Exploratory Factor Analysis (EFA) for AL and CSI
4. Discussion
4.1. Allostatic Load as Compared to the Chronic Stress Predictive Model
4.2. Broader Implications of Study and Results
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Occupational Activity
| Low occupational activity | High occupational activty |
| Executive, administrators, and managers | Waiters and waitresses |
| Management-related occupations | Cleaning and building service occupations |
| Engineers, architects and scientists | Farm and nursery workers |
| Teachers | Construction laborers |
| Secretaries, stenographers, and typists | Construction trades |
| Information clerks | Laborers, except construction |
| Records processing occupations | Freight, stock, and material movers, hand |
| Material recording, scheduling, and distributing clerks | Cooks |
| Miscellaneous administrative support occupations | Extractive and precision production occupations |
| Motor vehicle operators | Fabricators, assemblers, inspectors, and samplers |
| Health diagnosing, assessing and treating occupations | Machine operators, assorted materials |
| Writers, artists, entertainers, and athletes | Miscellaneous food preparation and service occupations |
| Other professional specialty occupations | Other helpers, equipment cleaners, hand packagers and laborers |
| Technicians and related support occupations | Other mechanics and repairers |
| Supervisors and proprietors, sales occupations | Other transportation and material moving occupations |
| Farm operators, managers, and supervisors | Protective service occupations |
| Health service occupations | Related agricultural, forestry, and fishing occupations |
| Personal service occupations | Textile, apparel, and furnishings machine operators |
| Private household occupations | Vehicle and mobile equipment mechanics and repairers |
| Sales representatives, finance, business, & commodities ex. retail | |
| Sales workers, retail and personal services | |
| This table organizes occupations into two main categories based on their activity level. Roles identified as having low occupational activity include those in professional, managerial, administrative, and clerical fields. Examples of such positions are executives, managers, engineers, secretaries, and technicians, typically involving less physical activity. In contrast, occupations classified under high occupational activity are largely made up of manual labor and skilled trades. This group includes construction workers, machine operators, and agricultural workers. Furthermore, occupations in the service industry, such as waiters and cooks, along with those in protective services, are also part of this high-activity category, demanding significant physical effort and continuous vigilance. |

{kind=link}
{kind=link}
{kind=link}
| AL Risk | ||||
|---|---|---|---|---|
| Characteristic | Overall, N = 25,098,492 | Low, N = 13,203,060 | High, N = 11,895,432 | p-Value |
| Current Occupational Activity (COA) | 0.900 | |||
| High *OA | 29.27% | 50.34% | 49.66% | |
| Low *OA | 48.94% | 49.78% | 50.22% | |
| Current Occupation | 0.400 | |||
| Cleaning and building service occupations | 1.51% | 52.53% | 47.47% | |
| Construction laborers | 0.52% | 41.28% | 58.72% | |
| Construction trades | 6.49% | 51.13% | 48.87% | |
| Cooks | 0.89% | 57.00% | 43.00% | |
| Engineers, architects and scientists | 4.26% | 49.78% | 50.22% | |
| Executive, administrators, and managers | 6.77% | 53.19% | 46.81% | |
| Extractive and precision production occupations | 0.65% | 100.00% | 0.00% | |
| Fabricators, assemblers, inspectors, and samplers | 2.15% | 48.47% | 51.53% | |
| Farm and nursery workers | 0.55% | 58.26% | 41.74% | |
| Farm operators, managers, and supervisors | 0.32% | 0.00% | 100.00% | |
| Freight, stock, and material movers, hand | 0.93% | 45.38% | 54.62% | |
| Health diagnosing, assessing and treating occupations | 1.93% | 43.56% | 56.44% | |
| Health service occupations | 2.67% | 35.23% | 64.77% | |
| Information clerks | 0.94% | 51.97% | 48.03% | |
| Laborers, except construction | 0.21% | 100.00% | 0.00% | |
| Machine operators, assorted materials | 3.03% | 45.46% | 54.54% | |
| Management-related occupations | 2.01% | 56.72% | 43.28% | |
| Material recording, scheduling, and distributing clerks | 1.18% | 43.12% | 56.88% | |
| Miscellaneous administrative support occupations | 5.45% | 63.30% | 36.70% | |
| Miscellaneous food preparation and service occupations | 1.65% | 45.67% | 54.33% | |
| Motor vehicle operators | 1.95% | 30.23% | 69.77% | |
| Other helpers, equipment cleaners, hand packagers and laborers | 1.23% | 44.28% | 55.72% | |
| Other mechanics and repairers | 1.19% | 33.77% | 66.23% | |
| Other professional specialty occupations | 1.44% | 50.63% | 49.37% | |
| Other transportation and material moving occupations | 1.81% | 21.04% | 78.96% | |
| Personal service occupations | 1.47% | 61.96% | 38.04% | |
| Private household occupations | 0.75% | 80.97% | 19.03% | |
| Protective service occupations | 1.45% | 42.91% | 57.09% | |
| Records processing occupations | 2.96% | 57.98% | 42.02% | |
| Occupations in agriculture, forestry, and fishing-related fields | 1.45% | 61.87% | 38.13% | |
| Sales representatives, finance, business, & commodities ex. retail | 1.87% | 28.23% | 71.77% | |
| Sales workers, retail and personal services | 3.11% | 59.65% | 40.35% | |
| Secretaries, stenographers, and typists | 0.88% | 56.07% | 43.93% | |
| Supervisors and proprietors, sales occupations | 1.47% | 45.60% | 54.40% | |
| Teachers | 2.09% | 30.86% | 69.14% | |
| Technicians and related support occupations | 3.52% | 50.26% | 49.74% | |
| Textile, apparel, and furnishings machine operators | 0.53% | 60.70% | 39.30% | |
| Vehicle and mobile equipment mechanics and repairers | 1.43% | 48.39% | 51.61% | |
| Waiters and waitresses | 1.61% | 78.96% | 21.04% | |
| Writers, artists, entertainers, and athletes | 1.90% | 40.07% | 59.93% | |
| Longest Occupational Activity (LOA) | 0.005 | |||
| High *OA | 22.24% | 43.82% | 56.18% | |
| Low *OA | 24.27% | 59.01% | 40.99% | |
| Longest Occupation | 0.200 | |||
| Cleaning and building service occupations | 1.35% | 32.90% | 67.10% | |
| Construction laborers | 0.60% | 41.43% | 58.57% | |
| Construction trades | 1.81% | 28.48% | 71.52% | |
| Cooks | 0.82% | 41.67% | 58.33% | |
| Engineers, architects and scientists | 1.05% | 52.05% | 47.95% | |
| Executive, administrators, and managers | 2.42% | 41.83% | 58.17% | |
| Extractive and precision production occupations | 2.00% | 51.26% | 48.74% | |
| Fabricators, assemblers, inspectors, and samplers | 1.23% | 49.51% | 50.49% | |
| Farm and nursery workers | 0.87% | 60.55% | 39.45% | |
| Farm operators, managers, and supervisors | 0.56% | 0.00% | 100.00% | |
| Freight, stock, and material movers, hand | 0.97% | 42.47% | 57.53% | |
| Health diagnosing, assessing and treating occupations | 1.05% | 60.14% | 39.86% | |
| Health service occupations | 1.58% | 57.54% | 42.46% | |
| Information clerks | 0.73% | 88.87% | 11.13% | |
| Laborers, except construction | 0.73% | 31.42% | 68.58% | |
| Machine operators, assorted materials | 1.53% | 35.26% | 64.74% | |
| Management-related occupations | 0.80% | 72.24% | 27.76% | |
| Material recording, scheduling, and distributing clerks | 0.23% | 26.71% | 73.29% | |
| Military occupations | 0.22% | 0.00% | 100.00% | |
| Miscellaneous administrative support occupations | 2.78% | 48.99% | 51.01% | |
| Miscellaneous food preparation and service occupations | 1.50% | 67.38% | 32.62% | |
| Motor vehicle operators | 1.27% | 40.95% | 59.05% | |
| Other helpers, equipment cleaners, hand packagers and laborers | 0.36% | 38.39% | 61.61% | |
| Other mechanics and repairers | 1.07% | 36.39% | 63.61% | |
| Other professional specialty occupations | 0.82% | 59.27% | 40.73% | |
| Other transportation and material moving occupations | 0.99% | 24.01% | 75.99% | |
| Personal service occupations | 0.90% | 93.33% | 6.67% | |
| Private household occupations | 0.29% | 53.69% | 46.31% | |
| Protective service occupations | 0.68% | 68.17% | 31.83% | |
| Records processing occupations | 0.78% | 100.00% | 0.00% | |
| Related agricultural, forestry, and fishing occupations | 1.23% | 42.48% | 57.52% | |
| Sales representatives, finance, business, & commodities ex. retail | 0.24% | 53.36% | 46.64% | |
| Sales workers, retail and personal services | 3.69% | 66.31% | 33.69% | |
| Secretaries, stenographers, and typists | 1.02% | 89.52% | 10.48% | |
| Supervisors and proprietors, sales occupations | 0.68% | 61.42% | 38.58% | |
| Teachers | 0.53% | 88.23% | 11.77% | |
| Technicians and related support occupations | 1.67% | 53.44% | 46.56% | |
| Textile, apparel, and furnishings machine operators | 0.83% | 62.30% | 37.70% | |
| Vehicle and mobile equipment mechanics and repairers | 1.11% | 65.87% | 34.13% | |
| Waiters and waitresses | 2.34% | 35.97% | 64.03% | |
| Writers, artists, entertainers, and athletes | 1.17% | 44.37% | 55.63% | |
| CSI Risk | ||||
|---|---|---|---|---|
| Characteristic | Overall, N = 22,862,802 | Low, N = 9,088,249 | High, N = 13,774,553 | p-Value |
| Current Occupational Activity (OA) | 0.005 | |||
| High OA | 32.08% | 32.57% | 67.43% | |
| Low OA | 43.73% | 49.04% | 50.96% | |
| Current Occupation | 0.049 | |||
| Cleaning and building service occupations | 1.44% | 58.71% | 41.29% | |
| Construction laborers | 0.65% | 18.98% | 81.02% | |
| Construction trades | 7.43% | 28.44% | 71.56% | |
| Cooks | 0.58% | 16.10% | 83.90% | |
| Engineers, architects and scientists | 3.08% | 58.19% | 41.81% | |
| Executive, administrators, and managers | 6.15% | 66.52% | 33.48% | |
| Extractive and precision production occupations | 2.48% | 44.42% | 55.58% | |
| Fabricators, assemblers, inspectors, and samplers | 1.39% | 15.77% | 84.23% | |
| Farm and nursery workers | 0.51% | 34.87% | 65.13% | |
| Farm operators, managers, and supervisors | 0.23% | 100.00% | 0.00% | |
| Freight, stock, and material movers, hand | 0.74% | 0.00% | 100.00% | |
| Health diagnosing, assessing and treating occupations | 1.50% | 69.96% | 30.04% | |
| Health service occupations | 2.53% | 21.83% | 78.17% | |
| Information clerks | 0.81% | 51.20% | 48.80% | |
| Laborers, except construction | 0.18% | 37.33% | 62.67% | |
| Machine operators, assorted materials | 2.47% | 51.24% | 48.76% | |
| Management-related occupations | 0.86% | 74.98% | 25.02% | |
| Material recording, scheduling, and distributing clerks | 1.92% | 25.21% | 74.79% | |
| Miscellaneous administrative support occupations | 6.35% | 54.59% | 45.41% | |
| Miscellaneous food preparation and service occupations | 1.70% | 43.84% | 56.16% | |
| Motor vehicle operators | 2.59% | 29.88% | 70.12% | |
| Other helpers, equipment cleaners, hand packagers and laborers | 0.89% | 8.01% | 91.99% | |
| Other mechanics and repairers | 2.03% | 39.15% | 60.85% | |
| Other professional specialty occupations | 1.00% | 71.07% | 28.93% | |
| Other transportation and material moving occupations | 1.55% | 13.41% | 86.59% | |
| Personal service occupations | 0.94% | 57.99% | 42.01% | |
| Private household occupations | 0.17% | 100.00% | 0.00% | |
| Protective service occupations | 1.27% | 23.38% | 76.62% | |
| Records processing occupations | 2.49% | 40.25% | 59.75% | |
| Related agricultural, forestry, and fishing occupations | 1.72% | 38.96% | 61.04% | |
| Sales representatives, finance, business, & commodities ex. retail | 2.02% | 37.44% | 62.56% | |
| Sales workers, retail and personal services | 3.88% | 33.62% | 66.38% | |
| Secretaries, stenographers, and typists | 0.72% | 46.55% | 53.45% | |
| Supervisors and proprietors, sales occupations | 1.59% | 12.50% | 87.50% | |
| Teachers | 1.30% | 57.63% | 42.37% | |
| Technicians and related support occupations | 2.36% | 39.92% | 60.08% | |
| Textile, apparel, and furnishings machine operators | 0.69% | 0.00% | 100.00% | |
| Vehicle and mobile equipment mechanics and repairers | 1.96% | 35.40% | 64.60% | |
| Waiters and waitresses | 2.40% | 40.01% | 59.99% | |
| Writers, artists, entertainers, and athletes | 1.22% | 100.00% | 0.00% | |
| Longest OA | 0.003 | |||
| High OA | 27.46% | 23.69% | 76.31% | |
| Low OA | 24.68% | 53.16% | 46.84% | |
| Longest Occupation | 0.023 | |||
| Cleaning and building service occupations | 1.48% | 33.39% | 66.61% | |
| Construction laborers | 1.17% | 0.00% | 100.00% | |
| Construction trades | 2.93% | 19.95% | 80.05% | |
| Cooks | 0.54% | 48.25% | 51.75% | |
| Engineers, architects and scientists | 1.09% | 47.19% | 52.81% | |
| Executive, administrators, and managers | 2.43% | 53.66% | 46.34% | |
| Extractive and precision production occupations | 2.77% | 7.66% | 92.34% | |
| Fabricators, assemblers, inspectors, and samplers | 1.86% | 34.56% | 65.44% | |
| Farm and nursery workers | 0.57% | 24.72% | 75.28% | |
| Farm operators, managers, and supervisors | 0.16% | 0.00% | 100.00% | |
| Freight, stock, and material movers, hand | 1.57% | 26.33% | 73.67% | |
| Health diagnosing, assessing and treating occupations | 0.49% | 46.52% | 53.48% | |
| Health service occupations | 1.50% | 40.69% | 59.31% | |
| Information clerks | 0.77% | 70.90% | 29.10% | |
| Laborers, except construction | 1.19% | 6.02% | 93.98% | |
| Machine operators, assorted materials | 1.55% | 41.71% | 58.29% | |
| Management-related occupations | 1.49% | 54.84% | 45.16% | |
| Material recording, scheduling, and distributing clerks | 0.49% | 0.00% | 100.00% | |
| Military occupations | 0.23% | 0.00% | 100.00% | |
| Miscellaneous administrative support occupations | 3.49% | 52.96% | 47.04% | |
| Miscellaneous food preparation and service occupations | 1.80% | 20.76% | 79.24% | |
| Motor vehicle operators | 1.38% | 9.67% | 90.33% | |
| Other helpers, equipment cleaners, hand packagers and laborers | 0.41% | 10.13% | 89.87% | |
| Other mechanics and repairers | 1.09% | 31.46% | 68.54% | |
| Other professional specialty occupations | 0.51% | 69.41% | 30.59% | |
| Other transportation and material moving occupations | 1.52% | 16.27% | 83.73% | |
| Personal service occupations | 1.13% | 22.74% | 77.26% | |
| Private household occupations | 0.15% | 0.00% | 100.00% | |
| Protective service occupations | 0.60% | 8.44% | 91.56% | |
| Records processing occupations | 1.02% | 79.77% | 20.23% | |
| Related agricultural, forestry, and fishing occupations | 1.29% | 28.28% | 71.72% | |
| Sales representatives, finance, business, & commodities ex. retail | 0.69% | 83.88% | 16.12% | |
| Sales workers, retail and personal services | 2.27% | 34.28% | 65.72% | |
| Secretaries, stenographers, and typists | 0.98% | 51.23% | 48.77% | |
| Supervisors and proprietors, sales occupations | 1.04% | 63.27% | 36.73% | |
| Teachers | 0.50% | 100.00% | 0.00% | |
| Technicians and related support occupations | 1.85% | 85.42% | 14.58% | |
| Textile, apparel, and furnishings machine operators | 0.93% | 7.35% | 92.65% | |
| Vehicle and mobile equipment mechanics and repairers | 1.77% | 32.87% | 67.13% | |
| Waiters and waitresses | 2.19% | 44.24% | 55.76% | |
| Writers, artists, entertainers, and athletes | 1.26% | 87.74% | 12.26% | |
References
- Perlman, G.; Cogo-Moreira, H.; Wu, C.-Y.; Herrmann, N.; Swardfager, W. Depression interacts with allostatic load to predict cognitive decline in middle age. Psychoneuroendocrinology 2022, 146, 105922. [Google Scholar] [CrossRef]
- McEwen, B.S. Stress, adaptation, and disease: Allostasis and allostatic load. Ann. N. Y. Acad. Sci. 1998, 840, 33–44. [Google Scholar] [CrossRef]
- Zefferino, R.; Di Gioia, S.; Conese, M. Molecular links between endocrine, nervous and immune system during chronic stress. Brain Behav. 2021, 11, e01960. [Google Scholar] [CrossRef] [PubMed]
- Guidi, J.; Lucente, M.; Sonino, N.; Fava, G.A. Allostatic load and its impact on health: A systematic review. Psychother. Psychosom. 2021, 90, 11–27. [Google Scholar] [CrossRef]
- McEwen, B.S. Protection and damage from acute and chronic stress: Allostasis and allostatic overload and relevance to the pathophysiology of psychiatric disorders. Ann. N. Y. Acad. Sci. 2004, 1032, 1–7. [Google Scholar] [CrossRef]
- McEwen, B.S.; Gianaros, P.J. Central role of the brain in stress and adaptation: Links to socioeconomic status, health, and disease. Ann. N. Y. Acad. Sci. 2010, 1186, 190–222. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Willett, W.C.; Hu, F.B. Global obesity: Trends, risk factors and policy implications. Nat. Rev. Endocrinol. 2013, 9, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Siew, R.V.K.; Nabe-Nielsen, K.; Turner, A.I.; Bujtor, M.; Torres, S.J. The role of combined modifiable lifestyle behaviors in the association between exposure to stressors and allostatic load: A systematic review of observational studies. Psychoneuroendocrinology 2022, 138, 105668. [Google Scholar] [CrossRef]
- Szanton, S.L.; Gill, J.M.; Allen, J.K. Allostatic load: A mechanism of socioeconomic health disparities? Biol. Res. Nurs. 2005, 7, 7–15. [Google Scholar] [CrossRef]
- Rothwell, D.W.; Han, C.K. Exploring the relationship between assets and family stress among low-income families. Fam. Relat. 2010, 59, 396–407. [Google Scholar] [CrossRef]
- Santiago, C.D.; Wadsworth, M.E.; Stump, J. Socioeconomic status, neighborhood disadvantage, and poverty-related stress: Prospective effects on psychological syndromes among diverse low-income families. J. Econ. Psychol. 2011, 32, 218–230. [Google Scholar] [CrossRef]
- Richardson, A.S.; Arsenault, J.E.; Cates, S.C.; Muth, M.K. Perceived stress, unhealthy eating behaviors, and severe obesity in low-income women. Nutr. J. 2015, 14, 122. [Google Scholar] [CrossRef]
- Stults-Kolehmainen, M.A.; Sinha, R. The effects of stress on physical activity and exercise. Sports Med. 2014, 44, 81–121. [Google Scholar] [CrossRef]
- Nguyen-Michel, S.T.; Unger, J.B.; Hamilton, J.; Spruijt-Metz, D. Associations between physical activity and perceived stress/hassles in college students. Stress Health J. Int. Soc. Investig. Stress 2006, 22, 179–188. [Google Scholar] [CrossRef]
- Corbin, W.R.; Farmer, N.M.; Nolen-Hoekesma, S. Relations among stress, coping strategies, coping motives, alcohol consumption and related problems: A mediated moderation model. Addict. Behav. 2013, 38, 1912–1919. [Google Scholar] [CrossRef] [PubMed]
- Brady, K.T.; Sonne, S.C. The role of stress in alcohol use, alcoholism treatment, and relapse. Alcohol Res. Health 1999, 23, 263. [Google Scholar] [PubMed]
- Siqueira, L.; Diab, M.; Bodian, C.; Rolnitzky, L. Adolescents becoming smokers: The roles of stress and coping methods. J. Adolesc. Health 2000, 27, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Kassel, J.D.; Stroud, L.R.; Paronis, C.A. Smoking, stress, and negative affect: Correlation, causation, and context across stages of smoking. Psychol. Bull. 2003, 129, 270. [Google Scholar] [CrossRef] [PubMed]
- Centers-For-Disease-Control-and-Prevention. Laboratory Procedure Manual. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2015-2016/labmethods/PFAS_I_MET.pdf (accessed on 3 March 2024).
- Griffiths, K.L.; Mackey, M.G.; Adamson, B.J. The impact of a computerized work environment on professional occupational groups and behavioural and physiological risk factors for musculoskeletal symptoms: A literature review. J. Occup. Rehabil. 2007, 17, 743–765. [Google Scholar] [CrossRef] [PubMed]
- Straker, L.; Dunstan, D.; Gilson, N.; Healy, G. Sedentary Work. Evidence on an Emergent Work Health and Safety Issue; Safe Work Australia: Canberra, Australia, 2016. [Google Scholar]
- National Research Council (US) and Institute of Medicine (US) Panel on Musculoskeletal Disorders and the Workplace. Musculoskeletal Disorders and the Workplace: Low Back and Upper Extremities; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Hill, M.; Mostafa, S.; Muganda, P.M.; Jeffers-Francis, L.K.; Obeng-Gyasi, E. The Association of Cytomegalovirus and Allostatic Load by Country of Birth and Length of Time in the United States. Diseases 2023, 11, 101. [Google Scholar] [CrossRef] [PubMed]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Kemeny, M.E. The psychobiology of stress. Curr. Dir. Psychol. Sci. 2003, 12, 124–129. [Google Scholar] [CrossRef]
- Kagias, K.; Nehammer, C.; Pocock, R. Neuronal responses to physiological stress. Front. Genet. 2012, 3, 222. [Google Scholar] [CrossRef] [PubMed]
- Lantos, P.M.; Hoffman, K.; Permar, S.R.; Jackson, P.; Hughes, B.L.; Kind, A.; Swamy, G. Neighborhood Disadvantage is Associated with High Cytomegalovirus Seroprevalence in Pregnancy. J. Racial Ethn. Health Disparities 2018, 5, 782–786. [Google Scholar] [CrossRef]
- Mareze, M.; Benitez, A.d.N.; Brandão, A.P.D.; Pinto-Ferreira, F.; Miura, A.C.; Martins, F.D.C.; Caldart, E.T.; Biondo, A.W.; Freire, R.L.; Mitsuka-Breganó, R.; et al. Socioeconomic vulnerability associated to Toxoplasma gondii exposure in southern Brazil. PLoS ONE 2019, 14, e0212375. [Google Scholar] [CrossRef]
- Locker, D. Social determinants of health and disease. In Sociology as Applied to Medicine; Saunders: Edinburgh, Ireland; Elsevier: New York, NY, USA, 2008. [Google Scholar]
- Rout, U.R.; Rout, J.K. Occupational stress. In Stress Management for Primary Health Care Professionals; Springer: Berlin/Heidelberg, Germany, 2002; pp. 25–39. [Google Scholar]
- Van der Doef, M.; Maes, S. The job demand-control (-support) model and psychological well-being: A review of 20 years of empirical research. Work Stress 1999, 13, 87–114. [Google Scholar] [CrossRef]
- Schedlowski, M.; Schmidt, R.E. Stress and the immune system. Naturwissenschaften 1996, 83, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Kunz-Ebrecht, S.; Owen, N.; Feldman, P.J.; Willemsen, G.; Kirschbaum, C.; Marmot, M. Socioeconomic status and stress-related biological responses over the working day. Psychosom. Med. 2003, 65, 461–470. [Google Scholar] [CrossRef]
- Baum, A.; Garofalo, J.; Yali, A.M. Socioeconomic status and chronic stress: Does stress account for SES effects on health? Ann. N. Y. Acad. Sci. 1999, 896, 131–144. [Google Scholar] [CrossRef]
- Gallo, L.C.; Shivpuri, S.; Gonzalez, P.; Fortmann, A.L.; de los Monteros, K.E.; Roesch, S.C.; Talavera, G.A.; Matthews, K.A. Socioeconomic status and stress in Mexican–American women: A multi-method perspective. J. Behav. Med. 2013, 36, 379–388. [Google Scholar] [CrossRef]
- Schmeer, K.K.; Tarrence, J. Racial-ethnic disparities in inflammation: Evidence of weathering in childhood? J. Health Soc. Behav. 2018, 59, 411–428. [Google Scholar] [CrossRef]
- Steptoe, A.; Wardle, J.; Pollard, T.M.; Canaan, L.; Davies, G.J. Stress, social support and health-related behavior: A study of smoking, alcohol consumption and physical exercise. J. Psychosom. Res. 1996, 41, 171–180. [Google Scholar] [CrossRef]
- Buttrick, N.R.; Oishi, S. The psychological consequences of income inequality. Soc. Personal. Psychol. Compass 2017, 11, e12304. [Google Scholar] [CrossRef]
- Assari, S.; Bazargan, M. Unequal associations between educational attainment and occupational stress across racial and ethnic groups. Int. J. Environ. Res. Public Health 2019, 16, 3539. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.A.; Patel, P.P.; Khadilkar, A.V.; Chiplonkar, S.; Patel, A.D. Impact of occupation on stress and anxiety among Indian women. Women Health 2017, 57, 392–401. [Google Scholar] [CrossRef] [PubMed]
- Bashir, T.; Obeng-Gyasi, E. Interaction of Per- and Polyfluoroalkyl Substances and Allostatic Load among Adults in Various Occupations. Diseases 2022, 10, 26. [Google Scholar] [CrossRef]
| CSI | AL |
|---|---|
| Systolic Blood Pressure | Systolic Blood Pressure |
| Diastolic Blood Pressure | Diastolic Blood Pressure |
| Total cholesterol | Total Cholesterol |
| Hemoglobin A1c | Hemoglobin A1c |
| BMI | BMI |
| Education Level | Triglycerides |
| Poverty status | High-Density Lipoprotein |
| Alcohol consumption | Albumin |
| Tobacco use | Creatinine Clearance |
| Physical activity | C-Reactive Protein |
| AL Risk | ||||
|---|---|---|---|---|
| Characteristic | Overall, N = 25,098,492 | Low, N = 13,203,060 | High, N = 11,895,432 | p-Value |
| Age | 34.79 (0.42) | 32.28 (0.54) | 37.57 (0.49) | <0.001 |
| Sex | <0.001 | |||
| Female | 47.95% | 59.28% | 40.72% | |
| Male | 52.05% | 46.45% | 53.55% | |
| Race/Ethnicity | 0.600 | |||
| NH White | 67.96% | 52.45% | 47.55% | |
| Mexican American | 9.75% | 59.34% | 40.66% | |
| NH Black | 12.17% | 50.50% | 49.50% | |
| Other and/or Multi-racial | 5.16% | 53.93% | 46.07% | |
| Other Hispanic | 4.96% | 45.24% | 54.76% | |
| Annual Income | 0.072 | |||
| $0–$4999 | 4.10% | 66.68% | 33.32% | |
| $10,000–$14,999 | 7.35% | 69.41% | 30.59% | |
| $15,000–$19,999 | 6.76% | 50.27% | 49.73% | |
| Under $20,000 | 0.86% | 81.02% | 18.98% | |
| Over $20,000 | 1.50% | 51.31% | 48.69% | |
| $20,000–$24,999 | 7.06% | 54.80% | 45.20% | |
| $25,000–$34,999 | 11.79% | 64.02% | 35.98% | |
| $35,000–$44,999 | 8.27% | 50.22% | 49.78% | |
| $45,000–$54,999 | 8.43% | 55.09% | 44.91% | |
| $5000–$9999 | 4.10% | 47.61% | 52.39% | |
| $55,000–$64,999 | 7.59% | 44.88% | 55.12% | |
| $65,000–$74,999 | 6.80% | 39.55% | 60.45% | |
| $75,000 and over | 23.98% | 46.83% | 53.17% | |
| Poverty | 0.200 | |||
| At or Below | 23.17% | 59.92% | 40.08% | |
| Above | 75.42% | 50.80% | 49.20% | |
| Education | 0.200 | |||
| High school graduate or GED equivalent. | 27.59% | 54.24% | 45.76% | |
| Grades 9–11 (Includes 12th grade without diploma) | 11.47% | 44.50% | 55.50% | |
| College graduate or above | 20.40% | 51.28% | 48.72% | |
| Less than 9th grade | 5.09% | 42.95% | 57.05% | |
| Some college or AA degree | 35.14% | 56.11% | 43.89% | |
| Physical Activity | 0.004 | |||
| No | 66.75% | 46.90% | 53.10% | |
| Unable to Do | 0.68% | 39.25% | 60.75% | |
| Yes | 32.57% | 64.57% | 35.43% | |
| Alcohol | 0.400 | |||
| No | 24.14% | 49.56% | 50.44% | |
| Yes | 75.86% | 53.58% | 46.42% | |
| Current Smoker | 0.500 | |||
| No | 16.94% | 45.78% | 54.22% | |
| Yes | 29.24% | 51.48% | 48.52% | |
| AL Risk | ||||
|---|---|---|---|---|
| Characteristic | Overall, N = 25,098,492 | Low, N = 13,203,060 | High, N = 11,895,432 | p-Value |
| AL | 2.55 (0.09) | 1.13 (0.05) | 4.13 (0.08) | <0.001 |
| CSI | 5.06 (0.12) | 4.20 (0.12) | 5.93 (0.12) | <0.001 |
| CSI Risk | <0.001 | |||
| Low | 17.96% | 78.76% | 21.24% | |
| High | 27.04% | 30.91% | 69.09% | |
| CMV IgM | 0.900 | |||
| Negative | 48.26% | 52.11% | 47.89% | |
| Positive | 0.73% | 56.17% | 43.83% | |
| CMV IgG | 0.600 | |||
| Negative | 44.43% | 54.01% | 45.99% | |
| Positive | 55.42% | 51.62% | 48.38% | |
| Toxoplasma IgG Result | 0.500 | |||
| Negative | 88.06% | 52.19% | 47.81% | |
| Positive | 11.94% | 55.63% | 44.37% | |
| Toxoplasma IgG | 12.39 (1.63) | 14.38 (2.62) | 10.19 (1.42) | 0.700 |
| Cancer Antigen 125 | 17.38 (0.75) | 17.01 (1.09) | 17.92 (1.26) | 0.700 |
| Cancer Antigen 15.3 | 2613.28 (404.49) | 2312.76 (550.73) | 3050.47 (659.93) | 0.600 |
| Cancer | 0.600 | |||
| No | 96.27% | 52.83% | 47.17% | |
| Yes | 3.67% | 46.07% | 53.93% | |
| Health Status | 0.005 | |||
| Fair | 10.57% | 43.61% | 56.39% | |
| Excellent | 14.09% | 70.48% | 29.52% | |
| Good | 33.62% | 48.27% | 51.73% | |
| Poor | 2.30% | 26.18% | 73.82% | |
| Very Good | 39.42% | 53.87% | 46.13% | |
| Liver Condition | 0.120 | |||
| No | 96.54% | 53.38% | 46.62% | |
| Yes | 3.35% | 31.12% | 68.88% | |
| Family History of Hypertension/Stroke | 0.400 | |||
| No | 57.06% | 54.45% | 45.55% | |
| Yes | 38.51% | 49.73% | 50.27% | |
| Family History of Diabetes | 0.200 | |||
| No | 46.25% | 55.33% | 44.67% | |
| Yes | 51.90% | 49.99% | 50.01% | |
| Chest Pain | 0.100 | |||
| No | 25.16% | 40.77% | 59.23% | |
| Yes | 10.58% | 30.23% | 69.77% | |
| Shortness of breath on stairs/inclines | 0.120 | |||
| No | 25.79% | 41.40% | 58.60% | |
| Yes | 9.95% | 27.92% | 72.08% | |
| Number of days mental health was not good | 3.83 (0.30) | 3.39 (0.39) | 4.32 (0.53) | 0.200 |
| Number of days physical health was not good | 3.24 (0.30) | 2.62 (0.46) | 3.93 (0.61) | 0.400 |
| CSI Risk | ||||
|---|---|---|---|---|
| Characteristic | Overall, N = 22,862,802 | Low, N = 9,088,249 | High, N = 13,774,553 | p-Value |
| Age | 35.36 (0.36) | 34.23 (0.66) | 36.10 (0.55) | 0.056 |
| Sex | <0.001 | |||
| Female | 45.64% | 47.42% | 52.58% | |
| Male | 54.36% | 33.32% | 66.68% | |
| Race/Ethnicity | <0.001 | |||
| NH White | 71.68% | 44.76% | 55.24% | |
| Mexican American | 8.01% | 27.97% | 72.03% | |
| NH Black | 9.31% | 14.31% | 85.69% | |
| Other and/or multi-racial | 4.53% | 35.76% | 64.24% | |
| Other Hispanic | 6.47% | 38.28% | 61.72% | |
| Annual Income | <0.001 | |||
| $0–$4999 | 4.50% | 25.51% | 74.49% | |
| $10,000–$14,999 | 7.66% | 7.89% | 92.11% | |
| $15,000–$19,999 | 8.70% | 14.62% | 85.38% | |
| Under $20,000 | 0.99% | 4.22% | 95.78% | |
| Over $20,000 | 1.72% | 14.86% | 85.14% | |
| $20,000–$24,999 | 8.62% | 43.40% | 56.60% | |
| $25,000–$34,999 | 12.05% | 50.35% | 49.65% | |
| $35,000–$44,999 | 9.38% | 50.41% | 49.59% | |
| $45,000–$54,999 | 12.50% | 50.99% | 49.01% | |
| $5000–$9999 | 5.23% | 10.03% | 89.97% | |
| $55,000–$64,999 | 6.02% | 55.36% | 44.64% | |
| $65,000–$74,999 | 4.66% | 41.16% | 58.84% | |
| $75,000 and over | 17.97% | 54.24% | 45.76% | |
| CSI Risk | ||||
|---|---|---|---|---|
| Characteristic | Overall, N = 22,862,802 | Low, N = 9,088,249 | High, N = 13,774,553 | p-Value |
| AL | 2.64 (0.13) | 1.44 (0.14) | 3.44 (0.13) | <0.001 |
| AL Risk | <0.001 | |||
| Low | 24.70% | 62.86% | 37.14% | |
| High | 24.70% | 16.95% | 83.05% | |
| CSI | 5.04 (0.07) | 3.38 (0.03) | 6.14 (0.04) | <0.001 |
| HDL | 49.67 (0.47) | 51.84 (1.01) | 48.25 (0.54) | <0.001 |
| Triglycerides | 152.76 (11.16) | 115.71 (11.40) | 177.27 (14.54) | <0.001 |
| Albumin | 25.68 (5.12) | 10.70 (1.72) | 35.62 (7.93) | <0.001 |
| CLCR | 144.20 (4.81) | 125.11 (6.51) | 156.88 (5.66) | <0.001 |
| CRP | 0.39 (0.02) | 0.22 (0.01) | 0.50 (0.03) | <0.001 |
| CMV IgM | 0.009 | |||
| Negative | 48.41% | 34.62% | 65.38% | |
| Positive | 0.81% | 82.60% | 17.40% | |
| CMV IgG | 0.028 | |||
| Negative | 44.18% | 44.63% | 55.37% | |
| Positive | 55.66% | 36.00% | 64.00% | |
| Toxoplasma IgG Result | 0.020 | |||
| Negative | 86.62% | 41.97% | 58.03% | |
| Positive | 13.38% | 25.39% | 74.61% | |
| Toxoplasma IgG | 13.74 (2.06) | 9.94 (3.14) | 16.24 (2.21) | 0.055 |
| Cancer Antigen 125 | 16.19 (0.68) | 16.99 (1.24) | 15.47 (0.88) | 0.200 |
| Cancer Antigen 15.3 | 3469.03 (518.52) | 2890.61 (986.28) | 3993.37 (758.96) | 0.050 |
| Cancer | 0.200 | |||
| No | 96.32% | 40.34% | 59.66% | |
| Yes | 3.49% | 25.77% | 74.23% | |
| Health Status | <0.001 | |||
| Fair | 11.66% | 16.02% | 83.98% | |
| Excellent | 12.03% | 59.96% | 40.04% | |
| Good | 35.97% | 30.57% | 69.43% | |
| Poor | 2.12% | 2.89% | 97.11% | |
| Very Good | 38.22% | 51.32% | 48.68% | |
| Liver Condition | 0.200 | |||
| No | 96.43% | 40.34% | 59.66% | |
| Yes | 3.42% | 24.80% | 75.20% | |
| Family History of Hypertension/Stroke | 0.077 | |||
| No | 60.47% | 44.15% | 55.85% | |
| Yes | 34.98% | 34.43% | 65.57% | |
| Family History of Diabetes | 0.010 | |||
| No | 48.95% | 44.71% | 55.29% | |
| Yes | 48.60% | 35.73% | 64.27% | |
| Chest Pain | 0.800 | |||
| No | 25.54% | 33.18% | 66.82% | |
| Yes | 11.97% | 34.82% | 65.18% | |
| Shortness of breath on stairs/inclines | 0.025 | |||
| No | 27.37% | 37.72% | 62.28% | |
| Yes | 10.14% | 22.88% | 77.12% | |
| Number of days mental health was not good | 4.88 (0.35) | 4.77 (0.45) | 4.95 (0.37) | 0.900 |
| Number of days physical health was not good | 3.54 (0.23) | 2.92 (0.38) | 3.94 (0.39) | 0.100 |
| AL Risk | ||
| Characteristic | OR (2.5%, 97.5%) | p-Values |
| Age | 1.07 (1.01, 1.12) | 0.019 |
| Sex | ||
| Male | 2.18 (1.08, 4.38) | 0.033 |
| Female | Reference | |
| Poverty | ||
| Above | 0.62 (0.21, 1.82) | 0.339 |
| At or Below | Reference | |
| Alcohol | ||
| Yes | 0.37 (0.11, 1.29) | 0.106 |
| No | Reference | |
| Current Smoker | ||
| Yes | 0.72 (0.27, 1.92) | 0.469 |
| No | Reference | |
| Longest OA | ||
| Low | 0.69 (0.31, 1.56) | 0.334 |
| High | Reference | |
| AIC | 312.81 | |
| CSI Risk | ||
| Characteristic | OR (2.5%, 97.5%) | p-Values |
| Age | 1.07 (1.03, 1.11) | 0.002 |
| Sex | ||
| Male | 1.03 (0.60, 1.75) | 0.915 |
| Female | Reference | |
| Alcohol | ||
| Yes | 1.19 (0.45, 3.13) | 0.695 |
| No | Reference | |
| Current Smoker | ||
| Yes | 4.70 (2.65, 8.33) | <0.001 |
| No | Reference | |
| Longest OA | ||
| Low | 0.27 (0.11, 0.65) | 0.008 |
| High | Reference | |
| AIC | 548.84 | |
| AL | CSI | |
|---|---|---|
| Age | ☑ | ☑ |
| Sex | ☑ | X |
| Race/Ethnicity | X | ☑ |
| CMV IgG | X | ☑ |
| Toxoplasma IgG | X | ☑ |
| Chest Pain | X | X |
| Shortness of Breath | X | ☑ |
| Cancer | X | X |
| Health | ☑ | ☑ |
| Liver Condition | X | X |
| FH Diabetes | X | ☑ |
| FH Hypertension/Stroke | X | X |
| Longest Occupation Activity (LOA) | ☑ | ☑ |
| Current Occupational Activity (COA) | X | ☑ |
| EFA Models | CSI | AL | ||||||
|---|---|---|---|---|---|---|---|---|
| Number of Factors | 1 * | 2 * | 3 * | 4 | 1 * | 2 * | 3 * | 4 * |
| SS Loadings | 1.234 | 1.012 | 0.747 | 0.616 | 1.271 | 1.171 | 1.021 | 0.790 |
| Cumulative Variance | 0.123 | 0.225 | 0.299 | 0.361 | 0.127 | 0.244 | 0.346 | 0.425 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hill, M.; Mostafa, S.; Obeng-Gyasi, E. Chronic Stress Indicator: A Novel Tool for Comprehensive Stress Analysis. Int. J. Environ. Res. Public Health 2024, 21, 302. https://doi.org/10.3390/ijerph21030302
Hill M, Mostafa S, Obeng-Gyasi E. Chronic Stress Indicator: A Novel Tool for Comprehensive Stress Analysis. International Journal of Environmental Research and Public Health. 2024; 21(3):302. https://doi.org/10.3390/ijerph21030302
Chicago/Turabian StyleHill, Matthew, Sayed Mostafa, and Emmanuel Obeng-Gyasi. 2024. "Chronic Stress Indicator: A Novel Tool for Comprehensive Stress Analysis" International Journal of Environmental Research and Public Health 21, no. 3: 302. https://doi.org/10.3390/ijerph21030302
APA StyleHill, M., Mostafa, S., & Obeng-Gyasi, E. (2024). Chronic Stress Indicator: A Novel Tool for Comprehensive Stress Analysis. International Journal of Environmental Research and Public Health, 21(3), 302. https://doi.org/10.3390/ijerph21030302