

Exploring Trauma- and Violence-Informed Pregnancy Care for Karen Women of Refugee Background: A Community-Based Participatory Study



{kind=link}
{kind=link}
Abstract
1. Introduction
1.1. Background
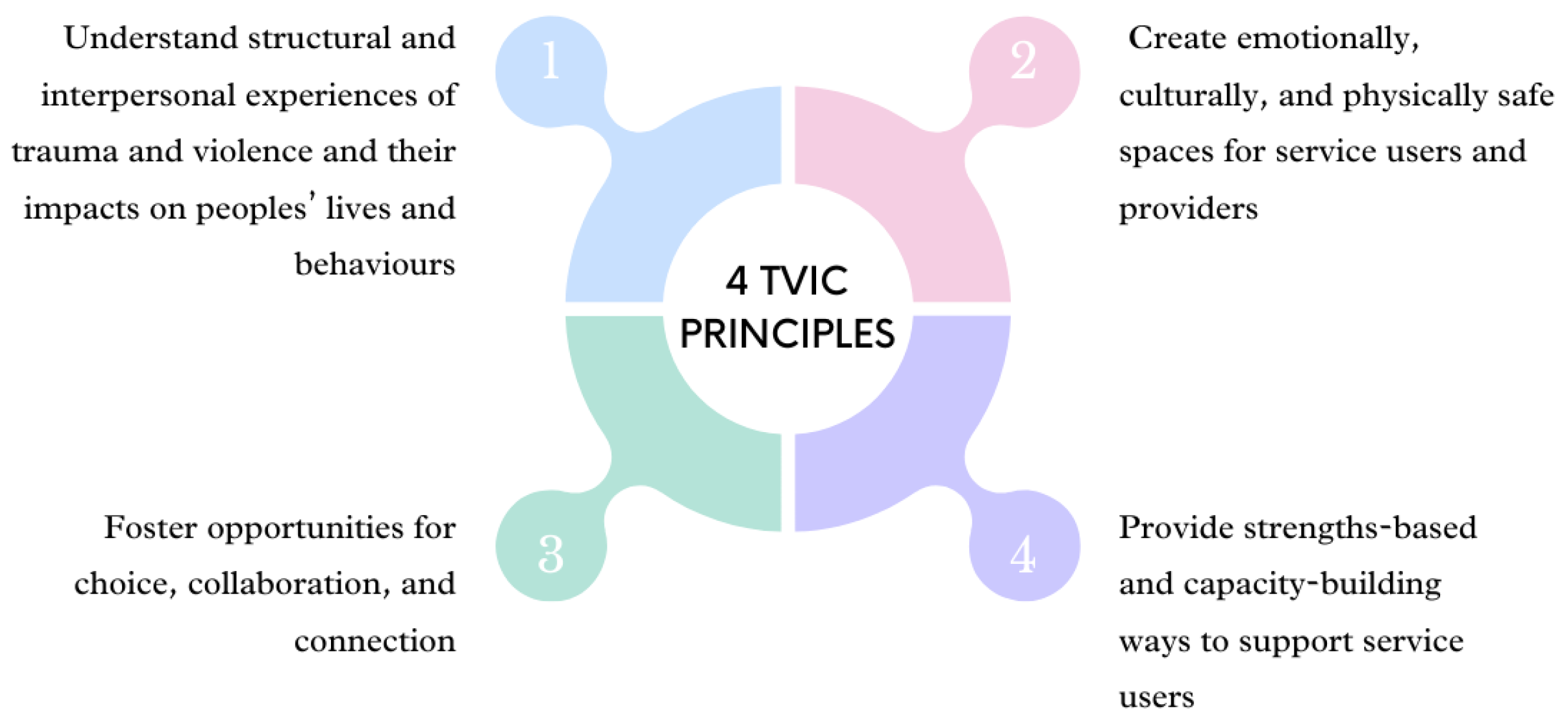
1.1.1. Trauma-Informed Framework
- Understand structural and interpersonal experiences of trauma and violence and their impacts on peoples’ lives and behaviours;
- Create emotionally, culturally, and physically safe spaces for service users and providers;
- Foster opportunities for choice, collaboration, and connection;
- Provide strengths-based and capacity-building ways to support service users.
1.1.2. Karen People of Refugee Background
1.2. Positionality
2. Methods
2.1. Methodology
2.2. Community Advisory Group
2.3. Participants
2.3.1. Inclusion Criteria
2.3.2. Sample
2.3.3. Recruitment
2.3.4. Consent
2.4. Data Collection
- What was your pregnancy care like?
- What did/didn’t you like about it? Why/not?
- Is there something that you wished had been part of your pregnancy care?
- What would have been like if that had been part of your care?
- When you were pregnant, what did you feel that you needed?
- What was it like using interpreter services?
- What do you think every Karen family needs in pregnancy care?
- Was there anything you found difficult when attending your appointments?
2.5. Data Analysis
2.6. Ethics
3. Results
3.1. Care Design and Accessibility
3.1.1. Accessing and Navigating the System
“[my husband] can speak a little bit here and there, so I asked him to let [the hospital] know we cannot make it to our appointment and that we were lost. He just spoke however he could, maybe they could understand him.”—Participant 2
3.1.2. Support Persons
Because we feel alone. Everybody would leave you… You’re just there aimlessly, I feel like I end up with more mental illness. Because you’re alone.—Participant 5
“Some of them looked unfriendly and of course we are scared of them. We already cannot speak their language, of course we feel inferior.”—Participant 5
“So when I have my relatives in the appointment with me they can help me by asking questions and thinking of what to say or talk about. What we can’t think of, they can help think for us and ask for us.”—Participant 7
“… If they make an appointment with me, I will have to take a friend. And they will give me an appointment time that my friend is also available for. That’s how they do it for me.”—Participant 3
3.2. Promoting Choice and Control
3.2.1. Roles and Responsibilities of the Health Professionals
“I thought because they are care providers they will understand and know more than us.”—Participant 6
“It was my fault for not asking them.”—Participant 2
3.2.2. Women Knowing Their Rights
“I don’t know, I want to be able to speak a lot but I don’t know what to say about what we need. I don’t know. I guess we need their help and support…They told me everything I wanted to know. And the things that I didn’t, well I was new and I didn’t know how to ask questions so they told me things, asked me to do things. That’s it.”—Participant 3
3.2.3. Comfort in Good Care
“If a [pregnant woman] feels like their care provider is good, it’s someone who speaks nicely. I feel like when you get a care provider like that, your pain and problems are already half gone.”—Participant 4
3.2.4. When Women Felt Unsafe
“The next time I got pregnant, I knew about it and purposely did not go for a check… It was like I was left [feeling] scared… When I had my daughter, I went for a check after 12 weeks (of pregnancy).”—Participant 4
3.3. Trauma-Informed Interpreting
3.3.1. When There Is No Interpreter
“Something important, I wanted to tell my health professional something, and there’s no one to interpret for me and I couldn’t tell her. I did not feel good.”—Participant 2
“Sometimes when the interpreters don’t come, we have to go back another day.”—Participant 1
3.3.2. Even When There Is an Interpreter
“If [the interpreter’s] tone is nice/friendly then it makes you feel good.”—Participant 5
“If they [interpreter] are being like that then I don’t want to ask questions anymore.”—Participant 7
“The health professional asked me whether I understood the interpreter and I said no, not really, he didn’t accurately interpret what you’re saying and what I’m saying. She said to me: because you couldn’t understand him, I will not call him again. There won’t be any difficult words for you to understand. Your husband will be able to understand also… I felt good.”—Participant 4
“They got an interpreter for me, but the interpreter just talked nonsense, the providers that were looking after me they changed to a new interpreter for me.”—Participant 6
“Well I told them, if you don’t have an interpreter for me, talk to me slowly and that’s what they did so that was fortunate. But I just felt more assured if I had an interpreter, it would be more accurate.”—Participant 5
“And some providers, the interpreter haven’t finished telling us all the information but the providers would stop the interpreter and interrupt them and then they say something to us later and we don’t understand everything. I think it will be a bit harder for those who do not understand it at all.”—Participant 6
“Yes, they interpreted… I still think about it… They asked a lot of questions and I had to sign a lot of things… I didn’t think anything of it at first… I thought it was important… they said I can sign if I wanted but I don’t have to… but I only arrived (in the country) recently so I didn’t understand…”—Participant 1
3.3.3. The Right Match
“for example, a good one is… this [interpreter] spoke to me very well, he speak to me clearly, and he was not fast, he spoke clearly, if you don’t understand he will repeat it for you, and he will check with the health professional as well.”—Participant 7
4. Discussion
4.1. Happy and Safe
4.2. Not Knowing, Power Imbalance, and Re-Traumatisation
4.3. Trauma-Informed Interpreting
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anderson, F.M.; Hatch, S.L.; Comacchio, C.; Howard, L.M. Prevalence and risk of mental disorders in the perinatal period among migrant women: A systematic review and meta-analysis. Arch. Women’s Ment. Health 2017, 20, 449–462. [Google Scholar] [CrossRef]
- Alhasanat, D.; Fry-McComish, J. Postpartum Depression Among Immigrant and Arabic Women: Literature Review. J. Immigr. Minor. Health 2015, 17, 1882–1894. [Google Scholar] [CrossRef]
- Falah-Hassani, K.; Shiri, R.; Vigod, S.; Dennis, C.-L. Prevalence of postpartum depression among immigrant women: A systematic review and meta-analysis. J. Psychiatr. Res. 2015, 70, 67–82. [Google Scholar] [CrossRef]
- Collins, C.H.; Zimmerman, C.; Howard, L.M. Refugee, asylum seeker, immigrant women and postnatal depression: Rates and risk factors. Arch. Women’s Ment. Health 2011, 14, 3–11. [Google Scholar] [CrossRef]
- Heslehurst, N.; Brown, H.; Pemu, A.; Coleman, H.; Rankin, J. Perinatal health outcomes and care among asylum seekers and refugees: A systematic review of systematic reviews. BMC Med. 2018, 16, 89. [Google Scholar] [CrossRef]
- Bollini, P.; Pampallona, S.; Wanner, P.; Kupelnick, B. Pregnancy outcome of migrant women and integration policy: A systematic review of the international literature. Soc. Sci. Med. 2009, 68, 452–461. [Google Scholar] [CrossRef]
- Department of Health. Clinical Practice Guidelines: Pregnancy Care; Australian Government Department of Health: Canberra, Australia, 2020.
- Abdullah, M.; Tuhin, B.; James, S.; Peter, D.S.; McIntyre, H.D.; Karen, T.; Frances, M.B.; Marloes, N.D.; Suhail, D.; Murray, M.; et al. Adverse childhood experiences, the risk of pregnancy complications and adverse pregnancy outcomes: A systematic review and meta-analysis. BMJ Open 2023, 13, e063826. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration. SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2014.
- Sperlich, M.; Seng, J.S.; Li, Y.; Taylor, J.; Bradbury-Jones, C. Integrating Trauma-Informed Care into Maternity Care Practice: Conceptual and Practical Issues. J. Midwifery Womens Health 2017, 62, 661–672. [Google Scholar] [CrossRef] [PubMed]
- Varcoe, C. From Trauma-Informed to Trauma-and Violence-Informed. Available online: https://www.youtube.com/watch?v=qjvMTZZ2GPg (accessed on 26 September 2021).
- Wathen, C.N.; Schmitt, B.; MacGregor, J.C.D. Measuring Trauma- (and Violence-) Informed Care: A Scoping Review. Trauma Violence Abus. 2021, 24, 261–277. [Google Scholar] [CrossRef] [PubMed]
- Wathen, C.N.; Varcoe, C. Trauma- & Violence-Informed Care: Prioritizing Safety for Survivors of Gender-Based Violence; Western University: London, ON, Canada, 2019. [Google Scholar]
- UNHCR. Global Trends Forced Displacement in 2022; UNHCR: Geneva, Switzerland, 2022. [Google Scholar]
- Public Information and Reporting Section. Australia’s Offshore Humanitarian Program: 2021–2022; Department of Home Affairs: Belconnen, Australia, 2022.
- Australian Bureau of Statistics. Cultural Diversity: Census (2021); Australian Bureau of Statistics: Canberra, Australia, 2022.
- Karen Culture and Social Support Foundation. The Karen People. Available online: http://kcssf.org.au/about-us/the-karen-people/ (accessed on 6 October 2023).
- Weis, P. The Refugee Convention, 1951; University of Cambridge: Cambridge, UK, 1951. [Google Scholar]
- Kaplan, I. Rebuilding Shattered Lives: Integrated Trauma Recovery for People of Refugee Background; The Victorian Foundation for Survivors of Torture Inc.: Victoria, Australia, 2020. [Google Scholar]
- Hoffman, S.J.; Vukovich, M.M.; Peden-McAlpine, C.; Robertson, C.L.; Wilk, K.; Wiebe, G.; Gaugler, J.E. Narratives as Borders: Using an Adapted Narrative Approach to Understand the Retelling of the Physical Narratives of Trauma by Karen Women with Refugee Status Resettled in the United States. ANS Adv. Nurs. Sci. 2021, 44, 238–253. [Google Scholar] [CrossRef] [PubMed]
- United Nations General Assembly. Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment; United Nations General Assembly: New York, NY, USA, 1984. [Google Scholar]
- Office of Refugee Resettlement Administration for Children and Families & United States Department of Health and Human Services. Torture Survivors Program (TSP) Eligibility Determination Guidance; Office of Refugee Resettlement: Washington, DC, USA, 2010.
- Guze, S.B. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV). Am. J. Psychiatry 1995, 152, 1228. [Google Scholar] [CrossRef]
- Solberg, Ø.; Sengoelge, M.; Nissen, A.; Saboonchi, F. Coping in Limbo? The Moderating Role of Coping Strategies in the Relationship between Post-Migration Stress and Well-Being during the Asylum-Seeking Process. Int. J. Environ. Res. Public Health 2021, 18, 1004. [Google Scholar] [CrossRef]
- Sudhinaraset, M.; Cabanting, N.; Ramos, M. The health profile of newly-arrived refugee women and girls and the role of region of origin: Using a population-based dataset in California between 2013 and 2017. Int. J. Equity Health 2019, 18, 158. [Google Scholar] [CrossRef] [PubMed]
- Au, M.; Anandakumar, A.D.; Preston, R.; Ray, R.A.; Davis, M. A model explaining refugee experiences of the Australian healthcare system: A systematic review of refugee perceptions. BMC Int. Health Hum. Rights 2019, 19, 22. [Google Scholar] [CrossRef]
- Phillips, J.; Agung-Igusti, R. Bi-Cultural Project; Cohealth: Melbourne, VIC, Australia, 2019. [Google Scholar]
- Tremblay, M.-C.; Martin, D.H.; McComber, A.M.; McGregor, A.; Macaulay, A.C. Understanding community-based participatory research through a social movement framework: A case study of the Kahnawake Schools Diabetes Prevention Project. BMC Public Health 2018, 18, 487. [Google Scholar] [CrossRef]
- Wallerstein, N.B.; Duran, B. Using Community-Based Participatory Research to Address Health Disparities. Health Promot. Pract. 2006, 7, 312–323. [Google Scholar] [CrossRef]
- Wallerstein, N.; Duran, B.; Oetzel, J.G.; Minkler, M. Community-Based Participatory Research for Health: Advancingsocial and Health Equity, 3rd ed.; Jossey-Bass: Hoboken, NJ, USA, 2017. [Google Scholar]
- Minkler, M.; Wallerstein, N. Community-Based Participatory Research for Health: From Process to Outcomes; John Wiley & Sons, Incorporated: Hoboken, NJ, USA, 2008. [Google Scholar]
- Riggs, E.; Davis, E.; Gibbs, L.; Block, K.; Szwarc, J.; Casey, S.; Duell-Piening, P.; Waters, E. Accessing maternal and child health services in Melbourne, Australia: Reflections from refugee families and service providers. BMC Health Serv. Res. 2012, 12, 117. [Google Scholar] [CrossRef] [PubMed]
- Riggs, E.; Yelland, J.; Szwarc, J.; Casey, S.; Chesters, D.; Duell-Piening, P.; Wahidi, S.; Fouladi, F.; Brown, S. Promoting the inclusion of Afghan women and men in research: Reflections from research and community partners involved in implementing a ‘proof of concept’ project. Int. J. Equity Health 2015, 14, 13. [Google Scholar] [CrossRef]
- Patton, M.Q.; Patton, M.Q.; Patton, M.Q. Qualitative Research & Evaluation Methods, 3rd ed.; Sage Publications: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- Liamputtong, P. Qualitative Research Methods, 5th ed.; Oxford University Press: Melbourne, Australia, 2020. [Google Scholar]
- Clarke, V.; Braun, V. Successful Qualitative Research: A Practical Guide for Beginners; Sage Publications: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Braun, V.; Clarke, V. Thematic Analysis: A Practical Guide; Sage: London, UK, 2021. [Google Scholar]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Cook, T.L.; Shannon, P.J.; Vinson, G.A.; Letts, J.P.; Dwee, E. War trauma and torture experiences reported during public health screening of newly resettled Karen refugees: A qualitative study. BMC Int. Health Hum. Rights 2015, 15, 8. [Google Scholar] [CrossRef]
- Vromans, L.; Schweitzer, R.D.; Brough, M.; Asic Kobe, M.; Correa-Velez, I.; Farrell, L.; Murray, K.; Lenette, C.; Sagar, V. Persistent psychological distress in resettled refugee women-at-risk at one-year follow-up: Contributions of trauma, post-migration problems, loss, and trust. Transcult. Psychiatry 2021, 58, 157–171. [Google Scholar] [CrossRef]
- Pangas, J.; Ogunsiji, O.; Elmir, R.; Raman, S.; Liamputtong, P.; Burns, E.; Dahlen, H.G.; Schmied, V. Refugee women’s experiences negotiating motherhood and maternity care in a new country: A meta-ethnographic review. Int. J. Nurs. Stud. 2019, 90, 31–45. [Google Scholar] [CrossRef] [PubMed]
- Johnson, H.; Thompson, A.; Downs, M. Non-Western interpreters’ experiences of trauma: The protective role of culture following exposure to oppression. Ethn. Health 2009, 14, 407–418. [Google Scholar] [CrossRef] [PubMed]
- Freedman, J. Sexual and gender-based violence against refugee women: A hidden aspect of the refugee “crisis”. Reprod Health Matters 2016, 24, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.; Raja, S. Secondary victimization of rape victims: Insights from mental health professionals who treat survivors of violence. Violence Vict. 1999, 14, 261–275. [Google Scholar] [CrossRef]
- Watkins, P.G. “Everybody Suffers”: Karen Refugee Women’s Experiences and Conceptualisations of Wellbeing and Distress. Ph.D. Thesis, University of New South Wales Sydney Australia, Sydney, Australia, 2012. [Google Scholar]
- Sobel, L.; O’Rourke-Suchoff, D.; Holland, E.; Remis, K.; Resnick, K.; Perkins, R.; Bell, S. Pregnancy and Childbirth After Sexual Trauma: Patient Perspectives and Care Preferences. Obstet. Gynecol. 2018, 132, 1461–1468. [Google Scholar] [CrossRef]
- Millar, H.C.; Lorber, S.; Vandermorris, A.; Thompson, G.; Thompson, M.; Allen, L.; Aggarwal, A.; Spitzer, R.F. “No, You Need to Explain What You Are Doing”: Obstetric Care Experiences and Preferences of Adolescent Mothers with a History of Childhood Trauma. J. Pediatr. Adolesc. Gynecol. 2021, 34, 538–545. [Google Scholar] [CrossRef]
- Wathen, C.N.; Varcoe, C. Implementing Trauma- and Violence-Informed Care: A Handbook; University of Toronto Press: Toronto, ON, Canada, 2023. [Google Scholar]
- Farmer, P.; Nizeye, B.; Stulac, S.; Keshavjee, S. Structural Violence and Clinical Medicine. PLoS Med. 2006, 3, e449. [Google Scholar] [CrossRef]
- Bancroft, M.A. Ideology, Ethics and Policy Development in Public Service Interpreting and Translation. In The Voice of Compassion: Exploring Trauma-Informed Interpreting; Carmen, V.-G., Rebecca, T., Eds.; Multilingual Matters: Bristol, UK, 2017; pp. 195–219. [Google Scholar] [CrossRef]
- Riggs, E.; Brown, S.; Szwarc, J.; Nesvadba, N.; Yelland, J. Teach-Back in Interpreter-Mediated Consultations: Reflections from a Case Study. Health Lit. Res. Pract. 2021, 5, e256–e261. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toke, S.; Correa-Velez, I.; Riggs, E. Exploring Trauma- and Violence-Informed Pregnancy Care for Karen Women of Refugee Background: A Community-Based Participatory Study. Int. J. Environ. Res. Public Health 2024, 21, 254. https://doi.org/10.3390/ijerph21030254
Toke S, Correa-Velez I, Riggs E. Exploring Trauma- and Violence-Informed Pregnancy Care for Karen Women of Refugee Background: A Community-Based Participatory Study. International Journal of Environmental Research and Public Health. 2024; 21(3):254. https://doi.org/10.3390/ijerph21030254
Chicago/Turabian StyleToke, Shadow, Ignacio Correa-Velez, and Elisha Riggs. 2024. "Exploring Trauma- and Violence-Informed Pregnancy Care for Karen Women of Refugee Background: A Community-Based Participatory Study" International Journal of Environmental Research and Public Health 21, no. 3: 254. https://doi.org/10.3390/ijerph21030254
APA StyleToke, S., Correa-Velez, I., & Riggs, E. (2024). Exploring Trauma- and Violence-Informed Pregnancy Care for Karen Women of Refugee Background: A Community-Based Participatory Study. International Journal of Environmental Research and Public Health, 21(3), 254. https://doi.org/10.3390/ijerph21030254