

Community Pharmacy Needle Exchange Programme: What Can Analysis of the Data Tell Us about the Changing Drug Market in Ireland?


Abstract
1. Introduction
2. Materials and Methods
3. Results
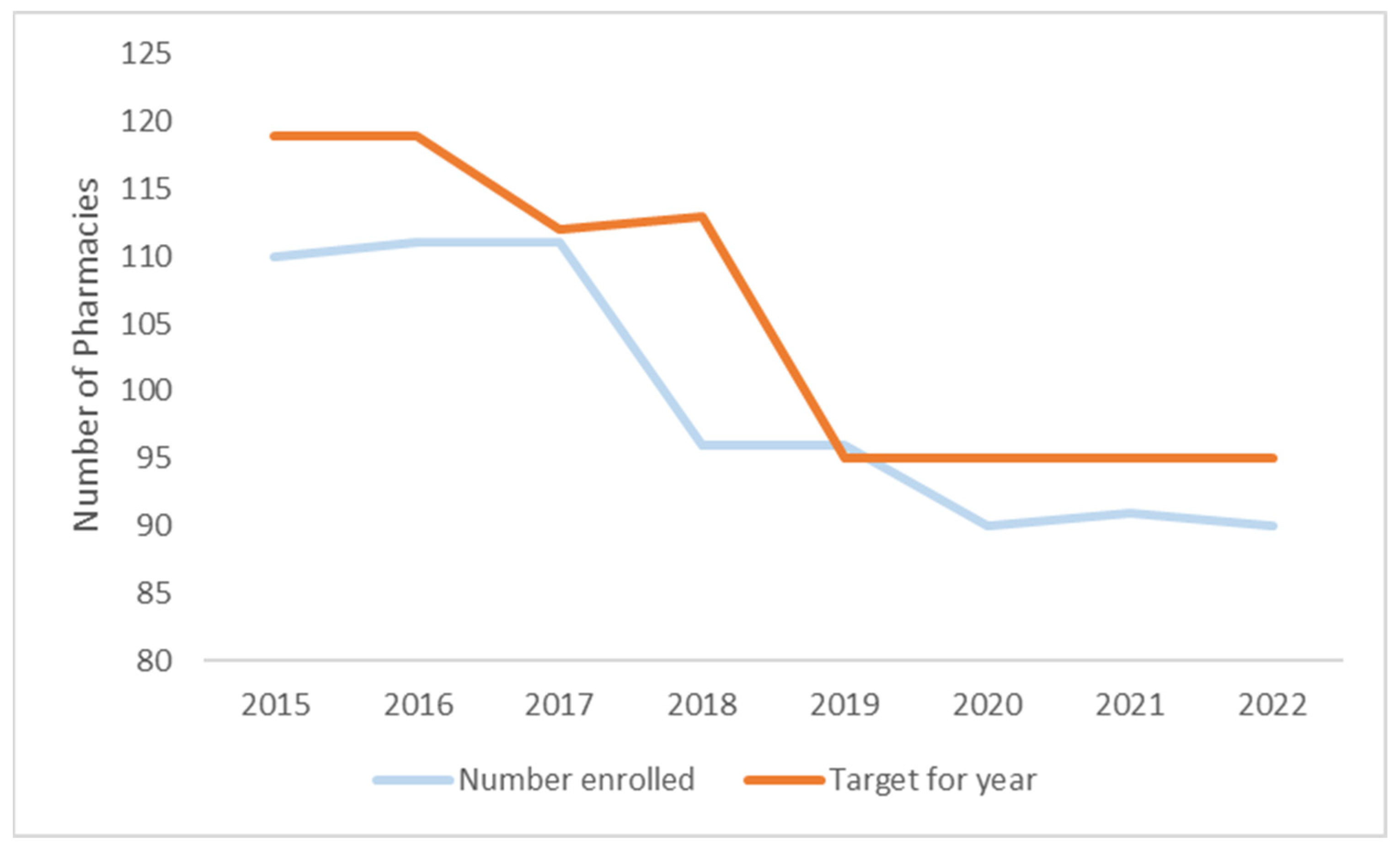
3.1. Number of Pharmacies in Programme
3.2. Number of People Using Programme
3.3. Packs Provided and Returned
3.4. Sterile Needles Provided
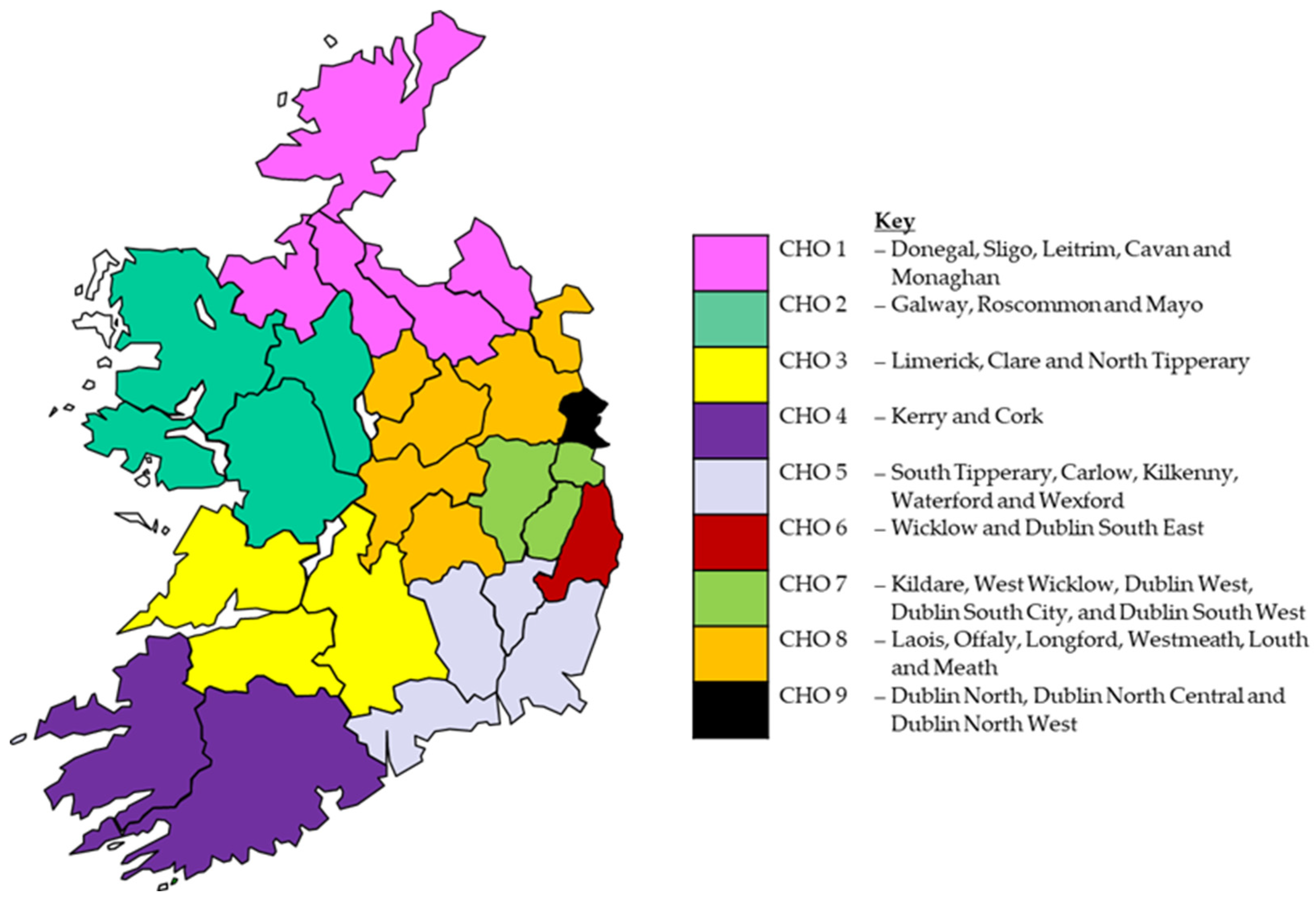
3.5. Regional Comparsions
4. Discussion
4.1. Size and Use of Service
4.2. Packs Returned
4.3. Regional Comparisons
4.4. Comparisons with Other Countries
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wodak, A. Harm reduction is now the mainstream global drug policy. Addiction 2009, 104, 343–345. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, T.; Hedrich, D. Harm Reduction: Evidence, Impacts, and Challenges. In EMCDDA Scientific Monograph Series No 10; European Monitoring Centre for Drugs and Drug Addiction: Luxembourg, 2010. [Google Scholar]
- European Monitoring Centre for Drugs and Drug Addiction. European Drug Report 2023: Trends and Developments; European Monitoring Centre for Drugs and Drug Addiction: Luxembourg, 2023. [Google Scholar]
- Harm Reduction International. The Global State of Harm Reduction 2022; Harm Reduction International: London, UK, 2022. [Google Scholar]
- Crépault, J.-F.; Russell, C.; Watson, T.M.; Strike, C.; Bonato, S.; Rehm, J. What is a public health approach to substance use? A qualitative systematic review and thematic synthesis. Int. J. Drug Policy 2023, 112, 103958. [Google Scholar] [CrossRef] [PubMed]
- Nelson, E.-U. Harm reduction interventions for people who inject drugs. Lancet Glob. Health 2023, 11, e632–e633. [Google Scholar] [CrossRef] [PubMed]
- Hawk, M.; Coulter, R.W.; Egan, J.E.; Fisk, S.; Friedman, M.R.; Tula, M.; Kinsky, S. Harm reduction principles for healthcare settings. Harm Reduct. J. 2017, 14, 70. [Google Scholar] [CrossRef]
- Joint United Nations Programme on HIV/AIDS. Fact Sheet-Latest Global and Regional Statistics on the Status of the AIDS Epidemic; United Nations: New York, NY, USA, 2023. [Google Scholar]
- Degenhardt, L.; Peacock, A.; Colledge, S.; Leung, J.; Grebely, J.; Vickerman, P.; Stone, J.; Cunningham, E.B.; Trickey, A.; Dumchev, K.; et al. Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: A multistage systematic review. Lancet Glob. Health 2017, 5, e1192–e1207. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Summary of Information on the Safety and Effectiveness of Syringe Services Programs (SSPs); Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021. [Google Scholar]
- Kåberg, M.; Karlsson, N.; Discacciati, A.; Widgren, K.; Weiland, O.; Ekström, A.M.; Hammarberg, A. Significant decrease in injection risk behaviours among participants in a needle exchange programme. Infect. Dis. 2020, 52, 336–346. [Google Scholar] [CrossRef]
- Robinson, J.; Gibney, S.; Keane, M.; Long, J. Profile of needle exchange services in Ireland. Drugnet Irel. 2008, 28, 16–17. [Google Scholar]
- Sharp, A.; Barnett, J.T.; Vroom, E.B. Community perceptions of harm reduction and its implications for syringe exchange policy. J. Drug Issues 2020, 50, 507–523. [Google Scholar] [CrossRef]
- Department of Community Rural and Gaeltacht Affairs. National Drugs Strategy (Interim) 2009–2016; Stationery Office: Dublin, Ireland, 2009. [Google Scholar]
- Department of Health, Reducing Harm, Supporting Recovery. A Health-Led Response to Drug and Alcohol Use in Ireland 2017–2025; Drugs Policy Unit, Department of Health: Dublin, Ireland, 2017. [Google Scholar]
- Borges, M.; Gouveia, M.; Fiorentino, F.; Jesus, G.; Cary, M.; Guerreiro, J.P.; Costa, S.; Carneiro, A.V. Costs and consequences of the Portuguese needle-exchange program in community pharmacies. Can. Pharm. J./Rev. Des Pharm. Du Can. 2020, 153, 170–178. [Google Scholar] [CrossRef]
- Long, J.; Doyle, J.; O’Driscoll, D. Pharmacy needle exchange in Ireland. Drugnet Irel. 2014, 49, 19–20. [Google Scholar]
- Thomson, K.; Hillier-Brown, F.; Walton, N.; Bilaj, M.; Bambra, C.; Todd, A. The effects of community pharmacy-delivered public health interventions on population health and health inequalities: A review of reviews. Prev. Med. 2019, 124, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Bingham, T.; Harnedy, N.; O’Driscoll, D.; Keane, R.; Doyle, J. Review of Needle Exchange Provision in Ireland; Health Service Executive: Dublin, Ireland, 2015. [Google Scholar]
- Bates, G.; Van Hout, M.C.; Hearne, E.; Mackridge, A.; McVeigh, J. Evaluation of the Pilot Stage of the Pharmacy Needle Exchange Programme in Ireland; Centre for Public Health Liverpool, John Moores University: Liverpool, UK, 2015. [Google Scholar]
- Mongan, D.; Millar, S.R.; Galvin, B. The 2019-20 Irish National Drug and Alcohol Survey: Main Findings; Health Research Board: Dublin, Ireland, 2021; Available online: https://www.drugsandalcohol.ie/34287/1/HRB_Irish_National_Drug_and_Alcohol_Survey_2019_20.pdf (accessed on 8 February 2024).
- O’Neill, D.; Lyons, S.; Carew, A.M. 2022 Drug Treatment Demand. In HRB Bulletin National Drug Treatment Reporting System; Health Research Board: Dublin, Ireland, 2023. [Google Scholar]
- Health Research Board. Factsheet: Cocaine—The Irish Situation; HRB National Drugs Library: Dublin, Ireland, 2023. [Google Scholar]
- Jarlais, D.C.D.; Sypsa, V.; Feelemyer, J.; Abagiu, A.O.; Arendt, V.; Broz, D.; Chemtob, D.; Seguin-Devaux, C.; Duwve, J.M.; Fitzgerald, M.; et al. HIV outbreaks among people who inject drugs in Europe, North America, and Israel. Lancet HIV 2020, 7, e434–e442. [Google Scholar] [CrossRef]
- McAuley, A.; Palmateer, N.E.; Goldberg, D.J.; Trayner, K.M.A.; Shepherd, S.J.; Gunson, R.N.; Metcalfe, R.; Milosevic, C.; Taylor, A.; Munro, A.; et al. Munro, Re-emergence of HIV related to injecting drug use despite a comprehensive harm reduction environment: A cross-sectional analysis. Lancet HIV 2019, 6, e315–e324. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guide to Starting and Managing Needle and Syringe Programmes; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Hanrahan, M.T.; Millar, S.R.; Phillips, K.P.; Reed, T.E.; Mongan, D.; Perry, I.J. Problematic Opioid Use in IRELAND, 2015–2019; Health Research Board: Dublin, Ireland, 2022; Available online: https://www.drugsandalcohol.ie/35856/1/HRB_CRC_Report-Problematic_opioid_use_in_Ireland_2015-2019.pdf (accessed on 8 February 2024).
- Millar, S. Not-fatal drug-related hospital admissions in Ireland, 2020. Drugnet Irel. 2022, 83, 16–20. [Google Scholar]
- Health Research Board. Health Research Board Reports Latest Drug-Related Deaths Figures. 2023. Available online: https://www.hrb.ie/news/press-releases/single-press-release/article/health-research-board-reports-latest-drug-related-deaths-figures/ (accessed on 8 February 2024).
- Hennigan, K.; Corrigan, N.; Killeen, N.; Scully, M.; Keenan, E. Response of tertiary addictions services to opioid dependence during the COVID-19 pandemic. Ir. J. Psychol. Med. 2021, 38, 301–306. [Google Scholar] [CrossRef]
- Whitfield, M.; Reed, H.; Webster, J.; Hope, V. The impact of COVID-19 restrictions on needle and syringe programme provision and coverage in England. Int. J. Drug Policy 2020, 83, 102851. [Google Scholar] [CrossRef] [PubMed]
- Wiessing, L.; Sypsa, V.; Abagiu, A.O.; Arble, A.; Berndt, N.; Bosch, A.; Buskin, S.; Chemtob, D.; Combs, B.; Conyngham, C.; et al. Conyngham, Impact of COVID-19 & response measures on HIV-HCV prevention services and social determinants in people who inject drugs in 13 sites with recent HIV outbreaks in Europe, North America and Israel. AIDS Behav. 2023, 27, 1140–1153. [Google Scholar]
- Durand, L.; Boland, F.; Harnedy, N.; Delargy, Í.; Scully, M.; Bourke, M.; Ebbitt, W.; Vázquez, M.O.; Keenan, E.; Cousins, G. Cousins, Impact of changes to the delivery of opioid agonist treatment, introduced during the COVID-19 pandemic, on treatment access and dropout in Ireland: An interrupted time series analysis. J. Subst. Use Addict. Treat. 2023, 149, 209029. [Google Scholar] [CrossRef]
- Wang, S.-C.; Maher, B. Substance use disorder, intravenous injection, and HIV infection: A review. Cell Transplant. 2019, 28, 1465–1471. [Google Scholar] [CrossRef]
- Tempalski, B.; Cooper, H.L.; Friedman, S.R.; Jarlais, D.C.D.; Brady, J.; Gostnell, K. Correlates of syringe coverage for heroin injection in 35 large metropolitan areas in the US in which heroin is the dominant injected drug. Int. J. Drug Policy 2008, 19, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Gionfriddo, M.R.; Owens, K.M.; Leist, S.E.; Schrum, L.T.; Covvey, J.R. Attitudes, beliefs, knowledge, and practices for over-the-counter syringe sales in community pharmacies: A systematic review. J. Am. Pharm. Assoc. 2023, 63, 1472–1489. [Google Scholar] [CrossRef] [PubMed]
- Lassi, D.L.S.; Malbergier, A.; Negrão, A.B.; Florio, L.; De Aquino, J.P.; Castaldelli-Maia, J.M. Pharmacological Treatments for Cocaine Craving: What Is the Way Forward? A Systematic Review. Brain Sci. 2022, 12, 1546. [Google Scholar] [CrossRef] [PubMed]
- Laitano, H.V.; Ely, A.; Sordi, A.O.; Schuch, F.B.; Pechansky, F.; Hartmann, T.; Hilgert, J.B.; Wendland, E.M.; Von Dimen, L.; Scherer, J.N.; et al. Scherer, Anger and substance abuse: A systematic review and meta-analysis. Braz. J. Psychiatry 2022, 44, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Lawson, E.; Walthall, H. Barriers to accessing sterile injecting equipment for people who inject drugs: An integrative review. J. Clin. Nurs. 2023, 32, 4502–4514. [Google Scholar] [CrossRef] [PubMed]
- Mc Shane, C. Crack Cocaine Use Amongst Heroin Users Lothian, An Emerging Trend? 2018. Available online: https://www.sdf.org.uk/wp-content/uploads/2018/10/Crack-Cocaine-Use-Amongst-Heroin-Users-in-Lothian-Carmen-McShane-Turning-Point-Scotland.pdf (accessed on 29 November 2023).
- Kimberlin, D.W.; Barnett, E.D.; Lynfield, R.; Sawyer, M.H. Injuries from Needles Discarded in the Community. In Red Book: 2021–2024 Report of the Committee on Infectious Diseases; American Academy of Pediatrics: Itasca, IL, USA, 2021. [Google Scholar]
- Moore, D.L. Needle stick injuries in the community. Paediatr. Child Health 2018, 23, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Osowicki, J.; Curtis, N. Question 2: A pointed question: Is a child at risk following a community-acquired needlestick injury? Arch. Dis. Child. 2014, 99, 1172–1175. [Google Scholar] [CrossRef] [PubMed]
- McCarron, P.; Smyth, B.P. Changes in HIV incidence in people who inject drugs in Ireland from 2000 to 2018: Longitudinal observational study. Addiction 2023, 118, 1177–1181. [Google Scholar] [CrossRef]
- Health Protection Surveillance Centre. Drug-Related Bloodborne Viruses in Ireland; Health Protection Surveillance Centre: Dublin, Ireland, 2018. [Google Scholar]
- Tung, M.; Jackson, J.; Ferreira, C.; Hayden, K.A.; Ens, T. Strategies for addressing needle debris: A scoping review of needle debris and discarded drug paraphernalia associated with substance use. Int. J. Drug Policy 2023, 120, 104183. [Google Scholar] [CrossRef]
- Health and Social Care Board and Public Health Agency. Northern Ireland Needle and Syringe Exchange Service Report; Health and Social Care Board, Public Health Agency: Belfast, Ireland, 2021; Available online: https://www.publichealth.hscni.net/sites/default/files/2021-09/NSES%20Annual%20Report%202019-20.pdf (accessed on 8 February 2024).
- Ksobiech, K. Return rates for needle exchange programs: A common criticism answered. Harm Reduct. J. 2004, 1, 2. [Google Scholar] [CrossRef][Green Version]
- Centers for Disease Control and Prevention. Needs-Based Syringe Distribution and Disposal at Syringe Services Programs, Frequently Asked Questions; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020. [Google Scholar]
- Drugs.ie. Dublin Implements Public Sharps Bins to Tackle Drug-Related Litter. 2016. Available online: https://www.drugs.ie/news/article/dublin_implements_public_sharps_bins_to_tackle_drug_related_litter (accessed on 1 January 2023).
- Paquette, C.E.; Syvertsen, J.L.; Pollini, R.A. Stigma at every turn: Health services experiences among people who inject drugs. Int. J. Drug Policy 2018, 57, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Government of Western Australia. Guideline: Provision of Needle and Syringe Programs (NSP) in Western Australia; Department of Health, State of Western Australia: Perth, Australia, 2022.
- Health Service Executive. HSE 12952—Tender for Pharmacy Needle Exchange Packs to the HSE Pharmacy Needle Exchange Programme. 2022. Available online: https://irl.eu-supply.com/ctm/Supplier/PublicPurchase/219076/0/0?returnUrl=ctm/Supplier/publictenders&b=ETENDERS_SIMPLE (accessed on 29 August 2023).
- Colledge-Frisby, S.; Ottaviano, S.; Webb, P.; Grebely, J.; Wheeler, A.; Cunningham, E.B.; Hajarizadeh, B.; Leung, J.; Peacock, A.; Vickerman, P.; et al. Global coverage of interventions to prevent and manage drug-related harms among people who inject drugs: A systematic review. Lancet Glob. Health 2023, 11, e673–e683. [Google Scholar] [CrossRef] [PubMed]
- Ksobiech, K. Assessing and improving needle exchange programs: Gaps and problems in the literature. Harm Reduct. J. 2004, 1, 4. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| KPIs | Year | |||||||
|---|---|---|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | |
| Number of pharmacies recruited | 119 | 119 | 112 | 113 | 95 | 95 | 95 | 95 |
| Number of individuals per month | 1200 | 1731 | 1647 | 1628 | 1650 | 1894 | 1486 | 1500 |
| Percentage of needle/syringe packs returned | 52 | 41 | 30 | 41 | 41 | 20 | 23 | 19 |
| Average number of clean needles per individual per month | 14 | 14 | 14 | 13 | 13 | 15 | 14 | 14 |
| KPIs | Community Health Organisation Area (CHO) * | |||||
|---|---|---|---|---|---|---|
| CHO1 | CHO2 | CHO3 | CHO4 | CHO5 | CHO8 | |
| Proportional breakdown of pharmacies providing programme 2022 | 10% | 11% | 13% | 18% | 16% | 32% |
| Proportional breakdown of individuals using programme 2022 | 2% | 4% | 3% | 48% | 23% | 20% |
| Percentage change in pharmacies providing programme 2015–2022 | −25% | −17% | −20% | −16% | −22% | −15% |
| Percentage change in individuals using the programme 2015–2022 | −20% | −53% | −84% | 98% | −3% | −27% |
| Mean number of individuals using programme per pharmacy 2022 | 3.5 | 6.4 | 3.6 | 48.4 | 26.5 | 11.3 |
| Proportion of packs returned 2022 | 15% | 6% | 7% | 8% | 21% | 33% |
| Percentage change in the proportion of packs returned per month 2015–2022 | −70% | −66% | −67% | −52% | −23% | 33% |
| Mean number of needles provided per individual per month 2022 | 13.4 | 2.4 | 9.2 | 11.4 | 11.9 | 10.4 |
| Percentage change in mean number of needles provided per individual per month 2015–2022 | −72% | −70% | −34% | −5% | −20% | −31% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evans, D.S.; Harnedy, N.; Keenan, E. Community Pharmacy Needle Exchange Programme: What Can Analysis of the Data Tell Us about the Changing Drug Market in Ireland? Int. J. Environ. Res. Public Health 2024, 21, 289. https://doi.org/10.3390/ijerph21030289
Evans DS, Harnedy N, Keenan E. Community Pharmacy Needle Exchange Programme: What Can Analysis of the Data Tell Us about the Changing Drug Market in Ireland? International Journal of Environmental Research and Public Health. 2024; 21(3):289. https://doi.org/10.3390/ijerph21030289
Chicago/Turabian StyleEvans, David S., Norma Harnedy, and Eamon Keenan. 2024. "Community Pharmacy Needle Exchange Programme: What Can Analysis of the Data Tell Us about the Changing Drug Market in Ireland?" International Journal of Environmental Research and Public Health 21, no. 3: 289. https://doi.org/10.3390/ijerph21030289
APA StyleEvans, D. S., Harnedy, N., & Keenan, E. (2024). Community Pharmacy Needle Exchange Programme: What Can Analysis of the Data Tell Us about the Changing Drug Market in Ireland? International Journal of Environmental Research and Public Health, 21(3), 289. https://doi.org/10.3390/ijerph21030289