

Integrating Mental Health Management into Empowerment Group Sessions for Out-of-School Adolescents in Kenyan Informal Settlements: A Process Paper

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
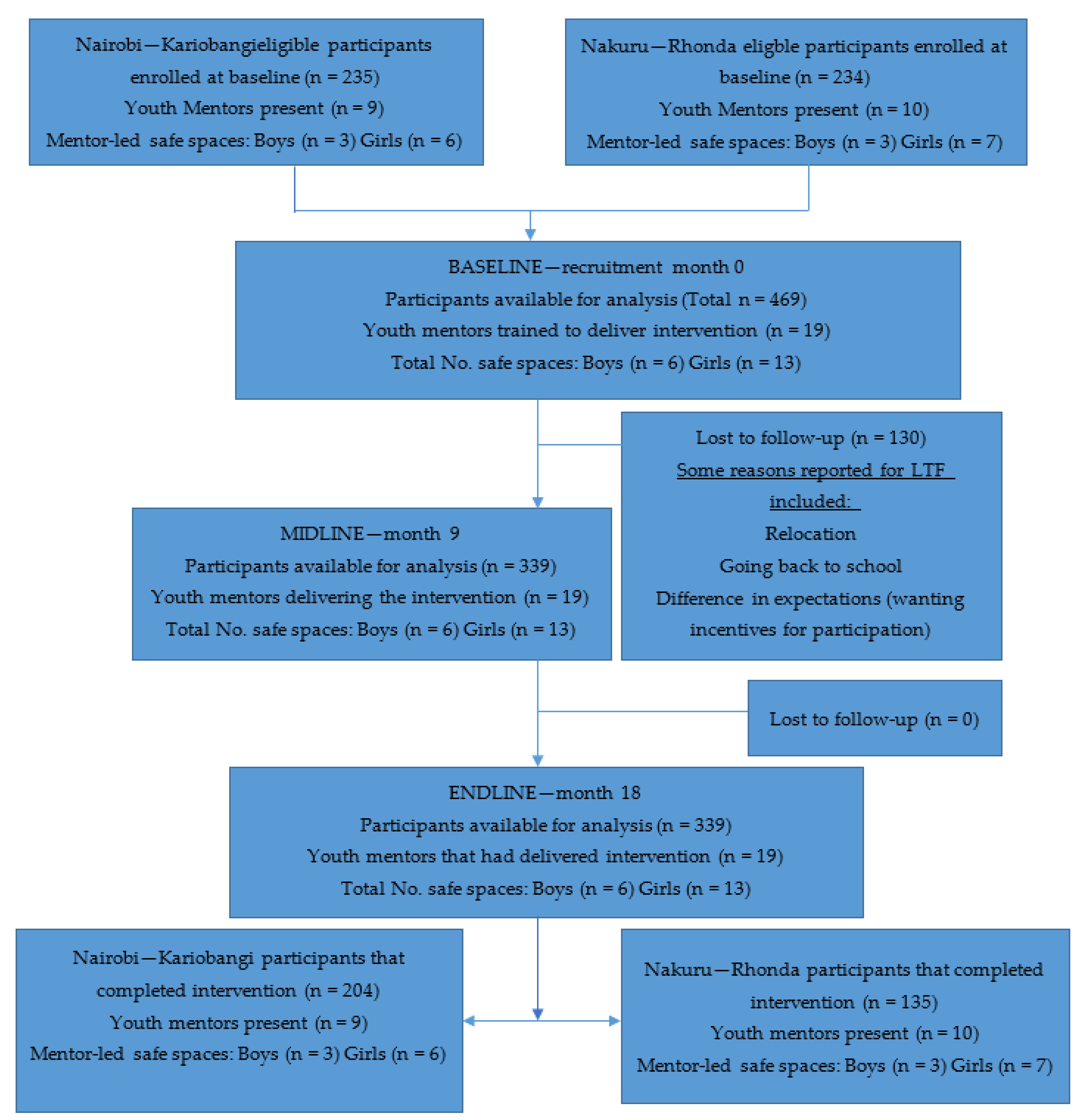
2.2. Participants, Sites, and Design
2.3. Teams Involved in Bridging the Gaps Feasibility Study
2.3.1. The Implementers—Community-Led Organizations
2.3.2. Youth Mentors
2.3.3. Research Team
2.3.4. Mental Health Team
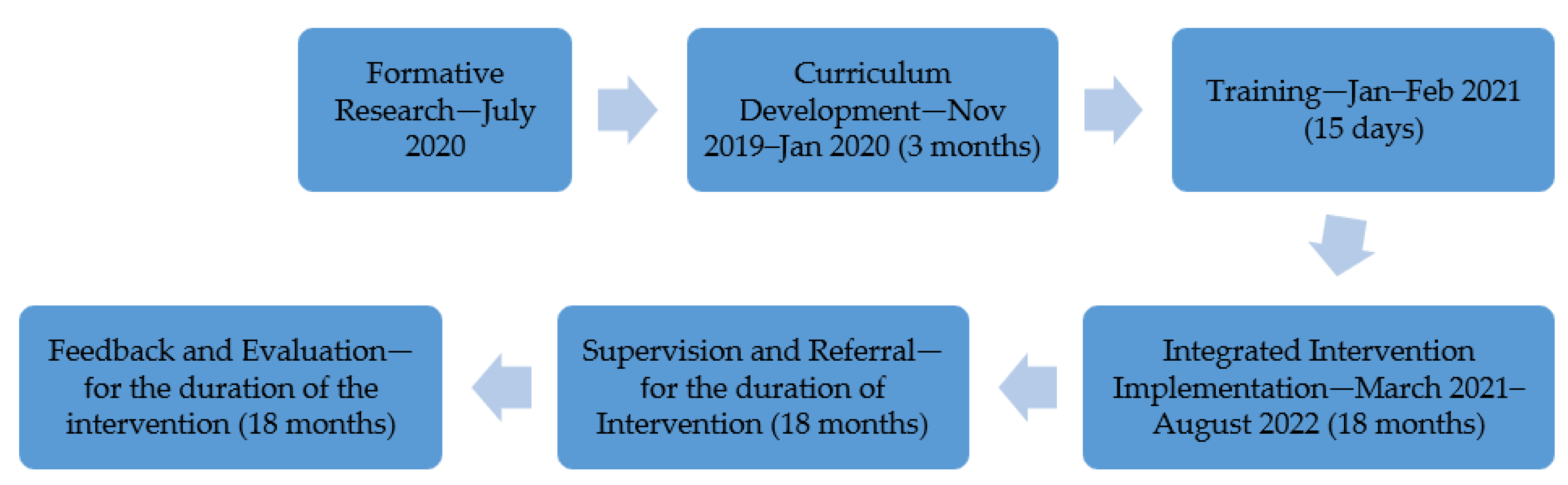
2.4. Phases of the Study
2.4.1. Formative Research
2.4.2. Formation of an External Advisory Group and Consultation
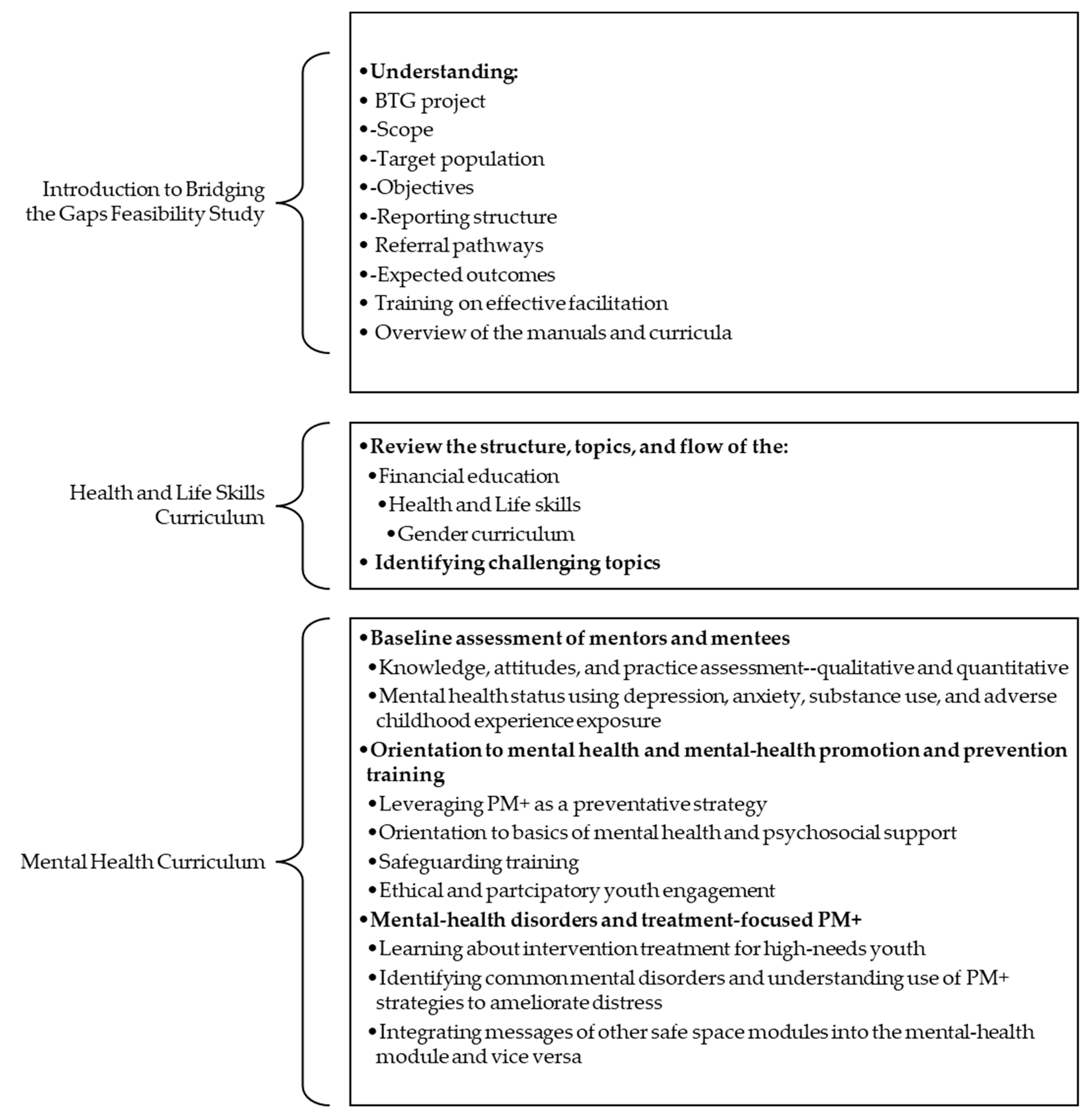
2.4.3. Curriculum Adaptation and Integration
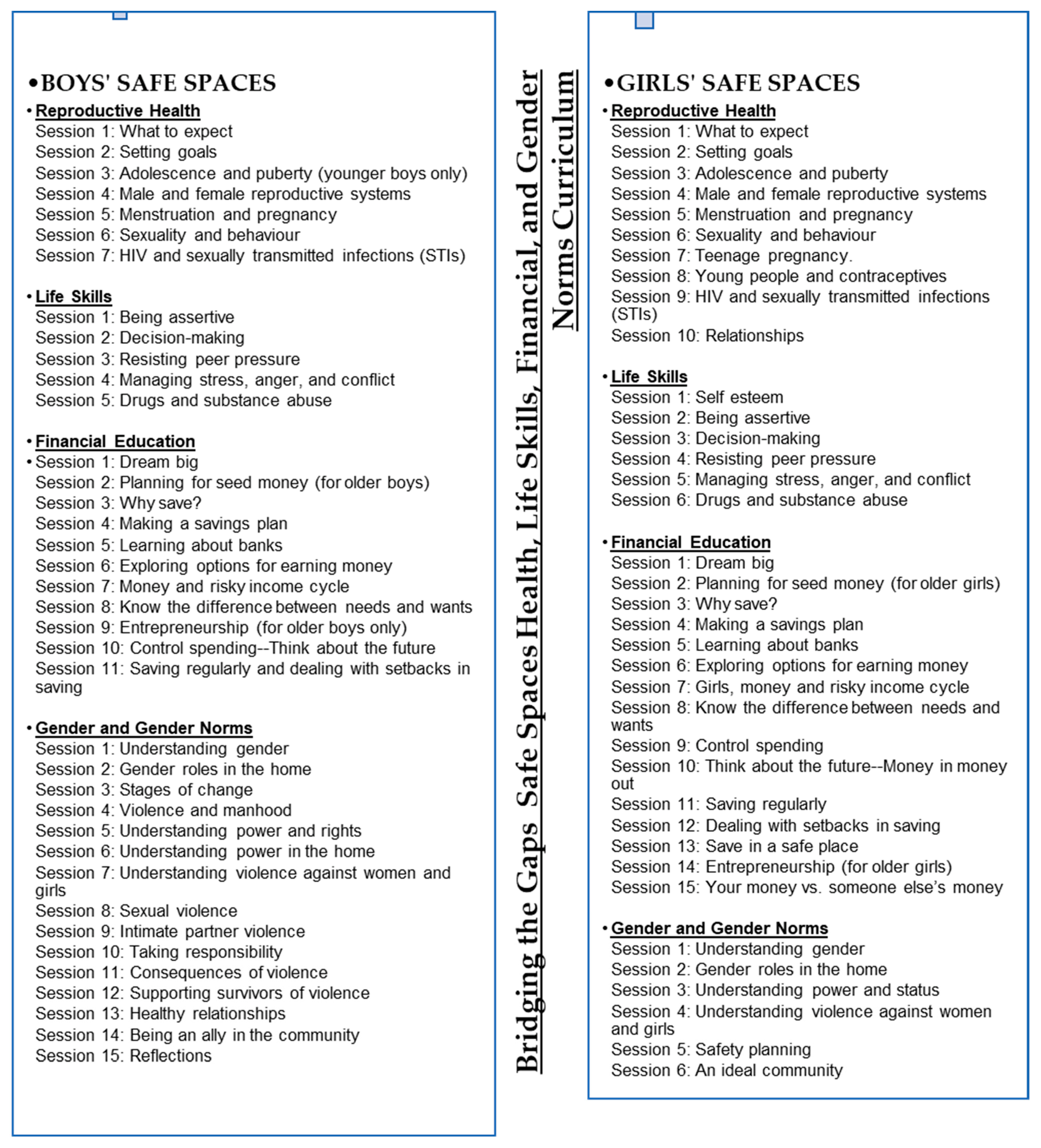
Health and Life Skills Curriculum
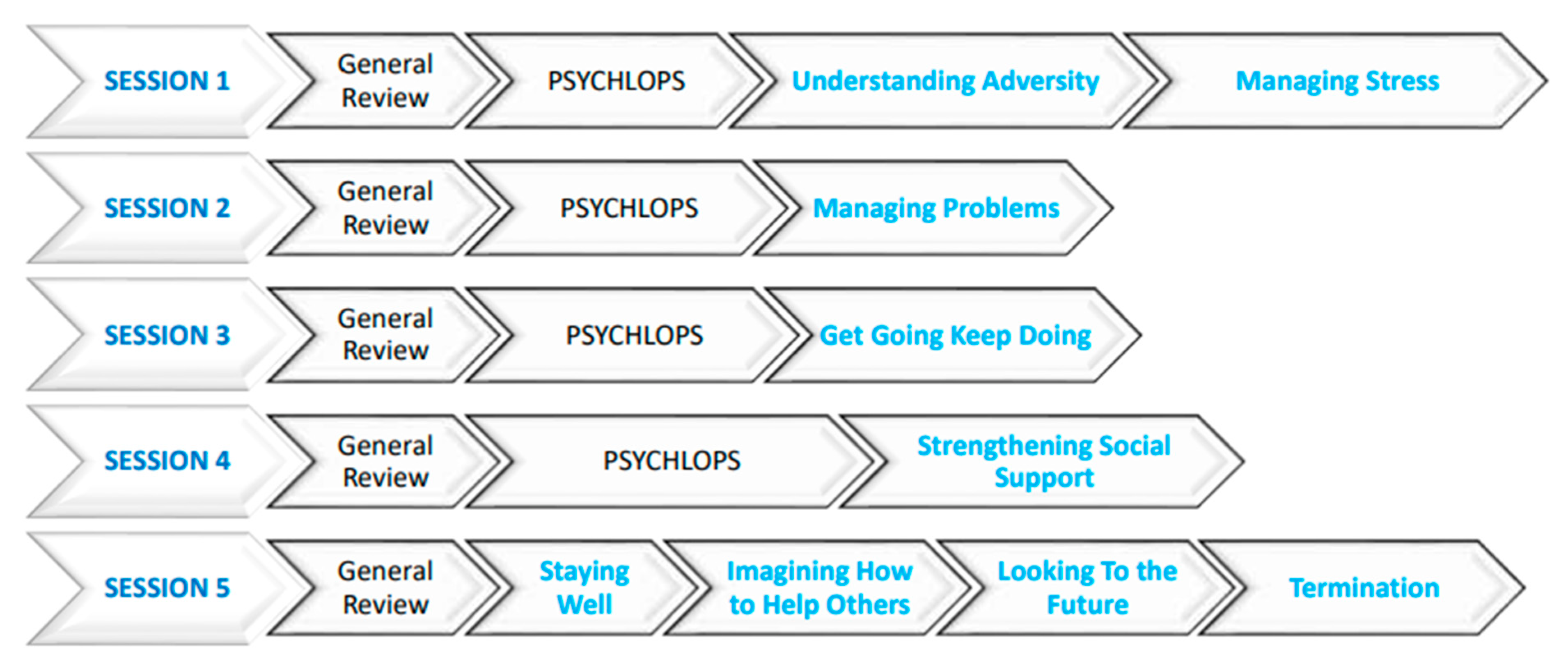
Mental Health Curriculum
2.4.4. Referral Pathway Mapping
2.4.5. Ethical Research Conduct and Child-Safeguarding Procedures
2.4.6. Integrated Curriculum Training and Skills-Building for Youth Mentors
2.4.7. Mental Health Curriculum Refresher Training Mid-Intervention
2.4.8. Integrated Intervention Implementation
Weekly BTG Implementation Update Meetings
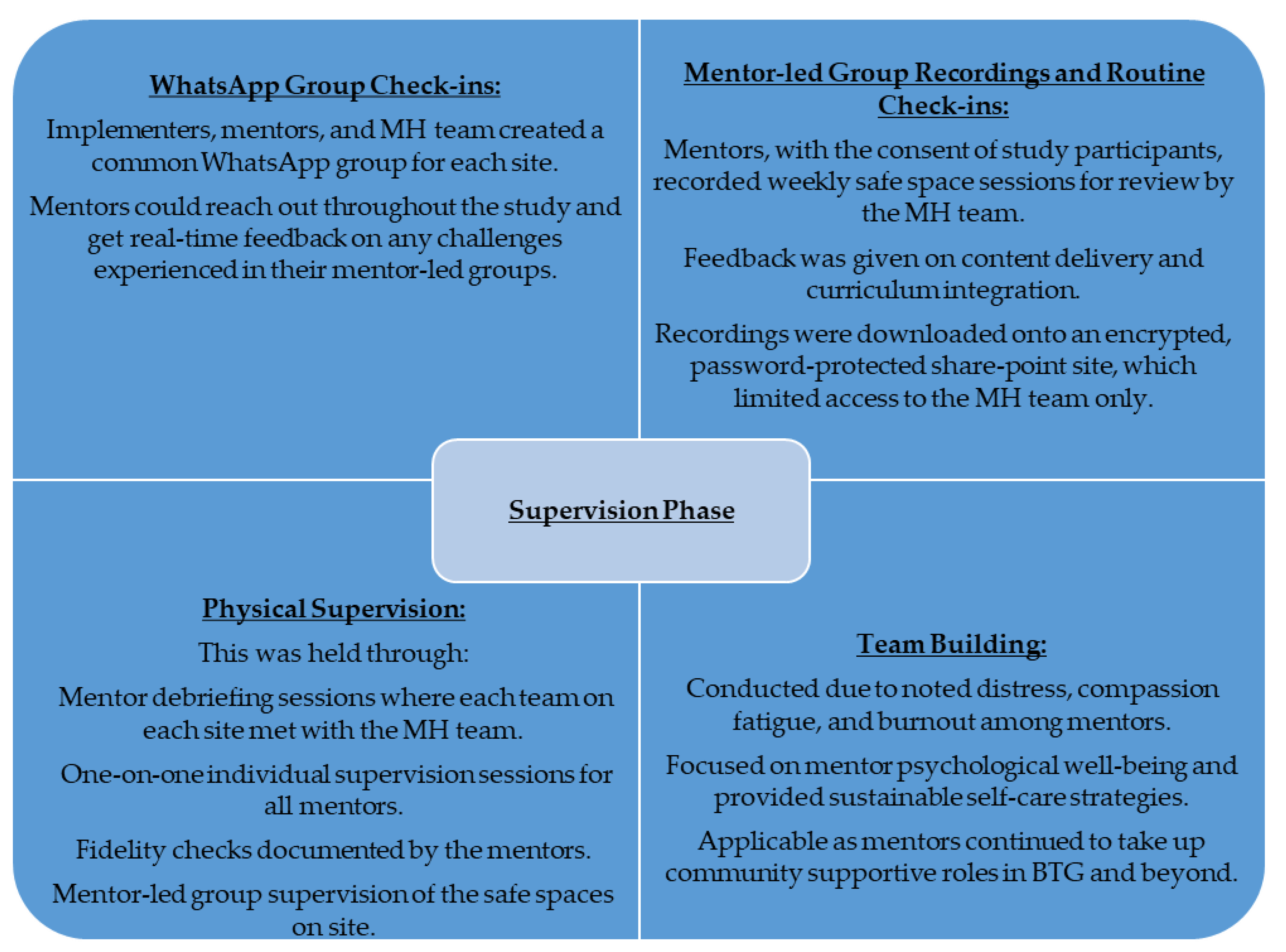
2.4.9. Supervision
2.4.10. Monitoring, Feedback, and Evaluation
3. Process Results Section
3.1. Curricula Restructuring
3.2. Training Outcomes
3.2.1. Youth Mentors
3.2.2. Training Schedule and Modalities
3.3. Study Intervention Integration
3.3.1. Supervision Outcomes
3.3.2. Participant Retention Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patton, G.C.; Sawyer, S.M.; Santelli, J.S.; Ross, D.A.; Afifi, R.; Allen, N.B.; Arora, M.; Azzopardi, P.; Baldwin, W.; Bonell, C.; et al. Lancet Commission on Child health. Lancet 2016, 387, 2423–2478. [Google Scholar] [CrossRef] [PubMed]
- Agyepong, I.A.; Agyepong, I.A.; Sewankambo, N.; Binagwaho, A.; Coll-Seck, A.M.; Corrah, T.; Ezeh, A.; Fekadu, A.; Kilonzo, N.; Lamptey, P.; et al. The path to longer and healthier lives for all Africans by 2030: The Lancet Commission on the future of health in sub-Saharan Africa. Lancet 2017, 390, 2803–2859. [Google Scholar] [CrossRef]
- Nebhinani, N.; Jain, S. Adolescent mental health: Issues, challenges, and solutions. Ann. Indian Psychiatry 2019, 3, 4. [Google Scholar] [CrossRef]
- Musindo, O.; Jafry, S.; Nyamiobo, J.; Becker, K.D.; Gellatly, R.; Maloy, C.; Lozano-Ruiz, A.; Romero-Gonzalez, B.; Kola, L.; Merali, Z.; et al. Mental health and psychosocial interventions integrating sexual and reproductive rights and health, and HIV care and prevention for adolescents and young people (10–24 years) in sub-Saharan Africa: A systematic scoping review. eClinicalMedicine 2023, 57, 101835. [Google Scholar] [CrossRef] [PubMed]
- Davidson, L.L.; Grigorenko, E.L.; Boivin, M.J.; Rapa, E.; Stein, A. A focus on adolescence to reduce neurological, mental health and substance-use disability. Nature 2015, 527, S161–S166. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Bhat, A.; Unützer, J.; Saxena, S. Editorial: Strengthening Child and Adolescent Mental Health (CAMH) Services and Systems in Lower-and-Middle-Income Countries (LMICs). Front. Psychiatry 2021, 12, 10–12. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Huang, K.Y.; Othieno, C.; Wamalwa, D.; Madeghe, B.; Osok, J.; Kahonge, S.N.; Nato, J.; McKay, M.M. Adolescent Pregnancy and Challenges in Kenyan Context: Perspectives from Multiple Community Stakeholders. Glob. Soc. Welf. 2018, 5, 11–27. [Google Scholar] [CrossRef]
- UNICEF. The State of the World ’s Children 2021: On My Mind-Promoting, Protecting and Caring for Children’s Mental Health; UNICEF: New York, NY, USA, 2021. [Google Scholar]
- De Neve, J.W.; Karlsson, O.; Canavan, C.R.; Chukwu, A.; Adu-Afarwuah, S.; Bukenya, J.; Darling, A.M.; Harling, G.; Moshabela, M.; Killewo, J.; et al. Are out-of-school adolescents at higher risk of adverse health outcomes? Evidence from 9 diverse settings in sub-Saharan Africa. Trop. Med. Int. Health 2020, 25, 70–80. [Google Scholar] [CrossRef]
- Belfer, M.L.; Saxena, S. WHO Child Atlas project. Lancet 2006, 367, 551–552. [Google Scholar] [CrossRef]
- Kumar, M.; Mutahi, J.; Kangwana, B. Leave no one behind: Integrated sexual and reproductive, mental health and psychosocial programming for not in employment, education or training (NEET) adolescents and youth in sub-Saharan Africa. BMJ Glob. Health 2023, 8, e013394. [Google Scholar] [CrossRef]
- Castillo, E.G.; Ijadi-Maghsoodi, R.; Shadravan, S.; Moore, E.; Mensah, M.O., 3rd; Docherty, M.; Aguilera Nunez, M.G.; Barcelo, N.; Goodsmith, N.; Halpin, L.E.; et al. Community Interventions to Promote Mental Health and Social Equity. Curr. Psychiatry Rep. 2019, 21, 35. [Google Scholar] [CrossRef]
- Mcleroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An Ecological Perspective on Health Promotion Programs. Health Educ. Behav. 1988, 15, 351–377. [Google Scholar] [CrossRef]
- Faregh, N.; Lencucha, R.; Ventevogel, P.; Dubale, B.W. Considering culture, context and community in mhGAP implementation and training: Challenges and recommendations from the field. Int. J. Ment. Health Syst. 2019, 13, 58. [Google Scholar] [CrossRef] [PubMed]
- Lange-Nielsen, I.I.; Kolltveit, S.; Mousa Thabet, A.A.; Dyregrov, A.; Pallesen, S.; Johnsen, T.B.; Laberg, J.C. Short-Term Effects of a Writing Intervention among Adolescents in Gaza. J. Loss Trauma 2012, 17, 403–422. [Google Scholar] [CrossRef]
- Mabrouk, A.; Mbithi, G.; Chongwo, E.; Too, E.; Sarki, A.; Namuguzi, M.; Atukwatse, J.; Ssewanyana, D.; Abubakar, A. Mental health interventions for adolescents in sub-Saharan Africa: A scoping review. Front. Psychiatry 2022, 13, 937723. [Google Scholar] [CrossRef]
- Simelane, S.R.N.; de Vries, P.J. Child and adolescent mental health services and systems in low and middle-income countries: From mapping to strengthening. Curr. Opin. Psychiatry 2021, 6, 608–616. [Google Scholar] [CrossRef] [PubMed]
- African Population & Health Research Center. Population and Health Dynamics in Nairobi’s Informal Settlements: Report of the Nairobi Cross-Sectional Slums Survey (NCSS) 2012. Nairobi, 2018. Available online: https://aphrc.org/publication/population-and-health-dynamics-in-nairobis-informal-settlements-report-of-the-nairobi-cross-sectional-slums-survey-ncss-2012-2/ (accessed on 22 February 2022).
- Austrian, K.; Soler-Hampejsek, E.; Hewett, P.C.; Hachonda, N.J.; Behrman, J.R. Adolescent Girls Empowerment Programme: Endline Technical Report; Population Council: Lusaka, Zambia, 2018. [Google Scholar]
- Karp, C.; Moreau, C.; Sheehy, G.; Anjur-Dietrich, S.; Mbushi, F.; Muluve, E.; Mwanga, D.; Nzioki, M.; Pinchoff, J.; Austrian, K. Youth Relationships in the Era of COVID-19: A Mixed-Methods Study Among Adolescent Girls and Young Women in Kenya. J. Adolesc. Health 2020, 69, 754–761. [Google Scholar] [CrossRef] [PubMed]
- Wado, Y.D.; Sully, E.A.; Mumah, J.N. Pregnancy and early motherhood among adolescents in five East African countries: A multi-level analysis of risk and protective factors. BMC Pregnancy Childbirth 2019, 19, 59. [Google Scholar] [CrossRef] [PubMed]
- Mwabe, J.; Austrian, K.; Macharia, S. Promises to Keep: Impact of COVID-19 on Adolescents in Kenya. Nairobi, 2021. Available online: https://www.popcouncil.org/uploads/pdfs/2021PGY_ImpactCovidAdolKenya.pdf (accessed on 22 February 2022).
- Triki, T.; Faye, I. Financial Inclusion in Africa; African Development Bank: Tunis Belvédère, Tunisia, 2013. [Google Scholar]
- Kassa, G.M.; Arowojolu, A.O.; Odukogbe, A.A.; Yalew, A.W. Prevalence and determinants of adolescent pregnancy in Africa: A systematic review and Meta-analysis. Reprod. Health 2018, 15, 195. [Google Scholar] [CrossRef] [PubMed]
- Scorgie, F.; Baron, D.; Stadler, J.; Venables, E.; Brahmbhatt, H.; Mmari, K. From fear to resilience: Adolescents’ experiences of violence in inner-city Johannesburg, South Africa. BMC Public Health 2017, 17, 441. [Google Scholar] [CrossRef]
- Temin, M.; Montgomery, M.R.; Engebretsen, S.; Barker, K.M. Girls on the Move: Adolescent Girls & Migration in the Developing World; Population Council: New York, NY, USA, 2013; pp. 1–115. [Google Scholar]
- IECE. Integrated Education for Community Empowerment (IECE). Available online: https://www.iefce.org/about/ (accessed on 22 February 2022).
- REPACTED. Available online: https://rising.globalvoices.org/repacted/about/ (accessed on 22 February 2022).
- Population Council. NISITU (Nisikilize Tujengane) Listen to Me, Let’s Grow Together; Population Council: New York, NY, USA, 2017. [Google Scholar]
- Population Council. NISITU: Engaging Men and Boys in Girl-Centered Programming; Population Council: New York, NY, USA, 2018. [Google Scholar]
- Ka, A. Evaluation of the NISITU Program: A Study to Determine the Effect of a Gender Attitudes and Gender-Based Violence Program for Adolescents in Nairobi, Kenya. 2018. Available online: http://www.isrctn.com/ISRCTN67829143 (accessed on 22 February 2022).
- KARHP; PATH; Population Council. ‘Tuko Pamoja: A Guide for Talking with Young People about Their Reproductive Health.’ Nairobi: Program for Appropriate Technology in Health (PATH); Population Council: New York, NY, USA, 2006. [Google Scholar] [CrossRef]
- International Rescue Committee. Violence Prevention and Response at the International Rescue Committee; International Rescue Committee: New York, NY, USA, 2014. [Google Scholar]
- Dawson, K.S.; Bryant, R.A.; Harper, M.; Tay, A.K.; Rahman, A.; Schafer, A.; Van Ommeren, M. Problem Management Plus (PM+): A WHO transdiagnostic psychological intervention for common mental health problems. World Psychiatry 2015, 14, 354–357. [Google Scholar] [CrossRef]
- Alozkan Sever, C.; Cuijpers, P.; Mittendorfer-Rutz, E.; Bryant, R.A.; Dawson, K.S.; Holmes, E.A.; Mooren, T.; Norredam, M.L.; Sijbrandij, M. Feasibility and acceptability of Problem Management Plus with Emotional Processing (PM + EP) for refugee youth living in the Netherlands: Study protocol Feasibility and acceptability of Problem Management Plus with Emotional. Eur. J. Psychotraumatol. 2021, 12, 1947003. [Google Scholar] [CrossRef] [PubMed]
- Dawson, K.S.; Schafer, A.; Anjuri, D.; Ndogoni, L.; Musyoki, C.; Sijbrandij, M.; van Ommeren, M.; Bryant, R.A. Feasibility trial of a scalable psychological intervention for women affected by urban adversity and gender-based violence in Nairobi. BMC Psychiatry 2016, 16, 410. [Google Scholar] [CrossRef]
- Sijbrandij, M.; Bryant, R.A.; Schafer, A.; Dawson, K.S.; Anjuri, D.; Ndogoni, L.; Ulate, J.; Hamdani, S.U.; van Ommeren, M. Problem Management Plus (PM+) in the treatment of common mental disorders in women affected by gender-based violence and urban adversity in Kenya; study protocol for a randomized controlled trial. Int. J. Ment. Health Syst. 2016, 10, 44. [Google Scholar] [CrossRef] [PubMed]
- Escoffery, C.; Lebow-Skelley, E.; Haardoerfer, R.; Boing, E.; Udelson, H.; Wood, R.; Hartman, M.; Fernandez, M.E. A systematic review of adaptations of evidence-based public health interventions globally. Implement. Sci. 2018, 13, 125. [Google Scholar] [CrossRef]
- Farrer, L.; Gulliver, A.; Chan, J.K.Y.; Batterham, P.J.; Reynolds, J.; Calear, A.; Tait, R.; Bennett, K.; Griffiths, K.M. Technology-Based Interventions for Mental Health in Tertiary Students: Systematic Review. J. Med. Internet Res. 2013, 15, e101. [Google Scholar] [CrossRef] [PubMed]
- Nyongesa, M.K.; Mwangome, E.; Mwangi, P.; Nasambu, C.; Mbuthia, J.W.; Koot, H.M.; Cuijpers, P.; Newton, C.R.J.C.; Abubakar, A. Adaptation, acceptability and feasibility of Problem Management Plus (PM +) intervention to promote the mental health of young people living with HIV in Kenya: Formative mixed-methods research. BJPsych Open 2022, 8, e161. [Google Scholar] [CrossRef]
- Coleman, S.F.; Mukasakindi, H.; Rose, A.L.; Galea, J.T.; Nyirandagijimana, B.; Hakizimana, J.; Bienvenue, R.; Kundu, P.; Uwimana, E.; Uwamwezi, A.; et al. Adapting Problem Management plus for Implementation: Lessons Learned from Public Sector Settings across Rwanda, Peru, Mexico and Malawi. Intervention 2021, 19, 58–66. [Google Scholar] [CrossRef]
- Eaton, J.; Gureje, O.; De Silva, M.; Sheikh, T.L.; Ekpe, E.E.; Abdulaziz, M.; Muhammad, A.; Akande, Y.; Onukogu, U.; Onyuku, T.; et al. A structured approach to integrating mental health services into primary care: Development of the Mental Health Scale Up Nigeria intervention (mhSUN). Int. J. Ment. Health Syst. 2018, 12, 11. [Google Scholar] [CrossRef]
- Molebatsi, K.; Musindo, O.; Ntlantsana, V.; Wambua, G.N. Mental Health and Psychosocial Support During COVID-19: A Review of Health Guidelines in Sub-Saharan Africa. Front. Psychiatry 2021, 12, 571342. [Google Scholar] [CrossRef]
- Semo, B.; Frissa, S.M. The mental health impact of COVID-19. Aust. J. Adv. Nurs. 2020, 37, 1–3. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Curriculum | Original Aspects | Adaptation/Restructuring Made |
|---|---|---|
| Adolescent Girls’ Initiative- Kenya curriculum | Designed for girls aged 11–14 with some topics suitable for only those on the older spectrum Has 4 different packages 3 packages aiming at a combination of multicomponent, multilevel interventions, and 1 focused on a community-level intervention Administered in weekly (1–2 h) group settings led by mentors Provides necessary referral based on need Some sessions allow for guest speakers No payment for participant attendance–voluntary Designed for those in school and out of school Facilitation through discussions, brainstorming, educational games, and role-plays with energizers as needed Has 28 sessions | Divided into 37 sessions |
| Tuko Pamoja curriculum (We Are Together) for Boys and Men | Adolescent reproductive health and life-skills curriculum Incorporates peer mentorship Sessions are divided into different topics that can be handled at different times Administered in weekly group settings | Divided into 38 sessions |
| NISITU curriculum–Engaging Men as Partners | Combination of the first 2 curricula (AGI-K and Tuko Pamoja) An asset-building approach to expand opportunities and reduce vulnerabilities (increase their power in relationships) for adolescent girls Applies the socio-ecological framework Using the theory of change, it aims at engaging boys and men in an evaluation of their attitudes on gender roles and power in relationships with girls and women Empowering boys and men increases their health and financial assets and will help achieve more equitable gender roles and reduce violence against girls and women To be delivered in same-sex safe spaces sessions Have monthly mixed sessions for both adolescent girls and boys Covers: Sexual and reproductive health skills, life skills, gender norms and power relations, and financial education | |
| WHO PM+ | Low-intensity mental-health intervention Aimed at individual adult women facing adversity Have 5 weekly 90 min sessions administered in a particular order Can be facilitated by lay workers Provides handouts and activities to be used between sessions | Adapted for out-of-school adolescents Adapted to be offered in group settings to promote mental wellness and prevent mental illness Incorporated age-appropriate activities for practice between sessions (e.g., Session 3 included playing football, dancing, etc., as behavior-activation activities and Session 1 included thinking about preparing different locally available fruits as a means of managing stress) Group session duration–3 h Groups with up to 8 participants or more The manual included specific case examples for youth mentors to practice integrating the different curricula Change in images and language to contextualize for target population Individualized PM+ adapted to be offered for 1 h weekly sessions by youth mentor |
| Day | Content | Activities | Teams |
|---|---|---|---|
| Day 1 | Introduction to teams Logistics Understanding the Feasibility Study Understanding Mentorship and Facilitation | Sharing documents and contacts Lecture sessions Practice sessions | Population Council REPACTED * IECE * Depending on the site |
| Day 2 and 3 | Pre-assessment Safety Planning Gender and Gender Norms Curriculum Financial Education Curriculum Reproductive Health Curriculum Life Skills Curriculum | Lectures Group Work practical | Population Council REPACTED IECE Depending on the site |
| Day 4 to Day 13 | Introduction to mental health and contextualizing it to the target population Role of mentorship in mental health promotion, prevention, and management Common Mental Disorders among adolescents Identifying and reporting mental ill-health to caregivers Task sharing in mental health WHO PM+ Mapping referral pathways Mental-health supervision Helper self-care for peer support Integrating all curricula | Lectures Group work Individual reflection Role-plays Group work practical | Mental-Health Team |
| Days 14 and 15 | Review of Day 2 and 3 content More practice in integrating the curricula ODK training and practice for participant recruitment | Practice sessions | Population Council REPACTED * IECE * Depending on the site |
| Safe Space Supervisory Report (Prevention, Promotion, and Management of Mental Health) | |||
|---|---|---|---|
| SITE | GROUP PM+ | INDIVIDUAL PM+ (High-Risk Cases) | REFERRALS |
| Rhonda | 19 participants had completed the 5 PM+ safe space sessions | 0 | 2 made as follows: 1-Suicide risk–psychological issues caused by financial stress 1-Financial Issues–Technical training for livelihood |
| 85 participants still had not gone through all the 5 weeks of PM+ sessions | 3 participants were enrolled and sessions were ongoing | 1-Intimate Partner Violence –referred to a rescue home but later relocated to the village 1 adolescent needed to be referred for psychological care as suicidality was likely, based on the Study Team assessment. The youth mentor informed. | |
| Kariobangi | 78 participants had completed all sessions | 0 | 9 referrals were made as follows: 3-antenatal care 2-SGBV care to report and hospital for physical and psychological well-being 2-psychological counseling at Health Centre 1 for economic empowerment at a local organization 1 for legal documentation as they were a foreigner |
| 54 participants still had not gone through the 5 weeks of the curriculum | 7 participants were enrolled and sessions were ongoing | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mutahi, J.; Kangwana, B.; Khasowa, D.; Muthoni, I.; Charo, O.; Muli, A.; Kumar, M. Integrating Mental Health Management into Empowerment Group Sessions for Out-of-School Adolescents in Kenyan Informal Settlements: A Process Paper. Int. J. Environ. Res. Public Health 2024, 21, 223. https://doi.org/10.3390/ijerph21020223
Mutahi J, Kangwana B, Khasowa D, Muthoni I, Charo O, Muli A, Kumar M. Integrating Mental Health Management into Empowerment Group Sessions for Out-of-School Adolescents in Kenyan Informal Settlements: A Process Paper. International Journal of Environmental Research and Public Health. 2024; 21(2):223. https://doi.org/10.3390/ijerph21020223
Chicago/Turabian StyleMutahi, Joan, Beth Kangwana, Dorcas Khasowa, Irene Muthoni, Oliver Charo, Alfred Muli, and Manasi Kumar. 2024. "Integrating Mental Health Management into Empowerment Group Sessions for Out-of-School Adolescents in Kenyan Informal Settlements: A Process Paper" International Journal of Environmental Research and Public Health 21, no. 2: 223. https://doi.org/10.3390/ijerph21020223
APA StyleMutahi, J., Kangwana, B., Khasowa, D., Muthoni, I., Charo, O., Muli, A., & Kumar, M. (2024). Integrating Mental Health Management into Empowerment Group Sessions for Out-of-School Adolescents in Kenyan Informal Settlements: A Process Paper. International Journal of Environmental Research and Public Health, 21(2), 223. https://doi.org/10.3390/ijerph21020223