
Mapping Access to Children’s Hospitals in Texas

 , ,
, ,
Abstract
1. Introduction and Background
2. Data and Methods
2.1. Study Area
2.2. Data
2.3. Methods and Analysis
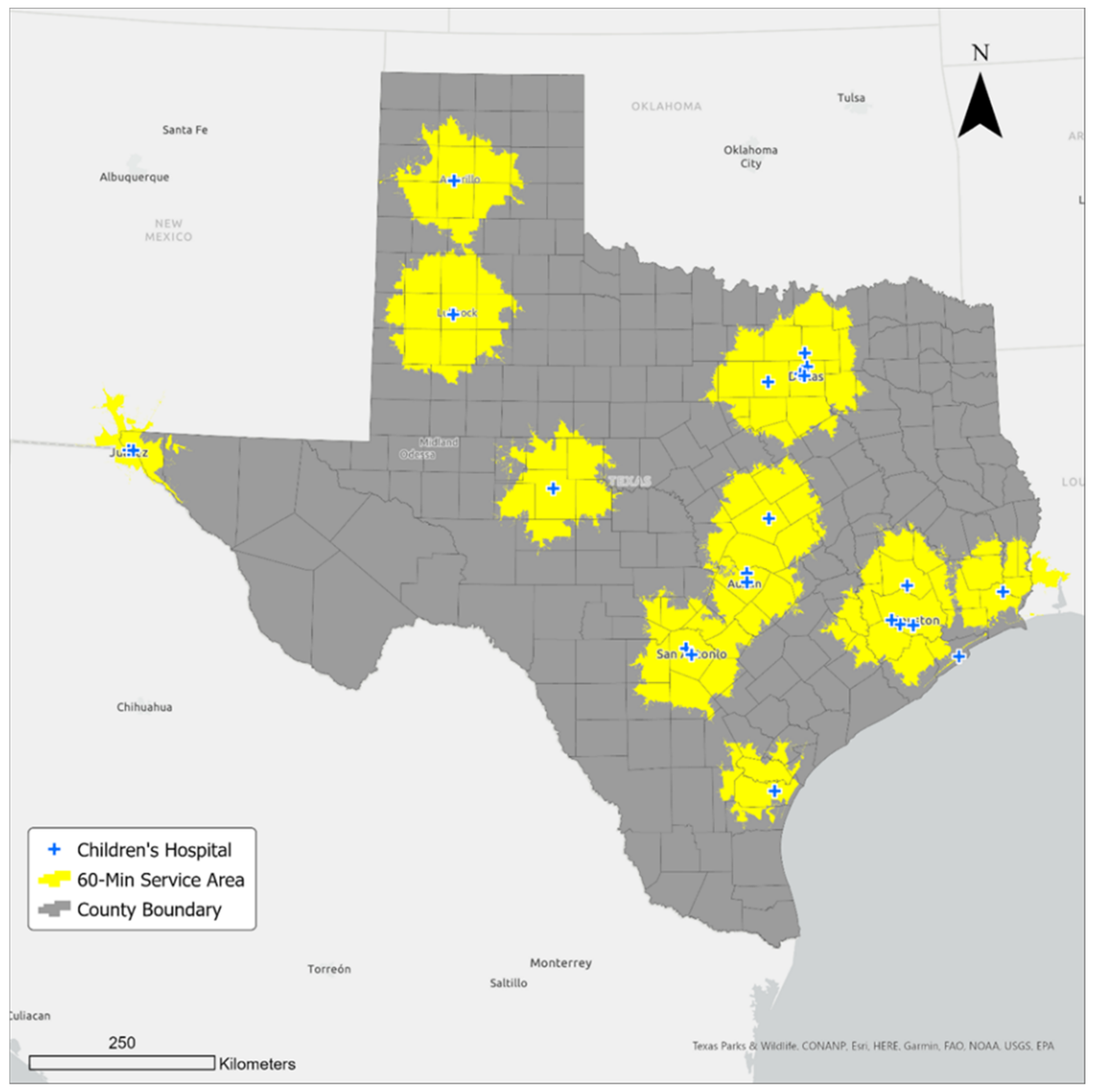
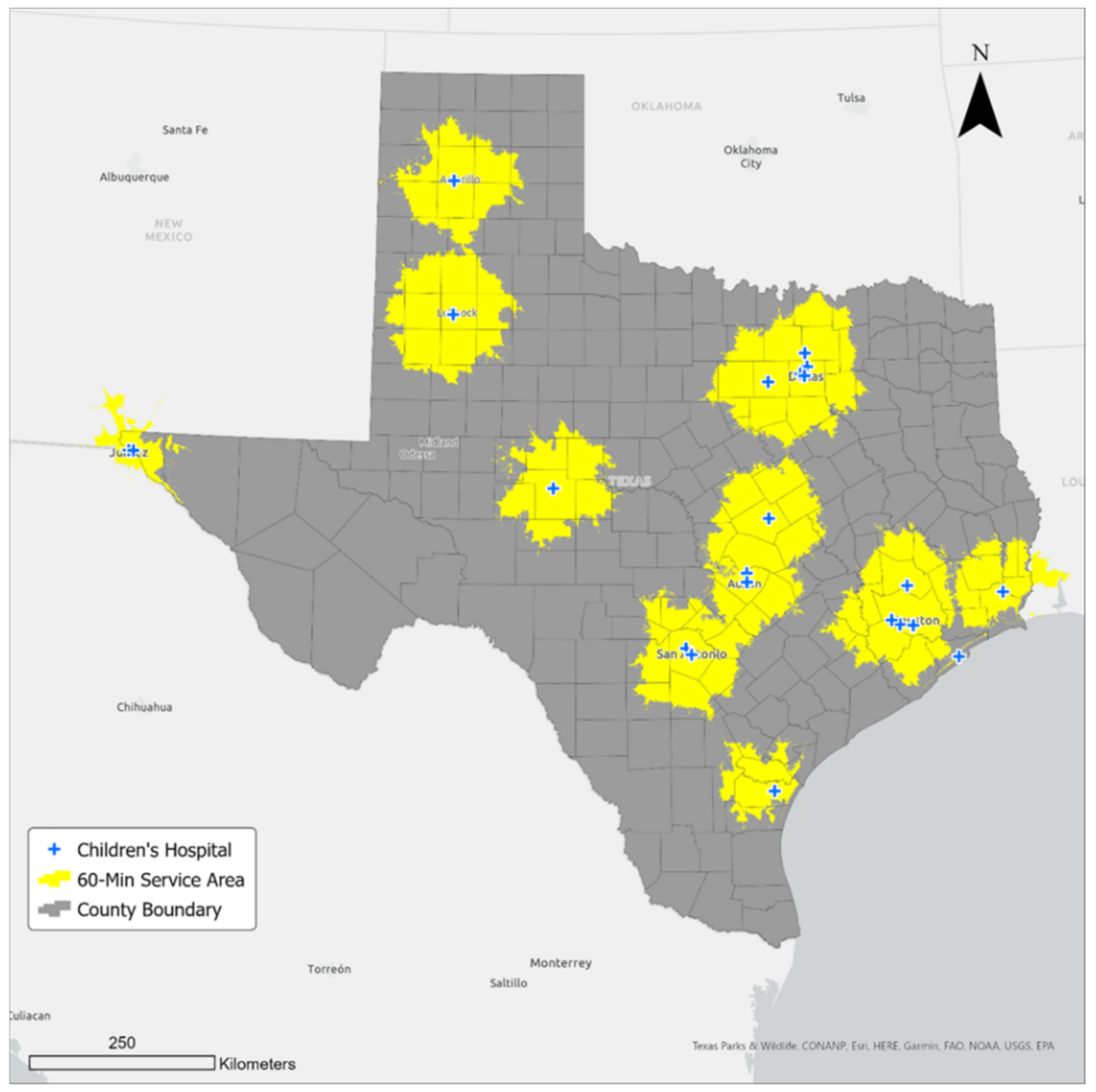
2.3.1. Calculating the Sixty-Minute Service Areas
2.3.2. Calculating Children’s Population within the Sixty-Minute Service Areas
2.3.3. Calculating Hospital Beds per Capita within the Sixty-Minute Service Areas
3. Results
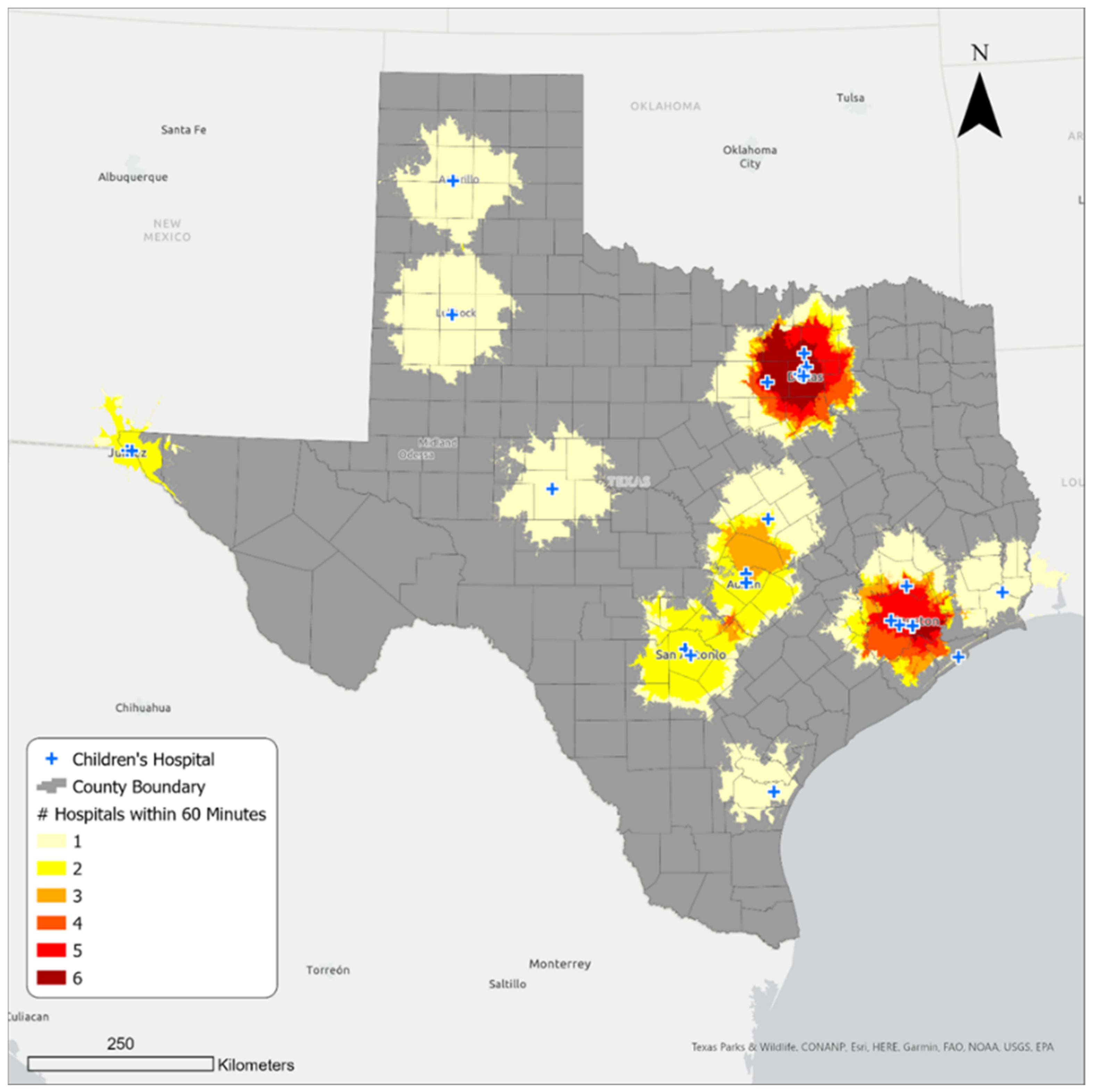
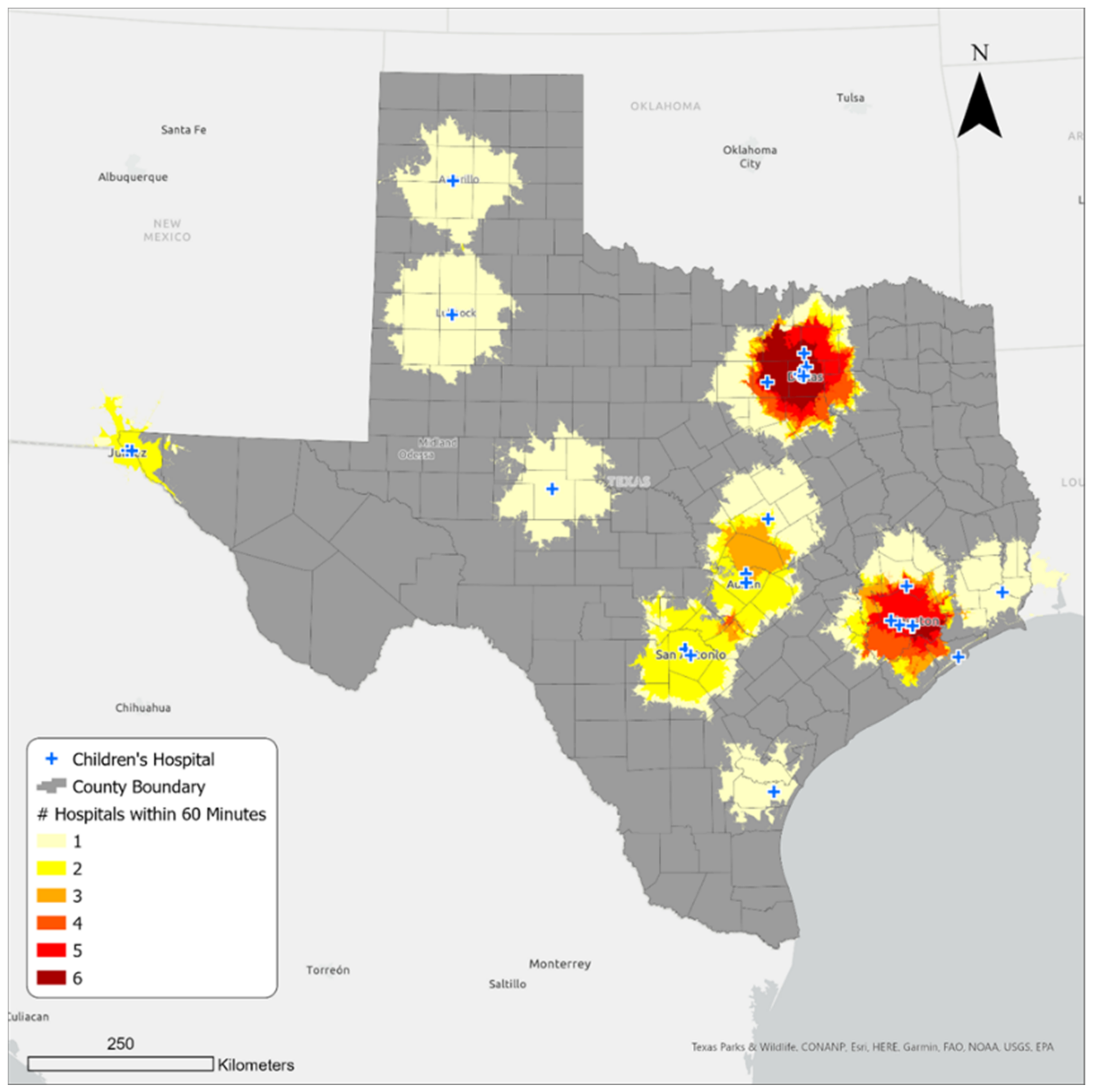
3.1. Geographic Access to Children’s Hospitals
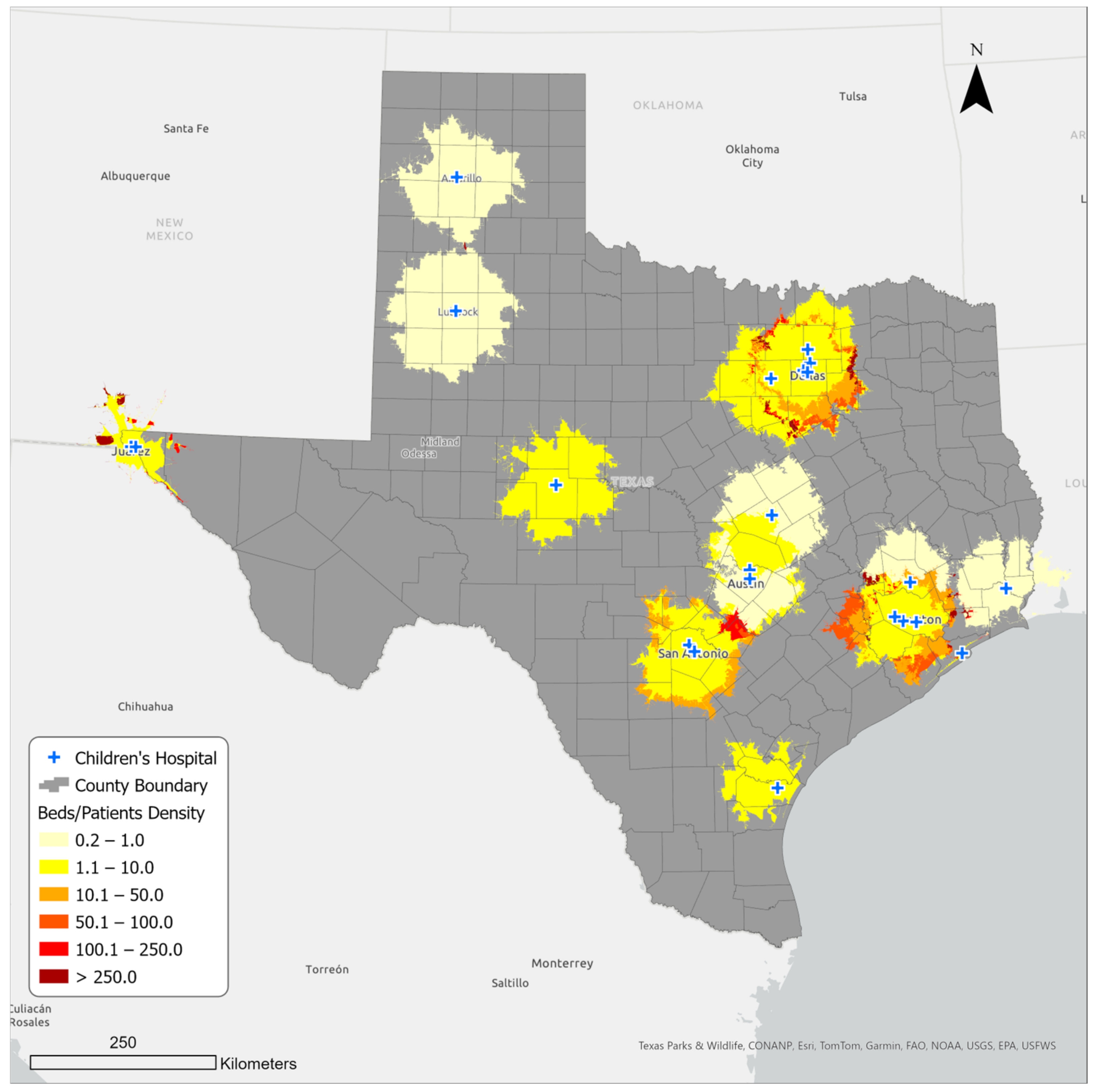
3.2. Bed Availability in Children’s Hospitals in Sixty-Minute Service Areas
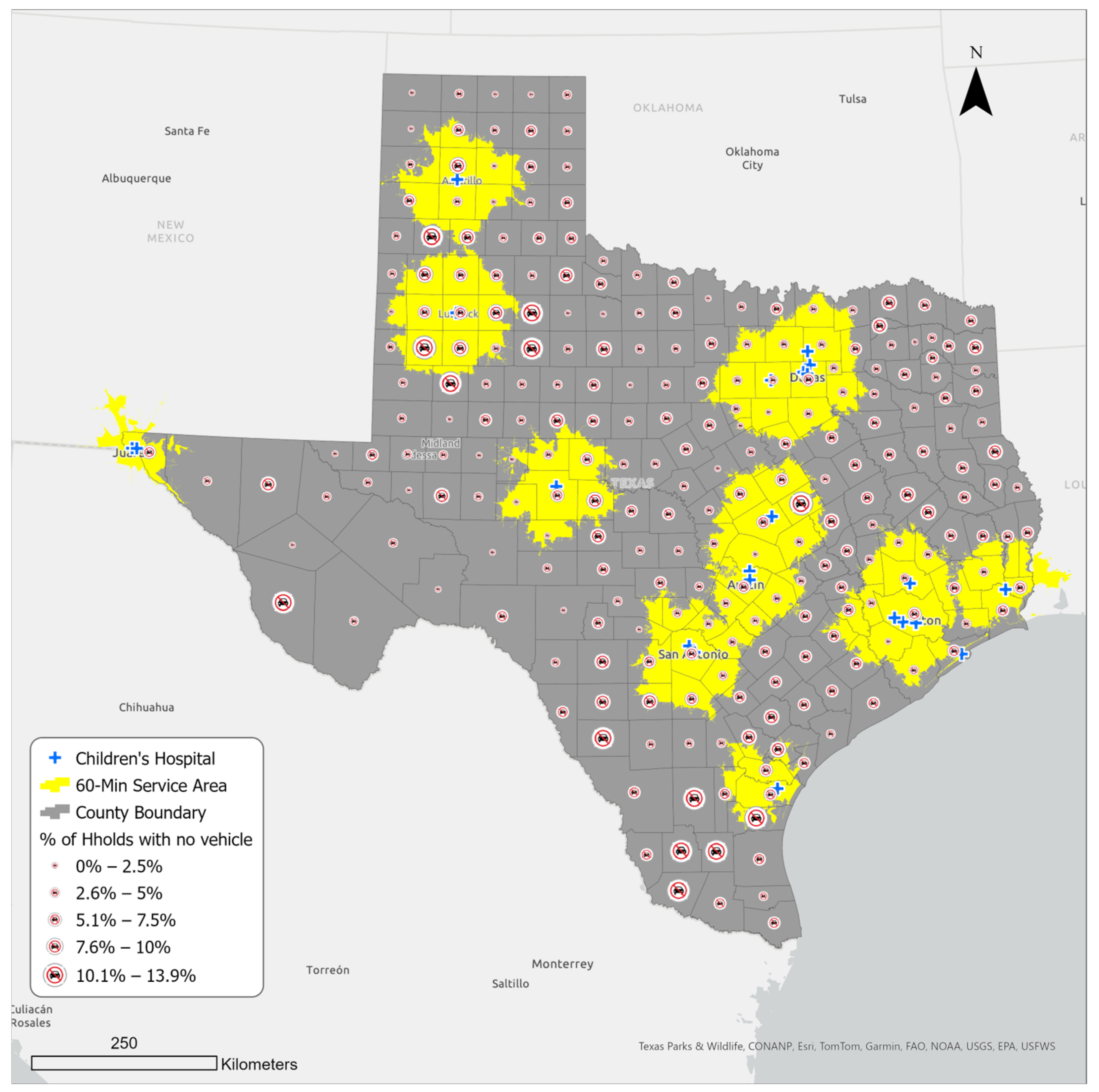
3.3. Household Vehicle Access in Counties within and outside the Sixty-Minute Service Area of a Children’s Hospital
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McDermott, K.W.; Stocks, C.; Freeman, W.J. Overview of Pediatric Emergency Department Visits, 2015; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2018.
- Tregoning, J.S.; Schwarze, J. Respiratory Viral Infections in Infants: Causes, Clinical Symptoms, Virology, and Immunology. Clin. Microbiol. Rev. 2010, 23, 74–98. [Google Scholar] [CrossRef]
- Newgard, C.D.; Lin, A.; Malveau, S.; Cook, J.N.B.; Smith, M.; Kuppermann, N.; Remick, K.E.; Gausche-Hill, M.; Goldhaber-Fiebert, J.; Burd, R.S.; et al. Emergency Department Pediatric Readiness and Short-term and Long-term Mortality Among Children Receiving Emergency Care. JAMA Netw. Open 2023, 6, e2250941. [Google Scholar] [CrossRef]
- França, U.L.; McManus, M.L. Trends in Regionalization of Hospital Care for Common Pediatric Conditions. Pediatrics 2018, 141, e20171940. [Google Scholar] [CrossRef]
- Romo, V. Children’s Hospitals Grapple with a Nationwide Surge in RSV Infections. 2022. Available online: https://www.npr.org/2022/10/24/1130764314/childrens-hospitals-rsv-surge (accessed on 3 December 2023).
- The Texas Tribune. Pediatric Hospitals Short on Beds as Respiratory Illnesses Surge among Children. 2022. Available online: https://www.texastribune.org/2022/10/28/texas-hospitals-children-flu-covid-rsv/ (accessed on 3 December 2023).
- My High Plains. COVID, Flu, and RSV Cases Affecting Rural Texas Hospitals. 2022. Available online: https://www.myhighplains.com/news/local-news/covid-flu-and-rsv-cases-affecting-rural-texas-hospitals/ (accessed on 3 December 2023).
- Patrick, S.W.; Davis, M.M.; Lehmann, C.U.; O Cooper, W. Increasing incidence and geographic distribution of neonatal abstinence syndrome: United States 2009 to 2012. J. Perinatol. 2015, 35, 650–655. [Google Scholar] [CrossRef]
- Quattrochi, J.P.; Hill, K.; Salomon, J.A.; Castro, M.C. The effects of changes in distance to nearest health facility on under-5 mortality and health care utilization in rural Malawi, 1980–1998. BMC Health Serv. Res. 2020, 20, 899. [Google Scholar] [CrossRef]
- Núñez, A.; Sreeganga, S.D.; Ramaprasad, A. Access to Healthcare during COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 2980. [Google Scholar] [CrossRef]
- Fullman, N.; Yearwood, J.; Abay, S.M.; Abbafati, C.; Abd-Allah, F.; Abdela, J.; Chang, H.Y. Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations: A systematic analysis from the Global Burden of Disease Study 2016. Lancet 2018, 391, 2236–2271. [Google Scholar] [CrossRef]
- Wendt, C. Mapping European healthcare systems: A comparative analysis of financing, service provision and access to healthcare. J. Eur. Soc. Policy 2009, 19, 432–445. [Google Scholar] [CrossRef]
- Maaz, M.; Papanastasiou, A. Determining the optimal capacity and occupancy rate in a hospital: A theoretical model using queuing theory and marginal cost analysis. Manag. Decis. Econ. 2020, 41, 1305–1311. [Google Scholar] [CrossRef]
- Weiss, D.J.; Nelson, A.; Vargas-Ruiz, C.A.; Gligorić, K.; Bavadekar, S.; Gabrilovich, E.; Bertozzi-Villa, A.; Rozier, J.; Gibson, H.S.; Shekel, T.; et al. Global maps of travel time to healthcare facilities. Nat. Med. 2020, 26, 1835–1838. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Li, S.; Liu, D. Unequable spatial accessibility to hospitals in developing megacities: New evidence from Beijing. Health Place 2020, 65, 102406. [Google Scholar] [CrossRef]
- Carrasco-Escobar, G.; Manrique, E.; Tello-Lizarraga, K.; Miranda, J.J. Travel Time to Health Facilities as a Marker of Geographical Accessibility Across Heterogeneous Land Coverage in Peru. Front. Public Health 2020, 8, 498. [Google Scholar] [CrossRef]
- Barbieri, S.; Jorm, L. Travel times to hospitals in Australia. Sci. Data 2019, 6, 248. [Google Scholar] [CrossRef]
- Mattson, J. Transportation, Distance, and Health Care Utilization for Older Adults in Rural and Small Urban Areas. Transp. Res. Rec. J. Transp. Res. Board 2011, 2265, 192–199. [Google Scholar] [CrossRef]
- Billi, J.E.; Pai, C.-W.; Spahlinger, D.A. The effect of distance to primary care physician on health care utilization and disease burden. Health Care Manag. Rev. 2007, 32, 22–29. [Google Scholar] [CrossRef]
- Oldenburg, C.E.; for the Étude CHAT Study Group; Sié, A.; Ouattara, M.; Bountogo, M.; Boudo, V.; Kouanda, I.; Lebas, E.; Brogdon, J.M.; Lin, Y.; et al. Distance to primary care facilities and healthcare utilization for preschool children in rural northwestern Burkina Faso: Results from a surveillance cohort. BMC Health Serv. Res. 2021, 21, 212. [Google Scholar] [CrossRef]
- Kelly, C.; Hulme, C.; Farragher, T.; Clarke, G. Are differences in travel time or distance to healthcare for adults in global north countries associated with an impact on health outcomes? A systematic review. BMJ Open 2016, 6, e013059. [Google Scholar] [CrossRef]
- Schoeps, A.; Gabrysch, S.; Niamba, L.; Sié, A.; Becher, H. The Effect of Distance to Health-Care Facilities on Childhood Mortality in Rural Burkina Faso. Am. J. Epidemiol. 2011, 173, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Buor, D. Distance as a predominant factor in the utilisation of health services in the Kumasi metropolis, Ghana. GeoJournal 2002, 56, 145–157. [Google Scholar] [CrossRef]
- Goddard, M.; Smith, P. Equity of Access to Health Care (No. 032cheop); Centre for Health Economics, University of York: Yorkshire, UK, 1998. [Google Scholar]
- Pun-Cheng, L.S. Distance decay. In International Encyclopedia of Geography: People, the Earth, Environment and Technology: People, the Earth, Environment and Technology; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2016; pp. 1–5. [Google Scholar]
- Rojas-Gualdrón, D.F.; Caicedo-Velázquez, B. Distancia al centro de atención en salud y mortalidad durante los primeros años de vida: Revisión sistemática y metaanálisis. Rev. Fac. Nac. Salud Pública 2017, 35, 420–431. [Google Scholar] [CrossRef]
- Doi, S.; Ide, H.; Takeuchi, K.; Fujita, S.; Takabayashi, K. Estimation and Evaluation of Future Demand and Supply of Healthcare Services Based on a Patient Access Area Model. Int. J. Environ. Res. Public Health. 2017, 14, 1367. [Google Scholar] [CrossRef]
- Gausche-Hill, M.; Ely, M.; Schmuhl, P.; Telford, R.; Remick, K.E.; Edgerton, E.A.; Olson, L.M. A National Assessment of Pediatric Readiness of Emergency Departments. JAMA Pediatr. 2015, 169, 527–534. [Google Scholar] [CrossRef]
- Cushing, A.M.; Bucholz, E.M.; Chien, A.T.; Rauch, D.A.; Michelson, K.A. Availability of Pediatric Inpatient Services in the United States. Pediatrics 2021, 148, e2020041723. [Google Scholar] [CrossRef]
- Chien, A.T.; Pandey, A.; Lu, S.; Bucholz, E.M.; Toomey, S.L.; Cutler, D.M.; Beaulieu, N.D. Pediatric Hospital Services Within a One-Hour Drive: A National Study. Pediatrics 2020, 146, e20201724. [Google Scholar] [CrossRef]
- Rees, C.P.; Hawkesworth, S.; Moore, S.E.; Dondeh, B.L.; Unger, S.A. Factors affecting access to healthcare: An observational study of children under 5 years of age presenting to a rural Gambian primary healthcare centre. PLoS ONE 2016, 11, e0157790. [Google Scholar] [CrossRef]
- Tanser, F.; Gijsbertsen, B.; Herbst, K. Modelling and understanding primary health care accessibility and utilization in rural South Africa: An exploration using a geographical information system. Soc. Sci. Med. 2006, 63, 691–705. [Google Scholar] [CrossRef]
- Shah, T.I.; Bell, S.; Wilson, K. Spatial Accessibility to Health Care Services: Identifying under-Serviced Neighbourhoods in Canadian Urban Areas. PLoS ONE 2016, 11, e0168208. [Google Scholar] [CrossRef]
- Blackstock, J.; Chae, K.B.; McDonald, A.; Mauk, G.W. Achieving access to mental health care for school-aged children in rural communities. Rural Educ. 2018, 39, 12–25. [Google Scholar]
- DeVoe, J.E.; Krois, L.; Stenger, R. Do children in rural areas still have different access to health care? Results from a state-wide survey of Oregon’s food stamp population. J. Rural Health 2009, 25, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Cancel-Tirado, D.I.; Feeney, S.L.; Washburn, I.J.; Greder, K.A.; Sano, Y. Health, Well-being, and Health Care Access in Rural Communities. Fam. Community Health 2018, 41, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, A.J.; Haney, D.; Blake, K.D.; Moser, R.P.; Hesse, B.W. Differences in Access to and Use of Electronic Personal Health Information Between Rural and Urban Residents in the United States. J. Rural. Health 2018, 34, s30–s38. [Google Scholar] [CrossRef]
- U.S. Census Bureaua. Quick Facts Texas. 2021. Available online: https://www.census.gov/quickfacts/fact/table/TX/AGE135221 (accessed on 3 December 2023).
- Kinder Institute for Urban Research. After Census Redefines Urban and Rural, Texas Remains Steadfastly Both. Available online: https://kinder.rice.edu/urbanedge/census-redefines-urban-rural#:~:text=As%20a%20percentage%20of%20overall,of%20around%2090%25%20or%20more (accessed on 3 December 2023).
- U.S. Census Bureaub. Texas Joins California as State with 30-Million-Plus Population. 2023. Available online: https://www.census.gov/library/stories/2023/03/texas-population-passes-the-30-million-mark-in-2022.html#:~:text=The%20population%20of%20Texas%2C%20the,the%20next%20largest%2Dgaining%20state (accessed on 3 December 2023).
- Commission on Community College Finance Working Group; Texas Demographic Center. Updates on Texas’ Demographic Trends and the On-going Research at TDC. 2021. Available online: https://demographics.texas.gov/Resources/Presentations/OSD/2022/2022_03_07_CommissiononCommunityCollegeFinanceWorkingGroup.pdf (accessed on 3 December 2023).
- Federal Reserve Bank of Dallas. Migration to Texas Fills Critical Gaps in Workforce, Human Capital. 2022. Available online: https://www.dallasfed.org/research/economics/2022/1129 (accessed on 3 December 2023).
- Texas Comptroller. Young Texans: Demographic Overview. 2020. Available online: https://comptroller.texas.gov/economy/fiscal-notes/2020/feb/texans.php (accessed on 3 December 2023).
- Hua, H.; Xie, H.; Tanin, E. Is Euclidean distance really that bad with road networks? In Proceedings of the 11th ACM SIGSPATIAL International Workshop on Computational Transportation Science, Seattle, WA, USA, 6 November 2018; pp. 11–20. [Google Scholar]
- Boscoe, F.P.; Henry, K.A.; Zdeb, M.S. A Nationwide Comparison of Driving Distance Versus Straight-Line Distance to Hospitals. Prof. Geogr. 2012, 64, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, J.; García-Palomares, J.C. Distance-Measure Impacts on the Calculation of Transport Service Areas Using GIS. Environ. Plan. B Plan. Des. 2008, 35, 480–503. [Google Scholar] [CrossRef]
- Silalahi, F.E.S.; Hidayat, F.; Dewi, R.S.; Purwono, N.; Oktaviani, N. GIS-based approaches on the accessibility of referral hospital using network analysis and the spatial distribution model of the spreading case of COVID-19 in Jakarta, Indonesia. BMC Health Serv. Res. 2020, 20, 1053. [Google Scholar] [CrossRef] [PubMed]
- Comber, A.; Brunsdon, C.; Green, E. Using a GIS-based network analysis to determine urban greenspace accessibility for different ethnic and religious groups. Landsc. Urban Plan. 2008, 86, 103–114. [Google Scholar] [CrossRef]
- Environmental Systems Research Institute (Esri). ArcMap. 2023. Available online: https://desktop.arcgis.com/en/arcmap/latest/extensions/network-analyst/itemdesc-generate-service-areas.htm#:~:text=A%20network%20service%20area%20is,from%20one%20or%20more%20facilities (accessed on 19 January 2024).
- Bauer, J.; Klingelhöfer, D.; Maier, W.; Schwettmann, L.; Groneberg, D.A. Spatial accessibility of general inpatient care in Germany: An analysis of surgery, internal medicine and neurology. Sci. Rep. 2020, 10, 19157. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Tan, Y.; Song, Y.; Wu, P.; Cheng, J.C.P.; Kim, M.J.; Wang, X. Spatial and temporal variations of spatial population accessibility to public hospitals: A case study of rural–urban comparison. GISci. Remote Sens. 2018, 55, 718–744. [Google Scholar] [CrossRef]
- McCarthy, S.; Moore, D.; Smedley, W.A.; Crowley, B.M.; Stephens, S.W.; Griffin, R.L.; Tanner, L.C.; Jansen, J.O. Impact of Rural Hospital Closures on Health-Care Access. J. Surg. Res. 2021, 258, 170–178. [Google Scholar] [CrossRef]
- Siegler, A.J.; Bratcher, A.; Weiss, K.M. Geographic Access to Preexposure Prophylaxis Clinics Among Men Who Have Sex with Men in the United States. Am. J. Public Health 2019, 109, 1216–1223. [Google Scholar] [CrossRef]
- Rayburn, W.F.M.; Richards, M.E.; Elwell, E.C.B. Drive Times to Hospitals with Perinatal Care in the United States. Obstet. Gynecol. 2012, 119, 611–616. [Google Scholar] [CrossRef]
- Branas, C.C.; MacKenzie, E.J.; Williams, J.C.; Schwab, C.W.; Teter, H.M.; Flanigan, M.C.; Blatt, A.J.; ReVelle, C.S. Access to Trauma Centers in the United States. JAMA 2005, 293, 2626–2633. [Google Scholar] [CrossRef]
- Texas Health and Human Services. Health Professional Shortage Area (HPSA) Application. 2023. Available online: https://experience.arcgis.com/experience/323d93aa45fd43e88515cdf65365bf78/page/Page-1/?views=MUA (accessed on 3 December 2023).
- Rural Health Information Hub. Rural Health Disparities Overview. 2023. Available online: https://www.ruralhealthinfo.org/topics/rural-health-disparities (accessed on 3 December 2023).
- The Texas Organization of Rural & Community Hospitals. Rural Hospital Closures. 2023. Available online: https://www.torchnet.org/advocacy--rural-hospital-closure.html (accessed on 3 December 2023).
- Miller, K.E.M.; James, H.J.; Holmes, G.M.; Van Houtven, C.H. The effect of rural hospital closures on emergency medical service response and transport times. Health Serv. Res. 2020, 55, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Khullar, D.; Song, Z.; Chokshi, D.A. Safety-net health systems at risk: Who bears the burden of uncompensated care? Health Aff. Forefr. 2018. [Google Scholar] [CrossRef]
- Carver, J.L. Why Health Care Is Still Hard to Access in Rural Towns Near Texas’ Bigger Cities. The Texas Tribune. 2023. Available online: https://www.texastribune.org/2023/03/16/texas-health-care-deserts/ (accessed on 3 December 2023).
- Despart, Z.; Kriel, L.; Serrano, A.; Lee, J.S.; Hernandez, A.; Cahlan, S.; Piper, I.; Garcia, U.J. Uvalde Records Reveal Chaotic Medical Response as Victims Lost Blood. The Washington Post. 2022. Available online: https://www.washingtonpost.com/investigations/interactive/2022/uvalde-shooting-victims-delayed-response/ (accessed on 3 December 2023).
- Akinlotan, M.; Primm, K.; Khodakarami, N.; Bolin, J.; Ferdinand, A.O. Rural-Urban Variations in Travel Burdens for Care: Findings from the 2017 National Household Travel Survey; Southwest Rural Health Research Center: College Station, TX, USA, 2021. [Google Scholar]
- Gujral, K.; Basu, A. Impact of Rural and Urban Hospital Closures on Inpatient Mortality (No. w26182); National Bureau of Economic Research: Cambridge, MA, USA, 2019. [Google Scholar]
- Gentili, M.; Harati, P.; Serban, N.; O’Connor, J.; Swann, J. Quantifying Disparities in Accessibility and Availability of Pediatric Primary Care across Multiple States with Implications for Targeted Interventions. Health Serv. Res. 2018, 53, 1458–1477. [Google Scholar] [CrossRef] [PubMed]
- Furlow, B. Triple-demic overwhelms pediatric units in US hospitals. Lancet Child Adolesc. Health 2023, 7, 86. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.; Meckler, G.; Doan, Q. Pediatric emergency department overcrowding and adverse patient outcomes. Pediatr. Child Health 2017, 22, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Liu, Z.; Lin, S.; Zhao, P. Perceived accessibility and mental health consequences of COVID-19 containment policies. J. Transp. Health 2022, 25, 101354. [Google Scholar] [CrossRef]
- Edward, J.; Biddle, D.J. Using Geographic Information Systems (GIS) to Examine Barriers to Healthcare Access for Hispanic and Latino Immigrants in the U.S. South. J. Racial Ethn. Health Dispar. 2017, 4, 297–307. [Google Scholar] [CrossRef]
- Peltz, A.; Wu, C.L.; White, M.L.; Wilson, K.M.; Lorch, S.A.; Thurm, C.; Hall, M.; Berry, J.G. Characteristics of Rural Children Admitted to Pediatric Hospitals. Pediatrics 2016, 137, e20153156. [Google Scholar] [CrossRef]
- Rural Health Information Hub. Transportation to Support Rural Healthcare. 2023. Available online: https://www.ruralhealthinfo.org/topics/transportation (accessed on 3 December 2023).
- Liu, Y.; Zhong, L.; Yuan, S.; van de Klundert, J. Why patients prefer high-level healthcare facilities: A qualitative study using focus groups in rural and urban China. BMJ Glob. Health 2018, 3, e000854. [Google Scholar] [CrossRef]
- Sobo, E.J.; Seid, M.; Gelhard, L.R. Parent-identified barriers to pediatric health care: A process-oriented model. Health Serv. Res. 2006, 41, 148–172. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| State population | 29,164,943 |
| Children’s population | 7,470,055 (25.6% of the total state population) |
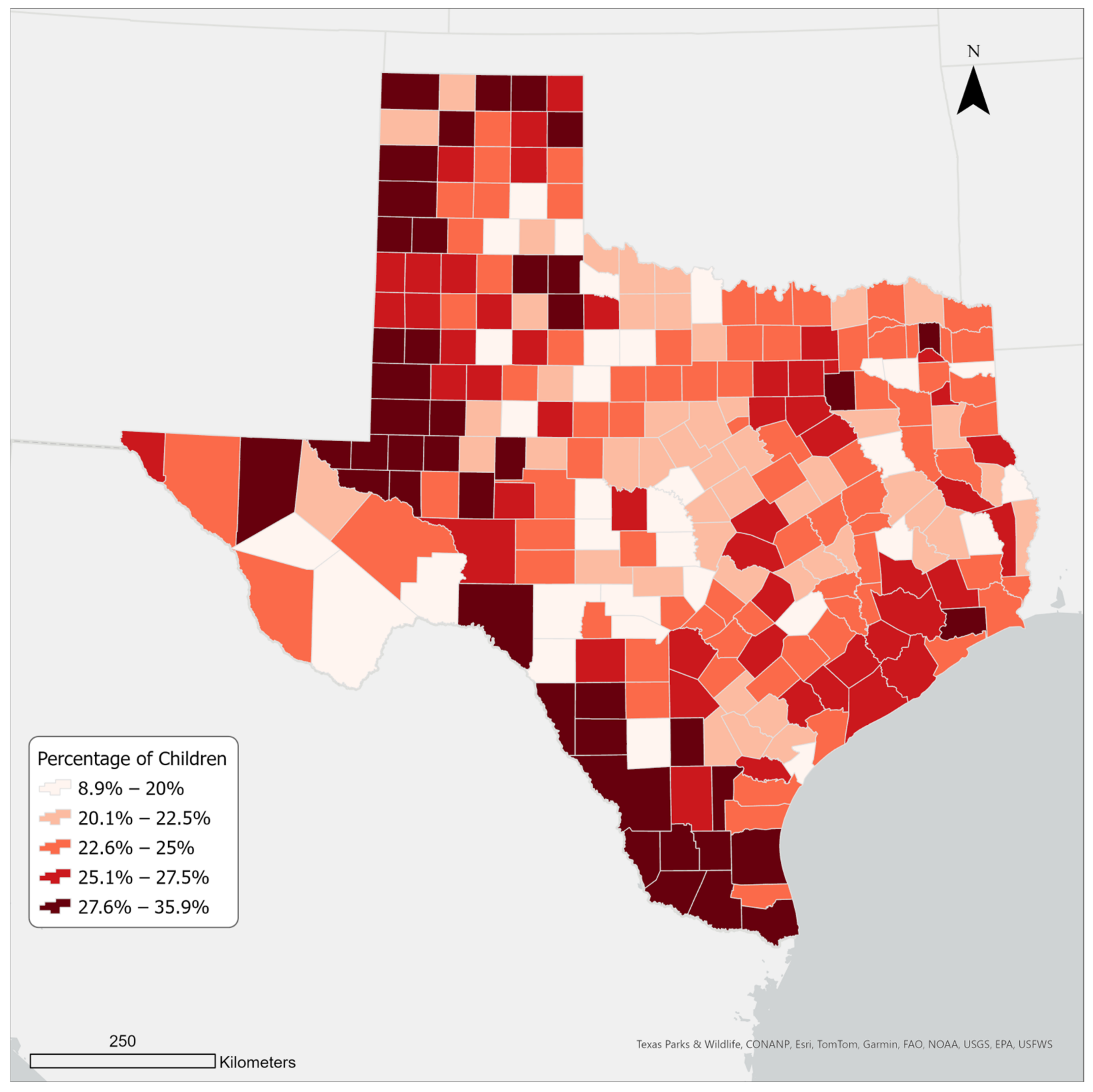
| Average percentage of children per county | 24 |
| Number of children’s hospitals | 24 |
| Characteristic | Value |
|---|---|
| Population of children | 7,470,055 |
| Population of children within the sixty-minute drive | 1,852,573 (24.8%) |
| Total number of counties in Texas | 254 |
| Texas counties that are completely or partially within the sixty-minute drive | 143 (56.3%) |
| Characteristic | Value |
|---|---|
| Number of households in Texas | 9,900,865 |
| Number of households in the 60-min service area | 7,518,876 (76%) |
| Number of households outside of the 60-min service area | 2,381,989 (24%) |
| Number of households without a vehicle in Texas | 533,500 (5.4%) |
| Number of households without a vehicle and in the 60-min service area | 396,833 (4%) |
| Number of households without a vehicle and outside the 60-min service area | 136,667 (1.4%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maleki, S.; Dede-Bamfo, N.; Ekren, E.; Mohammadalizadehkorde, M.; Villagran, M. Mapping Access to Children’s Hospitals in Texas. Int. J. Environ. Res. Public Health 2024, 21, 140. https://doi.org/10.3390/ijerph21020140
Maleki S, Dede-Bamfo N, Ekren E, Mohammadalizadehkorde M, Villagran M. Mapping Access to Children’s Hospitals in Texas. International Journal of Environmental Research and Public Health. 2024; 21(2):140. https://doi.org/10.3390/ijerph21020140
Chicago/Turabian StyleMaleki, Shadi, Nathaniel Dede-Bamfo, Elizabeth Ekren, Milad Mohammadalizadehkorde, and Melinda Villagran. 2024. "Mapping Access to Children’s Hospitals in Texas" International Journal of Environmental Research and Public Health 21, no. 2: 140. https://doi.org/10.3390/ijerph21020140
APA StyleMaleki, S., Dede-Bamfo, N., Ekren, E., Mohammadalizadehkorde, M., & Villagran, M. (2024). Mapping Access to Children’s Hospitals in Texas. International Journal of Environmental Research and Public Health, 21(2), 140. https://doi.org/10.3390/ijerph21020140